

Diagnostic Value of Whole-Blood and Plasma Samples in Epstein–Barr Virus Infections

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Samples
2.2. DNA Extraction
2.3. Nucleic Acid Amplification Test
2.4. Data Interpretation and Statistical Analysis
3. Results
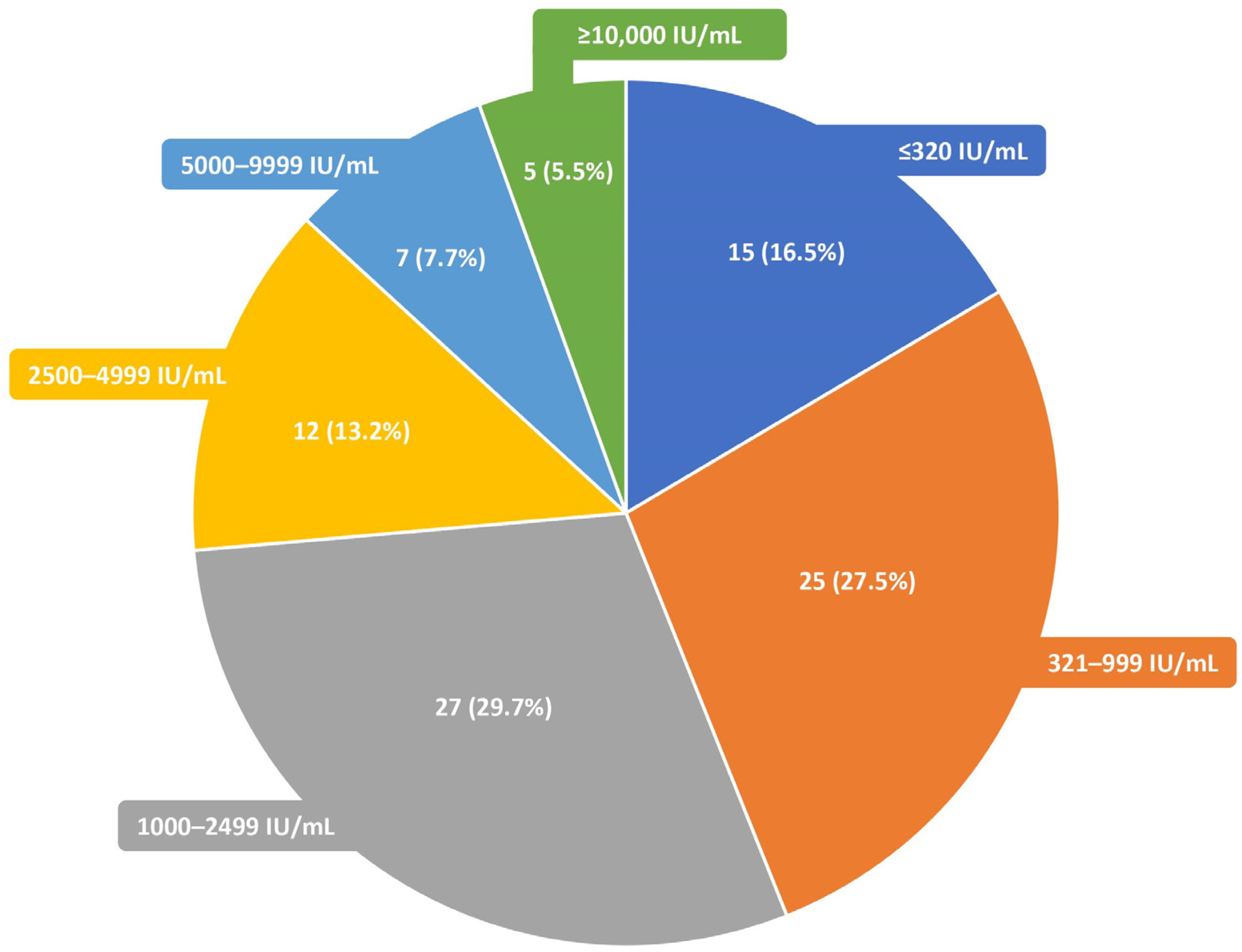
- Up to 5 times; 12 (32.4%) samples;
- 6–10 times; 9 (24.3%) samples;
- 11–25 times; 10 (27.0%) samples;
- >25 times; 6 (16.2%) samples.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Naughton, P.; Healy, M.; Enright, F.; Lucey, B. Infectious Mononucleosis: Diagnosis and Clinical Interpretation. Br. J. Biomed. Sci. 2021, 78, 107–116. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans Biological Agents. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100, 1–441. [Google Scholar]
- Münz, C. Latency and Lytic Replication in Epstein–Barr Virus-Associated Oncogenesis. Nat. Rev. Microbiol. 2019, 17, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Nowalk, A.; Green, M. Epstein-Barr Virus. Microbiol. Spectr. 2016, 4, 4.3.47. [Google Scholar] [CrossRef]
- Cohen, J.I.; Fauci, A.S.; Varmus, H.; Nabel, G.J. Epstein-Barr Virus: An Important Vaccine Target for Cancer Prevention. Sci. Transl. Med. 2011, 3, 107fs7. [Google Scholar] [CrossRef]
- Mazur-Melewska, K.; Breńska, I.; Jończyk-Potoczna, K.; Kemnitz, P.; Pieczonka-Ruszkowska, I.; Mania, A.; Służewski, W.; Figlerowicz, M. Neurologic Complications Caused by Epstein-Barr Virus in Pediatric Patients. J. Child. Neurol. 2016, 31, 700–708. [Google Scholar] [CrossRef]
- Costa, B.K.D.; Sato, D.K. Viral Encephalitis: A Practical Review on Diagnostic Approach and Treatment. J. Pediatr. 2020, 96, 12–19. [Google Scholar] [CrossRef]
- Ayee, R.; Ofori, M.E.; Wright, E.; Quaye, O. Epstein Barr Virus Associated Lymphomas and Epithelia Cancers in Humans. J. Cancer 2020, 11, 1737–1750. [Google Scholar] [CrossRef]
- Qiu, L.; Si, J.; Kang, J.; Chen, Z.; Nuermaimaiti, R.; Qian, Z.; Li, L.; Zhou, S.; You, M.J.; Zhang, H.; et al. A Retrospective Analysis of EBV-DNA Status with the Prognosis of Lymphoma. J. Cell. Mol. Med. 2022, 26, 5195–5201. [Google Scholar] [CrossRef]
- Styczynski, J.; van der Velden, W.; Fox, C.P.; Engelhard, D.; de la Camara, R.; Cordonnier, C.; Ljungman, P.; on behalf of the Sixth European Conference on Infections in Leukemia, a joint venture of the Infectious Diseases Working Party of the European Society of Blood and Marrow Transplantation (EBMT-IDWP), the Infectious Diseases Group of the European Organization for Research and Treatment of Cancer (EORTC-IDG), the International Immunocompromised Host Society (ICHS) and the European Leukemia Net (ELN). Management of Epstein-Barr Virus Infections and Post-Transplant Lymphoproliferative Disorders in Patients after Allogeneic Hematopoietic Stem Cell Transplantation: Sixth European Conference on Infections in Leukemia (ECIL-6) Guidelines. Haematologica 2016, 101, 803–811. [Google Scholar] [CrossRef]
- Curtis, R.E.; Travis, L.B.; Rowlings, P.A.; Socié, G.; Kingma, D.W.; Banks, P.M.; Jaffe, E.S.; Sale, G.E.; Horowitz, M.M.; Witherspoon, R.P.; et al. Risk of Lymphoproliferative Disorders after Bone Marrow Transplantation: A Multi-Institutional Study. Blood 1999, 94, 2208–2216. [Google Scholar] [PubMed]
- Patriarca, F.; Medeot, M.; Isola, M.; Battista, M.L.; Sperotto, A.; Pipan, C.; Toffoletti, E.; Dozzo, M.; Michelutti, A.; Gregoraci, G.; et al. Prognostic Factors and Outcome of Epstein-Barr Virus DNAemia in High-Risk Recipients of Allogeneic Stem Cell Transplantation Treated with Preemptive Rituximab. Transpl. Infect. Dis. 2013, 15, 259–267. [Google Scholar] [CrossRef]
- Ferla, V.; Rossi, F.G.; Goldaniga, M.C.; Baldini, L. Biological Difference Between Epstein–Barr Virus Positive and Negative Post-Transplant Lymphoproliferative Disorders and Their Clinical Impact. Front. Oncol. 2020, 10, 506. [Google Scholar] [CrossRef] [PubMed]
- Styczynski, J.; Reusser, P.; Einsele, H.; de la Camara, R.; Cordonnier, C.; Ward, K.N.; Ljungman, P.; Engelhard, D.; for the European Conference on Infections in Leukemia. Management of HSV, VZV and EBV Infections in Patients with Hematological Malignancies and after SCT: Guidelines from the Second European Conference on Infections in Leukemia. Bone Marrow Transpl. 2009, 43, 757–770. [Google Scholar] [CrossRef]
- Knipe, D.M.; Howley, P.M. (Eds.) Fields Virology, 6th ed.; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2013; ISBN 978-1-4511-0563-6. [Google Scholar]
- Hislop, A.D.; Taylor, G.S.; Sauce, D.; Rickinson, A.B. Cellular Responses to Viral Infection in Humans: Lessons from Epstein-Barr Virus. Annu. Rev. Immunol. 2007, 25, 587–617. [Google Scholar] [CrossRef]
- Nijland, M.L.; Kersten, M.J.; Pals, S.T.; Bemelman, F.J.; ten Berge, I.J.M. Epstein-Barr Virus–Positive Posttransplant Lymphoproliferative Disease After Solid Organ Transplantation: Pathogenesis, Clinical Manifestations, Diagnosis, and Management. Transplant. Direct. 2016, 2, e48. [Google Scholar] [CrossRef]
- San-Juan, R.; Comoli, P.; Caillard, S.; Moulin, B.; Hirsch, H.H.; Meylan, P. Epstein-Barr Virus-Related Post-Transplant Lymphoproliferative Disorder in Solid Organ Transplant Recipients. Clin. Microbiol. Infect. 2014, 20, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Kwong, Y.-L. EBV Viral Loads in Diagnosis, Monitoring, and Response Assessment. Front. Oncol. 2019, 9, 62. [Google Scholar] [CrossRef] [PubMed]
- Kanakry, J.; Ambinder, R. The Biology and Clinical Utility of EBV Monitoring in Blood. In Epstein Barr Virus; Münz, C., Ed.; Current Topics in Microbiology and Immunology; Springer International Publishing: Cham, Switzerland, 2015; Volume 2, pp. 475–499. ISBN 978-3-319-22833-4. [Google Scholar]
- Chan, K.C.A.; Woo, J.K.S.; King, A.; Zee, B.C.Y.; Lam, W.K.J.; Chan, S.L.; Chu, S.W.I.; Mak, C.; Tse, I.O.L.; Leung, S.Y.M.; et al. Analysis of Plasma Epstein–Barr Virus DNA to Screen for Nasopharyngeal Cancer. N. Engl. J. Med. 2017, 377, 513–522. [Google Scholar] [CrossRef]
- Fryer, J.F.; Heath, A.B.; Minor, P.D.; Collaborative Study Group. A Collaborative Study to Establish the 1st WHO International Standard for Human Cytomegalovirus for Nucleic Acid Amplification Technology. Biologicals 2016, 44, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Meerbach, A.; Wutzler, P.; Häfer, R.; Zintl, F.; Gruhn, B. Monitoring of Epstein-Barr Virus Load after Hematopoietic Stem Cell Transplantation for Early Intervention in Post-Transplant Lymphoproliferative Disease. J. Med. Virol. 2008, 80, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Tsai, D.E.; Douglas, L.; Andreadis, C.; Vogl, D.T.; Arnoldi, S.; Kotloff, R.; Svoboda, J.; Bloom, R.D.; Olthoff, K.M.; Brozena, S.C.; et al. EBV PCR in the Diagnosis and Monitoring of Posttransplant Lymphoproliferative Disorder: Results of a Two-Arm Prospective Trial. Am. J. Transplant. 2008, 8, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- van Esser, J.W.J.; van der Holt, B.; Meijer, E.; Niesters, H.G.M.; Trenschel, R.; Thijsen, S.F.T.; van Loon, A.M.; Frassoni, F.; Bacigalupo, A.; Schaefer, U.W.; et al. Epstein-Barr Virus (EBV) Reactivation Is a Frequent Event after Allogeneic Stem Cell Transplantation (SCT) and Quantitatively Predicts EBV-Lymphoproliferative Disease Following T-Cell–Depleted SCT. Blood 2001, 98, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Ruf, S.; Behnke-Hall, K.; Gruhn, B.; Bauer, J.; Horn, M.; Beck, J.; Reiter, A.; Wagner, H.J. Comparison of Six Different Specimen Types for Epstein-Barr Viral Load Quantification in Peripheral Blood of Pediatric Patients after Heart Transplantation or after Allogeneic Hematopoietic Stem Cell Transplantation. J. Clin. Virol. 2012, 53, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Lazzarotto, T.; Chiereghin, A.; Piralla, A.; Gibertoni, D.; Piccirilli, G.; Turello, G.; Campanini, G.; Gabrielli, L.; Costa, C.; Comai, G.; et al. Kinetics of Cytomegalovirus and Epstein-Barr Virus DNA in Whole Blood and Plasma of Kidney Transplant Recipients: Implications on Management Strategies. PLoS ONE 2020, 15, e0238062. [Google Scholar] [CrossRef] [PubMed]
- Lazzarotto, T.; Chiereghin, A.; Piralla, A.; Piccirilli, G.; Girello, A.; Campanini, G.; Gabrielli, L.; Costa, C.; Prete, A.; Bonifazi, F.; et al. Cytomegalovirus and Epstein-Barr Virus DNA Kinetics in Whole Blood and Plasma of Allogeneic Hematopoietic Stem Cell Transplantation Recipients. Biol. Blood Marrow Transplant. 2018, 24, 1699–1706. [Google Scholar] [CrossRef] [PubMed]
- Kanakry, J.A.; Hegde, A.M.; Durand, C.M.; Massie, A.B.; Greer, A.E.; Ambinder, R.F.; Valsamakis, A. The Clinical Significance of EBV DNA in the Plasma and Peripheral Blood Mononuclear Cells of Patients with or without EBV Diseases. Blood 2016, 127, 2007–2017. [Google Scholar] [CrossRef]
- Van Roosbroeck, K.; Calin, G.A. When Kissing (Disease) Counts. Blood 2016, 127, 1947–1948. [Google Scholar] [CrossRef]
- Wadowsky, R.M.; Laus, S.; Green, M.; Webber, S.A.; Rowe, D. Measurement of Epstein-Barr Virus DNA Loads in Whole Blood and Plasma by TaqMan PCR and in Peripheral Blood Lymphocytes by Competitive PCR. J. Clin. Microbiol. 2003, 41, 5245–5249. [Google Scholar] [CrossRef]
- Ouedraogo, D.E.; Bollore, K.; Viljoen, J.; Foulongne, V.; Reynes, J.; Cartron, G.; Vendrell, J.-P.; Van de Perre, P.; Tuaillon, E. Comparison of EBV DNA Viral Load in Whole Blood, Plasma, B-Cells and B-Cell Culture Supernatant: EBV DNA Load in Various Blood Specimens. J. Med. Virol. 2014, 86, 851–856. [Google Scholar] [CrossRef]
- Rzepka, M.; Depka, D.; Gospodarek-Komkowska, E.; Bogiel, T. Whole Blood versus Plasma Samples—How Does the Type of Specimen Collected for Testing Affect the Monitoring of Cytomegalovirus Viremia? Pathogens 2022, 11, 1384. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.-Y.; Liu, Q.-F.; Wang, H.; Jin, J.; Wang, W.-H.; Wang, S.-L.; Song, Y.-W.; Liu, Y.-P.; Fang, H.; Ren, H.; et al. Clinical Implications of Plasma Epstein-Barr Virus DNA in Early-Stage Extranodal Nasal-Type NK/T-Cell Lymphoma Patients Receiving Primary Radiotherapy. Blood 2012, 120, 2003–2010. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-X.; Li, P.-F.; Bai, B.; Gao, Y.; Rong, Q.-X.; Cai, Q.-Q.; Lin, S.-X.; Zhang, Y.-J.; Li, Z.-M.; Jiang, W.-Q.; et al. Differential Clinical Significance of Pre-, Interim-, and Post-Treatment Plasma Epstein–Barr Virus DNA Load in NK/T-Cell Lymphoma Treated with P-GEMOX Protocol. Leuk. Lymphoma 2019, 60, 1917–1925. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kim, K.H.; Kim, K.H.; Chang, M.H.; Ji, S.H.; Lim, D.H.; Kim, K.; Kim, S.J.; Ko, Y.; Ki, C.-S.; et al. Whole Blood Epstein-Barr Virus DNA Load as a Diagnostic and Prognostic Surrogate: Extranodal Natural Killer/T-Cell Lymphoma. Leuk. Lymphoma 2009, 50, 757–763. [Google Scholar] [CrossRef]
- Ha, J.Y.; Cho, H.; Sung, H.; Jung, A.R.; Lee, Y.S.; Lee, S.-W.; Ryu, J.-S.; Chae, E.J.; Kim, K.W.; Huh, J.; et al. Superiority of Epstein-Barr Virus DNA in the Plasma Over Whole Blood for Prognostication of Extranodal NK/T Cell Lymphoma. Front. Oncol. 2020, 10, 594692. [Google Scholar] [CrossRef]
- Yan, Z.; Yao, Z.; Wang, H.; Yao, S.; Wang, X.; Gao, Y.; Bai, B.; Chu, J.; Zhao, S.; Luo, X.; et al. Plasma EBV-DNA and Peripheral Blood Mononuclear Cell EBV-DNA Have Disparate Clinical Relevance in Patients with Extranodal NK/T-Cell Lymphoma. J. Clin. Virol. 2022, 157, 105320. [Google Scholar] [CrossRef]
- Ito, Y.; Kimura, H.; Maeda, Y.; Hashimoto, C.; Ishida, F.; Izutsu, K.; Fukushima, N.; Isobe, Y.; Takizawa, J.; Hasegawa, Y.; et al. Pretreatment EBV-DNA Copy Number Is Predictive of Response and Toxicities to SMILE Chemotherapy for Extranodal NK/T-Cell Lymphoma, Nasal Type. Clin. Cancer Res. 2012, 18, 4183–4190. [Google Scholar] [CrossRef]
- Park, J.H.; Yoon, D.H.; Kim, S.; Park, J.S.; Park, C.; Sung, H.; Lee, S.-W.; Huh, J.; Suh, C. Pretreatment Whole Blood Epstein-Barr Virus-DNA Is a Significant Prognostic Marker in Patients with Hodgkin Lymphoma. Ann. Hematol. 2016, 95, 801–808. [Google Scholar] [CrossRef]
- Tisi, M.C.; Cupelli, E.; Santangelo, R.; Maiolo, E.; Alma, E.; Giachelia, M.; Martini, M.; Bellesi, S.; D’Alò, F.; Voso, M.T.; et al. Whole Blood EBV-DNA Predicts Outcome in Diffuse Large B-Cell Lymphoma. Leuk. Lymphoma 2016, 57, 628–634. [Google Scholar] [CrossRef]
- Shi, T.; Huang, L.; Tian, J. Prevalence of Epstein-Barr Viral DNA among Children at a Single Hospital in Suzhou, China. J. Pediatr. 2022, 98, 142–146. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age Group | Sex | n | Percentage |
|---|---|---|---|
| Children | Female | 12 | 23.5% |
| Male | 12 | 23.5% | |
| Adults | Female | 12 | 23.5% |
| Male | 15 | 29.4% |
| Whole Blood | Plasma | ||
|---|---|---|---|
| Positive EBV DNA | Positive EBV DNA | Negative EBV DNA | |
| n | 134 | 43 | 91 |
| Percentage | 100% | 32.1% | 67.9% |
| Sample No. | EBV DNA (IU/mL) Level | Difference | |
|---|---|---|---|
| In Whole Blood | In Plasma | ||
| 15,729 | 1080 | 1350 | 270 |
| 15,679 | 22,400 | 22,800 | 400 |
| 18,216 | 320 | 360 | 40 |
| 17,343 | 630 | 5500 | 4870 |
| 15,407 | 400 | 510 | 110 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzepka, M.; Depka, D.; Gospodarek-Komkowska, E.; Bogiel, T. Diagnostic Value of Whole-Blood and Plasma Samples in Epstein–Barr Virus Infections. Diagnostics 2023, 13, 476. https://doi.org/10.3390/diagnostics13030476
Rzepka M, Depka D, Gospodarek-Komkowska E, Bogiel T. Diagnostic Value of Whole-Blood and Plasma Samples in Epstein–Barr Virus Infections. Diagnostics. 2023; 13(3):476. https://doi.org/10.3390/diagnostics13030476
Chicago/Turabian StyleRzepka, Mateusz, Dagmara Depka, Eugenia Gospodarek-Komkowska, and Tomasz Bogiel. 2023. "Diagnostic Value of Whole-Blood and Plasma Samples in Epstein–Barr Virus Infections" Diagnostics 13, no. 3: 476. https://doi.org/10.3390/diagnostics13030476
APA StyleRzepka, M., Depka, D., Gospodarek-Komkowska, E., & Bogiel, T. (2023). Diagnostic Value of Whole-Blood and Plasma Samples in Epstein–Barr Virus Infections. Diagnostics, 13(3), 476. https://doi.org/10.3390/diagnostics13030476