


Prehospital Targeting of 1-Year Mortality in Acute Chest Pain by Cardiac Biomarkers


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Issues
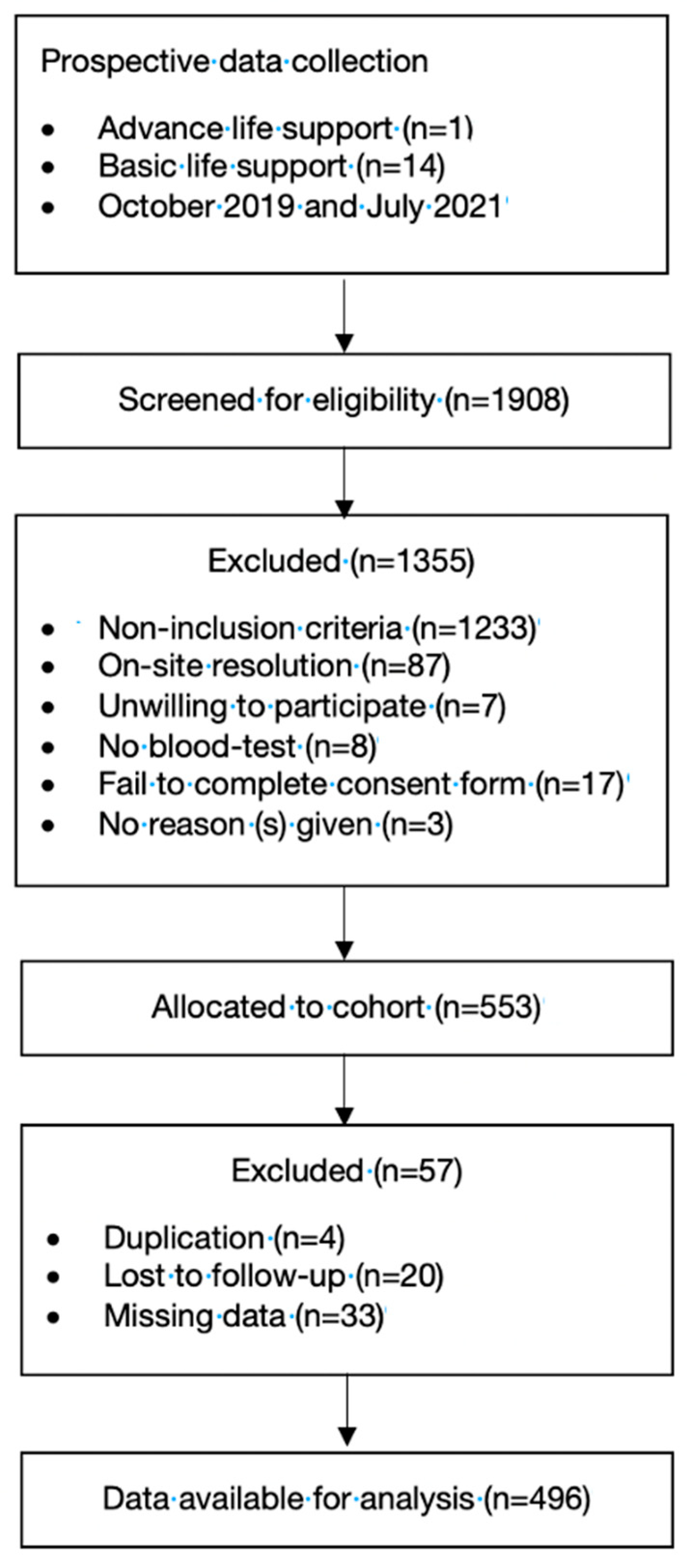
2.2. Participants
2.3. Outcomes
2.4. Predictors and Data Collection
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pedersen, C.K.; Stengaard, C.; Friesgaard, K.; Dodt, K.K.; Søndergaard, H.M.; Terkelsen, C.J.; Bøtker, M.T. Chest pain in the ambulance; prevalence, causes and outcome—A retrospective cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 84. [Google Scholar] [CrossRef] [PubMed]
- Raymondi, D.M.; Garcia, H.; Álvarez, I.; Hernández, L.; Molinero, J.P.; Villamandos, V. TUSARC: Prognostic Value of High-Sensitivity Cardiac Troponin T Assay in Asymptomatic Patients with High Cardiovascular Risk. Am. J. Med. 2019, 132, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.J. Prehospital Cardiac Care: Diagnosis and Management of Acute Chest Pain and Dyspnea. Eur. Hear. J. Acute Cardiovasc. Care 2020, 9 (Suppl. 1), 3–4. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, I.E.; Kozicky, R.; Dalgarno, D.; Simms, J.; Goulder, S.; Williamson, T.S.; Biesbroek, S.; Page, L.; Leaman, K.; Snozyk, S.; et al. Community paramedic point of care testing: Validity and usability of two commercially available devices. BMC Emerg. Med. 2019, 19, 30. [Google Scholar] [CrossRef] [PubMed]
- Martín-Rodríguez, F.; López-Izquierdo, R.; Medina-Lozano, E.; Rabbione, G.O.; Del Pozo Vegas, C.; Rodríguez, V.C.; Villamor, M.Á.C.; Sánchez-Soberon, I.; Sanz-García, A. Accuracy of prehospital point-of-care lactate in early in-hospital mortality. Eur. J. Clin. Investig. 2020, 50, e13341. [Google Scholar] [CrossRef] [PubMed]
- Dawson, L.P.; Nehme, E.; Nehme, Z.; Zomer, E.; Bloom, J.; Cox, S.; Anderson, D.; Stephenson, M.; Ball, J.; Zhou, J.; et al. Chest Pain Management Using Prehospital Point-of-Care Troponin and Paramedic Risk Assessment. JAMA Intern. Med. 2023, 183, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Castro-Portillo, E.; López-Izquierdo, R.; Sanz-García, A.; Ortega, G.J.; Delgado-Benito, J.F.; Villamor, M.A.C.; Sánchez-Soberón, I.; Vegas, C.d.P.; Martín-Rodríguez, F. Role of prehospital point-of-care N-terminal pro-brain natriuretic peptide in acute life-threatening cardiovascular disease. Int. J. Cardiol. 2022, 364, 126–132. [Google Scholar] [CrossRef]
- Oehme, R.; Sandholzer-Yilmaz, A.S.; Heise, M.; Frese, T.; Fankhaenel, T. Utilization of point-of-care tests among general practitioners, a cross-sectional study. BMC Prim. Care 2022, 23, 41. [Google Scholar] [CrossRef]
- Gulati, M.; Levy, P.D.; Mukherjee, D.; Amsterdam, E.; Bhatt, D.L.; Birtcher, K.K.; Blankstein, R.; Boyd, J.; Bullock-Palmer, R.P.; Conejo, T.; et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 144, e368–e454. [Google Scholar]
- Kaura, A.; Panoulas, V.; Glampson, B.; Davies, J.; Mulla, A.; Woods, K.; Omigie, J.; Shah, A.D.; Channon, K.M.; Weber, J.N.; et al. Association of troponin level and age with mortality in 250,000 patients: Cohort study across five UK acute care centers. BMJ 2019, 367, I6055. [Google Scholar] [CrossRef]
- Stewart, R.A.H.; Kirby, A.; White, H.D.; Marschner, S.L.; West, M.; Thompson, P.L.; Sullivan, D.; Janus, E.; Hunt, D.; Kritharides, L.; et al. B-Type Natriuretic Peptide and Long-Term Cardiovascular Mortality in Patients with Coronary Heart Disease. J. Am. Hear. Assoc. 2022, 11, e024216. [Google Scholar] [CrossRef] [PubMed]
- Mjelva, Ø.R.; Pönitz, V.; Brügger-Andersen, T.; Grundt, H.; Staines, H.; Nilsen, D.W. Long-term prognostic utility of pentraxin 3 and D-dimer as compared to high-sensitivity C-reactive protein and B-type natriuretic peptide in suspected acute coronary syndrome. Eur. J. Prev. Cardiol. 2016, 23, 1130–1140. [Google Scholar] [CrossRef] [PubMed]
- Martín-Rodríguez, F.; Sanz-Garcí, A.; Castro-Portillo, E.; Delgado-Benito, J.F.; Del Pozo Vegas, C.; Rabbione, G.O.; Martín-Herrero, F.; Martín-Conty, J.L.; López-Izquierdo, R. Prehospital troponin as a predictor of early clinical deterioration. Eur. J. Clin. Investig. 2021, 51, e13591. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Lalic, N.; Montanya, E.; Valensi, P.; Khunti, K.; Hummel, M.; Schnell, O. NT-proBNP point-of-care measurement as a screening tool for heart failure and CVD risk in type 2 diabetes with hypertension. J. Diabetes Complicat. 2023, 37, 108410. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Calle, E.; Espindola, P.; Spinke, J.; Lutz, S.; Nichtl, A.; Tgetgel, A.; Herbert, N.; Marcinowski, M.; Klepp, J.; Fischer, T.; et al. A new immunochemistry platform for a guideline-compliant cardiac troponin T assay at the point of care: Proof of principle. Clin. Chem. Lab. Med. 2017, 56, 1798–1804. [Google Scholar] [CrossRef] [PubMed]
- Welsh, P.; Campbell, R.T.; Mooney, L.; Kimenai, D.M.; Hayward, C.; Campbell, A.; Porteous, D.; Mills, N.L.; Lang, N.N.; Petrie, M.C.; et al. Reference Ranges for NT-proBNP (N-Terminal Pro-B-Type Natriuretic Peptide) and Risk Factors for Higher NT-proBNP Concentrations in a Large General Population Cohort. Circ. Heart Fail. 2022, 15, e009427. [Google Scholar] [CrossRef]
- Myhre, P.L.; Claggett, B.; Yu, B.; Skali, H.; Solomon, S.D.; Røsjø, H.; Omland, T.; Wiggins, K.L.; Psaty, B.M.; Floyd, J.S.; et al. Sex and Race Differences in N-Terminal Pro–B-type Natriuretic Peptide Concentration and Absolute Risk of Heart Failure in the Community. JAMA Cardiol. 2022, 7, 623–631. [Google Scholar] [CrossRef]
- Wang, J.; Gao, W.; Chen, G.; Chen, M.; Wan, Z.; Zheng, W.; Ma, J.; Pang, J.; Wang, G.; Wu, S.; et al. Biomarker-based risk model to predict cardiovascular events in patients with acute coronary syndromes—Results from BIPass registry. Lancet Reg. Health West. Pac. 2022, 25, 100479. [Google Scholar] [CrossRef]
- Sabbatinelli, J.; Giuliani, A.; Bonfigli, A.R.; Ramini, D.; Matacchione, G.; Campolucci, C.; Ceka, A.; Tortato, E.; Rippo, M.R.; Procopio, A.D.; et al. Prognostic value of soluble ST2, high-sensitivity cardiac troponin, and NT-proBNP in type 2 diabetes: A 15-year retrospective study. Cardiovasc Diabetol. 2022, 21, 180. [Google Scholar] [CrossRef]
- Cainzos-Achirica, M.; Acquah, I.; Dardari, Z.; Mszar, R.; Greenland, P.; Blankstein, R.; Bittencourt, M.; Rajagopalan, S.; Al-Kindi, S.G.; Polak, J.F.; et al. Long-Term Prognostic Implications and Role of Further Testing in Adults Aged ≤55 Years with a Coronary Calcium Score of Zero (from the Multi-Ethnic Study of Atherosclerosis). Am. J. Cardiol. 2021, 161, 26–35. [Google Scholar] [CrossRef]
- van der Zee, P.M.; Cornel, J.H.; Bholasingh, R.; Fischer, J.C.; van Straalen, J.P.; De Winter, R.J. N-Terminal Pro B-Type Natriuretic Peptide Identifies Patients with Chest Pain at High Long-term Cardiovascular Risk. Am. J. Med. 2011, 124, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Behnes, M.; Espeter, F.; Hoffmann, U.; Lang, S.; Brueckmann, M.; Akin, I.; Borggrefe, M.; Bertsch, T.; Weiss, C.; Neumaier, M.; et al. Value of Sensitive Troponin I in Symptomatic Patients Suspected of Acute Heart Failure. Clin. Lab. 2015, 61, 1737–1747. [Google Scholar] [PubMed]
- Simes, J.; Robledo, K.P.; White, H.D.; Espinoza, D.; Stewart, R.A.; Sullivan, D.R.; Zeller, T.; Hague, W.; Nestel, P.J.; Glasziou, P.P.; et al. D-Dimer Predicts Long-Term Cause-Specific Mortality, Cardiovascular Events, and Cancer in Patients with Stable Coronary Heart Disease: LIPID Study. Circulation 2018, 138, 712–723. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, H.; Khanal, M.K. Development of scoring system for risk stratification in clinical medicine: A step-by-step tutorial. Ann. Transl. Med. 2017, 5, 436. [Google Scholar] [CrossRef] [PubMed]
- Wibring, K.; Lingman, M.; Herlitz, J.; Amin, S.; Bång, A. Prehospital stratification in acute chest pain patient into high risk and low risk by emergency medical service: A prospective cohort study. BMJ Open 2021, 11, e044938. [Google Scholar] [CrossRef] [PubMed]
- Claret, P.G.; Bobbia, X.; Roger, C.; Sebbane, M.; de La Coussaye, J.E. Review of point-of-care testing and biomarkers of cardiovascular diseases in emergency and prehospital medicine. Acta Cardiol. 2015, 70, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, C.K.; Stengaard, C.; Bøtker, M.T.; Søndergaard, H.M.; Dodt, K.K.; Terkelsen, C.J. Accelerated Rule-Out of acute Myocardial Infarction using prehospital copeptin and in-hospital troponin: The AROMI study. Eur. Hear. J. 2023, 44, 3875–3888. [Google Scholar] [CrossRef]
- Aarts, G.W.A.; Camaro, C.; van Royen, N. Ready for rapid rule-out of acute myocardial infarction. Eur. Hear. J. 2023, 44, 3889–3891. [Google Scholar] [CrossRef]
- Stopyra, J.P.; Snavely, A.C.; Scheidler, J.F.; Smith, L.M.; Nelson, R.D.; Winslow, J.E.; Pomper, G.J.; Ashburn, N.P.; Hendley, N.W.; Riley, R.F.; et al. Point-of-Care Troponin Testing during Ambulance Transport to Detect Acute Myocardial Infarction. Prehospital Emerg. Care 2020, 24, 751–759. [Google Scholar] [CrossRef]
- Aung, S.; Vittinghoff, E.; Nah, G.; Lin, A.; Joyce, S.; Mann, N.C.; Marcus, G.M. Emergency activations for chest pain and ventricular arrhythmias related to regional COVID-19 across the US. Sci. Rep. 2021, 11, 23959. [Google Scholar] [CrossRef] [PubMed]
- Pines, J.M.; Zocchi, M.S.; Black, B.S.; Celedon, P.; Carlson, J.N.; Moghtaderi, A.; Venkat, A. The effect of the COVID-19 pandemic on emergency department visits for serious cardiovascular conditions. Am. J. Emerg. Med. 2021, 47, 42–51. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total | Survivors | Nonsurvivors | p Value 2 |
|---|---|---|---|---|
| No. (%) with data 1 | 496 | 436 (87.9) | 60 (12.1) | NA |
| Epidemiological variables | ||||
| Sex at birth, female | 190 (38.3) | 172 (39.4) | 18 (30) | 0.159 |
| Age, year | 71 (51–80) | 71 (57–80) | 75 (65–85) | 0.004 |
| Age groups, year | ||||
| 18–49 | 63 (12.7) | 58 (13.3) | 5 (8.3) | 0.061 |
| 50–74 | 231 (46.6) | 207 (47.5) | 24 (40) | |
| >75 | 202 (40.7) | 171 (39.2) | 31 (51.7) | |
| Zone, rural | 120 (24.2) | 106 (24.3) | 14 (23.3) | 0.869 |
| Transfer, ALS | 365 (71.8) | 305 (70) | 51 (85) | 0.015 |
| On-scene vital signs | ||||
| RR, breaths/min | 16 (14–19) | 16 (14–19) | 18 (14–27) | <0.001 |
| SpO2, % | 97 (95–98) | 97 (95–98) | 94 (85–97) | <0.001 |
| SBP, mmHg | 144 (122–168) | 146 (125–169) | 129 (89–156) | <0.001 |
| DBP, mmHg | 82 (69–95) | 83 (77–96) | 65 (46–81) | <0.001 |
| Heart rate, beats/min | 78 (65–95) | 77 (65–93) | 86 (68–124) | 0.004 |
| Temperature, °C | 36 (35.8–36.8) | 36.1 (35.8–36.5) | 36 (35.6–36.7) | 0.243 |
| Glasgow coma scale, points | 15 (15–15) | 15 (15–15) | 15 (7–15) | 0.001 |
| Baseline cardiac rhythm | ||||
| Sinus | 291 (51.7) | 275 (63.1) | 16 (26.7) | <0.001 |
| Tachycardia 3 | 149 (30) | 112 (25.7) | 37 (67.1) | |
| Bradycardia 4 | 46 (9.3) | 41 (9.8) | 5 (8.3) | |
| Pacemaker | 10 (2) | 8 (1.8) | 2 (3.3) | |
| ST elevation 5 | 113 (22.8) | 95 (21.8) | 18 (30) | 0.594 |
| Prehospital diagnosis | 0.021 | |||
| Acute chest pain | 352 (71) | 317 (72.7) | 35 (58.3) | |
| Myocardial infarction code | 144 (29) | 119 (27.3) | 25 (41.7) | |
| Cardiac biomarkers | ||||
| Troponin T, ng/L | 47 (0–109) | 42 (0–91) | 112 (57–336) | <0.001 |
| NT-proBNP, pg/mL | 235 (63–997) | 221 (0–643) | 2131 (932–5583) | <0.001 |
| D-dimer, microg/mL | 410 (220–753) | 352 (200–680) | 954 (414–2260) | <0.001 |
| Support on-scene | ||||
| Mechanical ventilation | 23 (4.6) | 4 (0.9) | 19 (31.7) | <0.001 |
| Defibrillation | 14 (2.8) | 3 (0.7) | 11 (18.3) | <0.001 |
| Cardioversion | 11 (2.2) | 6 (1.4) | 5 (8.3) | 0.001 |
| Transcutaneous pacemaker | 9 (1.8) | 7 (1.6) | 2 (3.3) | 0.348 |
| Vasoactive agents | 25 (5) | 6 (1.4) | 19 (31.7) | <0.001 |
| Hospital outcome | ||||
| ACCI, points | 2 (1–4) | 2 (1–3) | 3 (2–5) | 0.004 |
| Inpatient | 301 (60.7) | 249 (57.1) | 52 (86.7) | 0.001 |
| Hospitalization time, days | 3 (0–6) | 0 (0–1) | 2 (0–14) | 0.069 |
| Fibrinolysis | 17 (3.4) | 8 (1.8) | 9 (15) | <0.001 |
| PCI | 193 (38.1) | 163 (37.1) | 30 (50) | 0.061 |
| ECS | 9 (1.8) | 8 (1.8) | 1 (1.7) | 0.927 |
| Mechanical ventilation | 41 (8.3) | 17 (3.9) | 24 (40) | <0.001 |
| Vasoactive agents | 49 (9.9) | 20 (4.6) | 29 (48.3) | <0.001 |
| ICU-admission | 194 (39.1) | 157 (36) | 37 (61.7) | <0.001 |
| Variables | Acute Chest Pain | Myocardial Infarction Code | p Value 2 |
|---|---|---|---|
| No. (%) with data 1 | 352 (71) | 144 (29) | NA |
| Epidemiological variables | |||
| Sex at birth, female | 149 (42.3) | 41 (28.5) | 0.004 |
| Age, year | 73 (59–83) | 67 (56–77) | 0.119 |
| Zone, rural | 77 (21.8) | 43 (29.9) | 0.061 |
| Transfer, ALS | 137 (38.9) | 141 (97.9) | <0.001 |
| On-scene vital signs | |||
| RR, breaths/min | 16 (14–20) | 16 (13–18) | 0.057 |
| SpO2, % | 97 (95–98) | 96 (94–98) | 0.001 |
| SBP, mmHg | 145 (125–170) | 140 (115–165) | 0.006 |
| DBP, mmHg | 82 (70–95) | 80 (67–99) | 0.248 |
| Heart rate, beats/min | 78 (67–95) | 77 (60–96) | 0.803 |
| Temperature, °C | 36.1 (35.8–36.5) | 36 (35.8–36.4) | 0.132 |
| Glasgow coma scale, points | 15 (15–15) | 15 (15–15) | 0.186 |
| Baseline cardiac rhythm | |||
| Sinus | 206 (58.5) | 85 (59) | 0.758 |
| Tachycardiac 3 | 111 (31.5) | 38 (26.4) | |
| Bradycardiad 4 | 26 (7.4) | 20 (13.9) | |
| Pacemaker | 9 (2.6) | 1 (0.7) | |
| ST elevation | 12 (3.4) | 101 (70.1) | <0.001 |
| Cardiac biomarkers | |||
| Troponin T, ng/L | 0 (0–58) | 180 (57–431) | <0.001 |
| NT-proBNP, pg/mL | 201 (0–702) | 432 (199–1612) | 0.001 |
| D-dimer, microg/mL | 331 (199–751) | 469 (293–753) | 0.069 |
| Support on-scene | |||
| Mechanical ventilation | 4 (1.1) | 19 (13.2) | <0.001 |
| Defibrillation | 1 (0.3) | 13 (9) | <0.001 |
| Cardioversion | 7 (2) | 4 (2.8) | 0.589 |
| Transcutaneous pacemaker | 3 (0.9) | 6 (4.2) | 0.012 |
| Vasoactive agents | 7 (2) | 18 (12.5) | <0.001 |
| Hospital outcome | |||
| ACCI, points | 2 (1–4) | 2 (1–3) | 0.021 |
| Inpatient | 163 (46.3) | 138 (95.8) | <0.001 |
| Hospitalization time, days | 1 (0–6) | 5 (3–8) | 0.011 |
| Fibrinolysis | 8 (2.3) | 9 (6.3) | 0.027 |
| PCI | 76 (21.6) | 117 (81.3) | <0.001 |
| ECS | 5 (1.4) | 4 (2.8) | 0.305 |
| Mechanical ventilation | 15 (4.3) | 26 (18.1) | <0.001 |
| Vasoactive agents | 18 (5.1) | 31 (21.5) | <0.001 |
| ICU-admission | 70 (19.9) | 124 (86.1) | <0.001 |
| Variables | 0 | 1 | 2 |
|---|---|---|---|
| Troponin T, ng/L | ≤39 | 40–139 | ≥140 |
| NT-proBNP, pg/mL | ≤999 | ≥1000 | |
| D-dimer, microg/mL | ≤199 | 200–999 | ≥1000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zalama-Sánchez, D.; Martín-Rodríguez, F.; López-Izquierdo, R.; Benito, J.F.D.; Soberón, I.S.; Vegas, C.d.P.; Sanz-García, A. Prehospital Targeting of 1-Year Mortality in Acute Chest Pain by Cardiac Biomarkers. Diagnostics 2023, 13, 3681. https://doi.org/10.3390/diagnostics13243681
Zalama-Sánchez D, Martín-Rodríguez F, López-Izquierdo R, Benito JFD, Soberón IS, Vegas CdP, Sanz-García A. Prehospital Targeting of 1-Year Mortality in Acute Chest Pain by Cardiac Biomarkers. Diagnostics. 2023; 13(24):3681. https://doi.org/10.3390/diagnostics13243681
Chicago/Turabian StyleZalama-Sánchez, Daniel, Francisco Martín-Rodríguez, Raúl López-Izquierdo, Juan F. Delgado Benito, Irene Sánchez Soberón, Carlos del Pozo Vegas, and Ancor Sanz-García. 2023. "Prehospital Targeting of 1-Year Mortality in Acute Chest Pain by Cardiac Biomarkers" Diagnostics 13, no. 24: 3681. https://doi.org/10.3390/diagnostics13243681
APA StyleZalama-Sánchez, D., Martín-Rodríguez, F., López-Izquierdo, R., Benito, J. F. D., Soberón, I. S., Vegas, C. d. P., & Sanz-García, A. (2023). Prehospital Targeting of 1-Year Mortality in Acute Chest Pain by Cardiac Biomarkers. Diagnostics, 13(24), 3681. https://doi.org/10.3390/diagnostics13243681