
Plasma 25-Hydroxyvitamin D and 1,25-Dihydroxyvitamin D Levels in Breast Cancer Risk in Mali: A Case–Control Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Samples Collection
2.3. Analysis of Vitamin D Metabolites
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinico-Pathological Characteristics of the Study Population
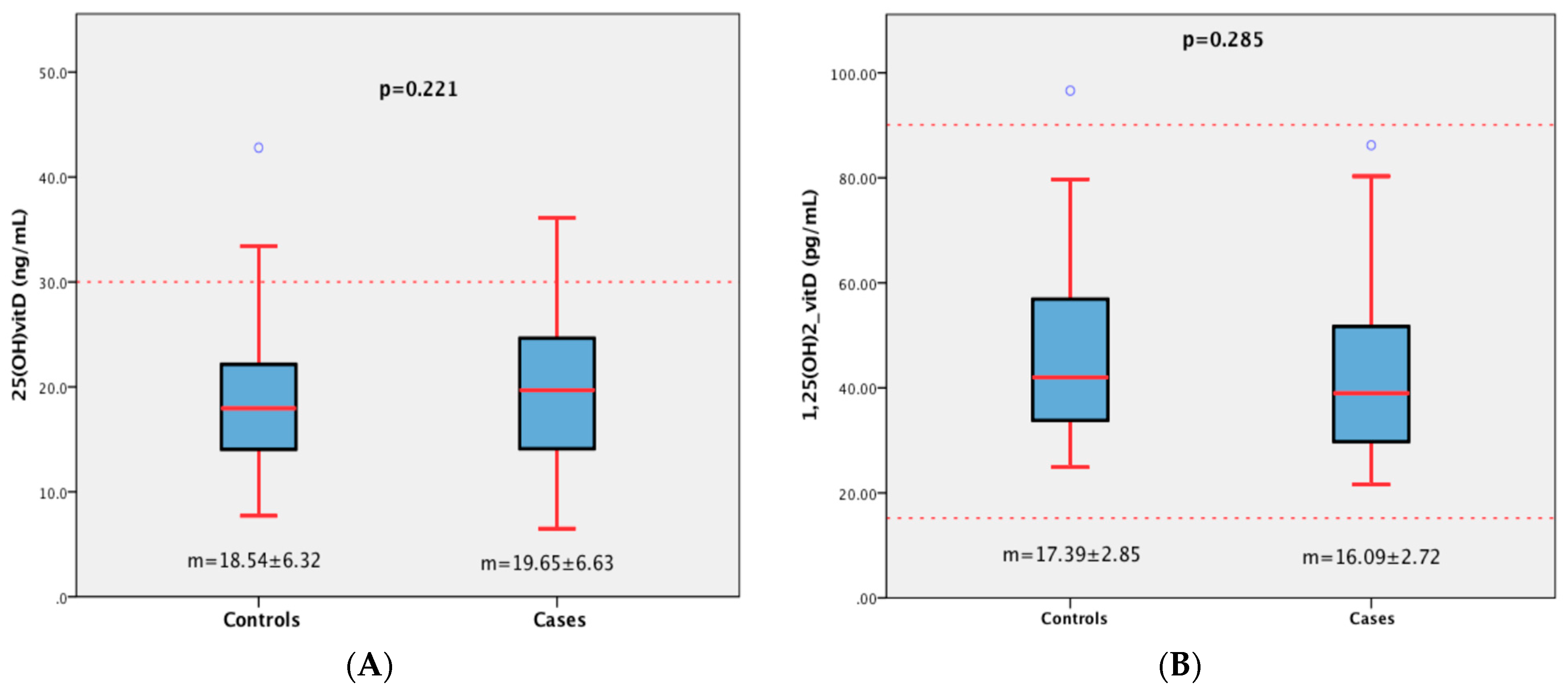
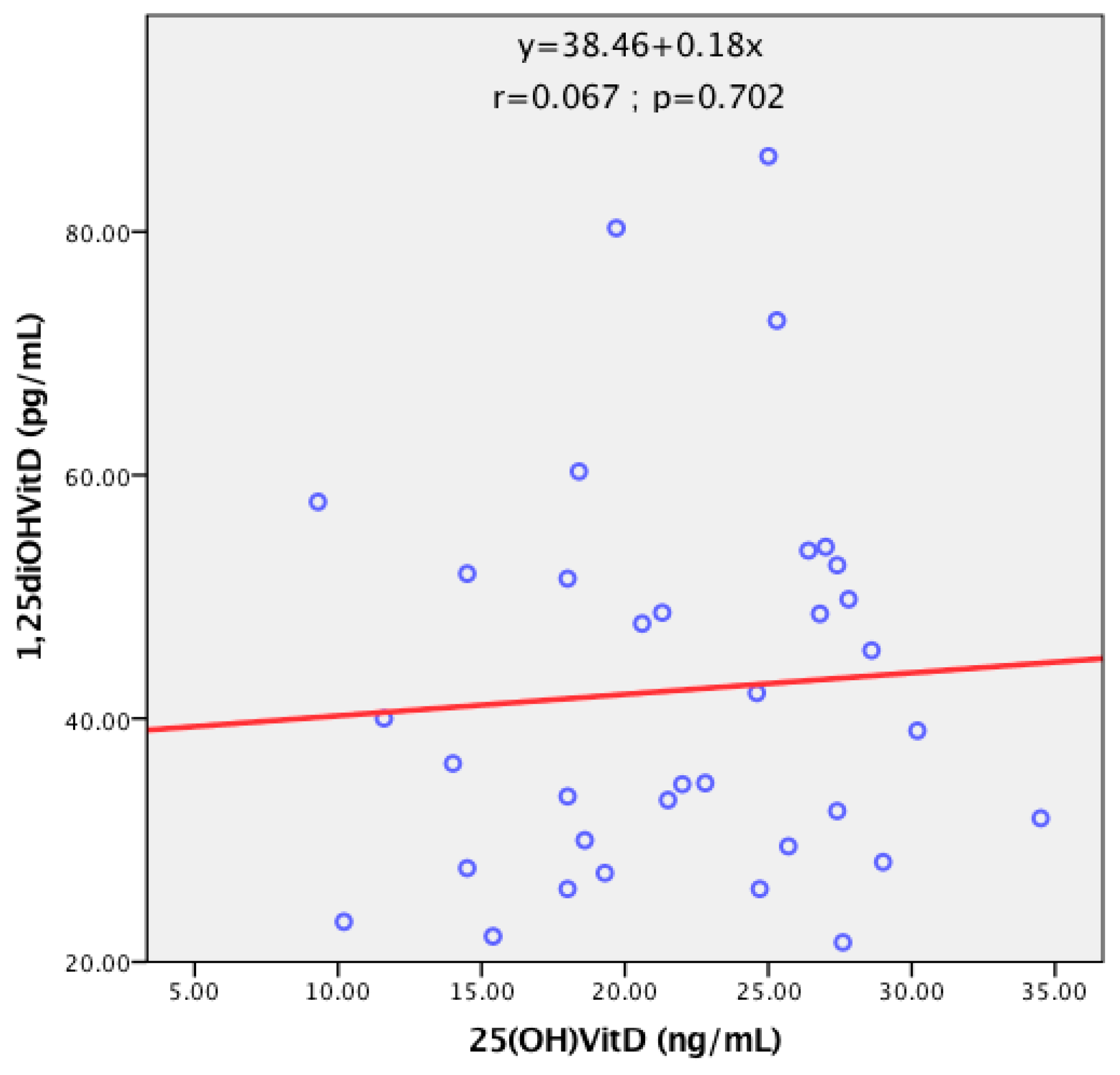
3.2. Vitamin D Metabolite Levels in Breast Cancer Patients
3.3. Vitamin D Metabolites and Breast Cancer Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sancho-Garnier, H.; Colonna, M. Épidémiologie des cancers du sein. La Presse Médicale 2019, 48, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Zaki, H.M.; Garba-Bouda, O.; Garba, S.M.; Nouhou, H. Profil Épidémiologique et Anatomopathologique Du Cancer Du Sein Au Niger. J. Afr. Du Cancer/Afr. J. Cancer 2013, 5, 185–191. [Google Scholar] [CrossRef]
- Mali Source Globocan 2020. International Agency for Research on Cancer; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Jeon, S.-M.; Shin, E.-A. Exploring Vitamin D Metabolism and Function in Cancer. Exp. Mol. Med. 2018, 50, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Christakos, S.; Li, S.; De La Cruz, J.; Bikle, D.D. New Developments in Our Understanding of Vitamin Metabolism, Action and Treatment. Metabolism 2019, 98, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef]
- Vanhevel, J.; Verlinden, L.; Doms, S.; Wildiers, H.; Verstuyf, A. The Role of Vitamin D in Breast Cancer Risk and Progression. Endocr.-Relat. Cancer 2022, 29, R33–R55. [Google Scholar] [CrossRef] [PubMed]
- Voutsadakis, I.A. Vitamin D Receptor (VDR) and Metabolizing Enzymes CYP27B1 and CYP24A1 in Breast Cancer. Mol. Biol. Rep. 2020, 47, 9821–9830. [Google Scholar] [CrossRef]
- Bertrand, K.A.; Rosner, B.; Eliassen, A.H.; Hankinson, S.E.; Rexrode, K.M.; Willett, W.; Tamimi, R.M. Premenopausal Plasma 25-Hydroxyvitamin D, Mammographic Density, and Risk of Breast Cancer. Breast Cancer Res. Treat. 2015, 149, 479–487. [Google Scholar] [CrossRef]
- Hossain, S.; Beydoun, M.A.; Beydoun, H.A.; Chen, X.; Zonderman, A.B.; Wood, R.J. Vitamin D and Breast Cancer: A Systematic Review and Meta-Analysis of Observational Studies. Clin. Nutr. ESPEN 2019, 30, 170–184. [Google Scholar] [CrossRef]
- Ma, H.; Lin, H.; Hu, Y.; Li, X.; He, W.; Jin, X.; Gao, J.; Zhao, N.; Liu, Z.; Gao, X. Serum 25-Hydroxyvitamin D Levels Are Associated with Carotid Atherosclerosis in Normotensive and Euglycemic Chinese Postmenopausal Women: The Shanghai Changfeng Study. BMC Cardiovasc. Disord. 2014, 14, 197. [Google Scholar] [CrossRef]
- Chen, P.; Hu, P.; Xie, D.; Qin, Y.; Wang, F.; Wang, H. Meta-Analysis of Vitamin D, Calcium and the Prevention of Breast Cancer. Breast Cancer Res. Treat. 2010, 121, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Boniol, M.; Haukka, J.; Byrnes, G.; Cox, B.; Sneyd, M.J.; Mullie, P.; Autier, P. Meta-Analysis of Observational Studies of Serum 25-Hydroxyvitamin D Levels and Colorectal, Breast and Prostate Cancer and Colorectal Adenoma. Int. J. Cancer 2011, 128, 1414–1424. [Google Scholar] [CrossRef] [PubMed]
- Hemida, M.A.; AbdElmoneim, N.A.; Hewala, T.I.; Rashad, M.M.; Abdaallah, S. Vitamin D Receptor in Breast Cancer Tissues and Its Relation to Estrogen Receptor Alpha (ER-α) Gene Expression and Serum 25-Hydroxyvitamin D Levels in Egyptian Breast Cancer Patients: A Case-Control Study. Clin. Breast Cancer 2019, 19, e407–e414. [Google Scholar] [CrossRef]
- Husain, N.; Suliman, A.; Abdelrahman, I.; Bedri, S.; Musa, R.; Osman, H.; Mustafa, A.; Gafer, N.; Farah, E.; Satir, A.; et al. Serum Vitamin D Level, Sun-Exposed Area, Dietary Factors, and Physical Activity as Predictors of Invasive Breast Cancer Risk among Sudanese Women: A Case–Control Study. J. Fam. Med. Prim. Care 2019, 8, 1706. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.R.; Patel, K.D.; Patel, K.R.; Gokani, R.A.; Patel, J.B.; Patel, P.S.; Shah, F.D. Clinical Significance of Serum 25 Hydroxyvitamin D in Breast Cancer: An Indian Scenario. J. Steroid Biochem. Mol. Biol. 2020, 202, 105726. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.; Ambrosone, C.B. Associations between Vitamin D Deficiency and Risk of Aggressive Breast Cancer in African-American Women. J. Steroid Biochem. Mol. Biol. 2013, 136, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Janowsky, E.C.; Lester, G.E.; Weinberg, C.R.; Millikan, R.C.; Schildkraut, J.M.; Garrett, P.A.; Hulka, B.S. Association between Low Levels of 1,25-Dihydroxyvitamin D and Breast Cancer Risk. Public Health Nutr. 1999, 2, 283–291. [Google Scholar] [CrossRef]
- Chauveau, P.; Aparicio, M. Ethnicité et vitamine D. Néphrologie Thérapeutique 2013, 9, 398–402. [Google Scholar] [CrossRef]
- Moukal, A.; El Farouqi, A.; Aghrouch, M.; Chadli, S.; Zekhnini, A.; Izaabel, E.H. Serum 25-Hydroxyvitamin D and the Risk of Breast Cancer in Women from Southern Morocco: A Case-Control Study. MNM 2022, 15, 361–368. [Google Scholar] [CrossRef]
- Zhu, H.; Doğan, B.E. American Joint Committee on Cancer’s Staging System for Breast Cancer, Eighth Edition: Summary for Clinicians. Eur. J. Breast Health 2021, 17, 234–238. [Google Scholar] [CrossRef]
- de La Puente-Yagüe, M.; Cuadrado-Cenzual, M.A.; Ciudad-Cabañas, M.J.; Hernández-Cabria, M.; Collado-Yurrita, L. Vitamin D: And Its Role in Breast Cancer. Kaohsiung J. Med. Sci. 2018, 34, 423–427. [Google Scholar] [CrossRef]
- Narvaez, C.J.; Matthews, D.; LaPorta, E.; Simmons, K.M.; Beaudin, S.; Welsh, J. The Impact of Vitamin D in Breast Cancer: Genomics, Pathways, Metabolism. Front. Physiol. 2014, 5, 213. [Google Scholar] [CrossRef]
- de Lyra, E.C.; da Silva, I.A.; Katayama, M.L.H.; Brentani, M.M.; Nonogaki, S.; Góes, J.C.S.; Folgueira, M.A.A.K. 25(OH)D3 and 1,25(OH)2D3 Serum Concentration and Breast Tissue Expression of 1alpha-Hydroxylase, 24-Hydroxylase and Vitamin D Receptor in Women with and without Breast Cancer. J. Steroid Biochem. Mol. Biol. 2006, 100, 184–192. [Google Scholar] [CrossRef]
- Eliassen, A.H.; Spiegelman, D.; Hollis, B.W.; Horst, R.L.; Willett, W.C.; Hankinson, S.E. Plasma 25-Hydroxyvitamin D and Risk of Breast Cancer in the Nurses’ Health Study II. Breast Cancer Res. 2011, 13, R50. [Google Scholar] [CrossRef]
- Abboud, S.F.; Saleh, B.O.; Ahmed, S.J.; Al Mussawi, K.K. Association between vitamin d receptor gene taqi (731236) polymorphisms and breast cancer risk in iraqi women. Biochem. Cell. Arch. 2022, 3713–3718. [Google Scholar] [CrossRef]
- Khedr, M.I.; Sharaf, S.A.F.; Aal, A.N.A.; Dessouky, I.S.; Soliman, M. Serum 25-Hydroxyvitamin D Level and Breast Cancer Risk in Egyptian Females. Asian J. Oncol. 2022, 8, 76–80. [Google Scholar] [CrossRef]
- Bertone-Johnson, E.R.; Chen, W.Y.; Holick, M.F.; Hollis, B.W.; Colditz, G.A.; Willett, W.C.; Hankinson, S.E. Plasma 25-Hydroxyvitamin D and 1,25-Dihydroxyvitamin D and Risk of Breast Cancer. Cancer Epidemiol. Biomarkers Prev. 2005, 14, 1991–1997. [Google Scholar] [CrossRef]
- Freedman, D.M.; Chang, S.-C.; Falk, R.T.; Purdue, M.P.; Huang, W.-Y.; McCarty, C.A.; Hollis, B.W.; Graubard, B.I.; Berg, C.D.; Ziegler, R.G. Serum Levels of Vitamin D Metabolites and Breast Cancer Risk in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Cancer Epidemiol. Biomark. Prev. 2008, 17, 889–894. [Google Scholar] [CrossRef]
- Hiatt, R.A.; Krieger, N.; Lobaugh, B.; Drezner, M.K.; Vogelman, J.H.; Orentreich, N. Prediagnostic Serum Vitamin D and Breast Cancer. JNCI J. Natl. Cancer Inst. 1998, 90, 461–463. [Google Scholar] [CrossRef]
- LaPorta, E.; Welsh, J. Modeling Vitamin D Actions in Triple Negative/Basal-like Breast Cancer. J. Steroid Biochem. Mol. Biol. 2014, 144, 65–73. [Google Scholar] [CrossRef]
- Zheng, Y.; Trivedi, T.; Lin, R.C.; Fong-Yee, C.; Nolte, R.; Manibo, J.; Chen, Y.; Hossain, M.; Horas, K.; Dunstan, C.; et al. Loss of the Vitamin D Receptor in Human Breast and Prostate Cancers Strongly Induces Cell Apoptosis through Downregulation of Wnt/β-Catenin Signaling. Bone Res. 2017, 5, 17023. [Google Scholar] [CrossRef]
- Bertone-Johnson, E.R. Vitamin D and Breast Cancer. Ann. Epidemiol. 2009, 19, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Welsh, J.; Wietzke, J.A.; Zinser, G.M.; Byrne, B.; Smith, K.; Narvaez, C.J. Vitamin D-3 Receptor as a Target for Breast Cancer Prevention. J. Nutr. 2003, 133, 2425S–2433S. [Google Scholar] [CrossRef] [PubMed]
- Stoll, F.; Akladios, C.Y.; Mathelin, C. Vitamine D et cancer du sein: Y a-t-il un lien? Gynécologie Obs. Fertil. 2013, 41, 242–250. [Google Scholar] [CrossRef]
- Lopes, N.; Sousa, B.; Martins, D.; Gomes, M.; Vieira, D.; Veronese, L.A.; Milanezi, F.; Paredes, J.; Costa, J.L.; Schmitt, F. Alterations in Vitamin D Signalling and Metabolic Pathways in Breast Cancer Progression: A Study of VDR, CYP27B1 and CYP24A1 Expression in Benign and Malignant Breast Lesions Vitamin D Pathways Unbalanced in Breast Lesions. BMC Cancer 2010, 10, 483. [Google Scholar] [CrossRef]
- Welsh, J. Function of the Vitamin D Endocrine System in Mammary Gland and Breast Cancer. Mol. Cell. Endocrinol. 2017, 453, 88–95. [Google Scholar] [CrossRef]
- Murray, A.; Madden, S.F.; Synnott, N.C.; Klinger, R.; O’Connor, D.; O’Donovan, N.; Gallagher, W.; Crown, J.; Duffy, M.J. Vitamin D Receptor as a Target for Breast Cancer Therapy. Endocr. Relat. Cancer 2017, 24, 181–195. [Google Scholar] [CrossRef]
- Francis, I.; AlAbdali, N.; Kapila, K.; John, B.; Al-Temaimi, R.A. Vitamin D Pathway Related Polymorphisms and Vitamin D Receptor Expression in Breast Cancer. Int. J. Vitam. Nutr. Res. 2019, 91, 124–132. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Cases (n = 104) | Controls (n = 104) | p-Value | |
|---|---|---|---|---|
| Age (y *), mean ± SD ** | 48.09 ± 12.42 | 47.79 ± 12.42 | 0.863 | |
| Age at menarche (y), mean ± SD | 14.32 ± 1.52 | 14.23 ± 1.35 | 0.715 | |
| First pregnancy age (y), mean ± SD | 20.16 ± 4.12 | 22.56 ± 4.96 | 0.001 | |
| BMI *** (kg/m2), mean ± SD | 26.39 ± 6.15 | 28.35 ± 6.21 | 0.024 | |
| Parity, mean ± SD | 5.53 ± 2.93 | 3.01 ± 2.13 | <10−3 | |
| Months of breastfeeding, mean ± SD | 20.41 ± 8.76 | 15.92 ± 8.05 | <10−3 | |
| Sleep time (hours) | 7.17 ± 1.19 | 6.90 ± 1.61 | 0.172 | |
| Sun exposure time (hours) | 2.48 ± 0.62 | 1.80 ± 0.80 | <10−3 | |
| Residence | Urban, n (%) | 67 (64.40) | 99 (95.20) | <10−3 |
| Rural, n (%) | 37 (35.60) | 5 (4.80) | ||
| Menopausal status | Menopausal women, n (%) | 52 (50) | 52 (50) | 1 |
| Premenopausal women, n (%) | 52 (50) | 52 (50) | ||
| Use of oral contraceptives | Yes, n (%) | 29 (27.90) | 51 (49) | 0.002 |
| No, n (%) | 75 (72.10) | 53 (51) | ||
| Menstrual cycle | Regular, n (%) | 90 (86.50) | 84 (80.80) | 0.261 |
| Irregular, n (%) | 14 (13.5) | 20 (19.20) | ||
| Smoking status | Current, n (%) | 37 (35.60) | 22 (21.20) | 0.176 |
| Never, n (%) | 67 (64.40) | 82 (78.80) | ||
| Professional status | Cleaning lady, n (%) | 64 (61.53) | 48 (46.15) | <10−3 |
| Entrepreneur, n (%) | 25 (24.03) | 28 (26.92) | ||
| State official, n (%) | 9 (8.65) | 11 (10.57) | ||
| Student, n (%) | 0 (0) | 2 (1.92) | ||
| Retiree, n (%) | 4 (3.84) | 11 (10.57) | ||
| Health official, n (%) | 2 (1.92) | 4 (3.84) | ||
| Socioeconomic status **** | High, n (%) | 10 (9.60) | 24 (23.10) | <10−3 |
| Moderate, n (%) | 21 (20.20) | 60 (57.70) | ||
| Low, n (%) | 73 (70.20) | 20 (19.20) | ||
| Education | Uneducated, n (%) | 77 (74) | 14 (13.50) | <10−3 |
| High school, n (%) | 9 (8.70) | 18 (17.30) | ||
| College graduate, n (%) | 6 (5.80) | 10 (9.60) | ||
| University, n (%) | 12 (11.50) | 62 (59.6) | ||
| Family history of cancer | Yes, n (%) | 13 (12.50) | 23 (22.10) | 0.049 |
| No, n (%) | 91 (87.50) | 81 (77.90) | ||
| Past abortion | Yes, n (%) | 47 (45.20) | 52 (50) | 0.277 |
| No, n (%) | 57 (54.80) | 52 (50) | ||
| Dress habits ***** | Loincloth and scarf set, n (%) | 88 (84.51) | 87 (83.65) | 0.569 |
| Hijab set, n (%) | 16 (15.39) | 17 (16.35) | ||
| Diet | Yes, n (%) | 79 (75.90) | 33 (31.70) | <10−3 |
| No, n (%) | 25 (24.10) | 71 (68.30) | ||
| Dairy products | At least once a day, n (%) | 55 (52.88) | 61 (58.65) | 0.248 |
| Sometimes, n (%) | 12 (11.50) | 14 (13.50) | ||
| Rarely, n (%) | 37 (35.6) | 25 (24) | ||
| Never, n (%) | 0 | 4 (3.80) | ||
| Meat consumption | At least once a day, n (%) | 87 (83.65) | 70 (67.30) | 0.059 |
| Sometimes, n (%) | 11 (10.60) | 22 (21.20) | ||
| Rarely, n (%) | 16 (15.80) | 11 (10.60) | ||
| Never, n (%) | 0 | 1 (1.00) | ||
| Fish consumption | At least once a day, n (%) | 84 (80.76) | 81 (77.88) | 0.892 |
| Sometimes, n (%) | 17 (16.30) | 18 (17.30) | ||
| Rarely, n (%) | 3 (2.90) | 5 (4.80) | ||
| Fruit consumption | At least once a day, n (%) | 86 (82.69) | 81 (77.88) | 0.044 |
| Sometimes, n (%) | 12 (11.50) | 16 (15.40) | ||
| Rarely, n (%) | 6 (5.80) | 7 (6.70) | ||
| Physical activity | Yes, n (%) | 100 (96.15) | 104 (100) | 0.043 |
| No, n (%) | 4 (3.80) | 0 (0.00) | ||
| Tumour grade | T1, n (%) | 2 (2.10) | ||
| T2, n (%) | 11 (11.7) | |||
| T3, n (%) | 17 (18.10) | |||
| T4, n (%) | 64 (68.10) | |||
| Nodal status | N0, n (%) | 12 (12.80) | ||
| N1, n (%) | 63 (67.00) | |||
| N2, n (%) | 16 (17.00) | |||
| N3, n (%) | 3 (2.60) | |||
| Metastasis | M0, n (%) | 69 (73.40) | ||
| M1, n (%) | 25 (26.60) | |||
| Clinical stage | I, n (%) | 2 (2.10) | ||
| II, n (%) | 15 (16.00) | |||
| III, n (%) | 52 (55.30) | |||
| IV, n (%) | 25 (26.60) | |||
| Study Cohort | p | |||
|---|---|---|---|---|
| Cases | Controls | |||
| Plasma 25(OH)D | Deficient, n (%) | 54 (51.9) | 65 (62.5) | 0.303 |
| Insufficient, n (%) | 44 (42.3) | 34 (32.7) | ||
| Normal, n (%) | 6 (5.8) | 5 (4.8) | ||
| Plasma 1,25(OH)2D | Normal, n (%) | 35 (100) | 34 (97.3) | 0.327 |
| Low, n (%) | 0 (0) | 1 (2.7) | ||
| High, n (%) | 0 (0) | 0 (0) | ||
| 25(OH)D | 1,25(OH)2D | ||
|---|---|---|---|
| Clinical Stages I and II | (n = 17) 17.10 ± 6.50 1 | (n = 6) 34.95 ± 12.53 2 | |
| Clinical Stages III and IV | (n = 77) 20.08 ± 6.57 1 | (n = 29) 43.84 ± 16.50 2 | |
| Metastasis | No | (n = 69) 19.71 ± 6.77 3 | (n = 25) 42.99 ± 17.79 4 |
| Yes | (n = 25) 18.89 ± 6.12 3 | (n = 10) 39.62 ± 11.60 4 | |
| p-Value | OR 2 | 95% CI 3 | ||
|---|---|---|---|---|
| Lower | Upper | |||
| 25(OH)D (n = 208) * | 0.13 | 1.08 | 0.98 | 1.18 |
| Q 11 (<14.10 ng/mL) | 0.25 | 0.40 | 0.08 | 1.91 |
| Q2 (14.10–18.84 ng/mL) | 0.16 | 0.32 | 0.06 | 1.60 |
| Q3 (18.85–23.51 ng/mL) | 0.23 | 0.38 | 0.08 | 1.80 |
| Q4 (≥23.52 ng/mL) | 1.00 | |||
| 1,25(OH)2D (n = 70) ** | 0.18 | 0.97 | 0.92 | 1.02 |
| Q1 (<31.92 pg/mL) | 0.03 | 71.84 | 1.36 | 3785.34 |
| Q2 (31.92–39.79 pg/mL) | 0.98 | 0.96 | 0.07 | 14.28 |
| Q3 (39.80–54.01 pg/mL) | 0.98 | 0.96 | 0.05 | 19.50 |
| Q4 (≥54.02 pg/mL) | 1.00 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bissan, A.D.T.; Ly, M.; Amegonou, A.E.H.; Sidibe, F.M.; Koné, B.S.; Barry, N.O.K.; Tall, M.; Timbiné, L.G.; Kouriba, B.; Reynier, P.; et al. Plasma 25-Hydroxyvitamin D and 1,25-Dihydroxyvitamin D Levels in Breast Cancer Risk in Mali: A Case–Control Study. Diagnostics 2023, 13, 3664. https://doi.org/10.3390/diagnostics13243664
Bissan ADT, Ly M, Amegonou AEH, Sidibe FM, Koné BS, Barry NOK, Tall M, Timbiné LG, Kouriba B, Reynier P, et al. Plasma 25-Hydroxyvitamin D and 1,25-Dihydroxyvitamin D Levels in Breast Cancer Risk in Mali: A Case–Control Study. Diagnostics. 2023; 13(24):3664. https://doi.org/10.3390/diagnostics13243664
Chicago/Turabian StyleBissan, Aboubacar D. T., Madani Ly, Awo Emmanuela H. Amegonou, Fatoumata M. Sidibe, Bocary S. Koné, Nènè Oumou K. Barry, Madiné Tall, Lassana G. Timbiné, Bourèma Kouriba, Pascal Reynier, and et al. 2023. "Plasma 25-Hydroxyvitamin D and 1,25-Dihydroxyvitamin D Levels in Breast Cancer Risk in Mali: A Case–Control Study" Diagnostics 13, no. 24: 3664. https://doi.org/10.3390/diagnostics13243664
APA StyleBissan, A. D. T., Ly, M., Amegonou, A. E. H., Sidibe, F. M., Koné, B. S., Barry, N. O. K., Tall, M., Timbiné, L. G., Kouriba, B., Reynier, P., & Ouzzif, Z. (2023). Plasma 25-Hydroxyvitamin D and 1,25-Dihydroxyvitamin D Levels in Breast Cancer Risk in Mali: A Case–Control Study. Diagnostics, 13(24), 3664. https://doi.org/10.3390/diagnostics13243664