


The Swedish Standardized Course of Care—Diagnostic Efficacy in Esophageal and Gastric Cancer


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
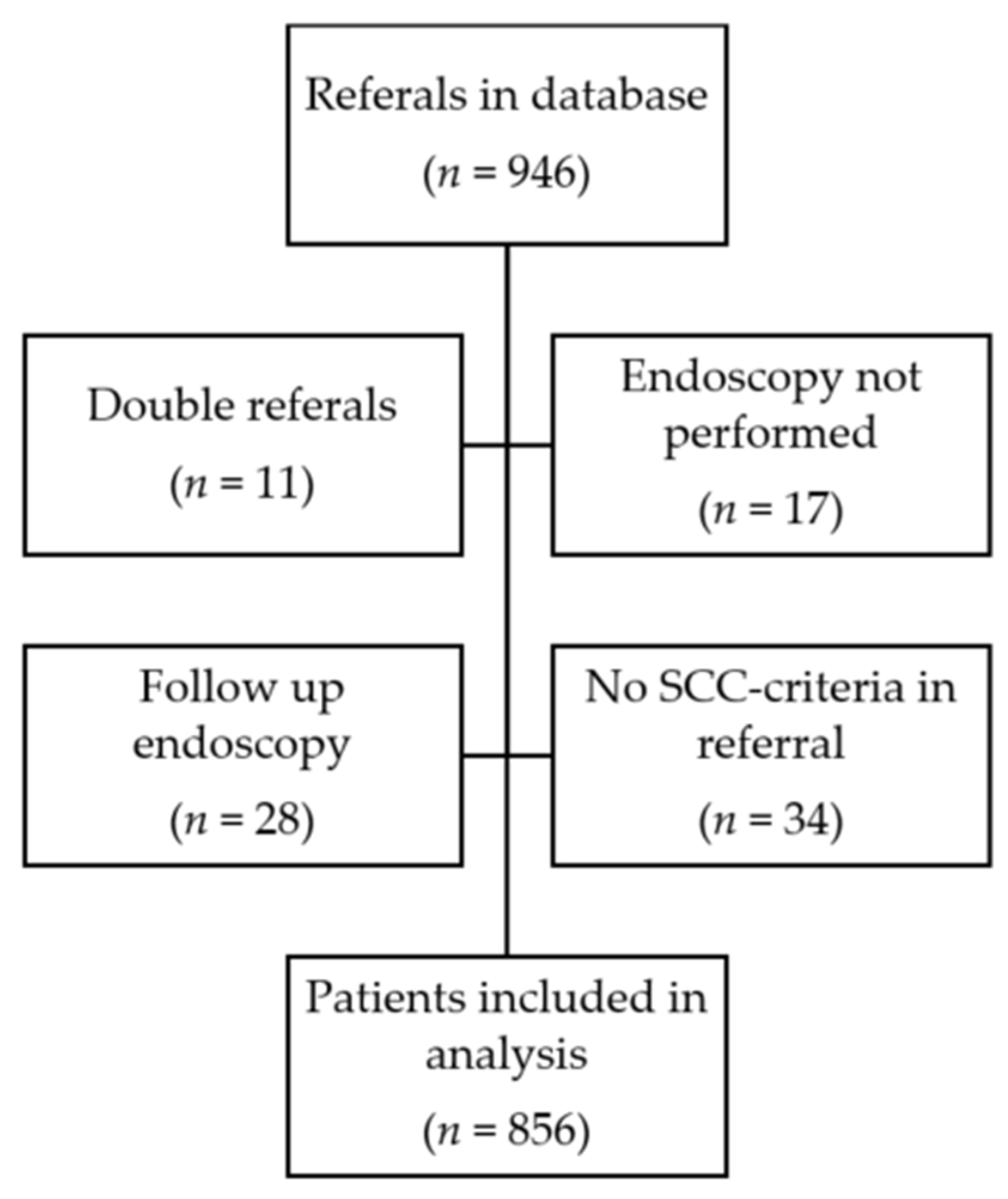
3.1. Patient Inclusion and Characteristics
3.2. Performance of SCC-EGC Criteria
3.3. Referrals to the Department of Surgery
3.4. Waiting Times and Characteristics in SCC and Non-SCC Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, A.L.; O’Byrne, K.; Steward, W.P. Chemotherapy for upper gastrointestinal tumours. Postgrad. Med. J. 2000, 76, 321. [Google Scholar] [CrossRef][Green Version]
- Waddingham, W.; Nieuwenburg, S.A.V.; Carlson, S.; Rodriguez-Justo, M.; Spaander, M.; Kuipers, E.J.; Jansen, M.; Graham, D.G.; Banks, M. Recent advances in the detection and management of early gastric cancer and its precursors. Frontline Gastroenterol. 2020, 12, 322–331. [Google Scholar] [CrossRef]
- Correa, P. Gastric Cancer: Overview. Gastroenterol. Clin. N. Am. 2013, 42, 211–217. [Google Scholar] [CrossRef]
- Rubenstein, J.H.; Shaheen, N.J. Epidemiology, Diagnosis, and Management of Esophageal Adenocarcinoma. Gastroenterology 2015, 149, 302–317.e1. [Google Scholar] [CrossRef]
- Takahashi, T.; Saikawa, Y.; Kitagawa, Y. Gastric Cancer: Current Status of Diagnosis and Treatment. Cancers 2013, 5, 48–63. [Google Scholar] [CrossRef]
- Maharaj, A.D.; Holland, J.F.; O Scarborough, R.; Evans, S.M.; Ioannou, L.J.; Brown, W.; Croagh, D.G.; Pilgrim, C.H.C.; Kench, J.G.; Lipton, L.R.; et al. The Upper Gastrointestinal Cancer Registry (UGICR): A clinical quality registry to monitor and improve care in upper gastrointestinal cancers. BMJ Open 2019, 9, e031434. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2020, 71, 209–249. [Google Scholar] [CrossRef]
- Sharpe, D.; Williams, R.N.; Ubhi, S.S.; Sutton, C.D.; Bowrey, D.J. The “two-week wait” referral pathway allows prompt treatment but does not improve outcome for patients with oesophago-gastric cancer. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2010, 36, 977–981. [Google Scholar] [CrossRef]
- Prades, J.; Espinàs, J.A.; Font, R.; Argimon, J.M.; Borràs, J.M. Implementing a Cancer Fast-track Programme between primary and specialised care in Catalonia (Spain): A mixed methods study. Br. J. Cancer 2011, 105, 753–759. [Google Scholar] [CrossRef]
- Zhou, Y.; Mendonca, S.C.; Abel, G.A.; Hamilton, W.; Walter, F.M.; Johnson, S.; Shelton, J.; Elliss-Brookes, L.; McPhail, S.; Lyratzopoulos, G. Variation in ‘fast-track’ referrals for suspected cancer by patient characteristic and cancer diagnosis: Evidence from 670,000 patients with cancers of 35 different sites. Br. J. Cancer 2018, 118, 24–31. [Google Scholar] [CrossRef]
- Standardiserade Vårdförlopp i Cancervården—Lägesrapport 2015. Socialstyrelsen 2015. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2015-11-6.pdf (accessed on 29 October 2023).
- Alarms Symptoms and Fast-Track Access Services—An Update of SBU Report 2014:222. 2014. Available online: https://www.regionorebrolan.se/contentassets/c7e22cd5393c42a996aac93759bfebc6/rapporter-2020/2020.34-snabbspar-for-alarmsymtom-och-tidig-upptackt-av-symtomgivande-cancer.pdf (accessed on 29 October 2023).
- Fallon, M.; Adil, M.T.; Ahmed, K.; Whitelaw, D.; Rashid, F.; Jambulingam, P. Impact of “two-week wait” referral pathway on the diagnosis, treatment and survival in upper and lower gastrointestinal cancers. Postgrad. Med. J. 2019, 95, 470–475. [Google Scholar] [CrossRef]
- Cavallin, F.; Scarpa, M.; Cagol, M.; Alfieri, R.; Ruol, A.; Sileni, V.C.; Rugge, M.; Ancona, E.; Castoro, C. Time to diagnosis in esophageal cancer: A cohort study. Acta Oncol. 2018, 57, 1179–1184. [Google Scholar] [CrossRef]
- Pasechnikov, V.; Chukov, S.; Fedorov, E.; Kikuste, I.; Leja, M. Gastric cancer: Prevention, screening and early diagnosis. World J. Gastroenterol. WJG 2014, 20, 13842–13862. [Google Scholar] [CrossRef]
- Berrill, J.W.; Turner, J.K.; Hurley, J.J.; Swift, G.; Dolwani, S.; Green, J.T. Upper gastrointestinal cancer in its early stages is predominantly asymptomatic. Frontline Gastroenterol. 2012, 3, 47–51. [Google Scholar] [CrossRef]
- Maconi, G.; Manes, G.; Porro, G.B. Role of symptoms in diagnosis and outcome of gastric cancer. World J. Gastroenterol. WJG 2008, 14, 1149–1155. [Google Scholar] [CrossRef]
- Rasmussen, S.; Haastrup, P.F.; Balasubramaniam, K.; Christensen, R.D.; Søndergaard, J.; Jarbøl, D.E. Predictive values of upper gastrointestinal cancer alarm symptoms in the general population: A nationwide cohort study. BMC Cancer 2018, 18, 440. [Google Scholar] [CrossRef]
- Lee, A.; Khulusi, S.; Watson, R. Which interval is most crucial to presentation and survival in gastroesophageal cancer: A systematic review. J. Adv. Nurs. 2017, 73, 2270–2282. [Google Scholar] [CrossRef]
- de Jong, J.J.; Lantinga, M.A.; Drenth, J.P. Prevention of overuse: A view on upper gastrointestinal endoscopy. World J. Gastroenterol. 2019, 25, 178–189. [Google Scholar] [CrossRef]
- O’sullivan, J.W.; Albasri, A.; Nicholson, B.D.; Perera, R.; Aronson, J.K.; Roberts, N.; Heneghan, C. Overtesting and undertesting in primary care: A systematic review and meta-analysis. BMJ Open 2018, 8, e018557. [Google Scholar] [CrossRef]
- van Kerkhoven, L.; van Rijswijck, S.; van Rossum, L.; Laheij, R.; Witteman, E.; Tan, A.; Jansen, J. Is there any association between referral indications for open-access upper gastrointestinal endoscopy and endoscopic findings? Endoscopy 2007, 39, 502–506. [Google Scholar] [CrossRef]
- Emami, M.H.; Ataie-Khorasgani, M.; Jafari-Pozve, N. Diagnostic value of alarm symptoms for upper GI malignancy in patients referred to GI clinic: A 7 years cross sectional study. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2017, 22, 76. [Google Scholar]
- Carter, K.; Hutchings, H.; Elwyn, G. The Two-Week Rule for NHS Gastrointestinal Cancer Referrals: A Systematic Review of Diagnostic Effectiveness. Open Color. Cancer J. 2009, 2, 27–33. [Google Scholar]
- Crouwel, F.; Meurs-Szojda, M.M.; Klemt-Kropp, M.; Fockens, P.; Grasman, M.E. The diagnostic yield of open-access endoscopy of the upper gastrointestinal tract in the Netherlands. Endosc. Int. Open 2018, 6, E383–E394. [Google Scholar] [CrossRef]
- Stapley, S.; Peters, T.J.; Neal, R.D.; Rose, P.W.; Walter, F.M.; Hamilton, W. The risk of oesophago-gastric cancer in symptomatic patients in primary care: A large case–control study using electronic records. Br. J. Cancer 2013, 108, 25–31. [Google Scholar] [CrossRef]
- Shapley, M.; Mansell, G.; Jordan, J.L.; Jordan, K.P. Positive predictive values of ≥5% in primary care for cancer: Systematic review. Br. J. Gen. Pract. 2010, 60, e366–e377. [Google Scholar] [CrossRef]
- Carucci, L.R.; Turner, M.A. Dysphagia Revisited: Common and Unusual Causes. RadioGraphics 2015, 35, 105–122. [Google Scholar] [CrossRef]
- Philpott, H.; Garg, M.; Tomic, D.; Balasubramanian, S.; Sweis, R. Dysphagia: Thinking outside the box. World J. Gastroenterol. 2017, 23, 6942–6951. [Google Scholar] [CrossRef]
- Fransen, G.A.J.; Janssen, M.J.R.; Muris, J.W.M.; Laheij, R.J.F.; Jansen, J.B.M.J. Meta-analysis: The diagnostic value of alarm symptoms for upper gastrointestinal malignancy. Aliment. Pharmacol. Ther. 2004, 20, 1045–1052. [Google Scholar] [CrossRef]
- Astin, M.P.; Martins, T.; Welton, N.; Neal, R.D.; Rose, P.W.; Hamilton, W. Diagnostic value of symptoms of oesophagogastric cancers in primary care: A systematic review and meta-analysis. Br. J. Gen. Pract. 2015, 65, e677–e691. [Google Scholar] [CrossRef]
- Vakil, N.; Moayyedi, P.; Fennerty, M.B.; Talley, N.J. Limited value of alarm features in the diagnosis of upper gastrointestinal malignancy: Systematic review and meta-analysis. Gastroenterology 2006, 131, 390–401. [Google Scholar] [CrossRef]
- Yusefi, A.R.; Lankarani, K.B.; Bastani, P.; Radinmanesh, M.; Kavosi, Z. Risk Factors for Gastric Cancer: A Systematic Review. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 591–603. [Google Scholar] [PubMed]
- Falk, G.W. Risk factors for esophageal cancer development. Surg. Oncol. Clin. N. Am. 2009, 18, 469–485. [Google Scholar] [CrossRef]
- Bird-Lieberman, E.L.; Fitzgerald, R.C. Early diagnosis of oesophageal cancer. Br. J. Cancer 2009, 101, 1–6. [Google Scholar] [CrossRef]
- Matstrups-Och Magsäckscancer. Nationellt Vårdprogram 2022-08-23 Version: 4.0. Available online: https://kunskapsbanken.cancercentrum.se/globalassets/cancerdiagnoser/matstrupe-och-magsack/vardprogram/nationellt-vardprogram-matstrups-magsackscancer.pdf (accessed on 29 October 2023).



{kind=link}
{kind=link}
| Characteristic | No Cancer (n = 803) | Cancer (n = 53) | p-Value |
|---|---|---|---|
| Age, mean (SD) | 67.8 (13.6) | 71.1 (11.6) | 0.145 ^ |
| Waiting time *, days (range) | 12.3 (0–308) | 8.9 (1–54) | 0.005 ^ |
| Sex—male, n (%) | 368 (45.8) | 33 (62.3) | 0.020 |
| Smoking status | |||
| Current, n (%) | 89 (11.1) | 8 (15.1) | 0.372 |
| Past, n (%) | 105 (13.1) | 12 (22.1) | 0.050 |
| Alcohol | |||
| Current, n (%) | 29 (3.6) | 3 (5.7) | 0.442 |
| Past, n (%) | 9 (1.1) | 1 (1.9) | 0.474 |
| BMI ≥ 30, n (%) | 173 (21.5) | 13 (24.5) | 0.610 |
| Factors in Referral | No Cancer (n = 803) (%) | Cancer (n = 53) (%) | PPV, % | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Sex—male | 368 (45.8) | 33 (62.3) | 8.2 | 1.95 (1.10–3.46) | 0.020 |
| Age ≥ 50 | 723 (90.0) | 51 (96.2) | 6.6 | 2.82 (0.67–11.81) | 0.138 |
| SCC criteria | |||||
| Recent-onset dysphagia | 329 (41.0) | 19 (35.8) | 5.5 | 0.81 (0.45–1.44) | 0.462 |
| (Esophageal dysphagia) | 220 (27.4) | 13 (24.5) | 5.6 | 0.86 (0.45–1.64) | 0.649 |
| Emesis a | 119 (14.8) | 10 (18.9) | 7.8 | 1.34 (0.65–2.73) | 0.425 |
| Early satiety a | 61 (7.6) | 9 (17.0) | 12.9 | 2.49 (1.16–5.34) | 0.016 |
| Unintentional weight loss a | 283 (35.2) | 27 (50.9) | 8.7 | 1.91 (1.09–3.33) | 0.021 |
| Gastrointestinal bleeding (any) | 192 (23.9) | 5 (9.4) | 2.5 | 0.33 (0.13–0.85) | 0.015 |
| Hematemesis | 15 (1.9) | 1 (1.9) | 6.3 | 1.01 (0.13–7.80) | 0.644 |
| Iron deficiency anemia | 220 (27.4) | 8 (15.1) | 3.5 | 0.47 (0.22–1.02) | 0.050 |
| Radiological findings (esophageal/gastric) | 71 (8.8) | 23 (43.4) | 24.5 | 7.90 (4.36–14.34) | <0.001 |
| (Any radiological finding suggestive of malignancy) | 96 (12.0) | 24 (45.3) | 20.0 | 6.10 (3.41–10.90) | <0.001 |
| Patient Characteristics | SCC (n = 40) | Non-SCC (n = 99) | Missing Cases (%) SCC/Non-SCC | p-Value |
|---|---|---|---|---|
| Male, n (%) | 29 (71.2) | 63 (63.6) | 0.317 | |
| Age (years), mean (SD) | 71.5 (11.8) | 71.2 (10.6) | 0.864 ^^ | |
| Risk factors | ||||
| Smoker, n (%) | 4 (10.0) | 18 (18.2) | 0.232 | |
| Former smoker, n (%) | 11 (27.5) | 21 (21.2) | 0.425 | |
| Obesity, n (%) | 6 (15.0) | 28 (28.3) | 0.099 | |
| Primary care origin of referral, n (%) | 30 (75.0) | 52 (52.5) | 0.015 | |
| Symptom duration (patient delay) | 17.5/25.3 | |||
| <1 month | 13 (38.2) | 30 (40.5) | 0.820 | |
| 1–6 months | 17 (50.0) | 34 (45.9) | 0.695 | |
| >6 months | 3 (8.8) | 10 (13.5) | 0.751 | |
| Diagnostic interval, median (IQR) * | 10 (10) | 16 (36) | 0.045 ^ | |
| ≥1 SCC criteria in referral | 38 (95.0) | 90 (88.9) | 0.347 |
| Signs and Symptoms in Referral | SCC | Non-SCC | p-Value |
|---|---|---|---|
| Dysphagia | 19 (51.4) | 45 (44.1) | 0.450 |
| Emesis | 9 (24.3) | 17 (16.7) | 0.306 |
| Weight loss | 21 (56.8) | 40 (39.2) | 0.065 |
| Early satiety | 7 (18.9) | 3 (2.9) | 0.004 |
| GI bleeding | 4 (10.8) | 17 (16.7) | 0.394 |
| Anemia | 7 (18.9) | 27 (26.5) | 0.360 |
| Abdominal pain/dyspepsia | 10 (27.0) | 45 (44.1) | 0.069 |
| Reflux | 7 (18.9) | 9 (8.8) | 0.131 |
| Altered bowel habits | 1 (2.7) | 6 (5.9) | 0.675 |
| ≥1 Specific alarming upper GI symptom * | 24 (64.9) | 60 (58.8) | 0.520 |
| Cancer Characteristics | SCC (n = 40) | Non-SCC (n = 99) | Missing Cases (%) SCC/Non-SCC | p-Value |
|---|---|---|---|---|
| Primary tumor | 12.5/6.1 | |||
| T1 | 3 (8.6) | 2 (2.2) | 0.125 | |
| T2 | 13 (37.1) | 31 (33.3) | 0.686 | |
| T3 | 13 (37.1) | 39 (41.9) | 0.623 | |
| T4 | 6 (17.1) | 20 (21.5) | 0.585 | |
| Metastasis | 10 (27.0) | 34 (36.2) | 7.5/5.1 | 0.319 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanold, P.; Nyhlin, N.; Szabo, E.; van Nieuwenhoven, M. The Swedish Standardized Course of Care—Diagnostic Efficacy in Esophageal and Gastric Cancer. Diagnostics 2023, 13, 3577. https://doi.org/10.3390/diagnostics13233577
Kanold P, Nyhlin N, Szabo E, van Nieuwenhoven M. The Swedish Standardized Course of Care—Diagnostic Efficacy in Esophageal and Gastric Cancer. Diagnostics. 2023; 13(23):3577. https://doi.org/10.3390/diagnostics13233577
Chicago/Turabian StyleKanold, Philip, Nils Nyhlin, Eva Szabo, and Michiel van Nieuwenhoven. 2023. "The Swedish Standardized Course of Care—Diagnostic Efficacy in Esophageal and Gastric Cancer" Diagnostics 13, no. 23: 3577. https://doi.org/10.3390/diagnostics13233577
APA StyleKanold, P., Nyhlin, N., Szabo, E., & van Nieuwenhoven, M. (2023). The Swedish Standardized Course of Care—Diagnostic Efficacy in Esophageal and Gastric Cancer. Diagnostics, 13(23), 3577. https://doi.org/10.3390/diagnostics13233577