
Determining the Optimal Energy Level of Virtual Monoenergetic Images in Dual-Source CT for Diagnosis of Bowel Obstruction and Colitis


 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Acquisition and Reconstruction Parameters
2.3. Dosimetric Analysis
2.4. Objective Image Quality Assessment
2.5. Subjective Image Quality Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. Dosimetric Analysis
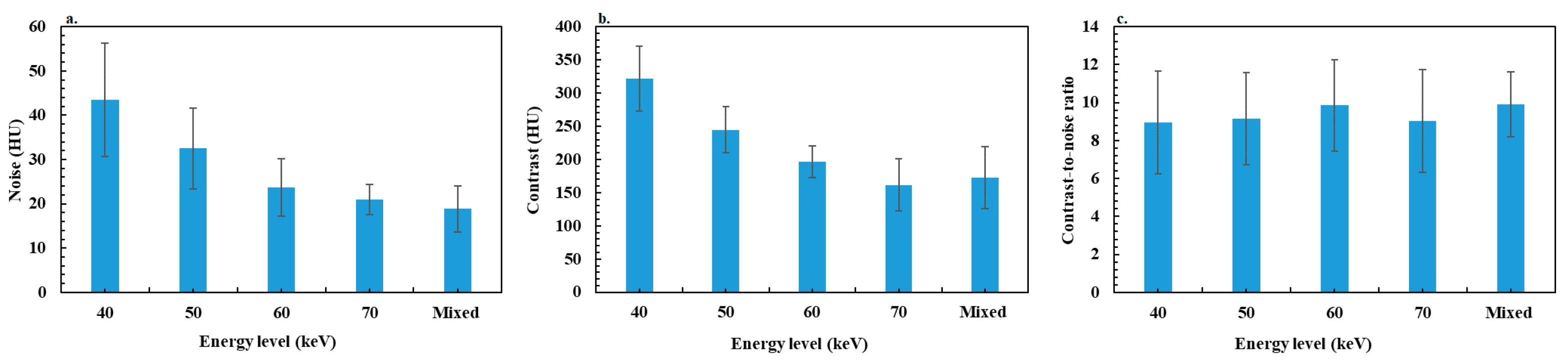
3.3. Objective Image Quality Assessment
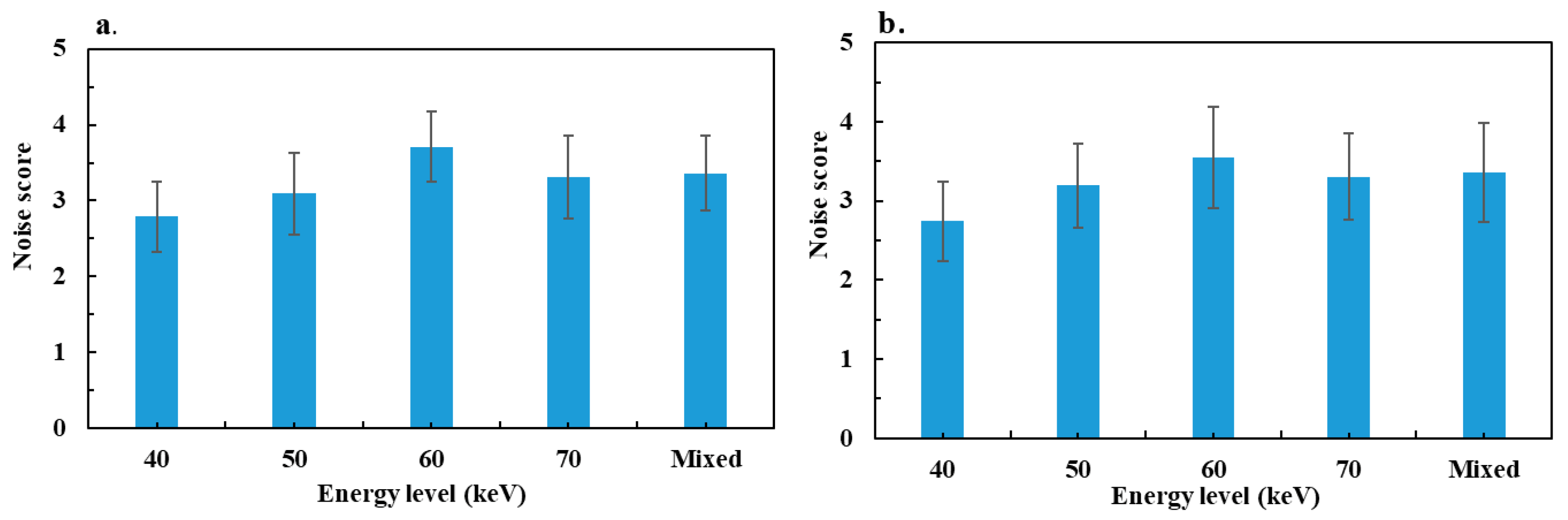
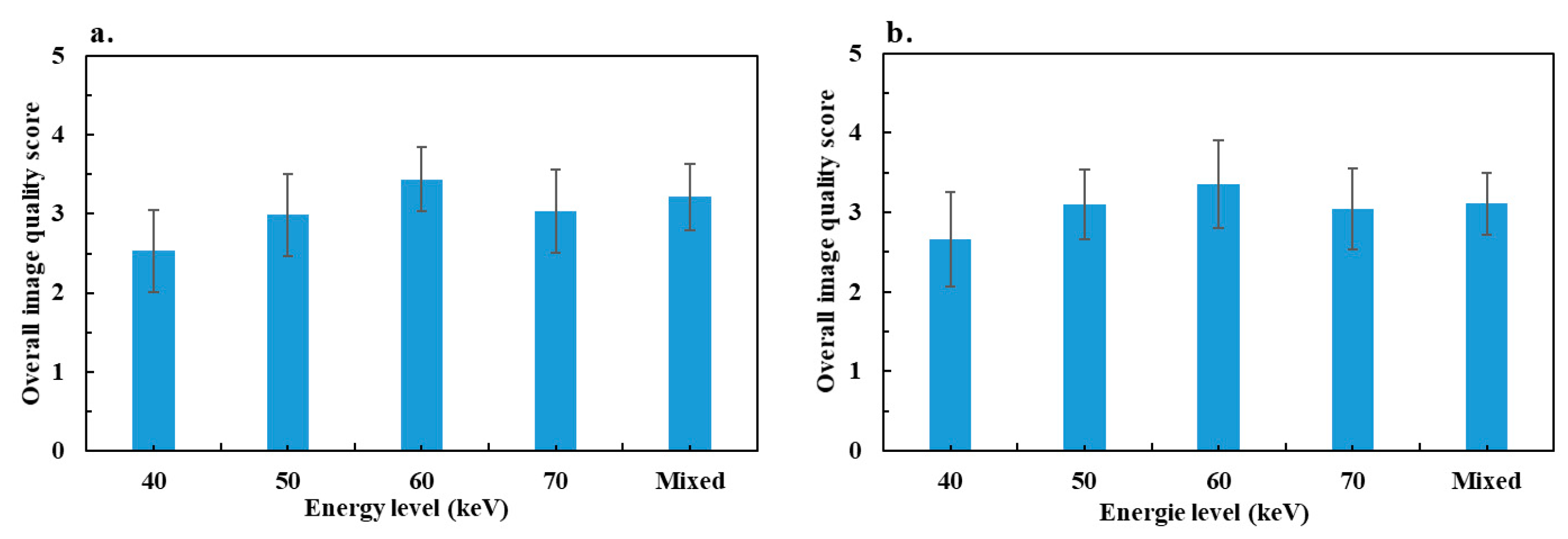
3.4. Subjective Image Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lestra, T.; Mulé, S.; Millet, I.; Carsin-Vu, A.; Taourel, P.; Hoeffel, C. Applications of dual energy computed tomography in abdominal imaging. Diagn. Interv. Imaging 2016, 97, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, M.H.; Vogl, T.J.; Martin, S.S.; Nance, J.W.; Duguay, T.M.; Wichmann, J.L.; De Cecco, C.N.; Varga-Szemes, A.; van Assen, M.; Tesche, C.; et al. Review of Clinical Applications for Virtual Monoenergetic Dual-Energy CT. Radiology 2019, 293, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Adam, S.Z.; Rabinowich, A.; Kessner, R.; Blachar, A. Spectral CT of the abdomen: Where are we now? Insights Into Imaging 2021, 12, 138. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.-W.; Zhou, Y.; Zhang, Z.-W.; Yan, G.-W.; Du, S.-L.; Zhang, X.-H.; Li, X.-Y.; Lv, F.-J.; Zheng, Q.; Li, Y.-M. Dual-energy CT with virtual monoenergetic images to improve the visualization of pancreatic supplying arteries: The normal anatomy and variations. Insights Into Imaging 2022, 13, 21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, G.; Xu, L.; Bai, X.; Lu, X.; Yu, S.; Sun, H.; Jin, Z. Utilisation of virtual non-contrast images and virtual mono-energetic images acquired from dual-layer spectral CT for renal cell carcinoma: Image quality and radiation dose. Insights Into Imaging 2022, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Murray, N.; Darras, K.E.; Walstra, F.E.; Mohammed, M.F.; McLaughlin, P.D.; Nicolaou, S. Dual-Energy CT in Evaluation of the Acute Abdomen. RadioGraphics 2019, 39, 264–286. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Boedeker, K.; Cody, D.; Duan, X.; Flohr, T.; Halliburton, S.S.; Hsieh, J.; Layman, R.R.; Pelc, N.J. Principles and applications of multienergy CT: Report of AAPM Task Group 291. Med. Phys. 2020, 47, E881–E912. [Google Scholar] [CrossRef] [PubMed]
- Greffier, J.; Villani, N.; Defez, D.; Dabli, D.; Si-Mohamed, S. Spectral CT imaging: Technical principles of dual-energy CT and multi-energy photon-counting CT. Diagn. Interv. Imaging 2023, 104, 167–177. [Google Scholar] [CrossRef]
- Dabli, D.; Frandon, J.; Hamard, A.; Belaouni, A.; Addala, T.; Beregi, J.-P.; Greffier, J. Optimization of image quality and accuracy of low iodine concentration quantification as function of kVp pairs for abdominal imaging using dual-source CT: A phantom study. Phys. Medica 2021, 88, 285–292. [Google Scholar] [CrossRef]
- Greffier, J.; Frandon, J.; Sadate, A.; Akessoul, P.; Belaouni, A.; Beregi, J.; Dabli, D. Impact of four kVp combinations available in a dual-source CT on the spectral performance of abdominal imaging: A task-based image quality assessment on phantom data. J. Appl. Clin. Med. Phys. 2021, 22, 243–254. [Google Scholar] [CrossRef]
- Lacroix, M.; Mulé, S.; Herin, E.; Pigneur, F.; Richard, P.; Zegai, B.; Baranes, L.; Djabbari, M.; Brunetti, F.; De’angelis, N.; et al. Virtual unenhanced imaging of the liver derived from 160-mm rapid-switching dual-energy CT (rsDECT): Comparison of the accuracy of attenuation values and solid liver lesion conspicuity with native unenhanced images. Eur. J. Radiol. 2020, 133, 109387. [Google Scholar] [CrossRef] [PubMed]
- Lundin, M.; Lidén, M.; Magnuson, A.; Mohammed, A.A.; Geijer, H.; Andersson, T.; Persson, A. Virtual non-contrast dual-energy CT compared to single-energy CT of the urinary tract: A prospective study. Acta Radiol. 2012, 53, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, L.; Rajiah, P.; Ahn, R.; Rassouli, N.; Xi, Y.; Soesbe, T.C.; Lewis, M.A.; Lenkinski, R.E.; Leyendecker, J.R.; Abbara, S. Spectral detector CT-derived virtual non-contrast images: Comparison of attenuation values with unenhanced CT. Abdom. Radiol. 2017, 42, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Virarkar, M.K.; Vulasala, S.S.R.; Gupta, A.V.; Gopireddy, D.; Kumar, S.; Hernandez, M.; Lall, C.; Bhosale, P. Virtual Non-contrast Imaging in The Abdomen and The Pelvis: An Overview. Semin. Ultrasound CT MRI 2022, 43, 293–310. [Google Scholar] [CrossRef] [PubMed]
- Leithner, D.; Wichmann, J.L.; Vogl, T.J.; Trommer, J.; Martin, S.S.; Scholtz, J.-E.; Bodelle, B.; De Cecco, C.N.; Duguay, T.; Nance, J.W.; et al. Virtual Monoenergetic Imaging and Iodine Perfusion Maps Improve Diagnostic Accuracy of Dual-Energy Computed Tomography Pulmonary Angiography with Suboptimal Contrast Attenuation. Investig. Radiol. 2017, 52, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, M.H.; Scholtz, J.-E.; Kraft, J.; Bauer, R.W.; Kaup, M.; Dewes, P.; Bucher, A.M.; Burck, I.; Wagenblast, J.; Lehnert, T.; et al. Assessment of an Advanced Monoenergetic Reconstruction Technique in Dual-Energy Computed Tomography of Head and Neck Cancer. Eur. Radiol. 2015, 25, 2493–2501. [Google Scholar] [CrossRef] [PubMed]
- Noda, Y.; Nakamura, F.; Yasuda, N.; Miyoshi, T.; Kawai, N.; Kawada, H.; Hyodo, F.; Matsuo, M. Advantages and disadvantages of single-source dual-energy whole-body CT angiography with 50% reduced iodine dose at 40 keV reconstruction. Br. J. Radiol. 2021, 94, 20201276. [Google Scholar] [CrossRef] [PubMed]
- Patino, M.; Parakh, A.; Lo, G.C.; Agrawal, M.; Kambadakone, A.R.; Oliveira, G.R.; Sahani, D.V. Virtual Monochromatic Dual-Energy Aortoiliac CT Angiography with Reduced Iodine Dose: A Prospective Randomized Study. Am. J. Roentgenol. 2019, 212, 467–474. [Google Scholar] [CrossRef]
- Matsumoto, K.; Jinzaki, M.; Tanami, Y.; Ueno, A.; Yamada, M.; Kuribayashi, S. Virtual Monochromatic Spectral Imaging with Fast Kilovoltage Switching: Improved Image Quality as Compared with That Obtained with Conventional 120-kVp CT. Radiology 2011, 259, 257–262. [Google Scholar] [CrossRef]
- Winkelmann, M.T.; Hagen, F.; Artzner, K.; Bongers, M.N.; Artzner, C. Dual-Energy CT for Accurate Discrimination of Intraperitoneal Hematoma and Intestinal Structures. Diagnostics 2022, 12, 2542. [Google Scholar] [CrossRef]
- Artzner, C.; Grozinger, G.; Kolb, M.; Walter, S.S.; Gatidis, S.; Bongers, M.N. Effect of acquisition techniques, latest kernels, and advanced monoenergetic post-processing for stent visualization with third-generation dual-source CT. Diagn. Interv. Radiol. 2022, 28, 364–369. [Google Scholar] [CrossRef]
- Greffier, J.; Dabli, D.; Hamard, A.; Akessoul, P.; Belaouni, A.; Beregi, J.-P.; Frandon, J. Impact of dose reduction and the use of an advanced model-based iterative reconstruction algorithm on spectral performance of a dual-source CT system: A task-based image quality assessment. Diagn. Interv. Imaging 2021, 102, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Dabli, D.; Frandon, J.; Belaouni, A.; Akessoul, P.; Addala, T.; Berny, L.; Beregi, J.-P.; Greffier, J. Optimization of image quality and accuracy of low iodine concentration quantification as function of dose level and reconstruction algorithm for abdominal imaging using dual-source CT: A phantom study. Diagn. Interv. Imaging 2022, 103, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Shayan, R.G.; Oladghaffari, M.; Sajjadian, F.; Ghaziyani, M.F. Image Quality and Dose Comparison of Single-Energy CT (SECT) and Dual-Energy CT (DECT). Radiol. Res. Pract. 2020, 2020, 1403957. [Google Scholar] [CrossRef]
- Greffier, J.; Si-Mohamed, S.; Dabli, D.; de Forges, H.; Hamard, A.; Douek, P.; Beregi, J.P.; Frandon, J. Performance of four dual-energy CT platforms for abdominal imaging: A task-based image quality assessment based on phantom data. Eur. Radiol. 2021, 31, 5324–5334. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, M.C.; Schellingerhout, D.; Wood, C.A.; Tamm, E.P.; Godoy, M.C.; Sun, J.; Cody, D.D. Intermanufacturer Comparison of Dual-Energy CT Iodine Quantification and Monochromatic Attenuation: A Phantom Study. Radiology 2018, 287, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Sellerer, T.; Noël, P.B.; Patino, M.; Parakh, A.; Ehn, S.; Zeiter, S.; Holz, J.A.; Hammel, J.; Fingerle, A.A.; Pfeiffer, F.; et al. Dual-energy CT: A phantom comparison of different platforms for abdominal imaging. Eur. Radiol. 2018, 28, 2745–2755. [Google Scholar] [CrossRef]
- Harsaker, V.; Jensen, K.; Andersen, H.K.; Martinsen, A.C. Quantitative benchmarking of iodine imaging for two CT spectral imaging technologies: A phantom study. Eur. Radiol. Exp. 2021, 5, 24. [Google Scholar] [CrossRef]
- Greffier, J.; Si-Mohamed, S.; Guiu, B.; Frandon, J.; Loisy, M.; de Oliveira, F.; Douek, P.; Beregi, J.-P.; Dabli, D. Comparison of virtual monoenergetic imaging between a rapid kilovoltage switching dual-energy computed tomography with deep-learning and four dual-energy CTs with iterative reconstruction. Quant. Imaging Med. Surg. 2022, 12, 1149–1162. [Google Scholar] [CrossRef]
- Dabli, D.; Loisy, M.; Frandon, J.; de Oliveira, F.; Meerun, A.M.; Guiu, B.; Beregi, J.-P.; Greffier, J. Comparison of image quality of two versions of deep-learning image reconstruction algorithm on a rapid kV-switching CT: A phantom study. Eur. Radiol. Exp. 2023, 7, 1. [Google Scholar] [CrossRef]
- Greffier, J.; Viry, A.; Barbotteau, Y.; Frandon, J.; Loisy, M.; de Oliveira, F.; Beregi, J.P.; Dabli, D. Phantom task-based image quality assessment of three generations of rapid kV-switching dual-energy CT systems on virtual monoenergetic images. Med. Phys. 2022, 49, 2233–2244. [Google Scholar] [CrossRef] [PubMed]
- Lourenco, P.D.M.; Rawski, R.; Mohammed, M.F.; Khosa, F.; Nicolaou, S.; McLaughlin, P. Dual-Energy CT Iodine Mapping and 40-keV Monoenergetic Applications in the Diagnosis of Acute Bowel Ischemia. Am. J. Roentgenol. 2018, 211, 564–570. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, T.; Cicero, G.; Mazziotti, S.; Ascenti, G.; Albrecht, M.H.; Martin, S.S.; Othman, A.E.; Vogl, T.J.; Wichmann, J.L. Dual energy computed tomography virtual monoenergetic imaging: Technique and clinical applications. Br. J. Radiol. 2019, 92, 20180546. [Google Scholar] [CrossRef] [PubMed]
- Mulé, S.; Pigneur, F.; Quelever, R.; Tenenhaus, A.; Baranes, L.; Richard, P.; Tacher, V.; Herin, E.; Pasquier, H.; Ronot, M.; et al. Can dual-energy CT replace perfusion CT for the functional evaluation of advanced hepatocellular carcinoma? Eur. Radiol. 2018, 28, 1977–1985. [Google Scholar] [CrossRef]
- Hokamp, N.G.; Höink, A.J.; Doerner, J.; Jordan, D.W.; Pahn, G.; Persigehl, T.; Maintz, D.; Haneder, S. Assessment of arterially hyper-enhancing liver lesions using virtual monoenergetic images from spectral detector CT: Phantom and patient experience. Abdom. Radiol. 2018, 43, 2066–2074. [Google Scholar] [CrossRef] [PubMed]
- McNamara, M.M.; Little, M.D.; Alexander, L.F.; Van Carroll, L.; Beasley, T.M.; Morgan, D.E. Multireader evaluation of lesion conspicuity in small pancreatic adenocarcinomas: Complimentary value of iodine material density and low keV simulated monoenergetic images using multiphasic rapid kVp-switching dual energy CT. Abdom. Imaging 2015, 40, 1230–1240. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.N.; Farjat, A.; Schabel, C.; Duvnjak, P.; Mileto, A.; Ramirez-Giraldo, J.C.; Marin, D. Energy-Specific Optimization of Attenuation Thresholds for Low-Energy Virtual Monoenergetic Images in Renal Lesion Evaluation. Am. J. Roentgenol. 2018, 210, W205–W217. [Google Scholar] [CrossRef]
- Gómez, D.; Cabrera-Vargas, L.F.; Pedraza, M.; Mendoza, A.; Pulido-Segura, J.A.; Villarreal-Viana, R.; Urrutia, A.; Sanchez-Ussa, S.; Di Saverio, S. Minimal invasive surgery for multiple adhesive small bowel obstruction: Results of a comparative multicenter study. Cirugía Y Cir. 2021, 89, 710–717. [Google Scholar] [CrossRef]
- Martin, S.S.; Pfeifer, S.; Wichmann, J.L.; Albrecht, M.H.; Leithner, D.; Lenga, L.; Scholtz, J.-E.; Vogl, T.J.; Bodelle, B. Noise-optimized virtual monoenergetic dual-energy computed tomography: Optimization of kiloelectron volt settings in patients with gastrointestinal stromal tumors. Abdom. Radiol. 2017, 42, 718–726. [Google Scholar] [CrossRef]
- Darras, K.E.; McLaughlin, P.D.; Kang, H.; Black, B.; Walshe, T.; Chang, S.D.; Harris, A.C.; Nicolaou, S. Virtual monoenergetic reconstruction of contrast-enhanced dual energy CT at 70keV maximizes mural enhancement in acute small bowel obstruction. Eur. J. Radiol. 2016, 85, 950–956. [Google Scholar] [CrossRef]
- Potretzke, T.A.; Brace, C.L.; Lubner, M.G.; Sampson, L.A.; Willey, B.J.; Lee, F.T. Early Small-Bowel Ischemia: Dual-Energy CT Improves Conspicuity Compared with Conventional CT in a Swine Model. Radiology 2015, 275, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Kim, S.H.; Ahn, S.J.; Kang, H.-J.; Kang, J.H.; Han, J.K. Virtual monoenergetic dual-layer, dual-energy CT enterography: Optimization of keV settings and its added value for Crohn’s disease. Eur. Radiol. 2018, 28, 2525–2534. [Google Scholar] [CrossRef] [PubMed]
- Zins, M.; Millet, I.; Taourel, P. Adhesive Small Bowel Obstruction: Predictive Radiology to Improve Patient Management. Radiology 2020, 296, 480–492. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.S.; Szczykutowicz, T.P. Evaluation of AAPM Reports 204 and 220: Estimation of effective diameter, water-equivalent diameter, and ellipticity ratios for chest, abdomen, pelvis, and head CT scans. J. Appl. Clin. Med. Phys. 2018, 19, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Fabacher, T.; Schaeffer, M.; Tuzin, N.; Séverac, F.; Lefebvre, F.; Mielcarek, M.; Sauleau, E.-A.; Meyer, N.; Godet, J. Biostatistiques médicales avec GMRC Shiny Stats—Un outil de formation par la pratique. Ann. Pharm. Françaises 2020, 78, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Tao, S.; Rajendran, K.; Zhou, W.; Fletcher, J.G.; McCollough, C.H.; Leng, S. Improving iodine contrast to noise ratio using virtual monoenergetic imaging and prior-knowledge-aware iterative denoising (mono-PKAID). Phys. Med. Biol. 2019, 64, 105014. [Google Scholar] [CrossRef] [PubMed]
- Krauss, B.; Grant, K.L.; Schmidt, B.T.; Flohr, T.G. The Importance of Spectral Separation: An Assessment of Dual-Energy Spectral Separation for Quantitative Ability and Dose Efficiency. Investig. Radiol. 2015, 50, 114–118. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Colitis | Bowel Occlusion | p Value | ||
|---|---|---|---|---|
| Dosimetric data | DLP (mGy × cm) | 366.13 ± 108.53 (198.50–630.75) | 514.05 ± 245.62 (183.06–1272.6) | 0.004 * |
| CTDIvol (mGy) | 7.45 ± 1.84 (4.53–12.04) | 10.00 ± 4.60 (4.08–27.43) | 0.005 * | |
| Effective diameter (cm) | 26.77 ± 4.00 (18.71–35.50) | 31.83 ± 3.77 (25.07–38.68) | <0.001 * | |
| SSDE (mGy) | 10.25 ± 2.03 (6.26–18.42) | 11.23 ± 4.31 (4.31–26.06) | 0.852 |
| Image Quality Metric | Energy Levels (keV) | Mixed Image | 70 | 60 | 50 |
|---|---|---|---|---|---|
| Noise | 40 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| 50 | <0.001 * | <0.001 * | <0.001 * | - | |
| 60 | <0.001 * | 0.475 | - | - | |
| 70 | 0.530 | - | - | - | |
| Contrast | 40 | <0.001 * | <0.001 * | <0.001 * | < 0.001 * |
| 50 | <0.001 * | <0.001 * | <0.001 * | - | |
| 60 | <0.001 * | <0.001 * | - | - | |
| 70 | 0.360 | - | - | - | |
| CNR ** | 40 | 0.314 | 0.608 | 0.262 | 0.664 |
| 50 | 0.977 | 0.294 | 0.903 | - | |
| 60 | 0.315 | 0.041 | - | - | |
| 70 | 0.245 | - | - | - |
| Image Quality Metric | Energy Levels (keV) | Mixed Image | 70 | 60 | 50 |
|---|---|---|---|---|---|
| Noise | 40 | <0.001 * | <0.001 * | <0.001 * | 0.006 * |
| 50 | <0.001 * | <0.001 * | <0.001 * | - | |
| 60 | <0.001 * | 0.059 | - | - | |
| 70 | 0.071 | - | - | - | |
| Contrast | 40 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| 50 | <0.001 * | <0.001 * | <0.001 * | - | |
| 60 | <0.001 * | 0.001 * | - | - | |
| 70 | 0.135 | - | - | - | |
| CNR ** | 40 | 0.083 | 0.484 | 0.048 | 0.857 |
| 50 | 0.064 | 0.595 | 0.095 | - | |
| 60 | 0.294 | 0.045 | - | - | |
| 70 | 0.066 | - | - | - |
| Image Quality Criterion | Energy Levels (keV) | Mixed Image | 70 | 60 | 50 |
|---|---|---|---|---|---|
| Noise | 40 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| 50 | <0.001 * | 0.039 * | <0.001 * | - | |
| 60 | 0.001 * | 0.010 * | - | - | |
| 70 | 0.521 | - | - | - | |
| Smoothing | 40 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| 50 | 0.035 * | 0.513 | <0.001 * | - | |
| 60 | 0.119 | <0.001 * | - | - | |
| 70 | 0.005 * | - | - | - | |
| Overall image quality | 40 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| 50 | 0.023 * | 0.476 | <0.001 * | - | |
| 60 | 0.009 * | 0.001 * | - | - | |
| 70 | 0.283 | - | - | - |
| Image Quality Criterion | Energy Levels (keV) | Mixed Image | 70 | 60 | 50 |
|---|---|---|---|---|---|
| Noise | 40 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| 50 | 0.014 * | 0.893 | <0.001 * | - | |
| 60 | 0.029 * | 0.004 * | - | - | |
| 70 | 0.066 | - | - | - | |
| Smoothing | 40 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| 50 | 0.014 * | 0.976 | <0.001 * | - | |
| 60 | 0.888 | 0.016 * | - | - | |
| 70 | 0.030 * | - | - | - | |
| Global image quality | 40 | <0.001 * | <0.001 * | <0.001 * | <0.001 * |
| 50 | 0.162 | 0.311 | <0.001 * | - | |
| 60 | 0.043 * | <0.001 * | - | - | |
| 70 | 0.057 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lahuna, L.; Greffier, J.; Goupil, J.; Frandon, J.; Pastor, M.; De Oliveira, F.; Beregi, J.P.; Dabli, D. Determining the Optimal Energy Level of Virtual Monoenergetic Images in Dual-Source CT for Diagnosis of Bowel Obstruction and Colitis. Diagnostics 2023, 13, 3491. https://doi.org/10.3390/diagnostics13233491
Lahuna L, Greffier J, Goupil J, Frandon J, Pastor M, De Oliveira F, Beregi JP, Dabli D. Determining the Optimal Energy Level of Virtual Monoenergetic Images in Dual-Source CT for Diagnosis of Bowel Obstruction and Colitis. Diagnostics. 2023; 13(23):3491. https://doi.org/10.3390/diagnostics13233491
Chicago/Turabian StyleLahuna, Loris, Joël Greffier, Jean Goupil, Julien Frandon, Maxime Pastor, Fabien De Oliveira, Jean Paul Beregi, and Djamel Dabli. 2023. "Determining the Optimal Energy Level of Virtual Monoenergetic Images in Dual-Source CT for Diagnosis of Bowel Obstruction and Colitis" Diagnostics 13, no. 23: 3491. https://doi.org/10.3390/diagnostics13233491
APA StyleLahuna, L., Greffier, J., Goupil, J., Frandon, J., Pastor, M., De Oliveira, F., Beregi, J. P., & Dabli, D. (2023). Determining the Optimal Energy Level of Virtual Monoenergetic Images in Dual-Source CT for Diagnosis of Bowel Obstruction and Colitis. Diagnostics, 13(23), 3491. https://doi.org/10.3390/diagnostics13233491