
Efficient Thorax Disease Classification and Localization Using DCNN and Chest X-ray Images


Abstract
:1. Introduction
- To identify the state-of-the-art technique for thorax disease classification and localization;
- To develop and design an architecture for thorax diseases, multi-classification, and their localization and implement it through the proposed model;
- To evaluate the proposed model and achieve higher accuracy (AUC-ROC) as compared to the state-of-the-art research.
2. Related Work
3. Dataset
3.1. ChestX-ray14
3.2. Preprocessing
3.3. Class Imbalance
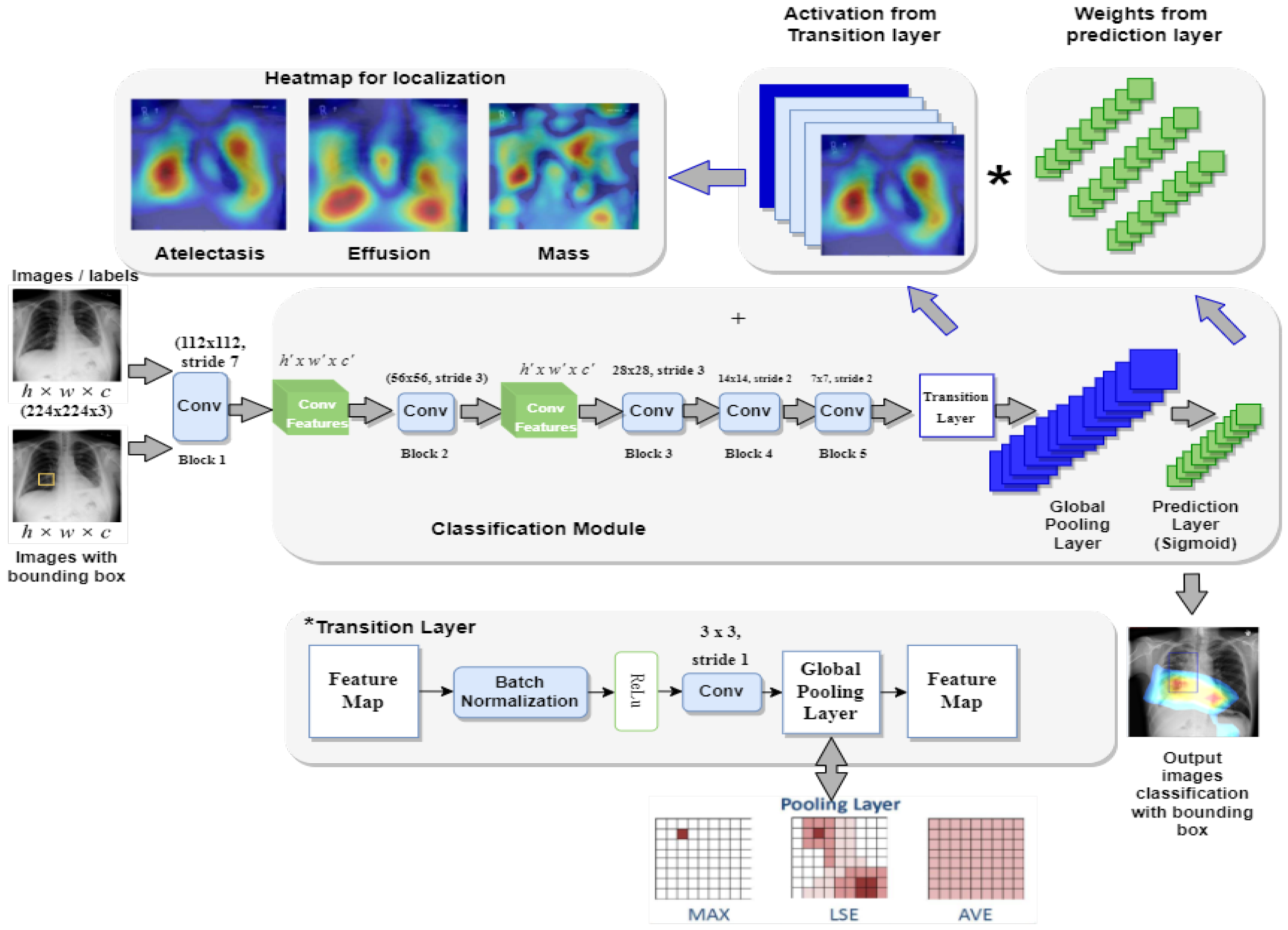
4. Proposed Z-Net Model
4.1. Z-Net Framework
4.2. Components of the Z-Net
- Multi-labeling;
- Transition Layer;
- Loss Layer;
- Global Pooling and Prediction Layer;
- Bounding Box Generation.
| Algorithm 1: Pseudocode of Z-Net model |
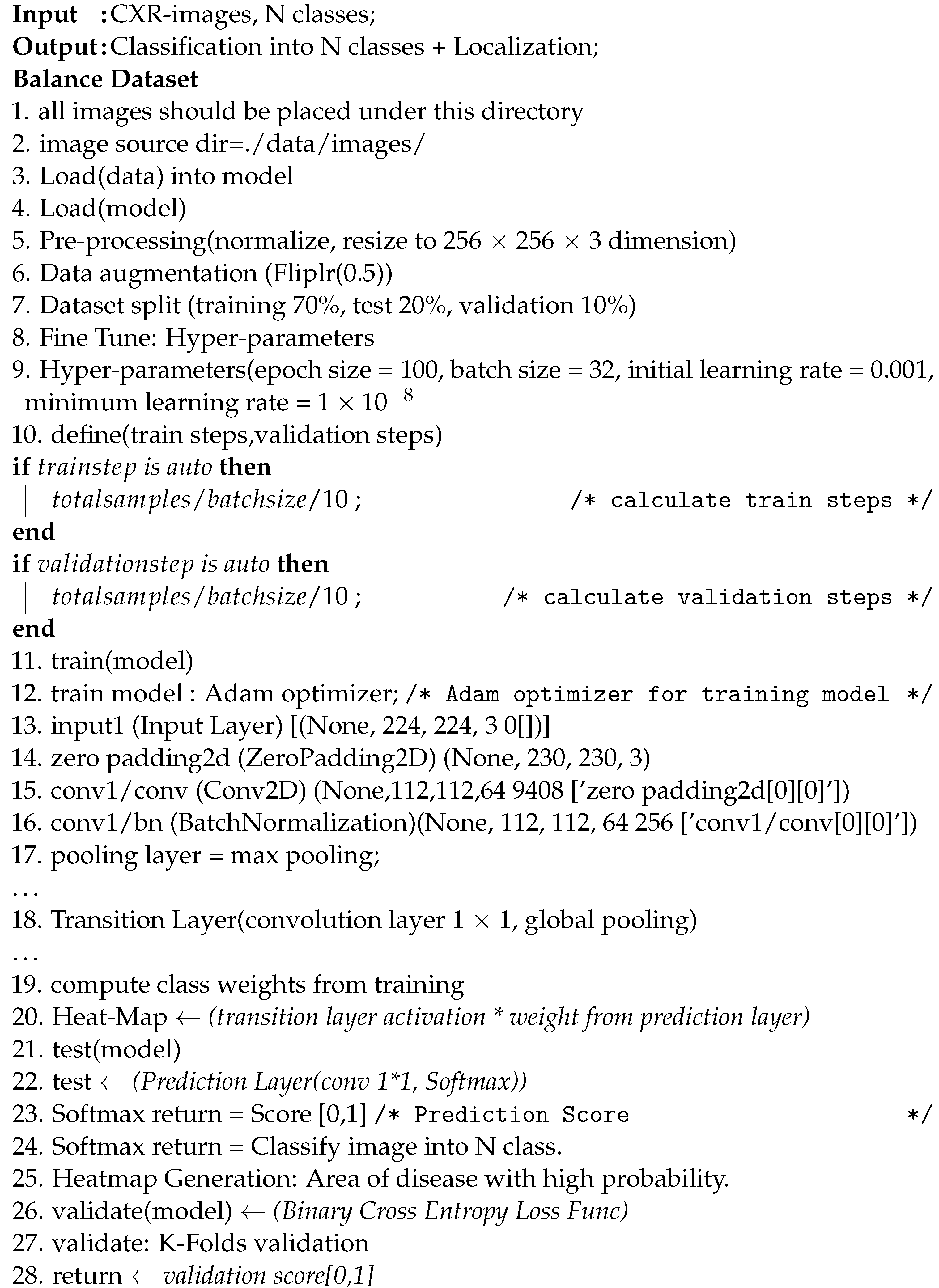 |
4.2.1. Multi-labeling
4.2.2. Transition Layer
4.2.3. Loss Layer
4.2.4. Global Pooling and Prediction Layer
4.2.5. Bounding Box Generation
4.3. Disease Localization
5. Experimental Setup
5.1. Dataset Preparation
5.2. Experimental Settings
6. Results and Comparison
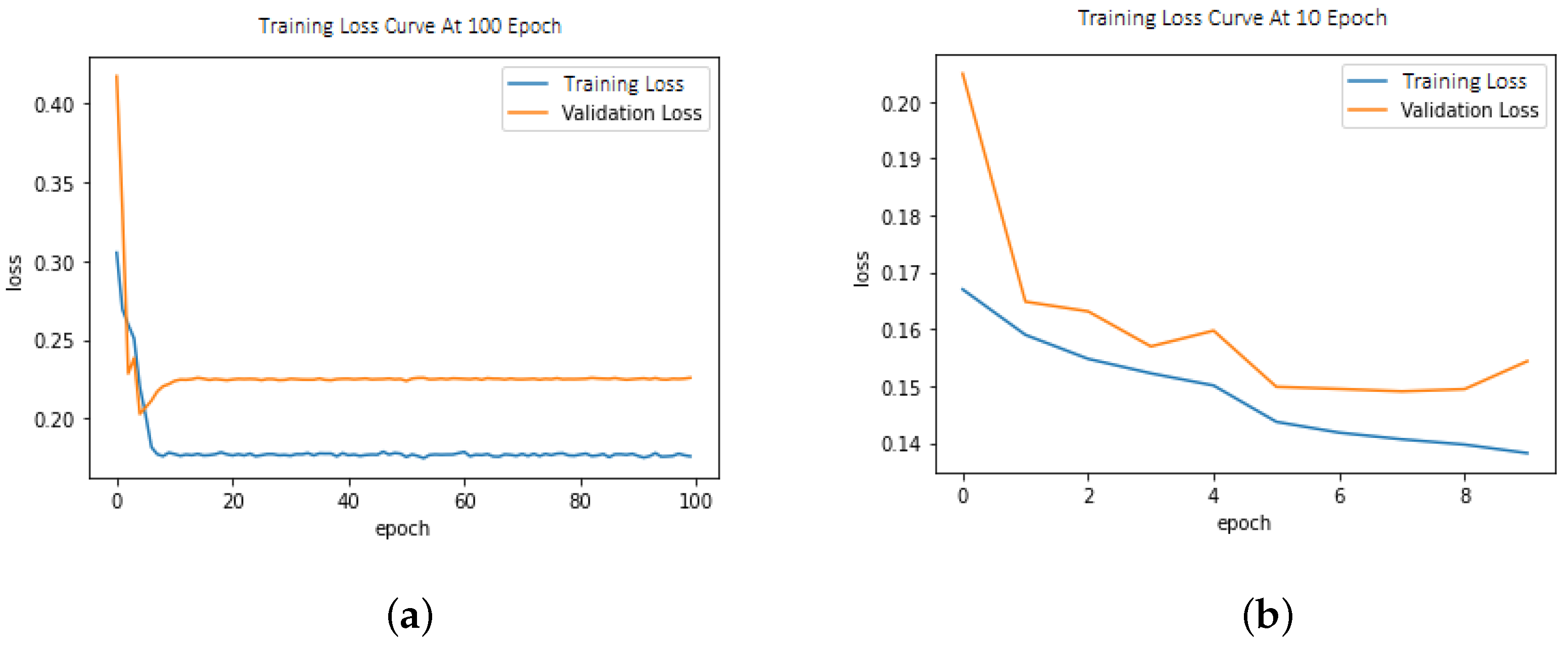
6.1. Loss Function
6.2. Multi-Label Disease Classification
6.3. Evaluation Metrics
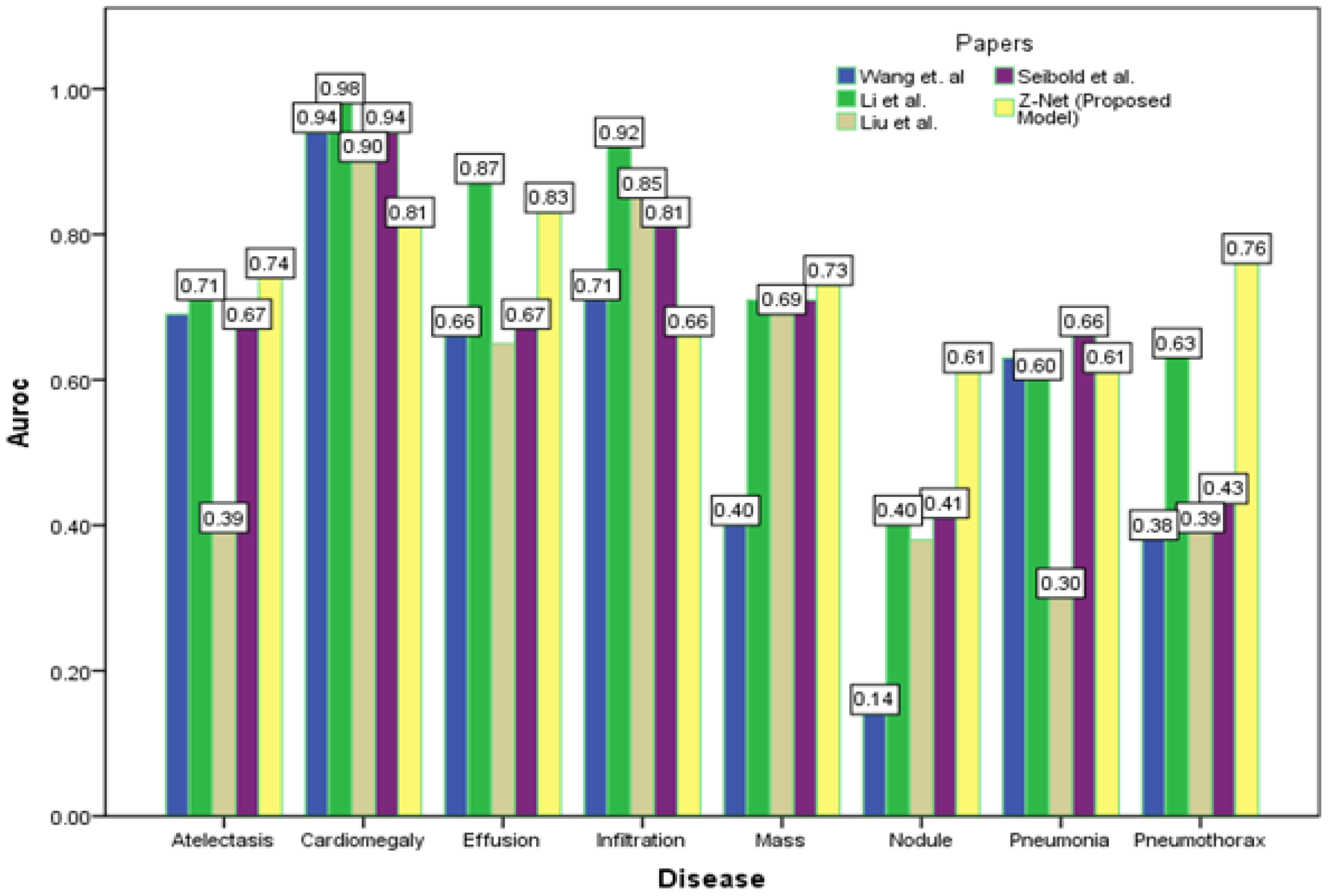
6.4. Comparative Analysis
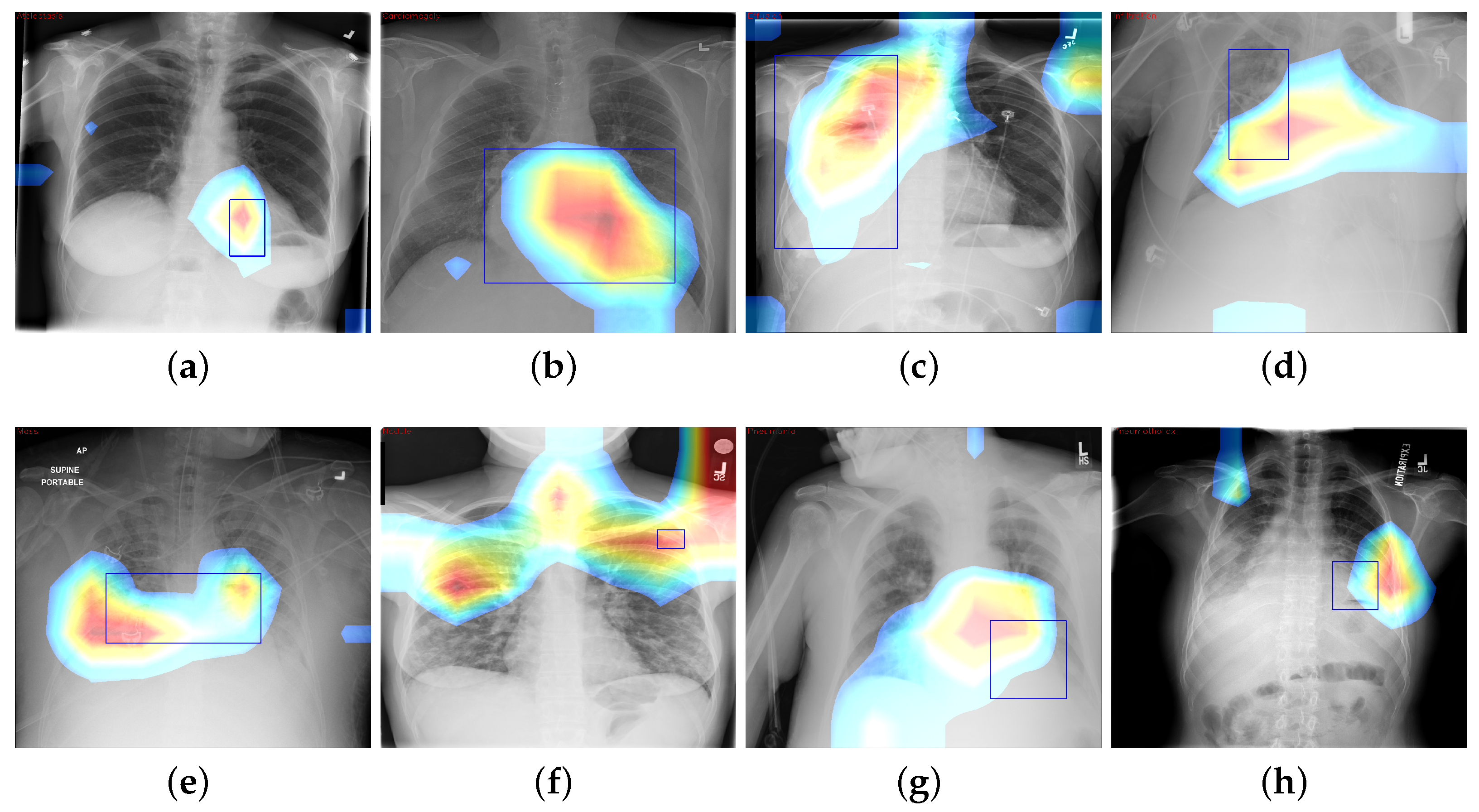
6.5. CAM Visualization
7. Discussion
8. Conclusions and Future Work
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Bagheri, M.; Summers, R. Chestx-ray8: Hospital-scale chest x-ray database and benchmarks on weakly-supervised classification and localization of common thorax diseases. In Proceedings of the IEEE CVPR 2017, Honolulu, HI, USA, 21–26 July 2017; pp. 2097–2106. [Google Scholar]
- Alfarghaly, O.; Khaled, R.; Elkorany, A.; Helal, M.; Fahmy, A. Automated radiology report generation using conditioned transformers. Inform. Med. Unlocked 2021, 24, 100557. [Google Scholar] [CrossRef]
- Li, Z.; Wang, C.; Han, M.; Xue, Y.; Wei, W.; Li, L.J.; Fei-Fei, L. Thoracic disease identification and localization with limited supervision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR 2018), Salt Lake City, UT, USA, 18–22 June 2018; pp. 8290–8299. [Google Scholar]
- Chen, B.; Zhang, Z.; Li, Y.; Lu, G.; Zhang, D. Multi-label chest X-ray image classification via semantic similarity graph embedding. IEEE Trans. Circuits Syst. Video Technol. 2021, 32, 2455–2468. [Google Scholar] [CrossRef]
- Xu, X.; Guo, Q.; Guo, J.; Yi, Z. Deepcxray: Automatically diagnosing diseases on chest X-rays using deep neural networks. IEEE Access 2018, 6, 66972–66983. [Google Scholar] [CrossRef]
- Lian, J.; Liu, J.; Zhang, S.; Gao, K.; Liu, X.; Zhang, D.; Yu, Y. A Structure-Aware Relation Network for Thoracic Diseases Detection and Segmentation. IEEE Trans. Med. Imaging 2021, 40, 2042–2052. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Li, J.; Lu, G.; Yu, H.; Zhang, D. Label co-occurrence learning with graph convolutional networks for multi-label chest X-ray image classification. IEEE J. Biomed. Health Inform. 2020, 24, 2292–2302. [Google Scholar] [CrossRef]
- Ouyang, X.; Karanam, S.; Wu, Z.; Chen, T.; Huo, J.; Zhou, X.S.; Wang, Q.; Cheng, J.Z. Learning hierarchical attention for weakly-supervised chest X-ray abnormality localization and diagnosis. IEEE Trans. Med. Imaging 2020, 40, 2698–2710. [Google Scholar] [CrossRef]
- Luo, L.; Yu, L.; Chen, H.; Liu, Q.; Wang, X.; Xu, J.; Heng, P.A. Deep mining external imperfect data for chest X-ray disease screening. IEEE Trans. Med. Imaging 2020, 39, 3583–3594. [Google Scholar] [CrossRef]
- Yan, C.; Yao, J.; Li, R.; Xu, Z.; Huang, J. Weakly supervised deep learning for thoracic disease classification and localization on chest X-rays. In Proceedings of the 2018 ACM International Conference on Bioinformatics, Computational Biology, and Health Informatics, Washington, DC, USA, 29 August–1 September 2018; pp. 103–110. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Zhao, G.; Fang, C.; Li, G.; Jiao, L.; Yu, Y. Contralaterally Enhanced Networks for Thoracic Disease Detection. IEEE Trans. Med. Imaging 2021, 40, 2428–2438. [Google Scholar] [CrossRef]
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Summers, R.M. Tienet: Text-image embedding network for common thorax disease classification and reporting in chest X-rays. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 9049–9058. [Google Scholar]
- Wang, H.; Jia, H.; Lu, L.; Xia, Y. Thorax-net: An attention regularized deep neural network for classification of thoracic diseases on chest radiography. IEEE J. Biomed. Health Inform. 2019, 24, 475–485. [Google Scholar] [CrossRef]
- Wang, H.; Xia, Y. Chestnet: A deep neural network for classification of thoracic diseases on chest radiography. arXiv 2018, arXiv:1807.03058. [Google Scholar]
- Wang, K.; Zhang, X.; Huang, S.; Chen, F.; Zhang, X.; Huangfu, L. Learning to recognize thoracic disease in chest X-rays with knowledge-guided deep zoom neural networks. IEEE Access 2020, 8, 159790–159805. [Google Scholar] [CrossRef]
- Ma, Y.; Ma, A.J.; Pan, Y.; Chen, X. Multi-Scale Feature Pyramids for Weakly Supervised Thoracic Disease Localization. In Proceedings of the 2020 IEEE International Conference on Image Processing (ICIP), Abu Dhabi, United Arab Emirates, 25–28 October 2020; pp. 2481–2485. [Google Scholar]
- Yadav, S.S.; Jadhav, S.M. Deep convolutional neural network based medical image classification for disease diagnosis. J. Big Data 2019, 6, 1–18. [Google Scholar] [CrossRef]
- Ratul, R.H.; Husain, F.A.; Purnata, T.H.; Pomil, R.A.; Khandoker, S.; Parvez, M.Z. Multi-Stage Optimization of Deep Learning Model to Detect Thoracic Complications. In Proceedings of the 2021 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Melbourne, Australia (Virtual), 17–20 October 2021; pp. 3000–3005. [Google Scholar]
- Guan, Q.; Huang, Y.; Luo, Y.; Liu, P.; Xu, M.; Yang, Y. Discriminative Feature Learning for Thorax Disease Classification in Chest X-ray Images. IEEE Trans. Image Process. 2021, 30, 2476–2487. [Google Scholar] [CrossRef] [PubMed]
- Seibold, C.; Kleesiek, J.; Schlemmer, H.P.; Stiefelhagen, R. Self-Guided Multiple Instance Learning for Weakly Supervised Thoracic DiseaseClassification and Localizationin Chest Radiographs. In Proceedings of the Asian Conference on Computer Vision, Kyoto, Japan, 30 November–4 December 2020; pp. 617–634. [Google Scholar]
- Guan, Q.; Huang, Y.; Zhong, Z.; Zheng, Z.; Zheng, L.; Yang, Y. Diagnose like a radiologist: Attention guided convolutional neural network for thorax disease classification. arXiv 2018, arXiv:1801.09927. [Google Scholar]
- Chen, B.; Li, J.; Lu, G.; Zhang, D. Lesion location attention guided network for multi-label thoracic disease classification in chest X-rays. IEEE J. Biomed. Health Inform. 2019, 24, 2016–2027. [Google Scholar] [CrossRef]
- Rehman, N.u.; Zia, M.S.; Meraj, T.; Rauf, H.T.; Damaševičius, R.; El-Sherbeeny, A.M.; El-Meligy, M.A. A self-activated cnn approach for multi-class chest-related COVID-19 detection. Appl. Sci. 2021, 11, 9023. [Google Scholar] [CrossRef]
- Jennifer, J.S.; Sharmila, T.S. A Neutrosophic Set Approach on Chest X-rays for Automatic Lung Infection Detection. Inf. Technol. Control 2023, 52, 37–52. [Google Scholar] [CrossRef]
- Jaszcz, A.; Połap, D.; Damaševičius, R. Lung X-ray image segmentation using heuristic red fox optimization algorithm. Sci. Program. 2022, 2022, 4494139. [Google Scholar] [CrossRef]
- Khan, M.A.; Rajinikanth, V.; Satapathy, S.C.; Taniar, D.; Mohanty, J.R.; Tariq, U.; Damaševičius, R. VGG19 network assisted joint segmentation and classification of lung nodules in CT images. Diagnostics 2021, 11, 2208. [Google Scholar] [CrossRef]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. Chexnet: Radiologist-level pneumonia detection on chest X-rays with deep learning. arXiv 2017, arXiv:1711.05225. [Google Scholar]
- Wang, H.; Wang, S.; Qin, Z.; Zhang, Y.; Li, R.; Xia, Y. Triple attention learning for classification of 14 thoracic diseases using chest radiography. Med. Image Anal. 2021, 67, 101846. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, P.; Thapar, D.; Bhavsar, A.; Nigam, A. Hierarchical X-ray report generation via pathology tags and multi head attention. In Proceedings of the Asian Conference on Computer Vision (ACCV 2020), Kyoto, Japan, 30 November–4 December 2020; pp. 600–616. [Google Scholar]
- Sanchez, E.; Bulat, A.; Zaganidis, A.; Tzimiropoulos, G. Semi-supervised facial action unit intensity estimation with contrastive learning. In Proceedings of the Asian Conference on Computer Vision (ACCV 2020), Kyoto, Japan, 30 November–4 December 2020; pp. 104–120. [Google Scholar]
- Tang, Y.; Wang, X.; Harrison, A.P.; Lu, L.; Xiao, J.; Summers, R.M. Attention-guided curriculum learning for weakly supervised classification and localization of thoracic diseases on chest radiographs. In Proceedings of the International Workshop on Machine Learning in Medical Imaging (MLMI 2018), Granada, Spain, 16 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; pp. 249–258. [Google Scholar]
- Cai, J.; Lu, L.; Xing, F.; Yang, L. Pancreas segmentation in CT and MRI via task-specific network design and recurrent neural contextual learning. In Deep Learning and Convolutional Neural Networks for Medical Imaging and Clinical Informatics; Springer: Berlin/Heidelberg, Germany, 2019; pp. 3–21. [Google Scholar]
- Karabayir, I.; Akbilgic, O.; Tas, N. A novel learning algorithm to optimize deep neural networks: Evolved gradient direction optimizer (EVGO). IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 685–694. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhao, G.; Fei, Y.; Zhang, M.; Wang, Y.; Yu, Y. Align, attend and locate: Chest X-ray diagnosis via contrast induced attention network with limited supervision. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Seoul, Republic of Korea, 27 October–2 November 2019; pp. 10631–10640. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Frequency of Images |
|---|---|
| Infiltration | 19,871 |
| Atelectasis | 11,535 |
| Pneumothorax | 5298 |
| Consolidation | 4667 |
| Edema | 2303 |
| Fibrosis | 1686 |
| Emphysema | 2516 |
| Effusion | 13,307 |
| Pleural Thickening | 3385 |
| Pneumonia | 1353 |
| Cardiomegaly | 2772 |
| Mass | 5746 |
| Nodule | 6323 |
| Hernia | 227 |
| No Finding | 60,412 |
| Train | Test | Validation |
|---|---|---|
| 70% | 20% | 10% |
| Parameters | Value |
|---|---|
| Number of epochs | 100 |
| Optimizer | Adam |
| Batch size | 32 |
| Initial learning rate | 0.001 |
| Minimum learning rate | |
| Activation function | Sigmoid |
| Loss function | Binary Cross-Entropy Loss |
| Pathology | Wang et at. [1] | Li et al. [3] | CheXNet [28] | Thorax-Net [14] | Guan et al. [20] | Seibold et al. [21] | Proposed Z-Net Model |
|---|---|---|---|---|---|---|---|
| Atelectasis | 0.706 | 0.800 | 0.779 | 0.750 | 0.785 | 0.78 | 0.821 |
| Consolidation | 0.708 | 0.800 | 0.754 | 0.741 | 0.763 | 0.75 | 0.746 |
| Infiltration | 0.6128 | 0.700 | 0.689 | 0.681 | 0.699 | 0.71 | 0.722 |
| Pneumothorax | 0.789 | 0.870 | 0.851 | 0.825 | 0.871 | 0.81 | 0.898 |
| Edema | 0.835 | 0.880 | 0.849 | 0.835 | 0.850 | 0.86 | 0.864 |
| Emphysema | 0.815 | 0.910 | 0.924 | 0.842 | 0.924 | 0.95 | 0.923 |
| Fibrosis | 0.769 | 0.780 | 0.821 | 0.804 | 0.831 | 0.85 | 0.764 |
| Effusion | 0.736 | 0.870 | 0.826 | 0.818 | 0.835 | 0.84 | 0.889 |
| Pneumonia | 0.633 | 0.670 | 0.735 | 0.693 | 0.738 | 0.74 | 0.755 |
| Pleural Thickening | 0.708 | 0.790 | 0.792 | 0.776 | 0.746 | 0.90 | 0.784 |
| Cardiomegaly | 0.814 | 0.870 | 0.881 | 0.871 | 0.899 | 0.88 | 0.872 |
| Nodule | 0.716 | 0.750 | 0.781 | 0.714 | 0.775 | 0.81 | 0.744 |
| Mass | 0.560 | 0.830 | 0.830 | 0.799 | 0.838 | 0.84 | 0.840 |
| Hernia | 0.767 | 0.770 | 0.932 | 0.902 | 0.922 | 0.94 | 0.768 |
| Mean AUC | 0.813 | 0.806 | 0.818 | 0.787 | 0.822 | 0.83 | 0.858 |
| Disease | Wang et al. [1] | Li et al. [3] | Liu et al. [35] | Seibold et al. [21] | Z-Net (Proposed Model) |
|---|---|---|---|---|---|
| Atelectasis | 0.69 | 0.71 | 0.39 | 0.67 | 0.74 |
| Cardiomegaly | 0.94 | 0.98 | 0.90 | 0.94 | 0.81 |
| Effusion | 0.66 | 0.87 | 0.65 | 0.67 | 0.83 |
| Infiltration | 0.71 | 0.92 | 0.85 | 0.81 | 0.66 |
| Mass | 0.40 | 0.71 | 0.69 | 0.71 | 0.73 |
| Nodule | 0.14 | 0.40 | 0.38 | 0.41 | 0.61 |
| Pneumonia | 0.63 | 0.60 | 0.30 | 0.66 | 0.61 |
| Pneumothorax | 0.38 | 0.63 | 0.39 | 0.43 | 0.76 |
| Mean | 0.57 | 0.73 | 0.60 | 0.66 | 0.71 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, Z.; Malik, A.K.; Qamar, N.; Islam, S.u. Efficient Thorax Disease Classification and Localization Using DCNN and Chest X-ray Images. Diagnostics 2023, 13, 3462. https://doi.org/10.3390/diagnostics13223462
Ahmad Z, Malik AK, Qamar N, Islam Su. Efficient Thorax Disease Classification and Localization Using DCNN and Chest X-ray Images. Diagnostics. 2023; 13(22):3462. https://doi.org/10.3390/diagnostics13223462
Chicago/Turabian StyleAhmad, Zeeshan, Ahmad Kamran Malik, Nafees Qamar, and Saif ul Islam. 2023. "Efficient Thorax Disease Classification and Localization Using DCNN and Chest X-ray Images" Diagnostics 13, no. 22: 3462. https://doi.org/10.3390/diagnostics13223462
APA StyleAhmad, Z., Malik, A. K., Qamar, N., & Islam, S. u. (2023). Efficient Thorax Disease Classification and Localization Using DCNN and Chest X-ray Images. Diagnostics, 13(22), 3462. https://doi.org/10.3390/diagnostics13223462