
Comparison of Ultrasound Contrast between H2O2-Responsive Nanoparticles and Microbubble Contrast According to Muscle Injury in Rat Models



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
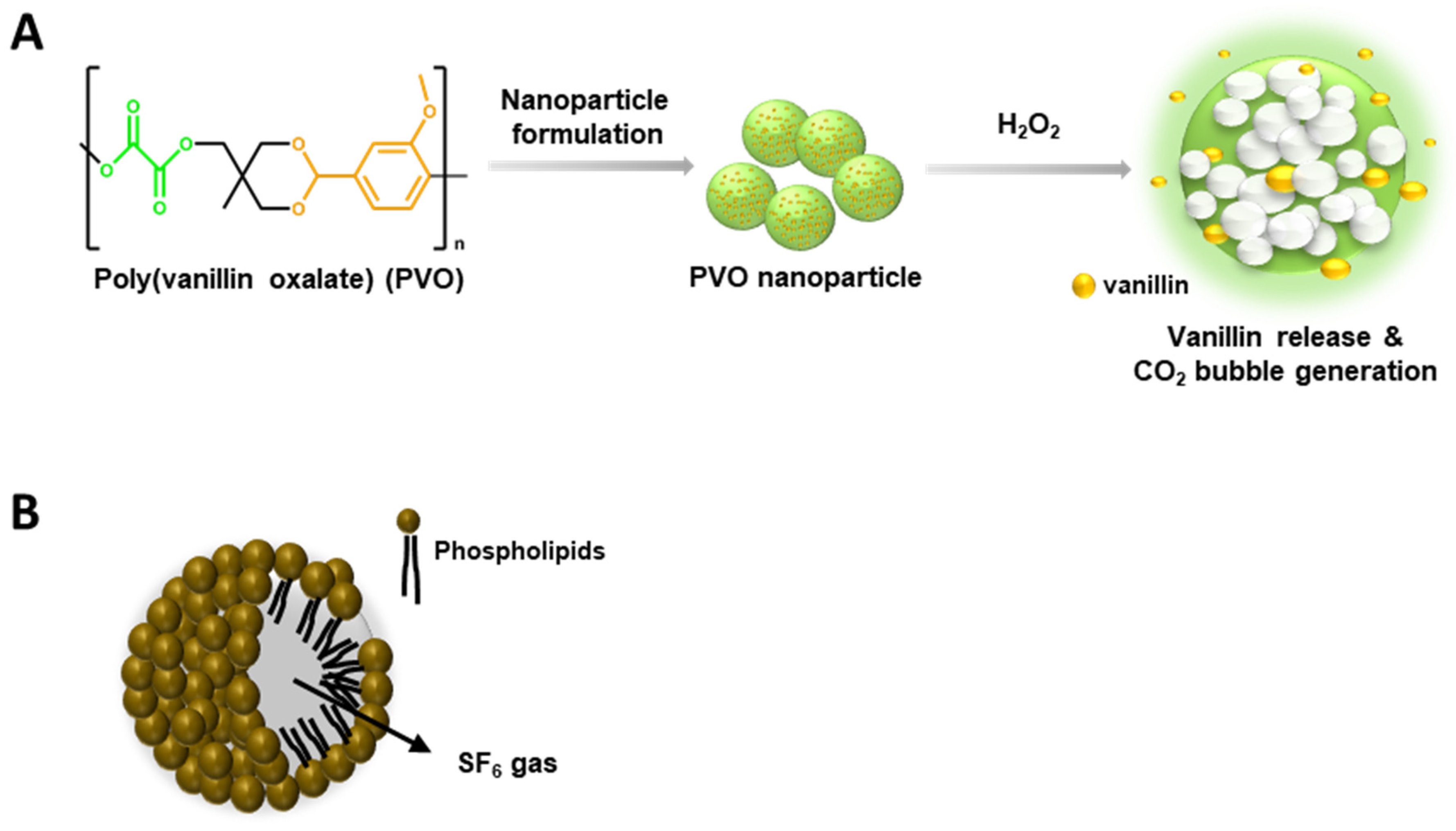
2.1. Preparation of PVO Nanoparticles and SonoVue®
2.2. Four Types of Muscle Injury Models in Rats
2.2.1. Laceration Injury
2.2.2. Punch Injury
2.2.3. Contusion Injury
2.2.4. Toxin Injection Injury
2.3. Determination of the Level H2O2 in the Site of Muscle Injuries
2.4. Ultrasonographic Imaging
2.5. Statistical Analysis
3. Results
3.1. Determination of H2O2 Level in Four Injury Models by Amplex Red Assay
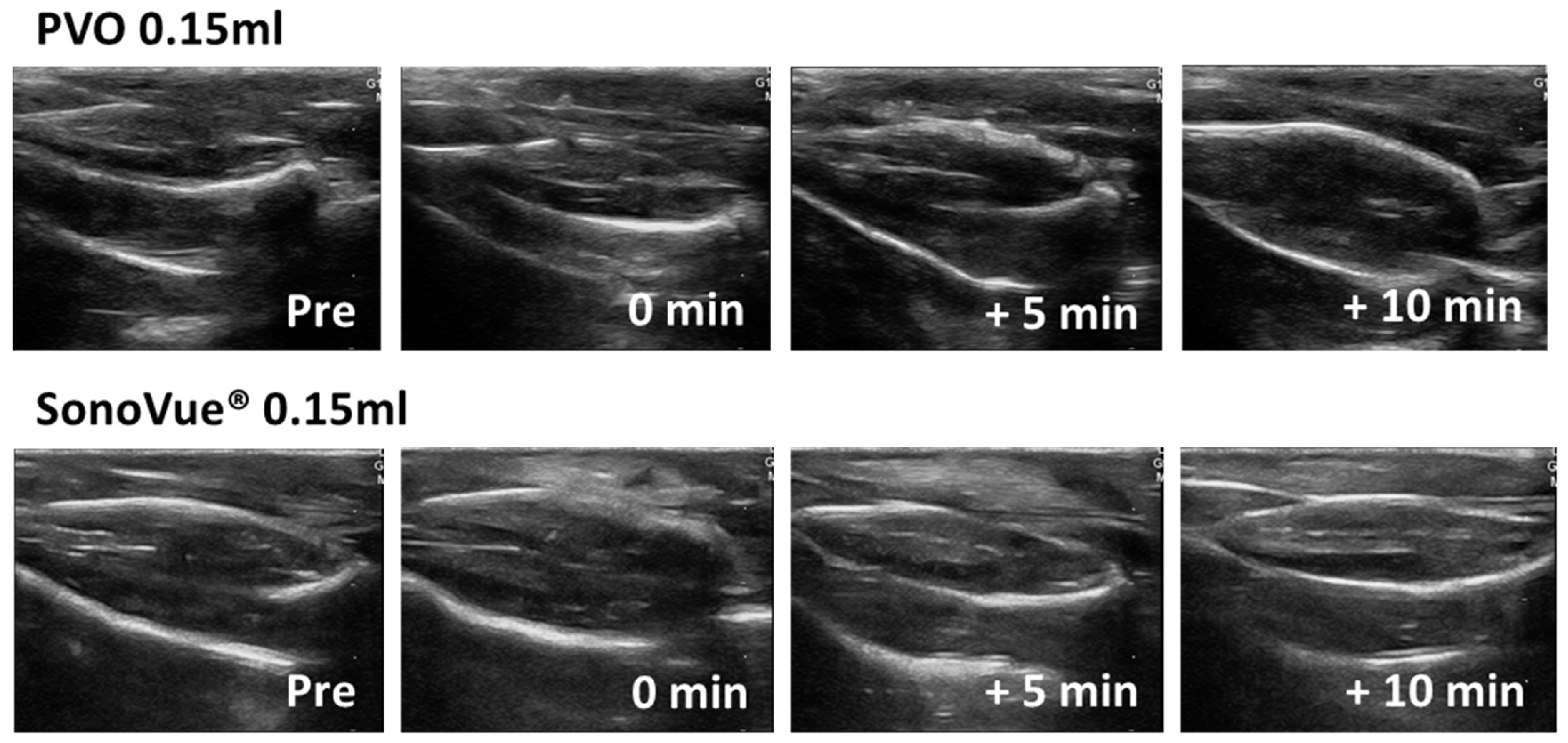
3.2. Contrast Enhanced Ultrasound Image Using PVO and SonoVue® in Sham Group
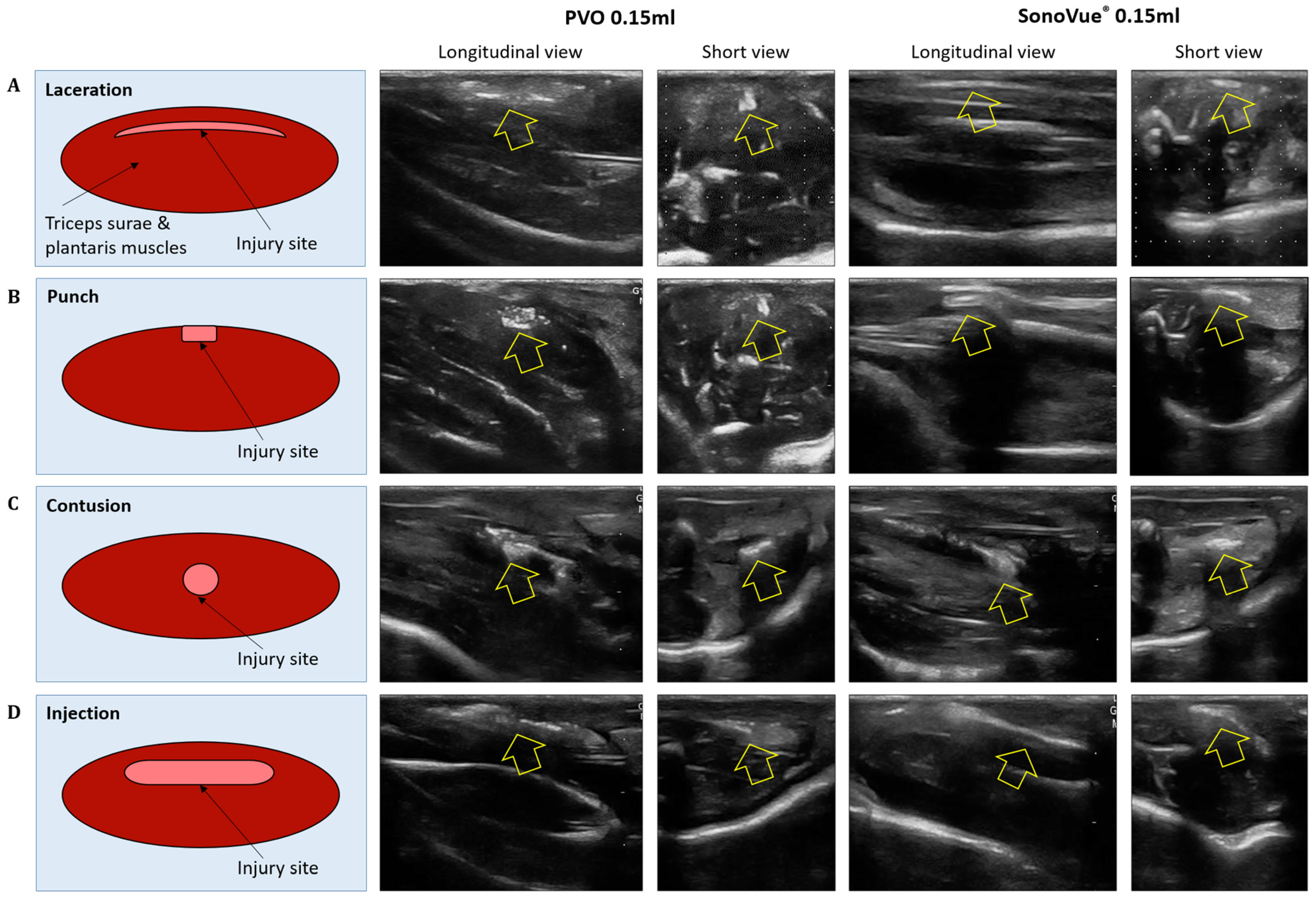
3.3. Ultrasound Images after PVO and SonoVue® Injection in the Muscle Injured Models
3.3.1. Laceration Model
3.3.2. Punch Models
3.3.3. Contusion Models
3.3.4. Toxin Injection Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ziskin, M.C.; Bonakdarpour, A.; Weinstein, D.P.; Lynch, P.R. Contrast agents for diagnostic ultrasound. Investig. Radiol. 1972, 7, 500–505. [Google Scholar] [CrossRef]
- Cosgrove, D. Ultrasound contrast agents: An overview. Eur. J. Radiol. 2006, 60, 324–330. [Google Scholar] [CrossRef]
- Frinking, P.; Segers, T.; Luan, Y.; Tranquart, F. Three Decades of Ultrasound Contrast Agents: A Review of the Past, Present and Future Improvements. Ultrasound Med. Biol. 2020, 46, 892–908. [Google Scholar] [CrossRef]
- Chang, K.V.; Lew, H.L.; Wang, T.-G.; Chen, W.-S. Use of contrast-enhanced ultrasonography in musculoskeletal medicine. Am. J. Phys. Med. Rehabil. 2012, 91, 449–457. [Google Scholar] [CrossRef]
- Adler, R.S.; Fealy, S.; Rudzki, J.R.; Kadrmas, W.; Verma, N.N.; Pearle, A.; Lyman, S.; Warren, R.F. Rotator cuff in asymptomatic volunteers: Contrast-enhanced US depiction of intratendinous and peritendinous vascularity. Radiology 2008, 248, 954–961. [Google Scholar] [CrossRef]
- Daniels, S.P.; Gettle, L.M.; Blankenbaker, D.G.; Lee, K.S.; Ross, A.B. Contrast-enhanced ultrasound-guided musculoskeletal biopsies: Our experience and technique. Skelet. Radiol. 2021, 50, 673–681. [Google Scholar] [CrossRef]
- Gamradt, S.C.; Gallo, R.A.; Adler, R.S.; Maderazo, A.; Altchek, D.W.; Warren, R.F.; Fealy, S. Vascularity of the supraspinatus tendon three months after repair: Characterization using contrast-enhanced ultrasound. J. Shoulder Elb. Surg. 2010, 19, 73–80. [Google Scholar] [CrossRef]
- Loizides, A.; Widmann, G.; Freuis, T.; Peer, S.; Gruber, H. Optimizing ultrasound-guided biopsy of musculoskeletal masses by application of an ultrasound contrast agent. Ultraschall Med. 2011, 32, 307–310. [Google Scholar] [CrossRef]
- Rudzki, J.R.; Rudzki, J.R.; Adler, R.; Kadrmas, W.R.; Verma, N.; Pearle, A.; Lyman, S.; Fealy, S. Contrast-enhanced ultrasound characterization of the vascularity of the rotator cuff tendon: Age- and activity-related changes in the intact asymptomatic rotator cuff. J. Shoulder Elb. Surg. 2008, 17 (Suppl. S1), 96–100. [Google Scholar] [CrossRef]
- Stramare, R.; Raffeiner, B.; Ciprian, L.; Scagliori, E.; Coran, A.; Perissinotto, E.; Fiocco, U.; Beltrame, V.; Rubaltelli, L. Evaluation of finger joint synovial vascularity in patients with rheumatoid arthritis using contrast-enhanced ultrasound with water immersion and a stabilized probe. J. Clin. Ultrasound 2012, 40, 147–154. [Google Scholar] [CrossRef]
- Tang, X.; Zhao, M.; Li, W.; Zhao, J. Nanoscale Contrast Agents for Ultrasound Imaging of Musculoskeletal System. Diagnostics 2022, 12, 2582. [Google Scholar] [CrossRef]
- Lee, D.; Bae, S.; Ke, Q.; Lee, J.; Song, B.; Karumanchi, S.A.; Khang, G.; Choi, H.S.; Kang, P.M. Hydrogen peroxide-responsive copolyoxalate nanoparticles for detection and therapy of ischemia–reperfusion injury. J. Control. Release 2013, 172, 1102–1110. [Google Scholar] [CrossRef]
- Negishi, Y.; Ishii, Y.; Shiono, H.; Akiyama, S.; Sekine, S.; Kojima, T.; Mayama, S.; Kikuchi, T.; Hamano, N.; Endo-Takahashi, Y.; et al. Bubble Liposomes and Ultrasound Exposure Improve Localized Morpholino Oligomer Delivery into the Skeletal Muscles of Dystrophic mdx Mice. Mol. Pharm. 2014, 11, 1053–1061. [Google Scholar] [CrossRef]
- Tang, Q.; Cui, J.; Tian, Z.; Sun, J.; Wang, Z.; Chang, S.; Zhu, S. Oxygen and indocyanine green loaded phase-transition nanoparticle-mediated photo-sonodynamic cytotoxic effects on rheumatoid arthritis fibroblast-like synoviocytes. Int. J. Nanomed. 2017, 12, 381–393. [Google Scholar] [CrossRef]
- Chen, L.; Ji, Y.; Hu, X.; Cui, C.; Liu, H.; Tang, Y.; Qi, B.; Niu, Y.; Hu, X.; Yu, A.; et al. Cationic poly-l-lysine-encapsulated melanin nanoparticles as efficient photoacoustic agents targeting to glycosaminoglycans for the early diagnosis of articular cartilage degeneration in osteoarthritis. Nanoscale 2018, 10, 13471–13484. [Google Scholar] [CrossRef]
- Jung, E.; Noh, J.; Kang, C.; Yoo, D.; Song, C.; Lee, D. Ultrasound imaging and on-demand therapy of peripheral arterial diseases using H2O2-Activated bubble generating anti-inflammatory polymer particles. Biomaterials 2018, 179, 175–185. [Google Scholar] [CrossRef]
- Wu, H.; He, Y.; Wu, H.; Zhou, M.; Xu, Z.; Xiong, R.; Yan, F.; Liu, H. Near-infrared fluorescence imaging-guided focused ultrasound-mediated therapy against Rheumatoid Arthritis by MTX-ICG-loaded iRGD-modified echogenic liposomes. Theranostics 2020, 10, 10092–10105. [Google Scholar] [CrossRef]
- Gong, Z.; He, Y.; Zhou, M.; Xin, H.; Pan, M.; Fiaz, M.; Liu, H.; Yan, F. Ultrasound imaging tracking of mesenchymal stem cells intracellularly labeled with biosynthetic gas vesicles for treatment of rheumatoid arthritis. Theranostics 2022, 12, 2370–2382. [Google Scholar] [CrossRef]
- Kim, G.-W.; Song, N.H.; Park, M.R.; Kim, T.E.; Kim, D.S.; Oh, Y.B.; Lee, D.W. Diagnosis and Simultaneous Treatment of Musculoskeletal Injury Using H2O2-Triggered Echogenic Antioxidant Polymer Nanoparticles in a Rat Model of Contusion Injury. Nanomaterials 2021, 11, 2571. [Google Scholar] [CrossRef]
- Kwon, J.; Kim, J.; Park, S.; Khang, G.; Kang, P.M.; Lee, D. Inflammation-responsive antioxidant nanoparticles based on a polymeric prodrug of vanillin. Biomacromolecules 2013, 14, 1618–1626. [Google Scholar] [CrossRef]
- Necas, J.; Bartosikova, L. Carrageenan: A review. Vet. Med. 2013, 58, 187–205. [Google Scholar] [CrossRef]
- Burns, P.N.; Wilson, S.R. Microbubble contrast for radiological imaging: 1. Principles. Ultrasound Q. 2006, 22, 5–13. [Google Scholar] [PubMed]
- Correas, J.-M.; Bridal, L.; Lesavre, A.; Méjean, A.; Claudon, M.; Hélénon, O. Ultrasound contrast agents: Properties, principles of action, tolerance, and artifacts. Eur. Radiol. 2001, 11, 1316–1328. [Google Scholar] [CrossRef] [PubMed]
- Unnikrishnan, S.; Klibanov, A.L. Microbubbles as Ultrasound Contrast Agents for Molecular Imaging: Preparation and Application. Am. J. Roentgenol. 2012, 199, 292–299. [Google Scholar] [CrossRef]
- Lee, H.J.; Chung, J.H. The application of contrast enhanced ultrasound in molecular imaging. J. Korean Soc. Ultrasound Med. 2009, 28, 139–145. [Google Scholar]
- Mody, V.; Siwale, R. Application of Nanoparticles in Diagnostic Imaging via Ultrasonography. Internet J. Med. Update 2011, 6, 8–15. [Google Scholar] [CrossRef]
- Lanza, G.M.; Wickline, S.A. Targeted ultrasonic contrast agents for molecular imaging and therapy. Prog. Cardiovasc. Dis. 2001, 44, 13–31. [Google Scholar] [CrossRef]
- Seo, M.; Gorelikov, I.; Williams, R.; Matsuura, N. Microfluidic assembly of monodisperse, nanoparticle-incorporated perfluorocarbon microbubbles for medical imaging and therapy. Langmuir 2010, 26, 13855–13860. [Google Scholar] [CrossRef]
- Chen, F.; Ma, M.; Wang, J.; Wang, F.; Chern, S.-X.; Zhao, E.R.; Jhunjhunwala, A.; Darmadi, S.; Chen, H.; Jokerst, J.V. Exosome-like silica nanoparticles: A novel ultrasound contrast agent for stem cell imaging. Nanoscale 2017, 9, 402–411. [Google Scholar] [CrossRef]
- Zhang, K.; Chen, H.; Guo, X.; Zhang, D.; Zheng, Y.; Zheng, H.; Shi, J. Double-scattering/reflection in a Single Nanoparticle for Intensified Ultrasound Imaging. Sci. Rep. 2015, 5, 8766. [Google Scholar] [CrossRef]
- Han, X.; Xu, K.; Taratula, O.; Farsad, K. Applications of nanoparticles in biomedical imaging. Nanoscale 2019, 11, 799–819. [Google Scholar] [CrossRef] [PubMed]
- Flegg, M.B.; Poole, C.M.; Whittaker, A.K.; Keen, I.; Langton, C.M. Rayleigh theory of ultrasound scattering applied to liquid-filled contrast nanoparticles. Phys. Med. Biol. 2010, 55, 3061–3076. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.-W.; Kang, C.; Oh, Y.-B.; Ko, M.-H.; Seo, J.-H.; Lee, D. Ultrasonographic imaging and anti-inflammatory therapy of muscle and tendon injuries using polymer nanoparticles. Theranostics 2017, 7, 2463. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-S.; Song, N.; Lee, D.; Kim, G.-W. Comparison of Ultrasound Contrast between H2O2-Responsive Nanoparticles and Microbubble Contrast According to Muscle Injury in Rat Models. Diagnostics 2023, 13, 3320. https://doi.org/10.3390/diagnostics13213320
Kim D-S, Song N, Lee D, Kim G-W. Comparison of Ultrasound Contrast between H2O2-Responsive Nanoparticles and Microbubble Contrast According to Muscle Injury in Rat Models. Diagnostics. 2023; 13(21):3320. https://doi.org/10.3390/diagnostics13213320
Chicago/Turabian StyleKim, Da-Sol, Nanhee Song, Dongwon Lee, and Gi-Wook Kim. 2023. "Comparison of Ultrasound Contrast between H2O2-Responsive Nanoparticles and Microbubble Contrast According to Muscle Injury in Rat Models" Diagnostics 13, no. 21: 3320. https://doi.org/10.3390/diagnostics13213320
APA StyleKim, D.-S., Song, N., Lee, D., & Kim, G.-W. (2023). Comparison of Ultrasound Contrast between H2O2-Responsive Nanoparticles and Microbubble Contrast According to Muscle Injury in Rat Models. Diagnostics, 13(21), 3320. https://doi.org/10.3390/diagnostics13213320