
Integrating Molecular Diagnostics and GIS Mapping: A Multidisciplinary Approach to Understanding Tuberculosis Disease Dynamics in South Africa Using Xpert MTB/RIF
 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Data Sources
2.3. Data Preparation
2.4. Analysis
2.4.1. Mapping and Spatial Analysis
2.4.2. Logistic Regression
2.5. Software
2.6. Ethics
3. Results
3.1. Spatial and Temporal Distribution of Mtb Testing
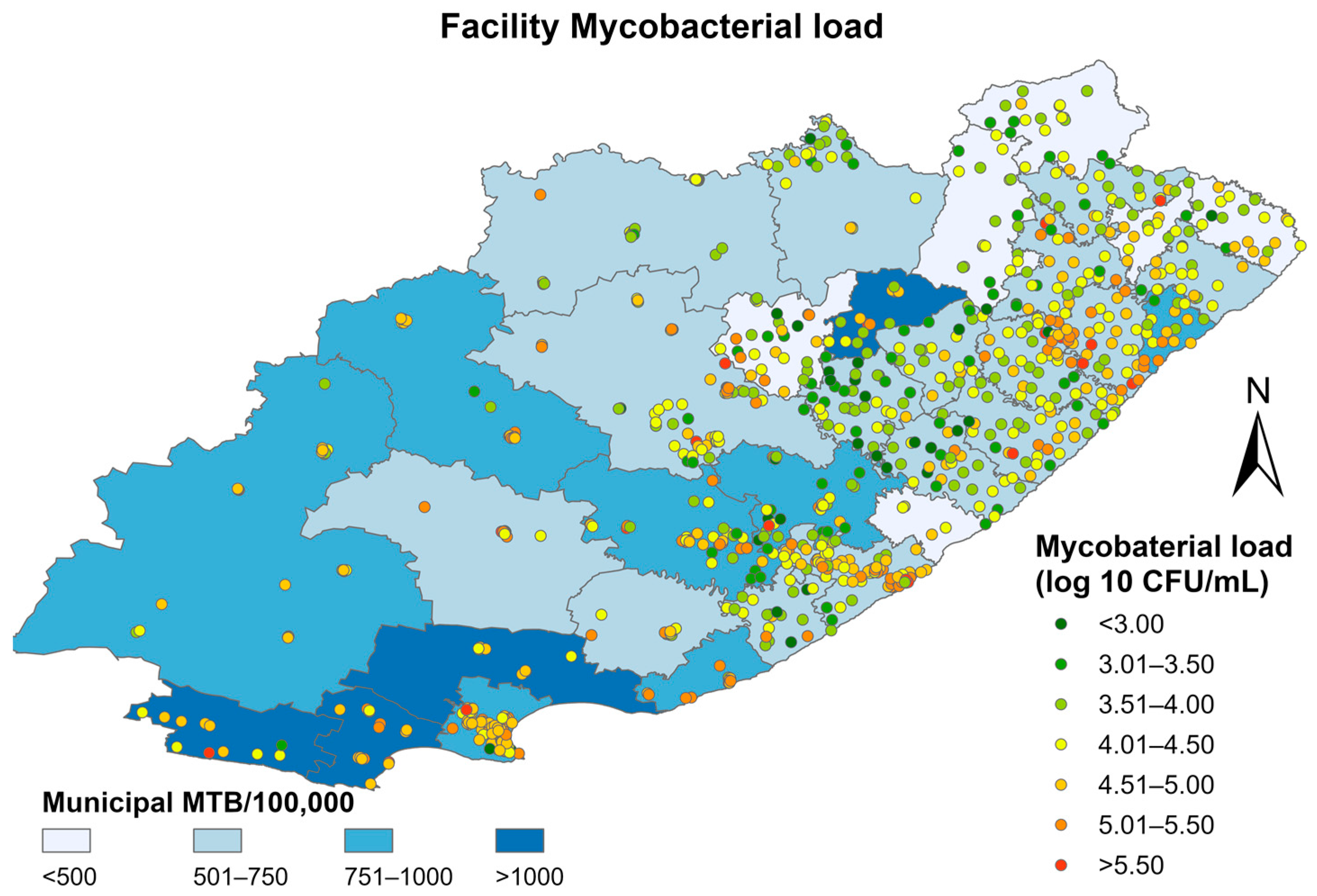
3.2. Spatial and Spatio-Temporal Analyses of Eastern Cape
3.3. Factors Associated with High Mycobacterial Load
3.4. Spatial Analysis of RR Mtb
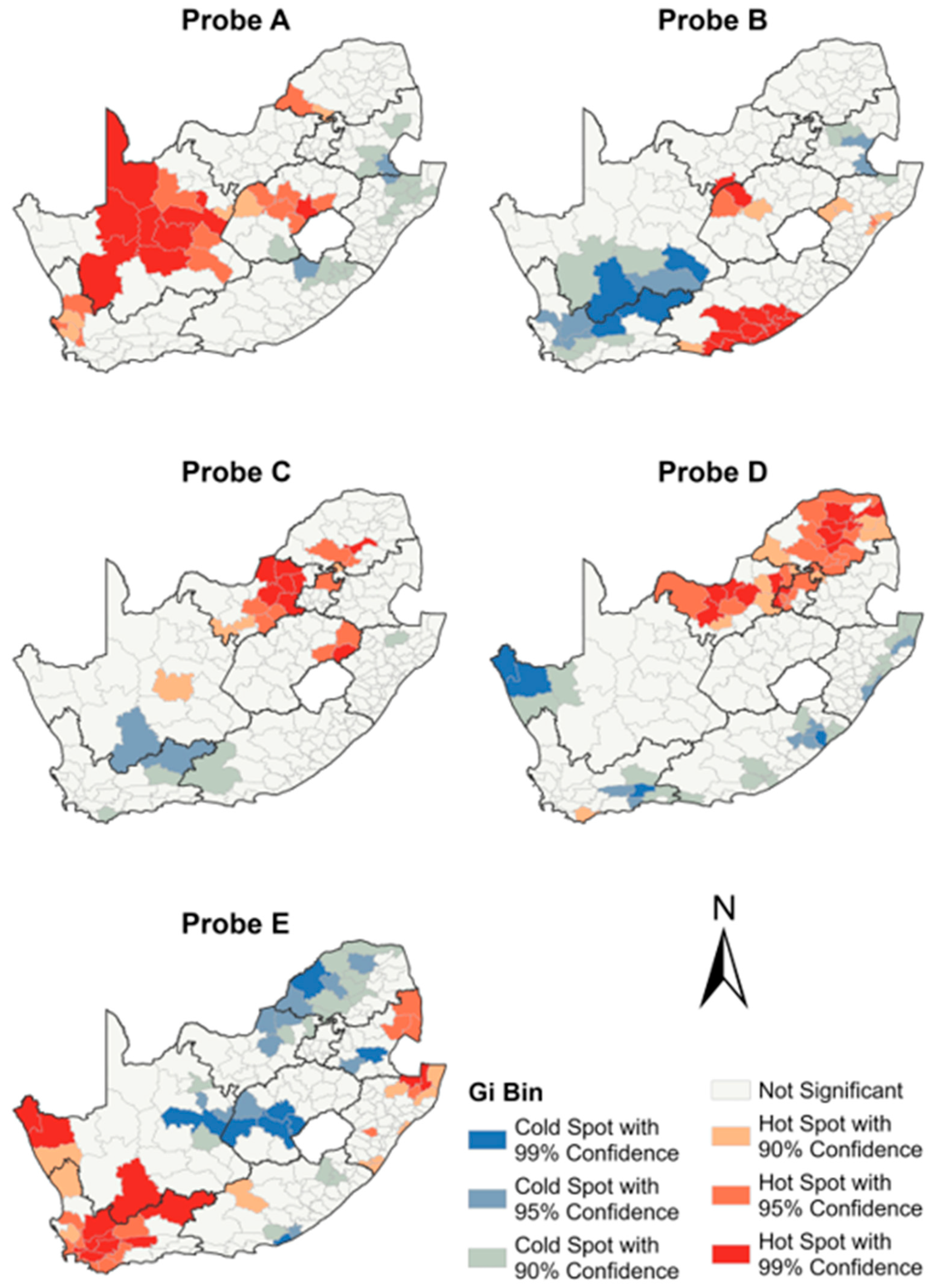
3.5. Spatial Analysis of the Five Xpert MTB/RIF Molecular Probes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Meyer-Rath, G.; Schnippel, K.; Long, L.; MacLeod, W.; Sanne, I.; Stevens, W.; Pillay, S.; Pillay, Y.; Rosen, S. The impact and cost of scaling up GeneXpert MTB/RIF in South Africa. PLoS ONE 2012, 7, e36966. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Communicable Diseases. COVID-19 Surveillance Reports; National Institute for Communicable Diseases: Johannesburg, South Africa, 2023. [Google Scholar]
- Rajendran, P.; Kumar, M.P.; Thiruvengadam, K.; Sreenivasan, P.; Veeraraghavan, T.; Ramalingam, R.; Hasini, S.; Dhanaraju, T.; Kuppamuthu, R.; Shanmugam, S.; et al. Characterization of probes associated with rifampicin resistance in M.tuberculosis detected by GenXpert from a national reference laboratory at Chennai. Tuberc. (Edinb) 2022, 133, 102182. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, H.E.; Gegia, M.; Furin, J.; Kalandadze, I.; Nanava, U.; Chakhaia, T.; Cohen, T. Geographical heterogeneity of multidrug-resistant tuberculosis in Georgia, January 2009 to June 2011. Euro Surveill 2014, 19, 20743. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jenkins, H.E.; Plesca, V.; Ciobanu, A.; Crudu, V.; Galusca, I.; Soltan, V.; Serbulenco, A.; Zignol, M.; Dadu, A.; Dara, M.; et al. Assessing spatial heterogeneity of multidrug-resistant tuberculosis in a high-burden country. Eur. Respir. J. 2013, 42, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Zelner, J.L.; Murray, M.B.; Becerra, M.C.; Galea, J.; Lecca, L.; Calderon, R.; Yataco, R.; Contreras, C.; Zhang, Z.; Manjourides, J.; et al. Identifying Hotspots of Multidrug-Resistant Tuberculosis Transmission Using Spatial and Molecular Genetic Data. J. Infect. Dis. 2016, 213, 287–294. [Google Scholar] [CrossRef]
- McIntosh, A.I.; Jenkins, H.E.; White, L.F.; Barnard, M.; Thomson, D.R.; Dolby, T.; Simpson, J.; Streicher, E.M.; Kleinman, M.B.; Ragan, E.J.; et al. Using routinely collected laboratory data to identify high rifampicin-resistant tuberculosis burden communities in the Western Cape Province, South Africa: A retrospective spatiotemporal analysis. PLoS Med. 2018, 15, e1002638. [Google Scholar] [CrossRef]
- Stevens, W.S.; Cunningham, B.; Cassim, N.; Gous, N.; Scott, L.E. Cloud-Based Surveillance, Connectivity, and Distribution of the GeneXpert Analyzers for Diagnosis of Tuberculosis (TB) and Multiple-Drug-Resistant TB in South Africa. Mol. Microbiol. Diagn. Princ. Pract. 2016, 5, 707–718. [Google Scholar]
- Schnippel, K.; Meyer-Rath, G.; Long, L.; Stevens, W.S.; Sanne, I.; Rosen, S. Diagnosing Xpert MTB/RIF negative TB: Impact and cost of alternative algorithms for South Africa. S. Afr. Med. J. 2013, 103, 101–106. [Google Scholar] [CrossRef]
- Seoudi, N.; Mitchell, S.L.; Brown, T.J.; Dashti, F.; Amin, A.K.; Drobniewski, F.A. Rapid molecular detection of tuberculosis and rifampicin drug resistance: Retrospective analysis of a national U.K. molecular service over the last decade. Thorax 2012, 67, 361–367. [Google Scholar] [CrossRef]
- Shenai, S.; Ronacher, K.; Malherbe, S.; Stanley, K.; Kriel, M.; Winter, J.; Peppard, T.; Barry, C.E.; Wang, J.; Dodd, L.E.; et al. Bacterial Loads Measured by the Xpert MTB/RIF Assay as Markers of Culture Conversion and Bacteriological Cure in Pulmonary TB. PLoS ONE 2016, 11, e0160062. [Google Scholar] [CrossRef]
- Hanrahan, C.F.; Theron, G.; Bassett, J.; Dheda, K.; Scott, L.; Stevens, W.; Sanne, I.; Van Rie, A. Xpert MTB/RIF as a measure of sputum bacillary burden. Variation by HIV status and immunosuppression. Am. J. Respir. Crit. Care Med. 2014, 189, 1426–1434. [Google Scholar] [CrossRef] [PubMed]
- Azam, K.; Cadir, N.; Madeira, C.; Gillespie, S.H.; Sabiiti, W. OMNIgene.SPUTUM suppresses contaminants while maintaining Mycobacterium tuberculosis viability and obviates cold-chain transport. ERJ Open Res. 2018, 4, 00074-2017. [Google Scholar] [CrossRef]
- Beynon, F.; Theron, G.; Respeito, D.; Mambuque, E.; Saavedra, B.; Bulo, H.; Sanz, S.; Dheda, K.; Garcia-Basteiro, A.L. Correlation of Xpert MTB/RIF with measures to assess Mycobacterium tuberculosis bacillary burden in high HIV burden areas of Southern Africa. Sci. Rep. 2018, 8, 5201. [Google Scholar] [CrossRef] [PubMed]
- Alemu, A.; Tadesse, M.; Seid, G.; Mollalign, H.; Eshetu, K.; Sinshaw, W.; Abebaw, Y.; Amare, M.; Dagne, B.; Diriba, G.; et al. Does Xpert(R) MTB/RIF assay give rifampicin resistance results without identified mutation? Review of cases from Addis Ababa, Ethiopia. BMC Infect. Dis. 2020, 20, 87. [Google Scholar] [CrossRef] [PubMed]
- Ochang, E.A.; Udoh, U.A.; Emanghe, U.E.; Tiku, G.O.; Offor, J.B.; Odo, M.; Nkombe, E.; Owuna, O.E.; Obeten, S.M.; Meremikwu, M.M. Evaluation of rifampicin resistance and 81-bp rifampicin resistant determinant region of rpoB gene mutations of Mycobacterium tuberculosis detected with XpertMTB/Rif in Cross River State, Nigeria. Int. J. Mycobacteriol. 2016, 5 (Suppl. S1), S145–S146. [Google Scholar] [CrossRef]
- Link, B.G.; Phelan, J. Social conditions as fundamental causes of disease. J. Health Soc. Behav. 1995, 36, 80–94. [Google Scholar] [CrossRef]
- Clouston, S.A.; Link, B.G.; Link, B.G. A retrospective on fundamental cause theory: State of the literature, and goals for the future. Annu. Rev. Sociol. 2021, 47, 131–156. [Google Scholar] [CrossRef]
- Municipal Demarcation Board. 2021. Available online: https://www.demarcation.org.za/ (accessed on 10 October 2022).
- Africa, S.S. The South Africa I Know, The Home I Understand. 2022. Available online: https://www.statssa.gov.za/ (accessed on 10 October 2022).
- Blakemore, R.; Nabeta, P.; Davidow, A.L.; Vadwai, V.; Tahirli, R.; Munsamy, V.; Nicol, M.; Jones, M.; Persing, D.H.; Hillemann, D.; et al. A multisite assessment of the quantitative capabilities of the Xpert MTB/RIF assay. Am. J. Respir. Crit. Care Med. 2011, 184, 1076–1084. [Google Scholar] [CrossRef]
- Lange, B.; Khan, P.; Kalmambetova, G.; Al-Darraji, H.A.; Alland, D.; Antonenka, U.; Brown, T.; Balcells, M.E.; Blakemore, R.; Denkinger, C.M.; et al. Diagnostic accuracy of the Xpert((R)) MTB/RIF cycle threshold level to predict smear positivity: A meta-analysis. Int. J. Tuberc. Lung Dis. 2017, 21, 493–502. [Google Scholar] [CrossRef]
- Nykiforuk, C.; Flaman, L.M. Exploring the Utilization of Geographic Information Systems in Health Promotion and Public Health; University of Alberta: Edmonton, AB, Canada, 2008. [Google Scholar]
- Alene, K.A.; Viney, K.; McBryde, E.S.; Clements, A.C. Spatial patterns of multidrug resistant tuberculosis and relationships to socio-economic, demographic and household factors in northwest Ethiopia. PLoS ONE 2017, 12, e0171800. [Google Scholar] [CrossRef]
- Ge, E.; Zhang, X.; Wang, X.; Wei, X. Spatial and temporal analysis of tuberculosis in Zhejiang Province, China, 2009–2012. Infect Dis. Poverty 2016, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, X.; Wang, W.; Li, Z.; Hou, M.; He, Y.; Wu, W.; Wang, H.; Liang, H.; Guo, X. Investigation of space-time clusters and geospatial hot spots for the occurrence of tuberculosis in Beijing. Int. J. Tuberc. Lung Dis. 2012, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef]
- Marx, F.M.; Yaesoubi, R.; Menzies, N.A.; Salomon, J.A.; Bilinski, A.; Beyers, N.; Cohen, T. Tuberculosis control interventions targeted to previously treated people in a high-incidence setting: A modelling study. Lancet Glob. Health 2018, 6, e426–e435. [Google Scholar] [CrossRef] [PubMed]
- Marx, F.M.; Cohen, T.; Lombard, C.; Hesseling, A.C.; Dlamini, S.S.; Beyers, N.; Naidoo, P. Notification of relapse and other previously treated tuberculosis in the 52 health districts of South Africa. Int. J. Tuberc. Lung Dis. 2019, 23, 891–899. [Google Scholar] [CrossRef]
- Trauer, J.M.; Dodd, P.J.; Gomes, M.G.M.; Gomez, G.B.; Houben, R.M.; McBryde, E.S.; Melsew, Y.A.; Menzies, N.A.; Arinaminpathy, N.; Shrestha, S.; et al. The Importance of Heterogeneity to the Epidemiology of Tuberculosis. Clin. Infect Dis. 2019, 69, 159–166. [Google Scholar] [CrossRef]
- Tadokera, R.; Bekker, L.G.; Kreiswirth, B.N.; Mathema, B.; Middelkoop, K. TB transmission is associated with prolonged stay in a low socio-economic, high burdened TB and HIV community in Cape Town, South Africa. BMC Infect Dis. 2020, 20, 120. [Google Scholar] [CrossRef]
- Gaiha, S.M.; Gadin, K.G. No time for health:’ exploring couples’ health promotion in Indian slums. Health Promot Int. 2020, 35, 70–81. [Google Scholar] [CrossRef]
- Bonadonna, L.V.; Saunders, M.J.; Zegarra, R.; Evans, C.; Alegria-Flores, K.; Guio, H. Why wait? The social determinants underlying tuberculosis diagnostic delay. PLoS ONE 2017, 12, e0185018. [Google Scholar] [CrossRef]
- Jenkins, H.E.; Ayuk, S.; Puma, D.; Brooks, M.B.; Millones, A.K.; Jimenez, J.; Lecca, L.; Galea, J.T.; Becerra, M.; Keshavjee, S.; et al. Geographic accessibility to health facilities predicts uptake of community-based tuberculosis screening in an urban setting. Int. J. Infect Dis. 2022, 120, 125–131. [Google Scholar] [CrossRef]
- Kaur, R.; Jindal, N.; Arora, S.; Kataria, S. Epidemiology of Rifampicin Resistant Tuberculosis and Common Mutations in rpoB Gene of Mycobacterium tuberculosis: A Retrospective Study from Six Districts of Punjab (India) Using Xpert MTB/RIF Assay. J. Lab. Physicians 2016, 8, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Ullah, I.; Shah, A.A.; Basit, A.; Ali, M.; Ullah, U.; Ihtesham, M.; Mehreen, S.; Mughal, A.; Javaid, A. Rifampicin resistance mutations in the 81 bp RRDR of rpoB gene in Mycobacterium tuberculosis clinical isolates using Xpert MTB/RIF in Khyber Pakhtunkhwa, Pakistan: A retrospective study. BMC Infect Dis. 2016, 16, 413. [Google Scholar] [CrossRef] [PubMed]
- Billington, O.J.; McHugh, T.D.; Gillespie, S.H. Physiological cost of rifampin resistance induced in vitro in Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 1999, 43, 1866–1869. [Google Scholar] [CrossRef]
- Musser, J.M. Antimicrobial agent resistance in mycobacteria: Molecular genetic insights. Clin. Microbiol. Rev. 1995, 8, 496–514. [Google Scholar] [CrossRef]
- Wolf, A.; Padayatchi, N.; Naidoo, K.; Master, I.; Mathema, B.; O’donnell, M.R. Spatiotemporal Clustering of Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis Is Associated With Human Immunodeficiency Virus Status and Drug-Susceptibility Patterns in KwaZulu-Natal, South Africa. Clin. Infect Dis. 2020, 70, 2224–2227. [Google Scholar] [CrossRef]
- Sy, K.T.L.; Leavitt, S.V.; de Vos, M.; Dolby, T.; Bor, J.; Horsburgh, C.R., Jr.; Warren, R.M.; Streicher, E.M.; Jenkins, H.E.; Jacobson, K.R. Spatial heterogeneity of extensively drug resistant-tuberculosis in Western Cape Province, South Africa. Sci. Rep. 2022, 12, 10844. [Google Scholar] [CrossRef]
- Mashamba, M.A.; Tanser, F.; Afagbedzi, S.; Beke, A. Multi-drug-resistant tuberculosis clusters in Mpumalanga province, South Africa, 2013–2016: A spatial analysis. Trop. Med. Int. Health 2022, 27, 185–191. [Google Scholar] [CrossRef]
- Green, E.; Obi, C.L.; Nchabeleng, M.; De Villiers, B.E.; Sein, P.P.; Letsoalo, T.; Hoosen, A.A.; Bessong, P.O.; Ndip, R.N. Drug-susceptibility patterns of Mycobacterium tuberculosis in Mpumalanga province, South Africa: Possible guiding design of retreatment regimen. J. Health Popul. Nutr. 2010, 28, 7–13. [Google Scholar]
- Sanchez-Padilla, E.; Merker, M.; Beckert, P.; Jochims, F.; Dlamini, T.; Kahn, P.; Bonnet, M.; Niemann, S. Detection of drug-resistant tuberculosis by Xpert MTB/RIF in Swaziland. N. Engl. J. Med. 2015, 372, 1181–1182. [Google Scholar] [CrossRef]
- Shah, N.S.; Auld, S.C.; Brust, J.C.; Mathema, B.; Ismail, N.; Moodley, P.; Mlisana, K.; Allana, S.; Campbell, A.; Mthiyane, T.; et al. Transmission of Extensively Drug-Resistant Tuberculosis in South Africa. N. Engl. J. Med. 2017, 376, 243–253. [Google Scholar] [CrossRef]
- Bor, J.; MacLeod, W.; Oleinik, K.; Potter, J.; Brennan, A.T.; Candy, S.; Maskew, M.; Fox, M.P.; Sanne, I.; Stevens, W.S.; et al. Building a National HIV Cohort from Routine Laboratory Data: Probabilistic Record-Linkage with Graphs. BioRxiv 2018. [Google Scholar] [CrossRef]
- Bor, J.; Harling, G.; Tanser, F.; Newell, M.-L.; Barnighausen, T.; Mutevedzi, T.; Pillay, D.; Herbst, K.; Bärnighausen, T. Building a national TB cohort from routine laboratory data: Record linkage in South Africa. In Proceedings of the 52nd Union World Conference on Lung Health, Virtual, 19–22 October 2021. [Google Scholar]
- Mekonnen, D.; Munshea, A.; Nibret, E.; Adnew, B.; Herrera-Leon, S.; Aramendia, A.A.; Benito, A.; Abascal, E.; Jacqueline, C.; Aseffa, A.; et al. Comparative whole-genome sequence analysis of Mycobacterium tuberculosis isolated from pulmonary tuberculosis and tuberculous lymphadenitis patients in Northwest Ethiopia. Front. Microbiol. 2023, 14, 1211267. [Google Scholar] [CrossRef] [PubMed]
- Shibabaw, A.; Gelaw, B.; Ghanem, M.; Legall, N.; Schooley, A.M.; Soehnlen, M.K.; Salvador, L.C.; Gebreyes, W.; Wang, S.H.; Tessema, B. Molecular epidemiology and transmission dynamics of multi-drug resistant tuberculosis strains using whole genome sequencing in the Amhara region, Ethiopia. BMC Genom. 2023, 24, 400. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.E.; Noble, L.D.; Singh-Moodley, A.; Kahamba, T.; Hardie, D.R.; Preiser, W.; Stevens, W.S. Challenges and complexities inevaluating severe acute respiratory syndrome coronavirus 2 molecular diagnostics during the COVID-19 pandemic. Afr. J. Lab. Med. 2022, 11, 1429. [Google Scholar] [CrossRef]
- Namugenyi, J.; Musaazi, J.; Katamba, A.; Kalyango, J.; Sendaula, E.; Kambugu, A.; Fehr, J.; Castelnouvo, B.; Manabe, Y.C.; Ssengooba, W.; et al. Baseline Xpert MTB/RIF ct values predict sputum conversion during the intensive phase of anti-TB treatment in HIV infected patients in Kampala, Uganda: A retrospective study. BMC Infect. Dis. 2021, 21, 513. [Google Scholar] [CrossRef]
- Scott, L.E.; Hsiao, N.Y.; Dor, G.; Hans, L.; Marokane, P.; da Silva, M.P.; Preiser, W.; Vreede, H.; Tsoka, J.; Mlisana, K.; et al. How South Africa Used National Cycle Threshold (Ct) Values to Continuously Monitor SARS-CoV-2 Laboratory Test Quality. Diagnostics 2023, 13, 2554. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Province | Number of Mtb Tests Performed | Number of Positive Mtb Tests | MTB Test Positivity (%) |
|---|---|---|---|
| Eastern Cape | 2,202,856 | 232,549 | 10.6 |
| Free State | 640,096 | 62,616 | 9.8 |
| Gauteng | 1,716,034 | 171,718 | 10 |
| KwaZulu Natal | 2,830,422 | 252,877 | 8.9 |
| Limpopo | 1,111,262 | 63,749 | 5.7 |
| Mpumalanga | 570,906 | 61,288 | 10.7 |
| North West | 765,694 | 70,987 | 9.3 |
| Northern Cape | 372,170 | 41,418 | 11.1 |
| Western Cape | 1,135,664 | 167,793 | 14.8 |
| Variable | 95% CI | p-Value |
|---|---|---|
| Median patient age | 0.86 (0.82–1.02) | 0.043 |
| Number of non-specified HCWs | 0.69 (0.46–0.89) | 0.007 |
| Land use class (Urban) | 82.43 (5.09–1334.23) | 0.001 |
| Province | Number of Mtb Tests Performed Reporting RR | Rate of RIF Positive Mtb Tests (%) |
|---|---|---|
| Eastern Cape | 13,971 | 6 |
| Free State | 3387 | 5.4 |
| Gauteng | 10,158 | 5.9 |
| KwaZulu Natal | 20,505 | 8.1 |
| Limpopo | 3363 | 5.3 |
| Mpumalanga | 5114 | 8.4 |
| North West | 3569 | 5 |
| Northern Cape | 2198 | 5.3 |
| Western Cape | 8331 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scott, L.E.; Shapiro, A.N.; Da Silva, M.P.; Tsoka, J.; Jacobson, K.R.; Emch, M.; Moultrie, H.; Jenkins, H.E.; Moore, D.; Van Rie, A.; et al. Integrating Molecular Diagnostics and GIS Mapping: A Multidisciplinary Approach to Understanding Tuberculosis Disease Dynamics in South Africa Using Xpert MTB/RIF. Diagnostics 2023, 13, 3163. https://doi.org/10.3390/diagnostics13203163
Scott LE, Shapiro AN, Da Silva MP, Tsoka J, Jacobson KR, Emch M, Moultrie H, Jenkins HE, Moore D, Van Rie A, et al. Integrating Molecular Diagnostics and GIS Mapping: A Multidisciplinary Approach to Understanding Tuberculosis Disease Dynamics in South Africa Using Xpert MTB/RIF. Diagnostics. 2023; 13(20):3163. https://doi.org/10.3390/diagnostics13203163
Chicago/Turabian StyleScott, Lesley Erica, Anne Nicole Shapiro, Manuel Pedro Da Silva, Jonathan Tsoka, Karen Rita Jacobson, Michael Emch, Harry Moultrie, Helen Elizabeth Jenkins, David Moore, Annelies Van Rie, and et al. 2023. "Integrating Molecular Diagnostics and GIS Mapping: A Multidisciplinary Approach to Understanding Tuberculosis Disease Dynamics in South Africa Using Xpert MTB/RIF" Diagnostics 13, no. 20: 3163. https://doi.org/10.3390/diagnostics13203163
APA StyleScott, L. E., Shapiro, A. N., Da Silva, M. P., Tsoka, J., Jacobson, K. R., Emch, M., Moultrie, H., Jenkins, H. E., Moore, D., Van Rie, A., & Stevens, W. S. (2023). Integrating Molecular Diagnostics and GIS Mapping: A Multidisciplinary Approach to Understanding Tuberculosis Disease Dynamics in South Africa Using Xpert MTB/RIF. Diagnostics, 13(20), 3163. https://doi.org/10.3390/diagnostics13203163