
3D Reconstruction of Wrist Bones from C-Arm Fluoroscopy Using Planar Markers

Abstract
1. Introduction
2. Materials and Methods
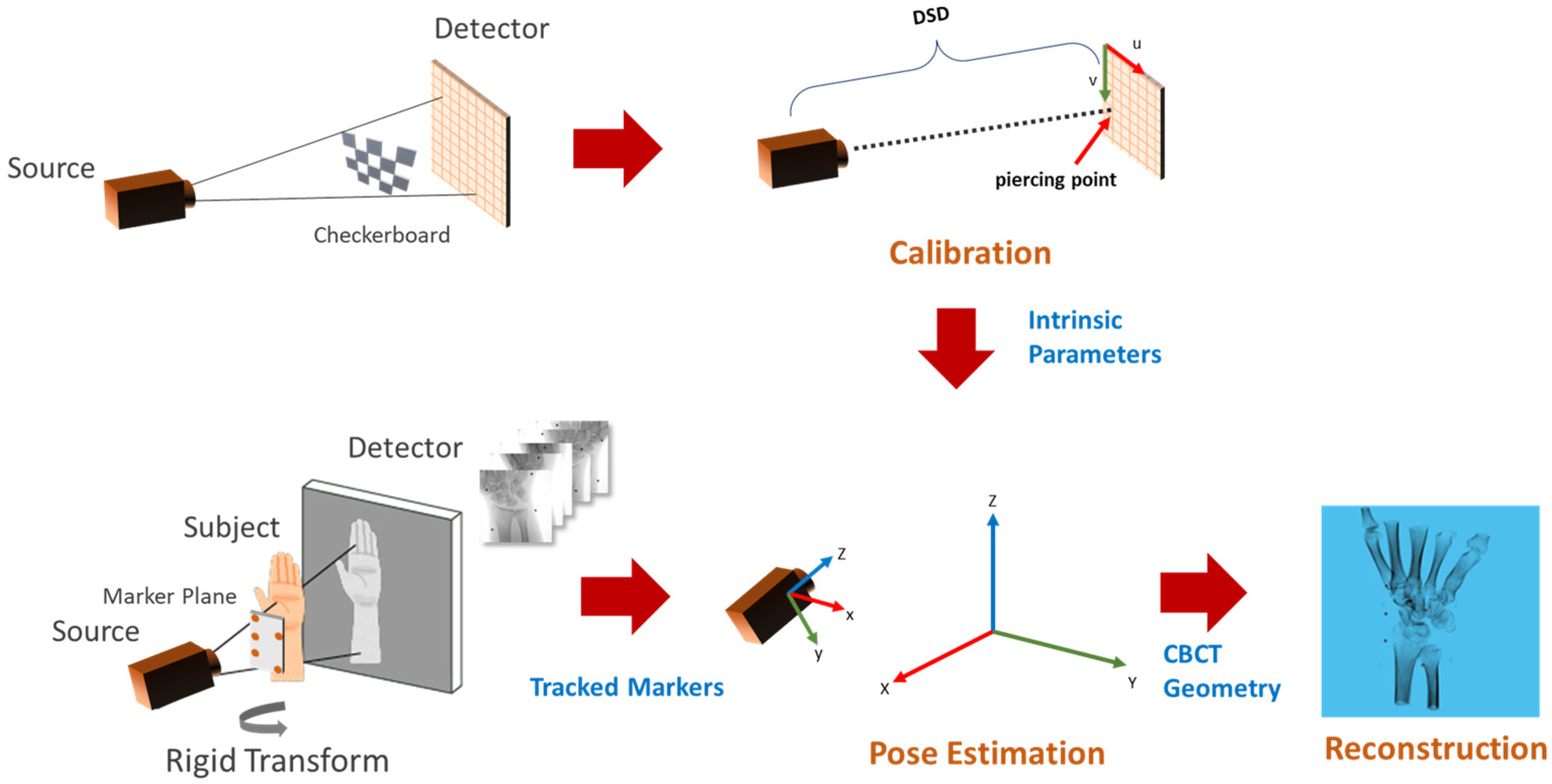
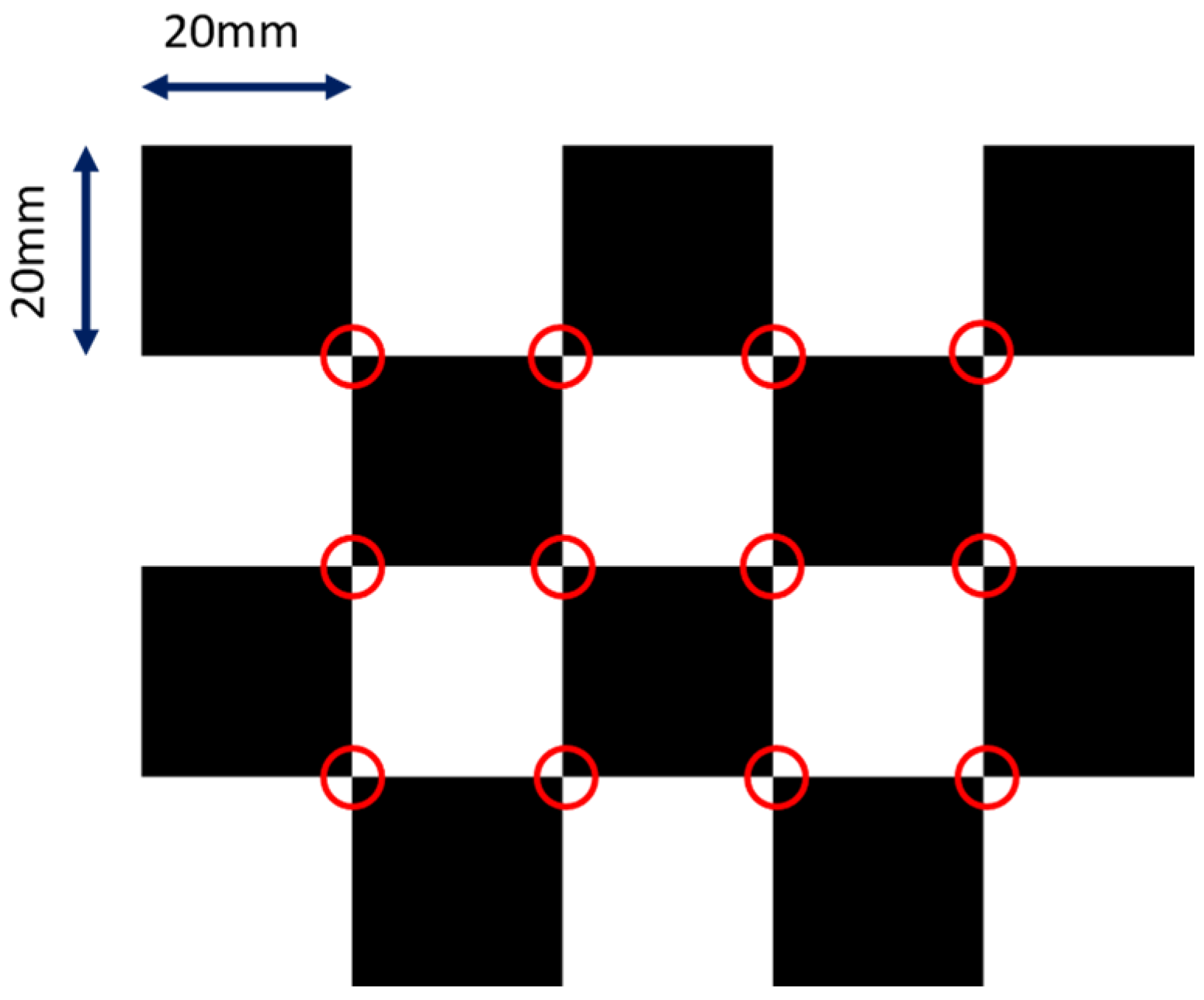
2.1. C-Arm Calibration
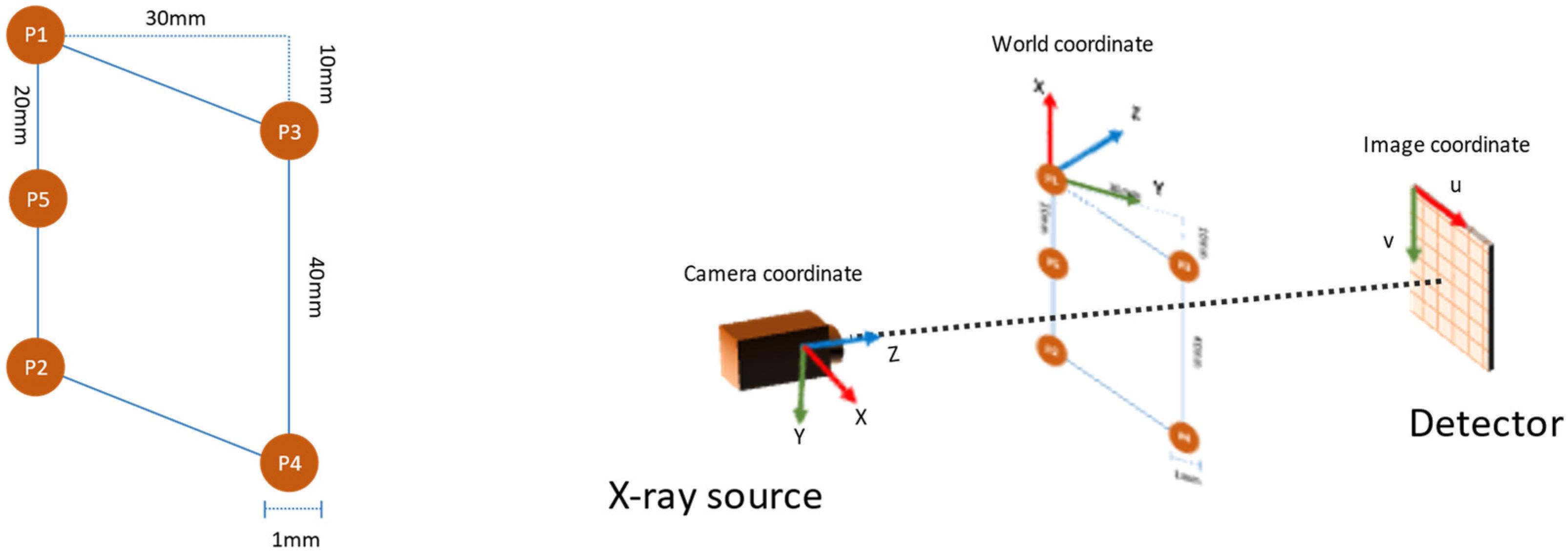
2.2. Pose Estimation
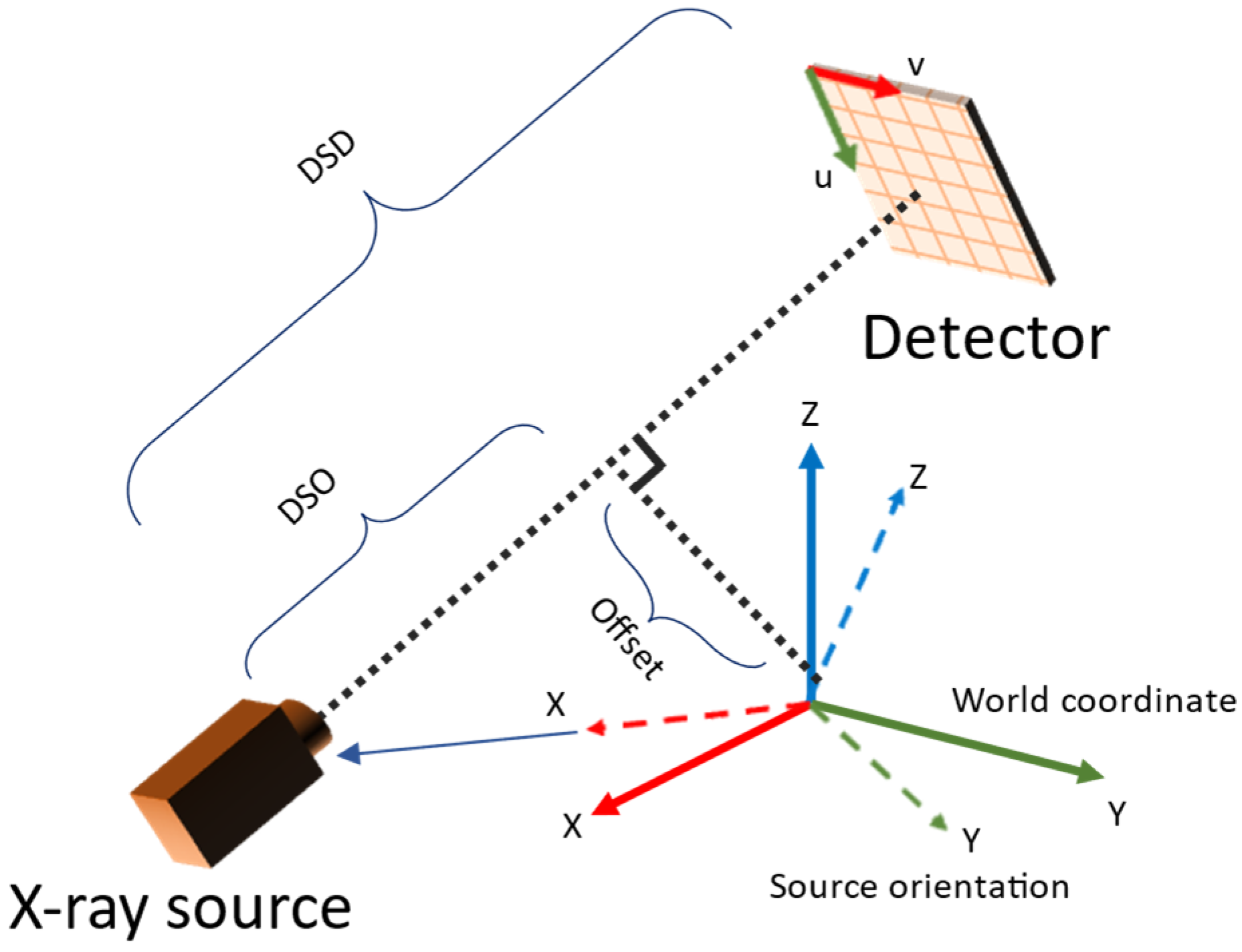
2.3. Reconstruction
3. Experiments and Results
3.1. Simulation Setup
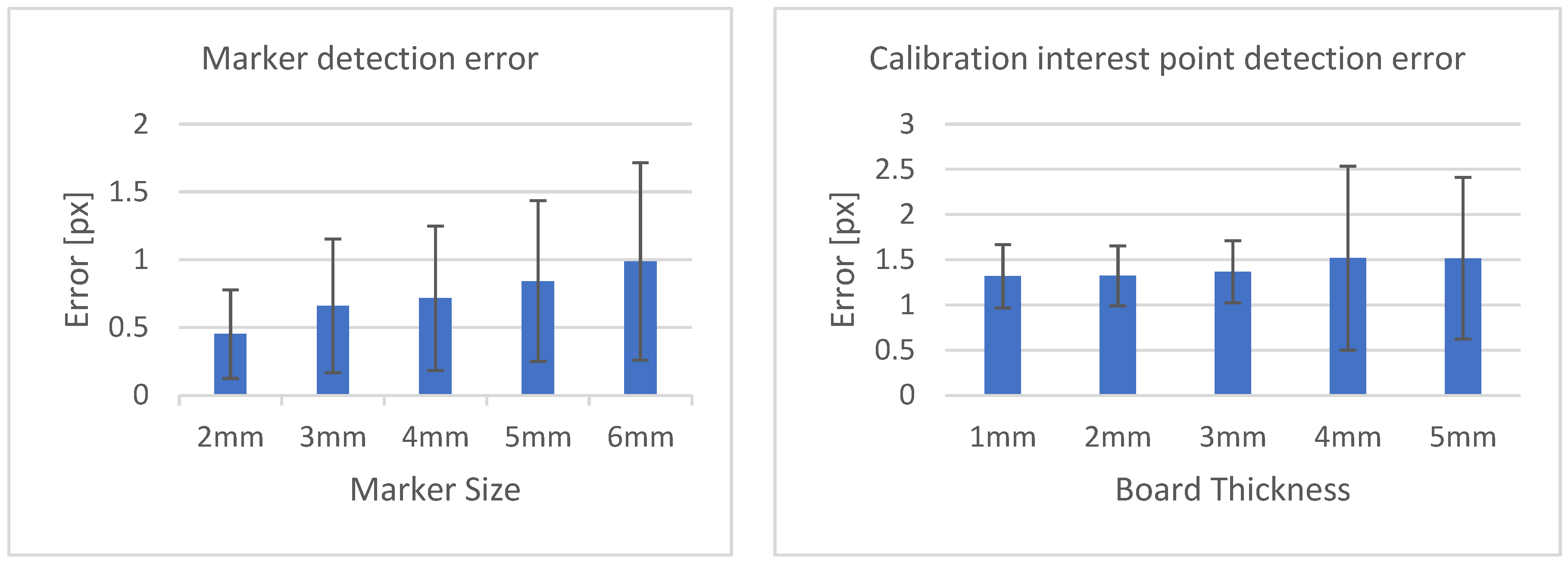
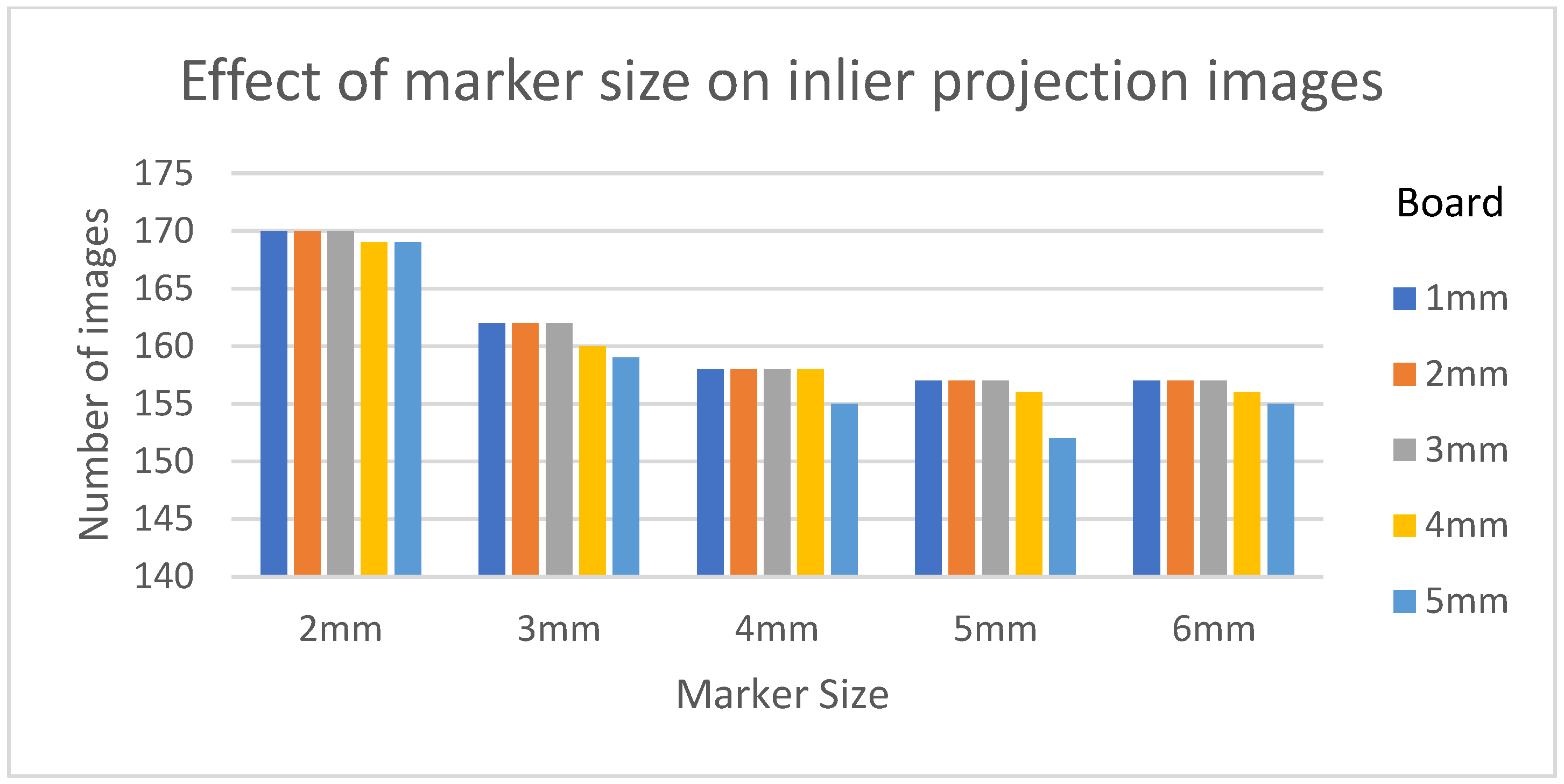
3.2. Effect of Board Thicknesses and Marker Sizes on Reconstructed Image Quality
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keil, H.; Trapp, O. Fluoroscopic Imaging: New Advances. Injury 2022, 53 (Suppl. 3), S8–S15. [Google Scholar] [CrossRef]
- Merloz, P.; Troccaz, J.; Vouaillat, H.; Vasile, C.; Tonetti, J.; Eid, A.; Plaweski, S. Fluoroscopy-Based Navigation System in Spine Surgery. Proc. Inst. Mech. Eng. H 2007, 221, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, Y.; Kusakabe, T.; Akita, K.; Tung, W.L.; Ishii, T. Reproducibility of Three Dimensional Digital Preoperative Planning for the Osteosynthesis of Distal Radius Fractures. J. Orthop. Res. 2017, 35, 2646–2651. [Google Scholar] [CrossRef]
- Harris, E.; Atthakomol, P.; Korteweg, J.; Li, G.; Hosseini, A.; Kachooei, A.; Chen, N.C. Non-Invasive 3D Fluoroscopic/CT Imaging of the Wrist. Orthop. J. Harv. Med. Sch. 2021, 22, 40–48. [Google Scholar]
- Wylie, J.D.; Ross, J.A.; Erickson, J.A.; Anderson, M.B.; Peters, C.L. Operative Fluoroscopic Correction Is Reliable and Correlates with Postoperative Radiographic Correction in Periacetabular Osteotomy. Clin. Orthop. Relat. Res. 2017, 475, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
- Reichert, J.C.; Hofer, A.; Matziolis, G.; Wassilew, G.I. Intraoperative Fluoroscopy Allows the Reliable Assessment of Deformity Correction during Periacetabular Osteotomy. J. Clin. Med. Res. 2022, 11, 4817. [Google Scholar] [CrossRef]
- Selles, C.A.; Beerekamp, M.S.H.; Leenhouts, P.A.; Segers, M.J.M.; Goslings, J.C.; Schep, N.W.L.; EF3X Study Group. The Value of Intraoperative 3-Dimensional Fluoroscopy in the Treatment of Distal Radius Fractures: A Randomized Clinical Trial. J. Hand Surg. Am. 2020, 45, 189–195. [Google Scholar] [CrossRef]
- Markelj, P.; Tomaževič, D.; Likar, B.; Pernuš, F. A Review of 3D/2D Registration Methods for Image-Guided Interventions. Med. Image Anal. 2012, 16, 642–661. [Google Scholar] [CrossRef]
- Posadzy, M.; Desimpel, J.; Vanhoenacker, F. Cone Beam CT of the Musculoskeletal System: Clinical Applications. Insights Imaging 2018, 9, 35–45. [Google Scholar] [CrossRef]
- Schonberger, J.L.; Frahm, J.-M. Structure-from-Motion Revisited. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 4104–4113. [Google Scholar]
- Cheung, G.K.; Baker, S.; Kanade, T. Shape-From-Silhouette Across Time Part I: Theory and Algorithms. Int. J. Comput. Vis. 2005, 62, 221–247. [Google Scholar] [CrossRef]
- Feldkamp, L.A.; Davis, L.C.; Kress, J.W. Practical Cone-Beam Algorithm. J. Opt. Soc. Am. A JOSAA 1984, 1, 612–619. [Google Scholar] [CrossRef]
- Andersen, A.H.; Kak, A.C. Simultaneous Algebraic Reconstruction Technique (SART): A Superior Implementation of the ART Algorithm. Ultrason. Imaging 1984, 6, 81–94. [Google Scholar] [CrossRef]
- Baka, N.; Kaptein, B.L.; de Bruijne, M.; van Walsum, T.; Giphart, J.E.; Niessen, W.J.; Lelieveldt, B.P.F. 2D-3D Shape Reconstruction of the Distal Femur from Stereo X-Ray Imaging Using Statistical Shape Models. Med. Image Anal. 2011, 15, 840–850. [Google Scholar] [CrossRef]
- Zheng, G. Personalized X-ray Reconstruction of the Proximal Femur via Intensity-Based Non-Rigid 2D-3D Registration. Med. Image Comput. Comput. Assist. Interv. 2011, 14, 598–606. [Google Scholar] [PubMed]
- Yu, W.; Chu, C.; Tannast, M.; Zheng, G. Fully Automatic Reconstruction of Personalized 3D Volumes of the Proximal Femur from 2D X-ray Images. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1673–1685. [Google Scholar] [CrossRef]
- Ying, X.; Guo, H.; Ma, K.; Wu, J.; Weng, Z.; Zheng, Y. X2CT-GAN: Reconstructing CT from Biplanar X-rays with Generative Adversarial Networks. In Proceedings of the 2019 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 15–20 June 2019; pp. 10611–10620. [Google Scholar] [CrossRef]
- Vachon, É.; Miró, J.; Duong, L. Online C-Arm Calibration Using a Marked Guide Wire for 3D Reconstruction of Pulmonary Arteries. In Proceedings of the Medical Imaging 2017: Image-Guided Procedures, Robotic Interventions, and Modeling, Orlando, FL, USA, 11–16 February 2017; Webster, R.J., Fei, B., Eds.; SPIE: Bellingham, WA, USA, 2017. [Google Scholar]
- Albiol, F.; Corbi, A.; Albiol, A. Geometrical Calibration of X-ray Imaging With RGB Cameras for 3D Reconstruction. IEEE Trans. Med. Imaging 2016, 35, 1952–1961. [Google Scholar] [CrossRef]
- Kalmykova, M.; Poyda, A.; Ilyin, V. An Approach to Point-to-Point Reconstruction of 3D Structure of Coronary Arteries from 2D X-ray Angiography, Based on Epipolar Constraints. Procedia Comput. Sci. 2018, 136, 380–389. [Google Scholar] [CrossRef]
- Pande, K.; Donatelli, J.J.; Parkinson, D.Y.; Yan, H.; Sethian, J.A. Joint Iterative Reconstruction and 3D Rigid Alignment for X-ray Tomography. Opt. Express 2022, 30, 8898–8916. [Google Scholar] [CrossRef]
- Abella, M.; de Molina, C.; Ballesteros, N.; García-Santos, A.; Martínez, Á.; García, I.; Desco, M. Enabling Tomography with Low-Cost C-Arm Systems. PLoS ONE 2018, 13, e0203817. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Moseley, D.J.; Siewerdsen, J.H.; Jaffray, D.A. Accurate Technique for Complete Geometric Calibration of Cone-Beam Computed Tomography Systems. Med. Phys. 2005, 32, 968–983. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z. A Flexible New Technique for Camera Calibration. IEEE Trans. Pattern Anal. Mach. Intell. 2000, 22, 1330–1334. [Google Scholar] [CrossRef]
- Biguri, A.; Dosanjh, M.; Hancock, S.; Soleimani, M. TIGRE: A MATLAB-GPU Toolbox for CBCT Image Reconstruction. Biomed. Phys. Eng. Express 2016, 2, 055010. [Google Scholar] [CrossRef]
- Yoshii, Y.; Teramura, S.; Oyama, K.; Ogawa, T.; Hara, Y.; Ishii, T. Development of three-dimensional preoperative planning system for the osteosynthesis of distal humerus fractures. BioMed Eng. Online 2020, 19, 56. [Google Scholar] [CrossRef]
- Yoshii, Y.; Ogawa, T.; Hara, Y.; Totoki, Y.; Ishii, T. An image fusion system for corrective osteotomy of distal radius malunion. BioMed Eng. Online 2021, 20, 66. [Google Scholar] [CrossRef]
- Lu, X.X. A Review of Solutions for Perspective-n-Point Problem in Camera Pose Estimation. J. Phys. Conf. Ser. 2018, 1087, 052009. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter Name | Description |
|---|---|
| DSD | Distance between the X-ray source and detector plane |
| DSO | Distance between the X-ray source and world origin |
| offOrigin | Offset applied to the volume in world origin |
| offDetector | Offset applied to the detector |
| angles | The angle of X-ray source from world origin in ZYZ convention |
| nVoxel | Number of voxels in the volume |
| dVoxel | Size of one voxel in the world coordinate |
| sVoxel | Total size occupied by the volume in the world coordinate |
| nDetector | Number of pixels in the detector panel |
| sDetector | The total size of the detector panel in the world coordinate |
| Parameter Name | Value |
|---|---|
| DSD | 780 mm |
| DSO | 390 mm |
| offOrigin | (0, 0, 0) |
| offDetector | (0, 0) |
| Angles | 180 samples between 0 and 180 degrees |
| nDetector | (1024 px, 1024 px) |
| sDetector | 210 mm |
| Calibration Board | |
| nVoxel [vx] | (500, 500, 500) |
| dVoxel [mm/vx] | (0.25, 0.25, 0.25) |
| sVoxel [mm] | (100, 100, 100) |
| CT Volume for Simulated X-ray | |
| nVoxel [vx] | (604, 604, 644) |
| dVoxel [mm/vx] | (0.25, 0.25, 0.25) |
| sVoxel [mm] | (151, 151, 161) |
| Reconstruction Volume | |
| nVoxel [vx] | (300, 300, 300) |
| dVoxel [mm/vx] | (0.5, 0.5, 0.5) |
| sVoxel [mm] | (150, 150, 150) |
| Board Thickness/Marker Size | 2 mm | 3 mm | 4 mm | 5 mm | 6 mm |
|---|---|---|---|---|---|
| 1 mm | 0.9435 | 0.9205 | 0.9235 | 0.9120 | 0.9114 |
| 2 mm | 0.9437 | 0.9206 | 0.9236 | 0.9122 | 0.9111 |
| 3 mm | 0.9441 | 0.9206 | 0.9237 | 0.9125 | 0.9107 |
| 4 mm | 0.9426 | 0.9225 | 0.9236 | 0.9116 | 0.9043 |
| 5 mm | 0.9352 | 0.9218 | 0.9221 | 0.9107 | 0.8982 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shrestha, P.; Xie, C.; Shishido, H.; Yoshii, Y.; Kitahara, I. 3D Reconstruction of Wrist Bones from C-Arm Fluoroscopy Using Planar Markers. Diagnostics 2023, 13, 330. https://doi.org/10.3390/diagnostics13020330
Shrestha P, Xie C, Shishido H, Yoshii Y, Kitahara I. 3D Reconstruction of Wrist Bones from C-Arm Fluoroscopy Using Planar Markers. Diagnostics. 2023; 13(2):330. https://doi.org/10.3390/diagnostics13020330
Chicago/Turabian StyleShrestha, Pragyan, Chun Xie, Hidehiko Shishido, Yuichi Yoshii, and Itaru Kitahara. 2023. "3D Reconstruction of Wrist Bones from C-Arm Fluoroscopy Using Planar Markers" Diagnostics 13, no. 2: 330. https://doi.org/10.3390/diagnostics13020330
APA StyleShrestha, P., Xie, C., Shishido, H., Yoshii, Y., & Kitahara, I. (2023). 3D Reconstruction of Wrist Bones from C-Arm Fluoroscopy Using Planar Markers. Diagnostics, 13(2), 330. https://doi.org/10.3390/diagnostics13020330