
The Diagnosis of Malignant Pleural Effusion Using Tumor-Marker Combinations: A Cost-Effectiveness Analysis Based on a Stacking Model

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Diagnostic Criteria
2.2. Specimen Collection and Measurement
2.3. The Construction of Stacking Model for Discriminating MPE
2.4. Cost-Effectiveness Analysis of Tumor-Marker Combinations
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
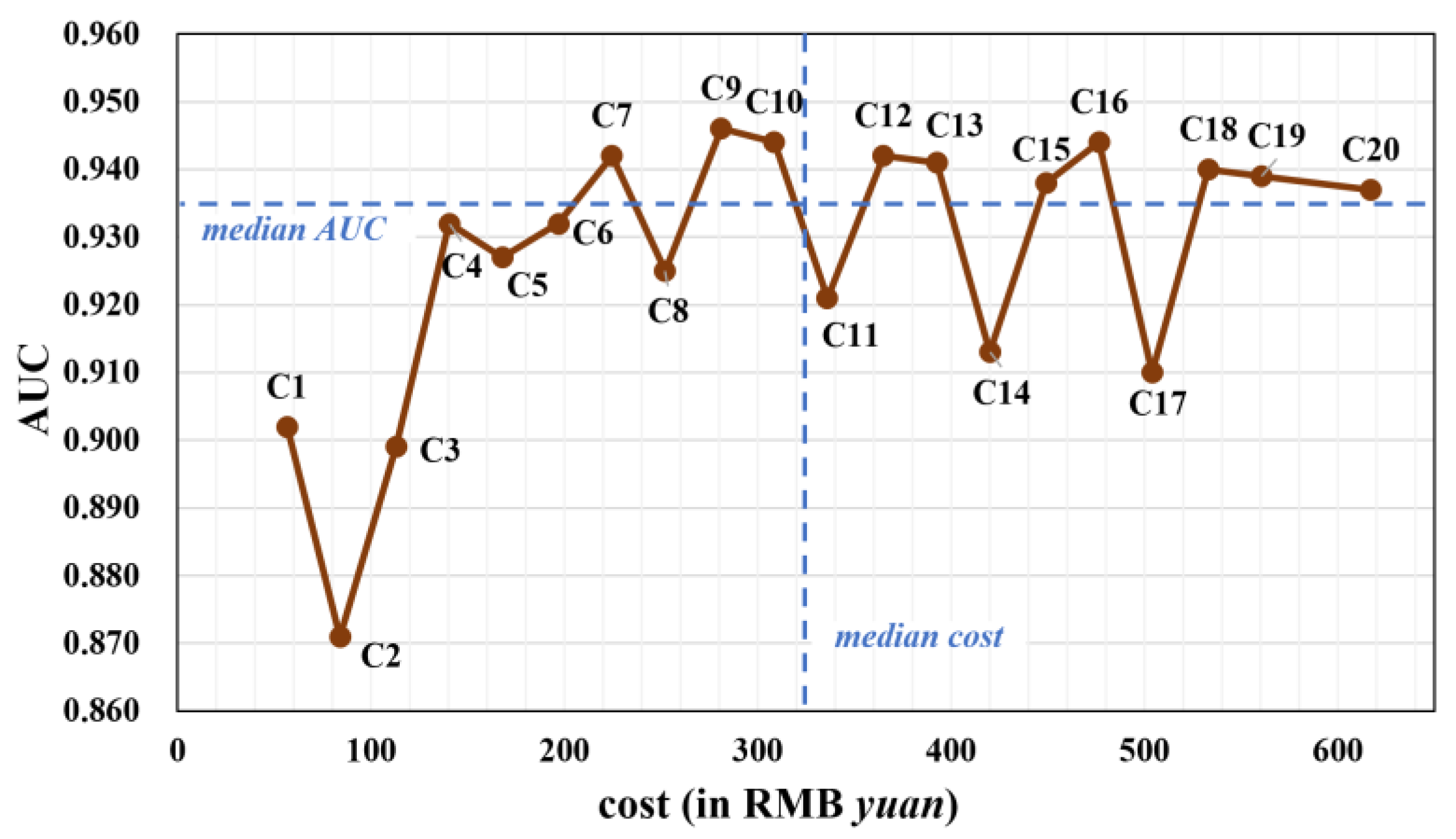
3.2. The Cost of Different Tumor-Marker Combinations
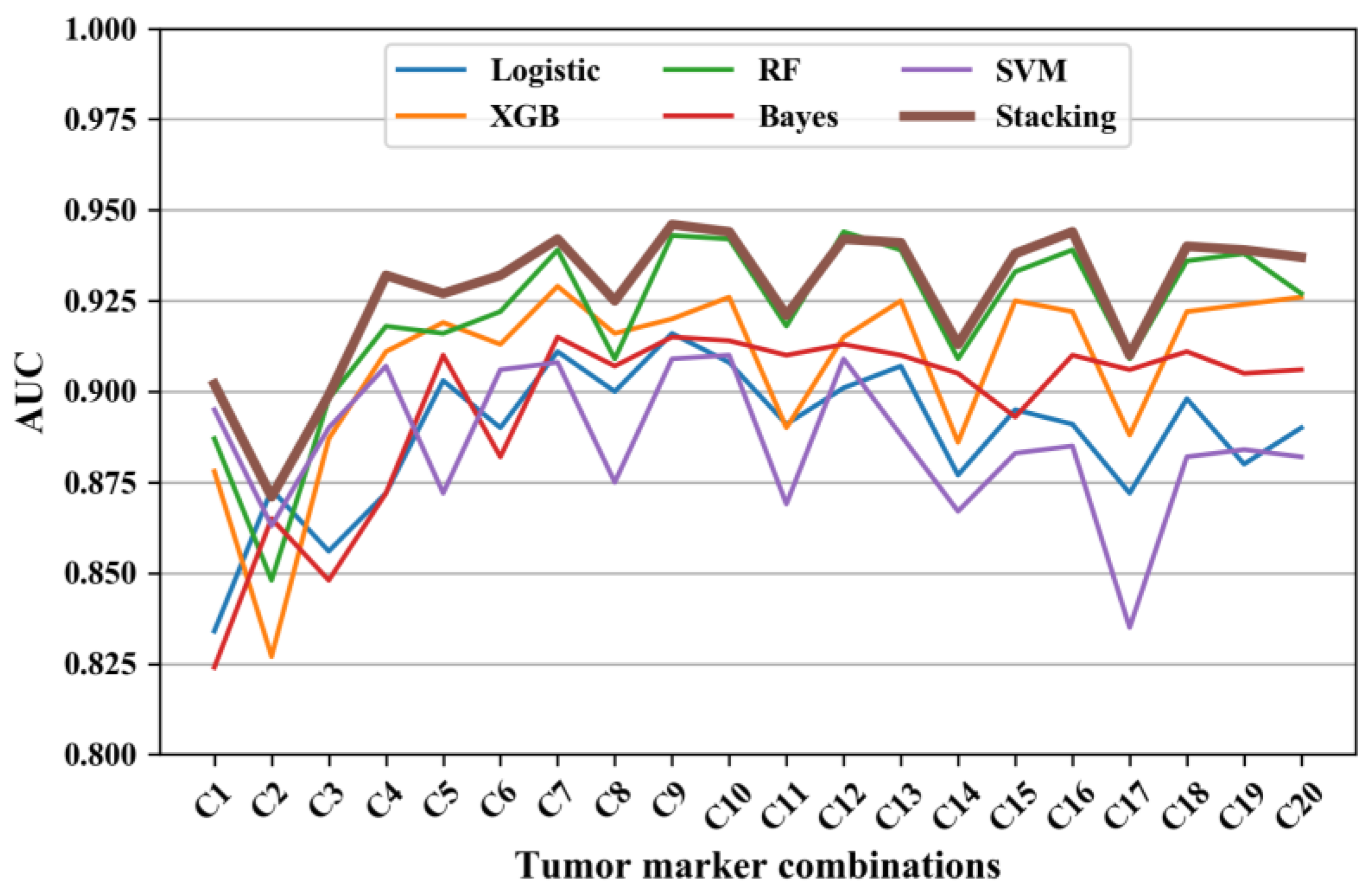
3.3. The Diagnostic Performance of the Stacking Model
3.4. The Diagnostic Performance of Different Tumor-Marker Combinations
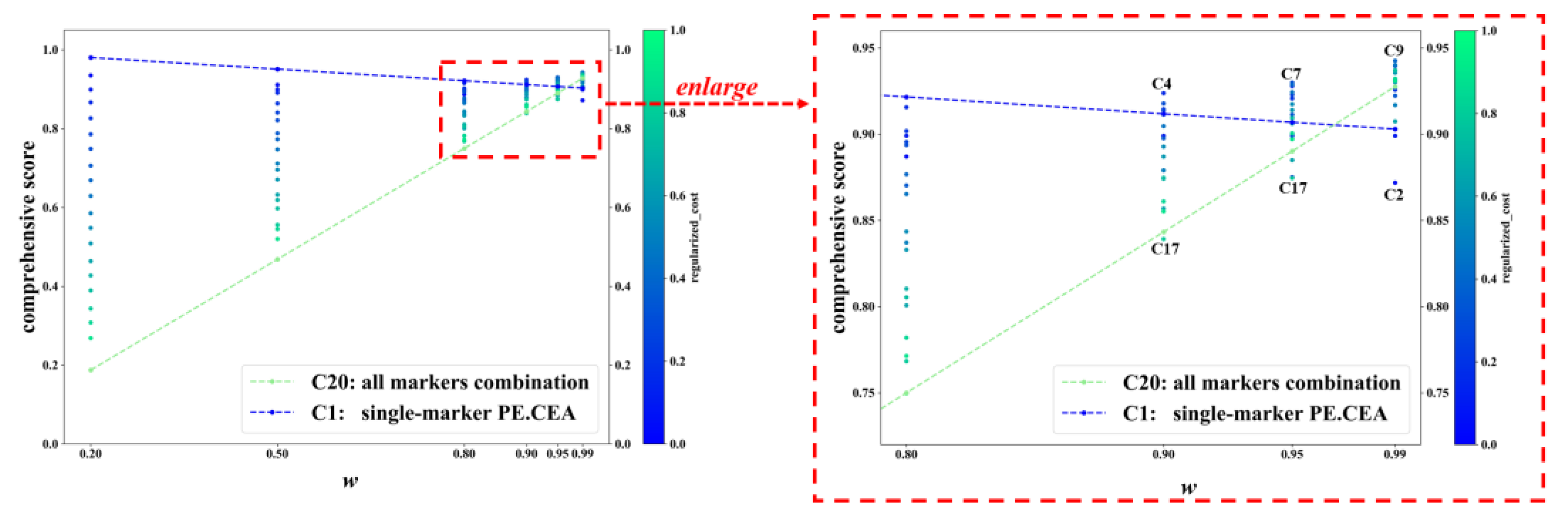
3.5. Cost-Effectiveness Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Son, S.M.; Han, H.S.; An, J.Y.; Choe, K.H.; Lee, K.M.; Lee, K.H.; Kim, S.S.; Lee, Y.M.; Lee, H.C.; Song, H.G.; et al. Diagnostic performance of CD66c in lung adenocarcinoma-associated malignant pleural effusion: Comparison with CEA, CA 19-9, and CYFRA 21-1. Pathology 2015, 47, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Starr, R.L.; Sherman, M.E. The Value of Multiple Preparations in the Diagnosis of Malignant Pleural Effusions—A Cost-Benefit-Analysis. Acta Cytol. 1991, 35, 533–537. [Google Scholar]
- Cheng, D.; Liang, B.; Li, Y.H. Application of MMP-7 and MMP-10 in Assisting the Diagnosis of Malignant Pleural Effusion. Asian Pac. J. Cancer Prev. 2012, 13, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Penz, E.D.; Mishra, E.K.; Davies, H.E.; Manns, B.J.; Miller, R.F.; Rahman, N.M. Comparing Cost of Indwelling Pleural Catheter vs Talc Pleurodesis for Malignant Pleural Effusion. Chest 2014, 146, 991–1000. [Google Scholar] [CrossRef]
- Puri, V.; Pyrdeck, T.L.; Crabtree, T.D.; Kreisel, D.; Krupnick, A.S.; Colditz, G.A.; Patterson, G.A.; Meyers, B.F. Treatment of Malignant Pleural Effusion: A Cost-Effectiveness Analysis. Ann. Thorac. Surg. 2012, 94, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Neragi-Miandoab, S. Malignant pleural effusion, current and evolving approaches for its diagnosis and management. Lung Cancer 2006, 54, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Miles, D.W.; Knight, R.K. Diagnosis and management of malignant pleural effusion. Cancer Treat. Rev. 1993, 19, 151–168. [Google Scholar] [CrossRef]
- Hae-Seong, N. Malignant Pleural Effusion: Medical Approaches for Diagnosis and Management. Tuberc. Respir. Dis. 2014, 76, 211–217. [Google Scholar]
- Lombardi, G.; Zustovich, F.; Nicoletto, M.O.; Donach, M.; Artioli, G.; Pastorelli, D. Diagnosis and treatment of malignant pleural effusion: A systematic literature review and new approaches. Am. J. Clin. Oncol. 2010, 33, 420–423. [Google Scholar] [CrossRef]
- Feller-Kopman, D.J.; Reddy, C.B.; DeCamp, M.M.; Diekemper, R.L.; Gould, M.K.; Henry, T.; Iyer, N.P.; Lee, Y.C.G.; Lewis, S.Z.; Maskell, N.A.; et al. Management of Malignant Pleural Effusions. An Official ATS/STS/STR Clinical Practice Guideline. Am. J. Resp. Crit. Care 2018, 198, 839–849. [Google Scholar] [CrossRef]
- Dutau, H.; Guinde, J.; Astoul, P. Management of Malignant Pleural Effusion: Where Are We Now? Semin. Respir. Crit. Care Med. 2022, 43, 559–569. [Google Scholar]
- Yang, Y.; Liu, Y.L.; Shi, H.Z. Diagnostic Accuracy of Combinations of Tumor Markers for Malignant Pleural Effusion: An Updated Meta-Analysis. Respiration 2017, 94, 62–69. [Google Scholar] [CrossRef]
- Zhang, M.; Yan, L.; Lippi, G.; Hu, Z.D. Pleural biomarkers in diagnostics of malignant pleural effusion: A narrative review. Transl. Lung Cancer Res. 2021, 10, 1557–1570. [Google Scholar] [CrossRef]
- Zhang, Y.X.; Wang, J.Y.; Liang, B.S.; Wu, H.Y.; Chen, Y.Y. Diagnosis of malignant pleural effusion with combinations of multiple tumor markers: A comparison study of five machine learning models. Int. J. Biol. Marker 2023, 38, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Olden, A.M.; Holloway, R. Treatment of malignant pleural effusion: PleuRx catheter or talc pleurodesis? A cost-effectiveness analysis. J. Palliat. Med. 2010, 13, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Wolpert, D.H. Stacked generalization. Neural Netw. 1992, 5, 241–259. [Google Scholar] [CrossRef]
- AbaeiKoupaei, N.; Al Osman, H. A Multi-Modal Stacked Ensemble Model for Bipolar Disorder Classification Tree. IEEE Trans. Affect. Comput. 2023, 14, 236–244. [Google Scholar] [CrossRef]
- Aboneh, T.; Rorissa, A.; Srinivasagan, R. Stacking-Based Ensemble Learning Method for Multi-Spectral Image Classification. Technologies 2022, 10, 17. [Google Scholar] [CrossRef]
- Zhou, T.; Jiao, H. Exploration of the Stacking Ensemble Machine Learning Algorithm for Cheating Detection in Large-Scale Assessment. Educ. Psychol. Meas. 2023, 83, 831–854. [Google Scholar] [CrossRef]
- Zhou, C.L.; Zhou, L.; Liu, F.; Chen, W.H.; Wang, Q.; Liang, K.L.; Guo, W.Q.; Zhou, L.Y. A Novel Stacking Heterogeneous Ensemble Model with Hybrid Wrapper-Based Feature Selection for Reservoir Productivity Predictions. Complexity 2021, 2021, 6675638. [Google Scholar] [CrossRef]
- Zheng, J.Y.; Wang, M.H.; Yao, T.C.; Tang, Y.C.; Liu, H.J. Dynamic Mechanical Strength Prediction of BFRC Based on Stacking Ensemble Learning and Genetic Algorithm Optimization. Buildings 2023, 13, 1155. [Google Scholar] [CrossRef]
- Zheng, H.; Sherazi, S.W.A.; Lee, J.Y. A Stacking Ensemble Prediction Model for the Occurrences of Major Adverse Cardiovascular Events in Patients with Acute Coronary Syndrome on Imbalanced Data. IEEE Access 2021, 9, 113692–113704. [Google Scholar] [CrossRef]
- Antonangelo, L.; Sales, R.K.; Cora, A.P.; Acencio, M.M.P.; Teixeira, L.R.; Vargas, F.S. Pleural fluid tumour markers in malignant pleural effusion with inconclusive cytologic results. Curr. Oncol. 2015, 22, E336–E341. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Liu, Y.Q.; Liang, Z.G.; Wang, S.S.; Yang, J.; Wu, A.H. Diagnostic Value of Six Tumor Markers for Malignant Pleural Effusion in 1,230 Patients: A Single-Center Retrospective Study. Pathol. Oncol. Res. 2022, 28, 1610280. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; Zhu, J.; Liang, L.Q.; Zeng, N.; Wu, Y.Q.; Wan, C.; Shen, Y.C.; Wen, F.Q. Diagnostic value of tumor markers for lung adenocarcinoma-associated malignant pleural effusion: A validation study and meta-analysis. Int. J. Clin. Oncol. 2017, 22, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Li, J.; Jiang, H.G.; Ge, L.P.; Wang, Y. Diagnostic value of MUC1 and EpCAM mRNA as tumor markers in differentiating benign from malignant pleural effusion. Int. J. Med. 2014, 107, 1001–1007. [Google Scholar] [CrossRef]
- Healthcare Security Administration of Hubei Province. No. 70; 2019. Available online: https://ybj.hubei.gov.cn/zfxxgk/zc/gfwj/201911/t20191129_1545137.shtml (accessed on 3 August 2023).
- Beijing Municipal Medical Insurance Bureau. No. 35; 2021. Available online: http://ybj.beijing.gov.cn/zwgk/2020_zcwj/202112/t20211231_2581064.html (accessed on 3 August 2023).
- Zhang, J.; Chen, Y.L.; He, G.D.; Jiang, X.B.; Chen, P.S.; Ouyang, J. Differential diagnosis of tuberculous and malignant pleural effusions: Comparison of the Th1/Th2 cytokine panel, tumor marker panel and chemistry panel. Scand. J. Clin. Lab. Inv. 2020, 80, 265–270. [Google Scholar] [CrossRef]
- Chen, X.J.; Lu, J.L.; Yao, Y.E.; Huang, Z.C.; Liu, K.; Jiang, W.N.; Li, C.Q. Effects of bevacizumab combined with oxaliplatin intrathoracic injection on tumor markers and survival rate in patients with malignant pleural effusion of lung cancer. Am. J. Transl. Res. 2021, 13, 2899–2906. [Google Scholar]
- Gu, J.P.; Wang, Q.Y.; Yu, J. Diagnostic value of combination measurement of tumor markers for differentiating malignant and pleural effusion. J. Dalian Med. Univ. 2011, 33, 74–77. [Google Scholar]
- Lanceta, J.; Toprak, M.; Rosca, O.C. Merkel cell carcinoma presenting as a malignant pleural effusion post-COVID-19 hospitalization: A case report and literature review. Diagn. Cytopathol. 2022, 50, E37–E41. [Google Scholar] [CrossRef]
- Paganuzzi, G.P.R.F.M. Tumor Markers for Diagnosing Malignant Pleural Effusion? Chest 2002, 121, 302–303. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | MPE (N = 111) | BPE (N = 208) | Total (N = 319) | p-Value |
|---|---|---|---|---|
| Age (years) | 60.94 (11.96) | 49.78 (19.02) | 53.67 (17.70) | <0.001 |
| Gender | 0.002 | |||
| Male | 59 | 148 | 207 | |
| Female | 52 | 60 | 112 | |
| Region | 0.160 | |||
| Beijing | 67 | 107 | 174 | |
| Wuhan | 44 | 101 | 145 | |
| Concentrations of tumor markers | ||||
| PE.CEA (ng/mL) | 967.15 (2307.31) | 16.80 (105.81) | 347.49 (1433.20) | <0.001 |
| PE.CA19-9 (U/mL) | 2000.31 (4200.90) | 5.74 (12.94) | 699.77 (2647.65) | <0.001 |
| PE.CA125 (U/mL) | 1807.16 (2473.70) | 715.22 (796.83) | 1095.17 (1673.73) | <0.001 |
| PE.CA15-3 (U/mL) | 99.97 (199.45) | 7.48 (7.80) | 39.66 (125.49) | <0.001 |
| PB.CEA (ng/mL) | 98.16 (254.14) | 2.12 (1.74) | 35.54 (156.34) | <0.001 |
| PB.CA19-9 (U/mL) | 628.56 (2312.09) | 13.88 (40.28) | 227.76 (1391.48) | <0.001 |
| PB.CA125 (U/mL) | 257.72 (502.10) | 155.21 (147.49) | 190.88 (322.11) | <0.001 |
| PB.CA15-3 (U/mL) | 38.79 (47.97) | 12.01 (9.21) | 21.33 (31.85) | <0.001 |
| Tumor-Marker Combination | Cost | AUC | SEN | SPE |
|---|---|---|---|---|
| C1: PE.CEA | 56.5 | 0.902 | 0.748 | 0.937 |
| C2: PE.CA15-3 | 84 | 0.871 | 0.595 | 0.962 |
| C3: PE.CEA + PB.CEA | 113 | 0.899 | 0.766 | 0.913 |
| C4: PE.CA19-9 + PE.CEA | 140.5 | 0.932 | 0.757 | 0.933 |
| C5: PE.CA19-9 + PE.CA15-3 | 168 | 0.927 | 0.721 | 0.957 |
| C6: PE.CA19-9 + PE.CEA+PB.CEA | 197 | 0.932 | 0.748 | 0.923 |
| C7: PE.CA19-9 + PE.CA15-3+PE.CEA | 224.5 | 0.942 | 0.775 | 0.942 |
| C8: PE.CA19-9 + PE.CA15-3+PB.CA15-3 | 252 | 0.925 | 0.739 | 0.952 |
| C9: PE.CA19-9 + PE.CA15-3+PE.CEA+PB.CEA | 281 | 0.946 | 0.748 | 0.928 |
| C10: PE.CA19-9 + PE.CA15-3+PE.CEA+PB.CA125 | 308.5 | 0.944 | 0.757 | 0.957 |
| C11: PE.CA19-9 + PE.CA15-3+PB.CA19-9+PB.CA125 | 336 | 0.921 | 0.712 | 0.947 |
| C12: PE.CA19-9 + PE.CA15-3+PE.CEA+PB.CA19-9+PB.CEA | 365 | 0.942 | 0.748 | 0.942 |
| C13: PE.CA19-9 + PE.CA125+PE.CA15-3+PE.CEA+PB.CA125 | 392.5 | 0.941 | 0.829 | 0.966 |
| C14: PE.CA19-9 + PE.CA15-3+PB.CA19-9+PB.CA125+PB.CA15-3 | 420 | 0.913 | 0.730 | 0.961 |
| C15: PE.CA19-9 + PE.CA125+PE.CEA+PB.CA125+PB.CA15-3+PB.CEA | 449 | 0.938 | 0.775 | 0.952 |
| C16: PE.CA19-9 + PE.CA125+PE.CA15-3+PE.CEA+PB.CA19-9+PB.CA125 | 476.5 | 0.944 | 0.793 | 0.957 |
| C17: PE.CA19-9 + PE.CA125+PE.CA15-3+PB.CA19-9+PB.CA125+PB.CA15-3 | 504 | 0.910 | 0.712 | 0.947 |
| C18: PE.CA19-9 + PE.CA125+PE.CA15-3+PE.CEA+PB.CA19-9+PB.CA125+PB.CEA | 533 | 0.940 | 0.802 | 0.957 |
| C19: PE.CA19-9+PE.125+PE.CA15-3+PE.CEA+PB.199+PB.125+PB.CA15-3 | 560.5 | 0.939 | 0.820 | 0.942 |
| C20: PE.CA19-9+PE.CA125+PE.CA15-3+PE.CEA+PB.199+PB.CA125+PB.CA15-3+PB.CEA | 617 | 0.937 | 0.793 | 0.961 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Zhou, J.; Wu, H.; Chen, Y.; Liang, B. The Diagnosis of Malignant Pleural Effusion Using Tumor-Marker Combinations: A Cost-Effectiveness Analysis Based on a Stacking Model. Diagnostics 2023, 13, 3136. https://doi.org/10.3390/diagnostics13193136
Wang J, Zhou J, Wu H, Chen Y, Liang B. The Diagnosis of Malignant Pleural Effusion Using Tumor-Marker Combinations: A Cost-Effectiveness Analysis Based on a Stacking Model. Diagnostics. 2023; 13(19):3136. https://doi.org/10.3390/diagnostics13193136
Chicago/Turabian StyleWang, Jingyuan, Jiangjie Zhou, Hanyu Wu, Yangyu Chen, and Baosheng Liang. 2023. "The Diagnosis of Malignant Pleural Effusion Using Tumor-Marker Combinations: A Cost-Effectiveness Analysis Based on a Stacking Model" Diagnostics 13, no. 19: 3136. https://doi.org/10.3390/diagnostics13193136
APA StyleWang, J., Zhou, J., Wu, H., Chen, Y., & Liang, B. (2023). The Diagnosis of Malignant Pleural Effusion Using Tumor-Marker Combinations: A Cost-Effectiveness Analysis Based on a Stacking Model. Diagnostics, 13(19), 3136. https://doi.org/10.3390/diagnostics13193136