

Diagnostic of Patients with COVID-19 Pneumonia Using Passive Medical Microwave Radiometry (MWR)

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, P.; Liu, T.; Huang, L.; Liu, H.; Lei, M.; Xu, W.; Hu, X.; Chen, J.; Liu, B. Use of chest CT in combination with negative RT-PCR assay for the 2019 novel coronavirus but high clinical suspicion. Radiology 2020, 295, 22–23. [Google Scholar] [CrossRef] [PubMed]
- Phan, L.T.; Nguyen, T.V.; Luong, Q.C.; Nguyen, T.V.; Nguyen, H.T.; Le, H.Q.; Nguyen, T.T.; Cao, T.M.; Pham, Q.D. Importation and human-to-human transmission of a novel coronavirus in Vietnam. N. Engl. J. Med. 2020, 382, 872–874. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). Coronavirus Disease 2019 (COVID-19) Situation Report e 28. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200217-sitrep-28-covid-19.pdf?sfvrsn¼a19cf2ad_2 (accessed on 19 April 2020).
- World Meter. Corona Virus Update (Live). Available online: https://www.worldometers.info/coronavirus/ (accessed on 19 April 2020).
- Guarner, J. Three emerging coronaviruses in two decades: The story of SARS, MERS, and now COVID-19. Clin. Infect Dis. 2020, 153, 420.e1. [Google Scholar]
- Rajgor, D.; Lee, M.; Archuleta, S.; Bagdasarian, N.; Quek, S. The many estimates of the COVID-19 case fatality rate. Lancet Infect Dis. 2020, 20, 776–777. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Qiu, H.; Huang, M.; Yang, Y. Lower mortality of COVID-19 by early recognition and intervention: Experience from Jiangsu Province. Ann. Intensiv. Care 2020, 10, 1.e4. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809.e15. [Google Scholar]
- Hui, D.S.; Azhar, E.I.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; Mchugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCOVID epidemic threat of novel coronaviruses to global health-The latest 2019 novel coronavirus outbreak in Wuhan, China. J. Infect 2020, 91, 264.e6. [Google Scholar]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann. Intern. Med. 2020, 172, 577.e82. [Google Scholar] [CrossRef]
- Lei, S.; Jiang, F.; Su, W.; Chen, C.; Chen, J.; Mei, W.; Zhan, L.-Y.; Jia, Y.; Zhang, L.; Liu, D.; et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalMedicine 2020, 54, 2.e3. [Google Scholar]
- Ioannidis, J.P.; Axfors, C.; Contopoulos-Ioannidis, D.G. Population-level COVID-19 mortality risk for non-elderly individuals overall and for non-elderly individuals without underlying diseases in pandemic epicenters. Environ. Res. 2020, 188, 109890. [Google Scholar] [CrossRef] [PubMed]
- Dash, S.; Chakraborty, C.; Giri, S.K.; Pani, S.K.; Frnda, J. BIFM: Big-Data Driven Intelligent Forecasting Model for COVID-19. IEEE Access 2021, 9, 97505–97517. [Google Scholar] [CrossRef]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of Coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RTPCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yang, M.; Shen, C.; Wang, F.; Yuan, J.; Li, J.; Zhang, M.; Wang, Z.; Xing, L.; Wei, J.; et al. Laboratory Diagnosis and Monitoring the Viral Shedding of SARS-CoV-2 Infection. Innovation 2020, 1, 100061. [Google Scholar] [CrossRef]
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef]
- Alanagreh, L.; Alzoughool, F.; Atoum, M. The human coronavirus disease COVID19: Its origin, characteristics, and insights into potential drugs and its mechanisms. Pathogens 2020, 9, 331. [Google Scholar] [CrossRef]
- Chinese Government. The Diagnostic and Treatment Protocol of COVID-19. Available online: http://www.gov.cn/zhengce/zhengceku/2020-02/19/content_5480948.htm (accessed on 19 April 2020).
- Wu, D.; Wu, T.; Liu, Q.; Yang, Z. The SARS-CoV-2 outbreak: What we know. Int. J. Infect. Dis. 2020, 94, 44–48. [Google Scholar] [CrossRef]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical feature of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef]
- Lake, M.A. What we know so far: COVID-19 current clinical knowledge and research. Clin. Med. 2020, 20, 124–127. [Google Scholar] [CrossRef]
- Al Johani, S.; Hajeer, A.H. MERS-CoV diagnosis: An update. J. Infect. Public Health 2016, 9, 216–219. [Google Scholar] [CrossRef]
- Zhou, S.; Wang, Y.; Zhu, T.; Xia, L. CT features of coronavirus disease 2019 (COVID-19) pneumonia in 62 patients in Wuhan, China. AJR Am. J. Roentgenol. 2020, 214, 1287–1294. [Google Scholar] [CrossRef]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology 2020, 295, 200230. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Zhong, Z.; Zhao, W.; Zheng, C.; Wang, F.; Liu, J. Chest CT for typical 2019-nCoV pneumonia: Relationship to negative RTPCR testing. Radiology 2020, 296, E41–E45. [Google Scholar] [CrossRef]
- Bhuyan, H.K.; Chakraborty, C.; Shelke, Y.; Pani, S.K. COVID-19 diagnosis system by deep learning approaches. Expert Syst. 2022, 39, e12776. [Google Scholar] [CrossRef]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.-B.; Wang, D.-C.; Mei, J.; et al. Performance of radiologists in differentiating COVID-19 from viral pneumonia on chest CT. Radiology 2020, 10, 8.e23. [Google Scholar] [CrossRef]
- Dai, W.-C.; Zhang, H.-W.; Yu, J.; Xu, H.-J.; Chen, H.; Luo, S.-P.; Zhang, H.; Liang, L.-H.; Wu, X.-L.; Lei, Y.; et al. CT imaging and differential diagnosis of COVID-19. Can. Assoc. Radiol J. 2020, 71, 195.e200. [Google Scholar] [CrossRef] [PubMed]
- Raptis, C.A.; Hammer, M.M.; Short, R.G.; Shah, A.; Bhalla, S.; Bierhals, A.J.; Filev, P.D.; Hope, M.D.; Jeudy, J.; Kligerman, S.J.; et al. Chest CT and coronavirus disease (COVID-19): A critical review of the literature to date. AJR 2020, 16, 1.e4. [Google Scholar]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: A multicenter study. AJR 2020, 214, 1072.e7. [Google Scholar] [CrossRef] [PubMed]
- Salehi, S.; Abedi, A.; Balakrishnan, S.; Gholamrezanezhad, A. Coronavirus disease 2019 (COVID-19): A systematic review of imaging findings in 919 patients. AJR 2020, 10, 1.e7. [Google Scholar] [CrossRef] [PubMed]
- Caruso, D.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Polidori, T.; Rucci, C.; Guido, G.; Bracci, B.; De Dominicis, C.; Laghi, A. Chest CT features of COVID-19 in Rome, Italy. Radiology 2020, 296, E79–E85. [Google Scholar] [CrossRef]
- Zhu, Y.; Gao, Z.H.; Liu, Y.L.; Xu, D.Y.; Guan, T.M.; Li, Z.P.; Kuang, J.Y.; Li, X.M.; Yang, Y.Y.; Feng, S.T. Clinical and CT imaging features of 2019 novel coronavirus disease (COVID-19). J. Infect. Dis. 2020, 81, 147–178. [Google Scholar] [CrossRef] [PubMed]
- Legua, P.; Forner-Giner, M.Á.; Nuncio-Jáuregui, N.; Hernández, F. Sensitivity of chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Goryanin, I.; Karbainov, S.; Shevelev, O.; Tarakanov, A.; Redpath, K.; Vesnin, S.; Ivanov, Y. Passive microwave radiometry in biomedical studies. Drug Discov. Today 2020, 25, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Raiko, J.; Koskensalo, K.; Sainio, T. Imaging-based internal body temperature measurements: The journal Temperature toolbox. Temperature 2020, 7, 363–388. [Google Scholar] [CrossRef] [PubMed]
- Manual MMWR2020 (RTM-01-RES). Available online: www.mmwr.co.uk (accessed on 26 January 2016).
- Laskari, K.; Siores, E.; Tektonidou, M.G.; Sfikakis, P.P. Microwave Radiometry for the Diagnosis and Monitoring of Inflammatory Arthritis. Diagnostics 2023, 13, 609. [Google Scholar] [CrossRef]
- Osmonov, B.; Ovchinnikov, L.; Galazis, C.; Emilov, B.; Karaibragimov, M.; Seitov, M.; Vesnin, S.; Losev, A.; Levshinskii, V.; Popov, I.; et al. Passive Microwave Radiometry for the Diagnosis of Coronavirus Disease 2019 Lung Complications in Kyrgyzstan. Diagnostics 2021, 11, 259. [Google Scholar] [CrossRef] [PubMed]
- Vesnin, S.G.; Sedankin, M.K.; Ovchinnikov, L.M.; Gudkov, A.G.; Leushin, V.Y.; Sidorov, I.A.; Goryanin, I.I. Portable microwave radiometer for wearable devices. Sens. Actuators A Phys. 2021, 318, 112506. [Google Scholar] [CrossRef]
- Gogna, A.; Yogendra, P.; Lee, S.H.E.; Aziz, A.; Cheong, E.; Chan, L.P.; Venkatanarasimha, N. Diagnostic ultrasound services during the coronavirus disease (COVID-19) pandemic. Am. J. Roentgenol. 2020, 215, 1130–1135. [Google Scholar] [CrossRef]
- Sharashova, E.E.; Kholmatova, K.K.; Gorbatova, M.A.; Grjibovsky, A.M. Application of multiple logistic regression analysis in healthcare using the SPSS statistical software package. Sci. Healthc. 2017, 4, 5–26. [Google Scholar] [CrossRef]
- Jacobi, A.; Chung, M.; Bernheim, A.; Eber, C. Portable chest X-ray in coronavirus disease-19 (COVID-19): A pictorial review. Clin. Imaging 2020, 64, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Bhosale, Y.H.; Patnaik, K.S. Application of Deep Learning Techniques in Diagnosis of COVID-19 (Coronavirus): A Systematic Review. Neural Process Lett. 2022, 55, 3551–3603. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Minimum | Maximum | Mean | Std. Deviation | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| average internal (Tint) | 50 | 31.57 | 34.08 | 32.60 | 0.52 | 32.45 | 32.74 |
| average skin (Tsk) | 50 | 29.59 | 33.06 | 31.37 | 0.84 | 31.13 | 31.60 |
| difference | 50 | −0.27 | 3.16 | 1.2280 | 0.73 | 1.02 | 1.43 |
| N | Minimum | Maximum | Mean | Std. Deviation | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Tint | 142 | 32.19 | 36.85 | 34.23 | 0.84 | 34.09 | 34.37 |
| Tsk | 142 | 30.06 | 36.07 | 33.21 | 0.78 | 33.08 | 33.34 |
| difference | 142 | −0.93 | 3.85 | 1.02 | 0.95 | 0.86 | 1.18 |
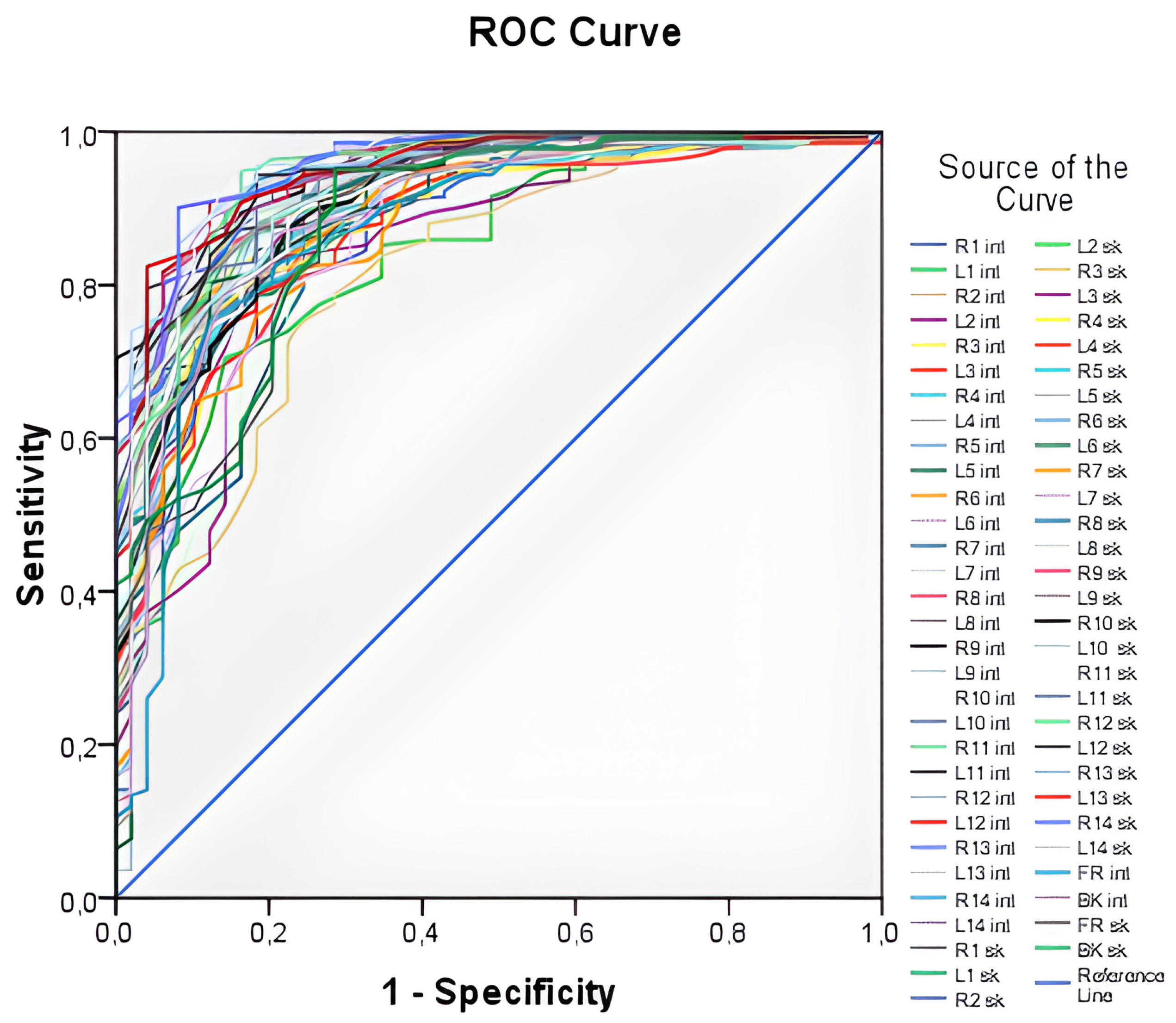
| Test Result Variable(s). | Area | Std. Error a | Asymptotic 95% Confidence Interval | |
|---|---|---|---|---|
| Lower Bound | Upper Bound | |||
| average internal (Tint) | 0.967 | 0.013 | 0.941 | 0.993 |
| average skin (Tsk) | 0.951 | 0.016 | 0.919 | 0.983 |
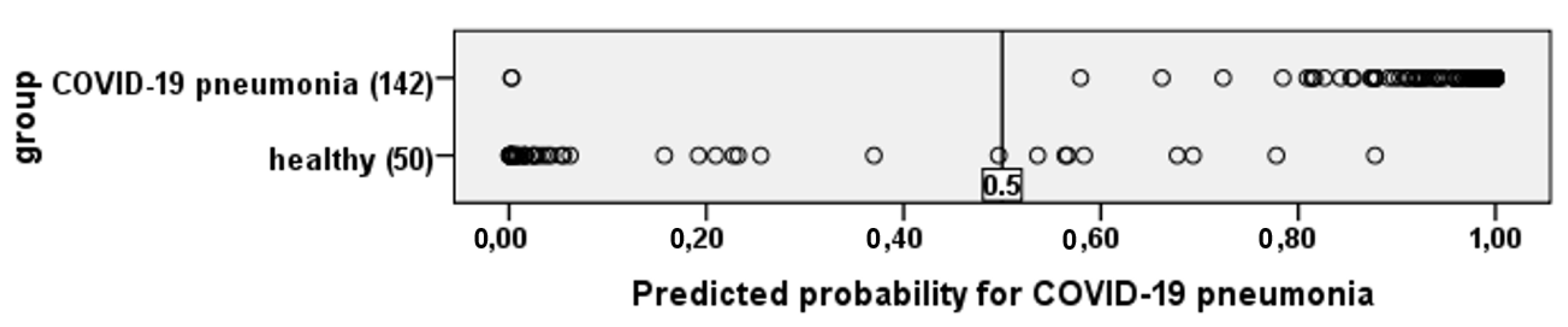
| Observed | ROC Curve Best Thresholds | Predicted Correct | ||
|---|---|---|---|---|
| Logistic Regression | Deep Neural Network | |||
| group | control group | 88.8% | 92.7% | 99.7% |
| COVID-19 pneumonia | 95.2% | 97.6% | 98.6% | |
| Overall efficiency | 91.5% | 94.8% | 99.1% | |
| B | S.E. | Wald | df | Exp(B) | 95.0% CI for EXP(B) | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Tint (b1) | 3.188 | 0.770 | 17.155 | 1 | 24.243 | 5.363 | 109.594 |
| Tsk (b2) | 1.677 | 0.524 | 10.236 | 1 | 5.351 | 1.915 | 14.951 |
| Const (b0) | −159,463 | 28,916 | 30,412 | 1 | 0.000 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emilov, B.; Sorokin, A.; Seiitov, M.; Kobayashi, B.T.; Chubakov, T.; Vesnin, S.; Popov, I.; Krylova, A.; Goryanin, I. Diagnostic of Patients with COVID-19 Pneumonia Using Passive Medical Microwave Radiometry (MWR). Diagnostics 2023, 13, 2585. https://doi.org/10.3390/diagnostics13152585
Emilov B, Sorokin A, Seiitov M, Kobayashi BT, Chubakov T, Vesnin S, Popov I, Krylova A, Goryanin I. Diagnostic of Patients with COVID-19 Pneumonia Using Passive Medical Microwave Radiometry (MWR). Diagnostics. 2023; 13(15):2585. https://doi.org/10.3390/diagnostics13152585
Chicago/Turabian StyleEmilov, Berik, Aleksander Sorokin, Meder Seiitov, Binsei Toshi Kobayashi, Tulegen Chubakov, Sergey Vesnin, Illarion Popov, Aleksandra Krylova, and Igor Goryanin. 2023. "Diagnostic of Patients with COVID-19 Pneumonia Using Passive Medical Microwave Radiometry (MWR)" Diagnostics 13, no. 15: 2585. https://doi.org/10.3390/diagnostics13152585
APA StyleEmilov, B., Sorokin, A., Seiitov, M., Kobayashi, B. T., Chubakov, T., Vesnin, S., Popov, I., Krylova, A., & Goryanin, I. (2023). Diagnostic of Patients with COVID-19 Pneumonia Using Passive Medical Microwave Radiometry (MWR). Diagnostics, 13(15), 2585. https://doi.org/10.3390/diagnostics13152585