
High-Field Magnetic Resonance Imaging of the Temporomandibular Joint Low Agreement with Clinical Diagnosis in Asymptomatic Females

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Examination
- 0—normal
- IIa—dislocation of the disc with reduction (DDWR)
- IIb—dislocation of the disc without reduction (DDWOR) with limited jaw opening
- IIc—DDWOR and without limited jaw opening
- 0—normal
- IIIa—arthralgia
- IIIb—osteoarthritis
- IIIc—osteoarthrosis
2.3. MRI Protocol
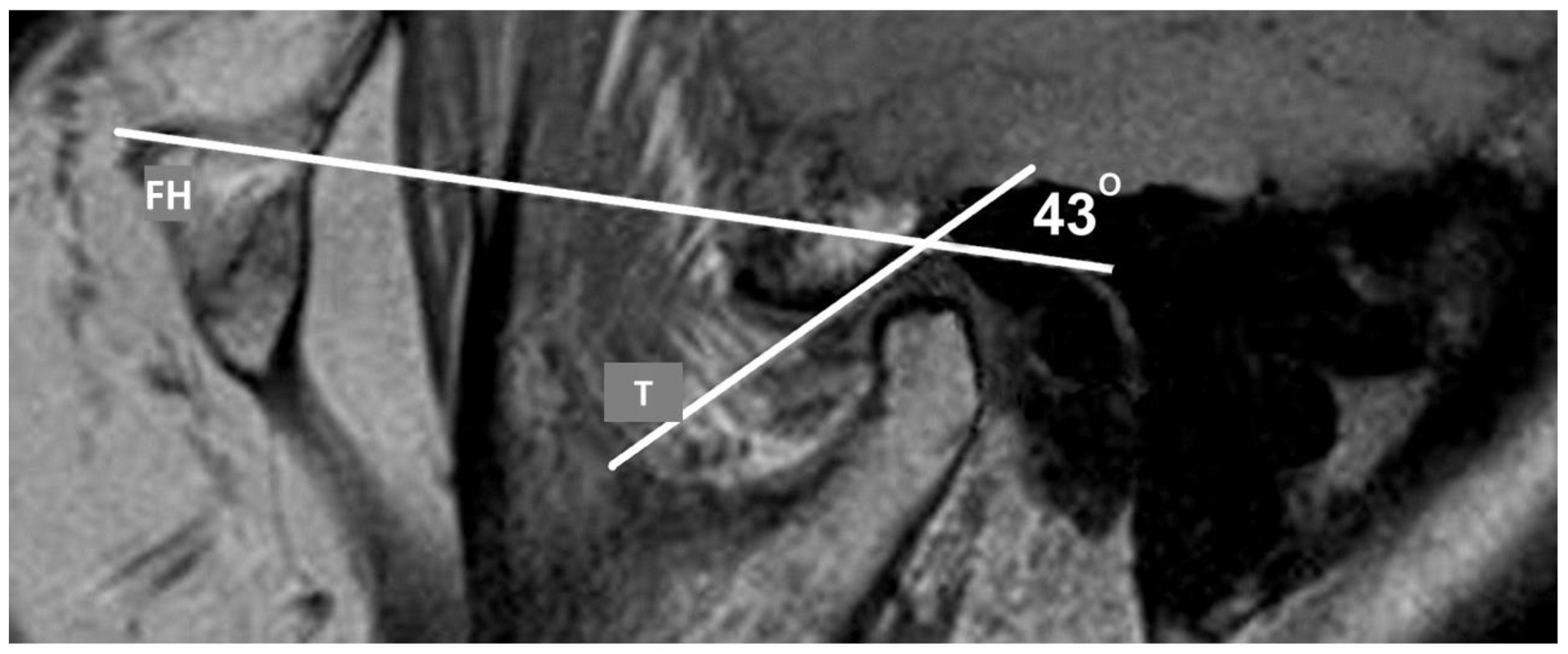
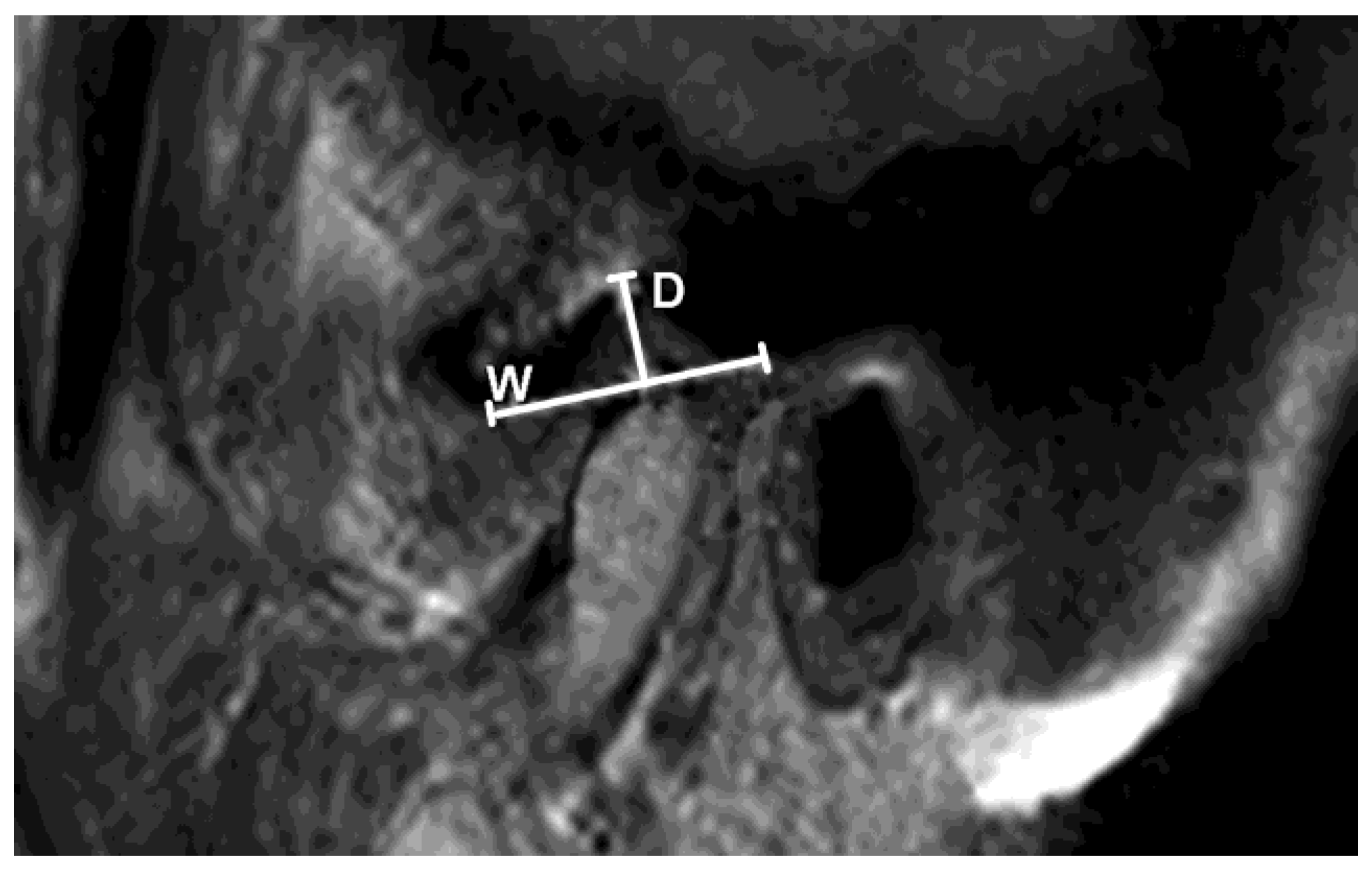
2.4. Analysis of TMJ
2.5. Statistical Analysis
3. Results
3.1. Subjects’ Features
3.2. Clinical and MRI Findings
3.3. Agreement Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McNeill, C. Management of temporomandibular disorders: Concepts and controversies. J. Prosthet. Dent. 1997, 77, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Okeson, J.P. Management of Temporomandibular Disorder and Occlusion—E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2008; pp. 1–333. [Google Scholar]
- Anatomy, G. The Anatomical Basis of Clinical Practice; Elsevier Churchill Livingston: Edinburgh, Scotland, 2005. [Google Scholar]
- Research. NIoDaC. Facial. Pain. 2013. Available online: http://www.nidcr.nih.gov/DataStatistics/FindDataByTopic/FacialPain/ (accessed on 21 November 2021).
- Naeije, M.; Te Veldhuis, A.H.; Te Veldhuis, E.C.; Visscher, C.M.; Lobbezoo, F. Disc displacement within the human temporo-mandibular joint: A systematic review of a ‘noisy annoyance’. J. Oral Rehab. 2013, 40, 139–158. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-H.; Lee, K.M.; Auh, Q.-S. MRI-Based Assessment of Masticatory Muscle Changes in TMD Patients after Whiplash Injury. J. Clin. Med. 2021, 10, 1404. [Google Scholar] [CrossRef] [PubMed]
- Reinoso, P.A.C.; Delgado, E.R.; Robalino, J.J. Biomechanics of the Temporomandibular joint. In Temporomandibular Joint—Surgical Reconstruction and Management; Kummoona, R., Ed.; Intech Open: Rijeka, Croatia, 2022. [Google Scholar]
- Saito, E.T.; Akashi, P.M.H.; Sacco, I.D.C.N. Global Body Posture Evaluation in Patients with Temporomandibular Joint Disorder. Clinics 2009, 64, 35–39. [Google Scholar] [CrossRef]
- Barcelos, E. Efeitos dos exercícios terapêuticos na disfunção temporomandi-bular: Estudo de caso [monografia] Tubarão: Universidade do Sul de Santa Catarina; 2008.Ferreira FV, Ferreira FV. Peroni AB, Tabarelli, Z. Desordens temporomandibulares: Uma abordagem fisioterapêutica e odontológica. Stomatos 2009, 15, 27–37. [Google Scholar]
- Jo, J.-H.; Chung, J.-W. Gender Differences in Clinical Characteristics of Korean Temporomandibular Disorder Patients. Appl. Sci. 2021, 11, 3583. [Google Scholar] [CrossRef]
- Silva, M.A.G.; Pantoja, L.L.Q.; Dutra-Horstmann, K.L.; Valladares-Neto, J.; Wolff, F.L.; Porporatti, A.L.; Guerra, E.N.S.; Canto, G.D.L. Prevalence of degenerative disease in temporomandibular disorder patients with disc displacement: A systematic review and meta-analysis. J. Cranio-Maxillofac. Surg. 2020, 48, 942–955. [Google Scholar] [CrossRef]
- Sambataro, S.; Cervino, G.; Bocchieri, S.; La Bruna, R.; Cicciù, M. TMJ Dysfunctions Systemic Implications and Postural Assessments: A Review of Recent Literature. J. Funct. Morphol. Kinesiol. 2019, 4, 58. [Google Scholar] [CrossRef]
- Manfredini, D.; Piccotti, F.; Ferronato, G.; Guarda-Nardini, L. Age peaks of different RDC/TMD diagnoses in a patient pop-ulation. J. Dent. 2010, 38, 392–399. [Google Scholar] [CrossRef]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef]
- Manfredini, D. Current Concepts on Temporomandibular Disorders; Quintessence Publishing: Berlin, Germany, 2010. [Google Scholar]
- Jeremic-Knezevic, M.; Knezevic, A.; Boban, N.; Koprivica, D.D.; Boban, J. Correlation of somatization, depression, and chronic pain with clinical findings of the temporomandibular disorders in asymptomatic women. CRANIO 2018, 39, 17–23. [Google Scholar] [CrossRef]
- Bristela, M.; Schmid-Schwap, M.; Eder, J.; Reichenberg, G.; Kundi, M.; Piehslinger, E.; Robinson, S. Magnetic resonance imaging of temporomandibular joint with anterior disc dislocation without reposition- long-term results. Clin. Oral Investig. 2017, 21, 237–245. [Google Scholar] [CrossRef]
- Zhang, J.; Yu, W.; Wang, J.; Wang, S.; Li, Y.; Jing, H.; Li, Z.; Li, X.; Liang, M.; Wang, Y. A Comparative Study of Temporomandibular Joints in Adults with Definite Sleep Bruxism on Magnetic Resonance Imaging and Cone-Beam Computer Tomography Images. J. Clin. Med. 2023, 12, 2570. [Google Scholar] [CrossRef]
- Zhang, Q.; Ye, Z.; Wu, Y.; Zhu, Y.; Liu, J.; Yang, W.; Ye, C.; Han, S.L.R.; Wang, J.; Xiong, X. Nonlinear Relationship between Temporomandibular Joint Disc Displacement Distance and Disc Length: A Magnetic Resonance Imaging Analysis. J. Clin. Med. 2022, 11, 7160. [Google Scholar] [CrossRef]
- Gharavi, S.M.; Qiao, Y.; Faghihimehr, A.; Vossen, J. Imaging of the Temporomandibular Joint. Diagnostics 2022, 12, 1006. [Google Scholar] [CrossRef]
- Dworkin, S.F.; LeResche, L. Research diagnostic criteria for temporomandibular disorders: Review, criteria, examinations and specifications, critique. J. Craniomandib. Disord. Facial Oral Pain 1992, 6, 301–355. [Google Scholar]
- Kraemer, H.C.; Periyakoil, V.S.; Noda, A. Agreement Statistics. In Tutorials in Biostatistics; D’Agostino, R.B., Ed.; Volume I: Statistical Methods in Clinical Studies; John Wiley & Sons, Ltd.: Norwich, England, 2004. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Manfredini, D.; Guarda-Nardni, L.; Winocur, E.; Piccotti, F.; Ahlberg, J.; Lobbezoo, F. Research diagnostic criteria for tem-poromandibular disorders: Asystematic review of axis I epidemiological findings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 453–462. [Google Scholar] [CrossRef]
- Chang, C.; Wang, D.; Yang, M.; Hsu, W.; Hsu, M. Functional disorders of the temporomandibular joints: Internal derangement of the temporomandibular joint. Kaohsiung J. Med. Sci. 2018, 34, 223–230. [Google Scholar] [CrossRef]
- Chopra, P.; Tinkle, B.; Hamonet, C.; Brock, I.; Gompel, A.; Bulbena, A.; Francomano, C. Pain management in the Ehlers-Danlos syndromes. Am. J. Med. Genet. Part C Semin. Med. Genet. 2017, 175, 212–219. [Google Scholar] [CrossRef]
- Rybalov, O.V.; Yatsenko, P.I.; Yatsenko, O.I.; Khorosh, M.V.; Korol, D.M.; Kindiy, D.D.; Kindiy, V.D. Hypermobility of the articular heads of the temporomandibular joint: Pathology or variant of the norm? Wiad Lek. 2019, 72, 1883–1889. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Sela, M.C.; Ran, L.Z.; Rushinek, H.; Talisman, S.; Casap, N. Increased Prevalence of Generalized Joint Hypermobility Observed in Patients With Recurrent Temporomandibular Joint Dislocation. J. Oral Maxillofac. Surg. 2023; in press. [Google Scholar] [CrossRef]
- Campos, M.; Campos, P.; Cangussu, M.; Guimarães, R.; Line, S.R.P. Analysis of magnetic resonance imaging characteristics and pain in temporomandibular joints with and without degenerative changes of the condyle. Int. J. Oral Maxillofac. Surg. 2008, 37, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Sonnesen, L.; Petersson, A.; Wiese, M.; Jensen, K.E.; Svanholt, P.; Bakke, M. Osseus osteoartritic-like changes and joint mobility of the temporomandibular joints and upper cervical spine: Is there a relation? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Hirata, F.H.; Guimarães, A.S.; de Oliveira, J.X.; Moreira, C.R.; Ferreira, E.T.T.; Cavalcanti, M.G.P. Evaluation of TMJ articular eminence morphology and disc patterns in patients with disc displacement in MRI. Braz. Oral Res. 2007, 21, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.; Detamore, M.; Mercuri, L. Degenerative Disorders of the Temporomandibular Joint: Etiology, Diagnosis, and Treatment. J. Dent. Res. 2008, 87, 296–307. [Google Scholar] [CrossRef]
- Taskaya-Yilmaz, N.; Ogutcen-Toller, M. Magnetic resonance imaging evaluation of temporomandibular joint disc de-formities in relation to type of disc displacement. J. Oral Maxillofac. Surg. 2001, 59, 860–865. [Google Scholar] [CrossRef]
- Santos, K.C.P.; Dutra, M.E.P.; Warmling, L.V.; Oliveira, J.X. Correlation Among the Changes Observed in Temporomandibular Joint Internal Derangements Assessed by Magnetic Resonance in Symptomatic Patients. J. Oral Maxillofac. Surg. 2013, 71, 1504–1512. [Google Scholar] [CrossRef]
- Okochi, K.; Ida, M.; Honda, E.; Kobayashi, K.; Kurabayashi, T. MRI and clinical findings of posterior disk displacement in the temporomandibular joint. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2008, 105, 644–648. [Google Scholar] [CrossRef]
- Rabelo, K.A.; Melo, S.L.S.; Torres, M.G.G.; Campos, P.S.F.; Bento, P.M.; de Melo, D.P. Condyle Excursion Angle, Articular Eminence Inclination, and Temporomandibular Joint Morphologic Relations With Disc Displacement. J. Oral Maxillofac. Surg. 2017, 75, 938.e1–938.e10. [Google Scholar] [CrossRef]
- Shahid, S.; Vojdani, M.; Paknahad, M. Correlation between articular eminence steepness measured with cone-beam com-puted tomography and clinical dysfunction index in patients with temporomandibular joint dysfunction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 91–97. [Google Scholar] [CrossRef]
- Erzurumlu, Z.U.; Celenk, P. A radiological evaluation of the effects of edentulousness on the temporomandibular joint. J. Oral Rehabil. 2019, 47, 319–324. [Google Scholar] [CrossRef]
- Ren, Y.-F.; Isberg, A.; Westesson, P.-L. Steepness of the articular eminence in the temporomandibular joint: Tomographic comparison between asymptomatic volunteers with normal disk position and patients with disk displacement. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1995, 80, 258–266. [Google Scholar] [CrossRef]
- Emshoff, R.; Rudisch, A.; Innerhofer, K.; Brandlmaier, I.; Moschen, I.; Bertram, S. Magnetic resonance imaging findings of in-ternal derangement in temporomandibular joints without a clinical diagnosis of temporomandibular disorder. J. Oral Rehab. 2002, 29, 516–522. [Google Scholar] [CrossRef]
- Manfredini, D.; Guarda-Nardini, L. Agreement between Research Diagnostic Criteria for Temporomandibular Disorders and Magnetic Resonance Diagnoses of Temporomandibular disc displacement in a patient population. Int. J. Oral Maxillofac. Surg. 2008, 37, 612–616. [Google Scholar] [CrossRef]
- Emshoff, R.; Rudisch, A. Validity of clinical diagnostic criteria for temporomandibular disorders: Clinical versus magnetic resonance imaging diagnosis of temporomandibular joint internal derangement and osteoarthrosis. Oral Surg. Oral Med. Oral Path. Oral Radiol. 2001, 91, 50–55. [Google Scholar] [CrossRef]
- Manoliu, A.; Spinner, G.; Wyss, M.; Erni, S.; Ettlin, D.A.; Nanz, D.; Ulbrich, E.J.; Gallo, L.; Andreisek, G. Quantitative and qualitative comparison of MR imaging of the temporomandibular joint at 1.5 and 3.0 T using an optimized high-resolution protocol. Dentomaxillofacial Radiol. 2016, 45, 20150240. [Google Scholar] [CrossRef]
- Marpaung, C.M.; Kalaykova, S.I.; Lobbezoo, F.; Naeije, M. Validity of functional diagnostic examination for temporoman-dibular joint disc displacement with reduction. J. Oral Rehab. 2014, 41, 243–249. [Google Scholar] [CrossRef]
- Vieira-Queiroz, I.; Gomes Torres, M.G.; de Oliveira-Santos, C.; Flores Campos, P.S.; Crusoe-Rebello, I.M. Biometric parameters of the temporomandibular joint and association with disc dispacement and pain: A magnetic resonance study. Int. J. Oral Maxillofac. Surg. 2013, 42, 765–770. [Google Scholar] [CrossRef]
- Ribeiro, R.F.; Tallents, R.H.; Katzberg, R.W.; Murphy, W.C.; Moss, M.E.; Magalhaes, A.C.; Tavano, O. The prevalence of disc displacement in symptomatic and asymptomatic volunteers aged 6 to 25 years. J. Orofac. Pain 1997, 11, 37–47. [Google Scholar]
- Hegab, A.F.; Al Hameed, H.I.; Karam, K.S. Classification of temporomandibular joint internal derangement based on magnetic resonance imaging and clinical findings of 435 patients contributing to a nonsurgical treatment protocol. Sci. Rep. 2021, 11, 20917. [Google Scholar] [CrossRef]
- Ahmad, M.; Hollender, L.; Anderson, Q.; Kartha, K.; Ohrbach, R.; Truelove, E.L.; John, M.T.; Schiffman, E.L. Research diagnostic criteria for tem-poromandibular disorders (RDC/TMD): Development of image analysis criteria and examiner reliability for image analysis. Oral Surg. Oral Med. Oral Path. Oral Radiol. 2009, 107, 844–860. [Google Scholar] [CrossRef] [PubMed]
- Jeremić-Knežević, M.; Boban, J.; Đurović-Koprivica, D.; Krstić, V.; Marković, V.; Knežević, A. Imaging of the temporoman-dibular joint: Contemporary clinical and radiological implications. Srp. Arh. Za Celok. Lekarstvo. 2020, 148, 242–250. [Google Scholar] [CrossRef]
- Cong, N.; Wang, N.; Huang, S.; Cheng, T.; Yan, X. Diagnostic significance of magnetic resonance imaging in distinguishing tem-poromandibular disorders: A retrospective chart review. BMC Oral Health 2021, 21, 481. [Google Scholar] [CrossRef] [PubMed]
- Krishnakumar Raja, V.B. Temporomandibular joint dislocation. In Oral and Maxillofacial Surgery for the Clinician; Bonanthaya, K., Panneerselvam, E., Manuel, S., Kumar, V.V., Rai, A., Eds.; Springer: Singapore, 2021; pp. 1381–1399. [Google Scholar]
- Vogl, T.J.; Günther, D.; Weigl, P.; Scholtz, J.-E. Diagnostic value of dynamic magnetic resonance imaging of temporomandibular joint dysfunction. Eur. J. Radiol. Open 2021, 8, 100390. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis based on RDC/TMD 1 Criteria | N (%) | Diagnosis based on MR Imaging | N (%) |
|---|---|---|---|
| Normal | 170 (86.7) | Normal | 99 (50.5) |
| Disc dislocation with reduction | 13 (6.6) | Anterior dislocation with reduction | 23(11.7) |
| Disc dislocation without reduction | 5 (2.6) | Anterior dislocation without reduction | 9 (4.6) |
| Posterior dislocation | 2 (1,0) | ||
| Arthralgia/Osteoarthritis/Osteoarthrosis | 5 (2.6) | Osteoarthritis | 46 (23.5) |
| Arthralgia/Osteoarthritis/Osteoarthrosis+ Disc dislocation with reduction | 2 (1.0) | Anterior dislocation with reduction + Osteoarthritis | 10 (5.1) |
| Arthralgia/Osteoarthritis/Osteoarthrosis+ Disc dislocation without reduction | 1 (0.5) | Anterior dislocation without reduction + Osteoarthritis | 10 (5.1) |
| Posterior dislocation + Osteoarthritis | 4 (2.0) | ||
| Total | 196 (100) | Total | 196 (100) |
| N | Mean | SD | Minimum | Maximum | F | p | ||
|---|---|---|---|---|---|---|---|---|
| Depth of GF (mm) | Normal | 145 | 4.00 | 1.10 | 2.00 | 7.00 | 1.417 | 0.245 |
| Anterior dislocation with reduction | 33 | 3.88 | 1.11 | 2.00 | 6.00 | |||
| Anterior dislocation without reduction | 12 | 4.50 | 1.17 | 3.00 | 6.00 | |||
| Total | 190 | 4.01 | 1.11 | 2.00 | 7.00 | |||
| Angle of articular eminence (o) | Normal | 145 | 46.36 | 6.37 | 31.00 | 64.00 | 0.531 | 0.589 |
| Anterior dislocation with reduction | 33 | 47.18 | 6.68 | 34.00 | 61.00 | |||
| Anterior dislocation without reduction | 12 | 48.00 | 5.39 | 39.00 | 55.00 | |||
| Total | 190 | 46.61 | 6.36 | 31.00 | 64.00 | |||
| Disc length (mm) | Normal | 145 | 9.98 | 1.73 | 6.00 | 14.00 | 1.188 | 0.307 |
| Anterior dislocation with reduction | 33 | 9.46 | 1.58 | 6.00 | 12.00 | |||
| Anterior dislocation without reduction | 12 | 10.00 | 2.76 | 4.00 | 13.00 | |||
| Total | 190 | 9.89 | 1.79 | 4.00 | 14.00 | |||
| Sensitivity | Specificity | K | p | |
|---|---|---|---|---|
| Normal | ||||
| Anterior DDWR | 24.2% | 94.9% | 0.240 | <0.001 |
| Anterior DDWOR | 25.0% | 99.4% | 0.355 | <0.001 |
| Disc dislocation overall | 31.1%. | 95.9% | 0.301 | <0.001 |
| Osteoarthritis of the TMJ | 4.8% | 96.2% | 0.013 | 0.740 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knezevic, M.J.; Knezevic, A.; Boban, J.; Maletin, A.; Milekic, B.; Koprivica, D.D.; Puskar, T.; Semnic, R. High-Field Magnetic Resonance Imaging of the Temporomandibular Joint Low Agreement with Clinical Diagnosis in Asymptomatic Females. Diagnostics 2023, 13, 1986. https://doi.org/10.3390/diagnostics13121986
Knezevic MJ, Knezevic A, Boban J, Maletin A, Milekic B, Koprivica DD, Puskar T, Semnic R. High-Field Magnetic Resonance Imaging of the Temporomandibular Joint Low Agreement with Clinical Diagnosis in Asymptomatic Females. Diagnostics. 2023; 13(12):1986. https://doi.org/10.3390/diagnostics13121986
Chicago/Turabian StyleKnezevic, Milica Jeremic, Aleksandar Knezevic, Jasmina Boban, Aleksandra Maletin, Bojana Milekic, Daniela Djurovic Koprivica, Tatjana Puskar, and Robert Semnic. 2023. "High-Field Magnetic Resonance Imaging of the Temporomandibular Joint Low Agreement with Clinical Diagnosis in Asymptomatic Females" Diagnostics 13, no. 12: 1986. https://doi.org/10.3390/diagnostics13121986
APA StyleKnezevic, M. J., Knezevic, A., Boban, J., Maletin, A., Milekic, B., Koprivica, D. D., Puskar, T., & Semnic, R. (2023). High-Field Magnetic Resonance Imaging of the Temporomandibular Joint Low Agreement with Clinical Diagnosis in Asymptomatic Females. Diagnostics, 13(12), 1986. https://doi.org/10.3390/diagnostics13121986