
Virtual Chromoendoscopy in Capsule Endoscopy: A Narrative Review


Abstract
1. Introduction
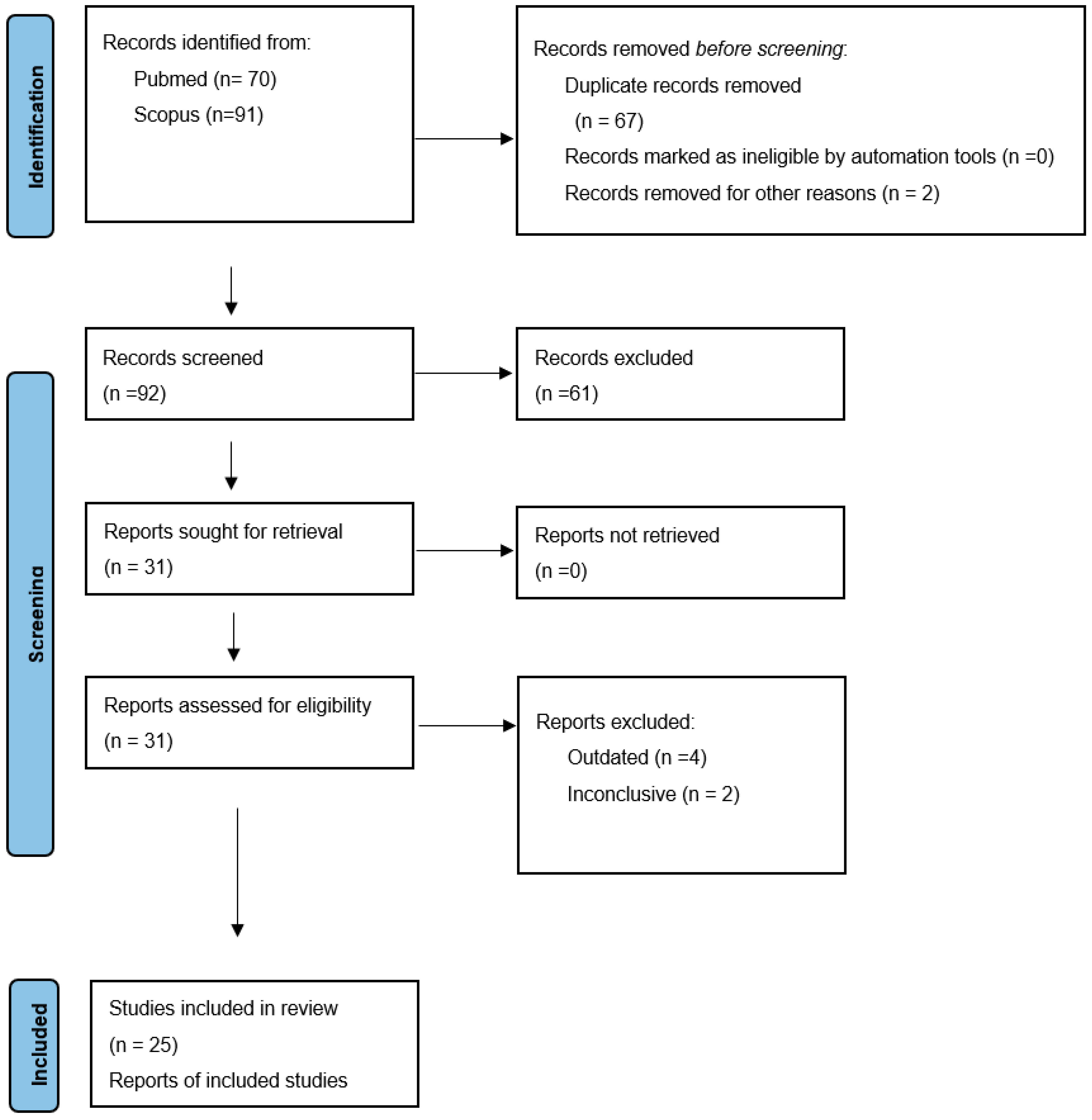
2. Materials and Methods
3. Discussion
3.1. Small Bowel Capsule Endoscopy
3.1.1. Angiectasias, Erosions/Ulcers and Tumors
3.1.2. Coeliac Disease
3.2. Colon Capsule Endoscopy
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yung, D.E.; Carvalho, P.B.; Giannakou, A.; Kopylov, U.; Rosa, B.; Rondonotti, E.; Toth, E.; Plevris, J.N.; Koulaouzidis, A. Clinical validity of flexible spectral imaging color enhancement (FICE) in small-bowel capsule endoscopy: A systematic review and meta-analysis. Endoscopy 2017, 49, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, J.R.; Pinho, R.; Rodrigues, A.; Ponte, A.; Rodrigues, J.; Sousa, M.; Carvalho, J. Evaluation of the Usefulness of Virtual Chromoendoscopy with Different Color Modes in the MiroCam® System for Characterization of Small Bowel Lesions. GE-Port. J. Gastroenterol. 2018, 25, 222–229. [Google Scholar] [CrossRef]
- Nakamura, M.; Ohmiya, N.; Miyahara, R.; Ando, T.; Watanabe, O.; Kawashima, H.; Itoh, A.; Hirooka, Y.; Goto, H. Usefulness of flexible spectral imaging color enhancement (FICE) for the detection of angiodysplasia in the preview of capsule endoscopy. Hepatogastroenterology 2012, 59, 1474–1477. [Google Scholar]
- Ogata, N.; Ohtsuka, K.; Ogawa, M.; Maeda, Y.; Ishida, F.; Kudo, S.E. Image-Enhanced Capsule Endoscopy Improves the Identification of Small Intestinal Lesions. Diagnostics 2021, 11, 2122. [Google Scholar] [CrossRef]
- Carvalho, P.B.; Magalhães, J.; de Castro, F.D.; Gonçalves, T.C.; Rosa, B.; Moreira, M.J.; Cotter, J. Virtual chromoendoscopy improves the diagnostic yield of small bowel capsule endoscopy in obscure gastrointestinal bleeding. Dig. Liver Dis. 2016, 48, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Van Gossum, A. Image-enhanced capsule endoscopy for characterization of small bowel lesions. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Ogata, N.; Ohtsuka, K.; Sasanuma, S.; Ogawa, M.; Maeda, Y.; Ichimasa, K.; Mori, Y.; Misawa, M.; Kudo, T.; Hisayuki, T.; et al. White light-emitting contrast image capsule endoscopy for visualization of small intestine lesions: A pilot study. Endosc. Int. Open 2018, 6, E315–E321. [Google Scholar] [CrossRef] [PubMed]
- Rimbaş, M.; Negreanu, L.; Ciobanu, L.; Benguş, A.; Spada, C.; Băicuş, C.R.; Costamagna, G. Is virtual chromoendoscopy useful in the evaluation of subtle ulcerative small-bowel lesions detected by video capsule endoscopy? Endosc. Int. Open 2015, 3, E615–E620. [Google Scholar] [CrossRef] [PubMed]
- Sakai, E.; Endo, H.; Kato, S.; Matsuura, T.; Tomeno, W.; Taniguchi, L.; Uchiyama, T.; Hata, Y.; Yamada, E.; Ohkubo, H.; et al. Capsule endoscopy with flexible spectral imaging color enhancement reduces the bile pigment effect and improves the detectability of small bowel lesions. BMC Gastroenterol. 2012, 12, 83. [Google Scholar] [CrossRef] [PubMed]
- Cotter, J.; Magalhães, J.; de Castro, F.D.; Barbosa, M.; Carvalho, P.B.; Leite, S.; Moreira, M.J.; Rosa, B. Virtual chromoendoscopy in small bowel capsule endoscopy: New light or a cast of shadow? World J. Gastrointest. Endosc. 2014, 6, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Sagawa, T.; Hirakawa, M.; Ohnuma, H.; Osuga, T.; Okagawa, Y.; Tamura, F.; Horiguchi, H.; Takada, K.; Hayashi, T.; et al. Clinical utility of capsule endoscopy with flexible spectral imaging color enhancement for diagnosis of small bowel lesions. Endosc. Int. Open 2014, 2, E80–E87. [Google Scholar]
- Dias de Castro, F.; Magalhães, J.; Boal Carvalho, P.; Cúrdia Gonçalves, T.; Rosa, B.; Moreira, M.J.; Cotter, J. Improving diagnostic yield in obscure gastrointestinal bleeding—How virtual chromoendoscopy may be the answer. Eur. J. Gastroenterol. Hepatol. 2015, 27, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Imagawa, H.; Oka, S.; Tanaka, S.; Noda, I.; Higashiyama, M.; Sanomura, Y.; Shishido, T.; Yoshida, S.; Chayama, K. Improved detectability of small-bowel lesions via capsule endoscopy with computed virtual chromoendoscopy: A pilot study. Scand. J. Gastroenterol. 2011, 46, 1133–1137. [Google Scholar] [CrossRef] [PubMed]
- Rincón, O.N.; Rodríguez, B.M.; Asanza, C.G.; Fernández-Pacheco, P.M. Utility of capsule endoscopy with flexible spectral imaging color enhancement in the diagnosis of small bowel lesions. Gastroenterol. Hepatol. 2013, 36, 63–68. [Google Scholar] [CrossRef]
- Pohl, J.; Aschmoneit, I.; Schuhmann, S.; Ell, C. Computed image modification for enhancement of small-bowel surface structures at video capsule endoscopy. Endoscopy 2010, 42, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Konishi, M.; Shibuya, T.; Mori, H.; Kurashita, E.; Takeda, T.; Nomura, O.; Fukuo, Y.; Matsumoto, K.; Sakamoto, N.; Osada, T.; et al. Usefulness of flexible spectral imaging color enhancement for the detection and diagnosis of small intestinal lesions found by capsule endoscopy. Scand. J. Gastroenterol. 2014, 49, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, T.; Fukumoto, A.; Shigita, K.; Asayama, N.; Mukai, S.; Nagata, S. Bile pigment in small-bowel water content may reflect bowel habits: A retrospective analysis of a capsule endoscopy imaging series. BMC Gastroenterol. 2020, 20, 237. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Watabe, H.; Yamada, A.; Hirata, Y.; Yamaji, Y.; Yoshida, H.; Koike, K. Efficacy of flexible spectral imaging color enhancement on the detection of small intestinal diseases by capsule endoscopy. J. Dig. Dis. 2012, 13, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Duque, G.; Almeida, N.; Figueiredo, P.; Monsanto, P.; Lopes, S.; Freire, P.; Ferreira, M.; Carvalho, R.; Gouveia, H.; Sofia, C. Virtual chromoendoscopy can be a useful software tool in capsule endoscopy. Rev. Esp. Enferm. Dig. 2012, 104, 231–236. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Krystallis, C.; Koulaouzidis, A.; Douglas, S.; Plevris, J.N. Chromoendoscopy in small bowel capsule endoscopy: Blue mode or Fuji Intelligent Colour Enhancement? Dig. Liver Dis. 2011, 43, 953–957. [Google Scholar] [CrossRef] [PubMed]
- Koulaouzidis, A.; Douglas, S.; Plevris, J.N. Blue mode does not offer any benefit over white light when calculating Lewis score in small-bowel capsule endoscopy. World J. Gastrointest. Endosc. 2012, 4, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Gupta, T.; Ibrahim, M.; Deviere, J.; Van Gossum, A. Evaluation of Fujinon intelligent chromo endoscopy-assisted capsule endoscopy in patients with obscure gastroenterology bleeding. World J. Gastroenterol. 2011, 17, 4590–4595. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, T.; Arai, M.; Sato, T.; Nakagawa, T.; Maruoka, D.; Tsuboi, M.; Hata, S.; Arai, E.; Katsuno, T.; Imazeki, F.; et al. Efficacy of computed image modification of capsule endoscopy in patients with obscure gastrointestinal bleeding. World J. Gastrointest. Endosc. 2012, 4, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Zammit, S.C.; McAlindon, M.E.; Ellul, P.; Rondonotti, E.; Carretero, C.; Sanders, D.S.; Sidhu, R. Improving Diagnostic Yield of Capsule Endoscopy in Coeliac Disease: Can Flexible Spectral Imaging Colour Enhancement Play a Role? Digestion 2020, 101, 347–354. [Google Scholar]
- Nakazawa, K.; Nouda, S.; Kakimoto, K.; Kinoshita, N.; Tanaka, Y.; Tawa, H.; Koshiba, R.; Naka, Y.; Hirata, Y.; Ota, K.; et al. The differential diagnosis of colorectal polyps using colon capsule endoscopy. Intern. Med. 2021, 60, 1805–1812. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Number of Patients Enrolled | FICE1 | FICE2 | FICE3 | BF | Conclusions |
|---|---|---|---|---|---|---|---|
| Ogata et al. [4] | 2018 | 24 |  | | | | Increased detectability of erosions/angioectasias/small ulcers. |
| Da Silva et al. [2] | 2018 | 22 |  | | | | No significant difference was found in detectability of small bowel vascular lesions between WLI and CE. |
| Rimbas et al. | 2015 | 250 | | |  | | Increased detectability of ulceration with CE vs. WLI. |
| Nakamura et al. [3] | 2012 | 50 | | | | NA | FICE readings had statistically significant better sensitivity (91% vs. 80%) in angiodysplasia. |
| Sakai et al. [9] | 2012 | 12 | | | | NA | FICE 1 and FICE 2 significantly improved the detectability of vascular lesions (angioectasias/erosions/ulcerations) (p < 0.01) |
| Cotter et al. [10] | 2014 | 49 | | | | | FICE 1 and FICE 2 significantly improved the delineation of vascular lesions. |
| Sato et al. [11] | 2014 | 50/189 images | | | | NA | FICE1 and FICE2 significantly improved the detectability of vascular lesions, with FICE 2 increasing the visibility of erosions/ulcers. |
| De Castro et al. [12] | 2015 | 42 | | | | NA | FICE 1 increased the detectability of previously missed erosions/angioectasias vs standard mode CE (p < 0.05). |
| Imagawa et al. [13] | 2011 | 50 | | | | NA | FICE 1 and 2 increased the detectability of angioectasias only (p < 0.001). |
| Rinkon et al. | 2013 | 41 | | | | NA | FICE 1 and 2 significantly increased the detection of vascular lesions/erosions and ulcers. |
| Carvahlo et al. | 2016 | 60 | | | | NA | FICE 1 significantly increased the detection of small erosions and angioectasias (P2 lesions) |
| Pohl et al. [15] | 2010 | 20 | | | | NA | FICE 1 increased the detectability of vascular lesions. |
| Konishi et al. [16] | 2014 | 10 | | | | NA | Increased detectability of vascular lesions and especially erosions and angioectasias with FICE 1 and 2 (p < 0.001) |
| Aoyama et al. [17] | 2020 | 134 | | | | NA | FICE1 was found useful in detection of vascular lesions and especially angioectasias.Only study that FICE1 was proven helpful in diagnosis of bile acid associated diarrhea. |
| Van Gossum et al. [6] | 2015 | 122 | NA | Improvement in detection of vascular lesions with FICE 1 and 2. | |||
| Nakazawa et al. [25] | 2021 | 51 | | | | | Improved differentiation of hyperplastic vs adenomatous polyps in colon capsule endoscopy. |
| Kalaouzidis et al. | 2012 | 27 | NA | NA | NA | | BF did not increase detectability of small bowel inflammation in IBD patients. |
| Krystallis et al. [20] | 2011 | 200 | | | | | BF significantly improved visibility of luminal blood and vascular lesions. |
| Duque et al. [19] | 2012 | 20 | NA | | NA | NA | FICE2 mode identified significantly more erosions but no gross lesions(p < 0.01). |
| Kobayashi et al. [18] | 2012 | 24 | | | | NA | FICE mode did not increase sensitivity or specificity over conventional CE for small bowel lesions overall.However, in per-lesion analysis, FICE 1 increased the detection of angioectasias (p < 0.05) but missed more tumors (p < 0.05). |
| Gupta et al. [22] | 2011 | 60 | | | | NA | No significant difference between FICE and WLI in OGIB. |
| Matsumura et al. [23] | 2012 | 81 | | | | NA | No significant difference between FICE and WLI in OGIB. |
| Chetkuti et al. | 2020 | 50 | | | | | No significant difference between FICE and WLI in coeliac disease. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toskas, A.; Laskaratos, F.-M.; Coda, S. Virtual Chromoendoscopy in Capsule Endoscopy: A Narrative Review. Diagnostics 2022, 12, 1818. https://doi.org/10.3390/diagnostics12081818
Toskas A, Laskaratos F-M, Coda S. Virtual Chromoendoscopy in Capsule Endoscopy: A Narrative Review. Diagnostics. 2022; 12(8):1818. https://doi.org/10.3390/diagnostics12081818
Chicago/Turabian StyleToskas, Alexandros, Faidon-Marios Laskaratos, and Sergio Coda. 2022. "Virtual Chromoendoscopy in Capsule Endoscopy: A Narrative Review" Diagnostics 12, no. 8: 1818. https://doi.org/10.3390/diagnostics12081818
APA StyleToskas, A., Laskaratos, F.-M., & Coda, S. (2022). Virtual Chromoendoscopy in Capsule Endoscopy: A Narrative Review. Diagnostics, 12(8), 1818. https://doi.org/10.3390/diagnostics12081818