
Maternal Mental Health Symptom Profiles and Infant Sleep: A Cross-Sectional Survey

 ,
,
Abstract
:1. Introduction
1.1. Comorbidity of Maternal Mental Health Difficulties and Their Influence on Infant Sleep
1.2. The Current Study
2. Materials and Methods
2.1. Study Design and Population
2.2. Infant and Maternal Measures
2.3. Procedure
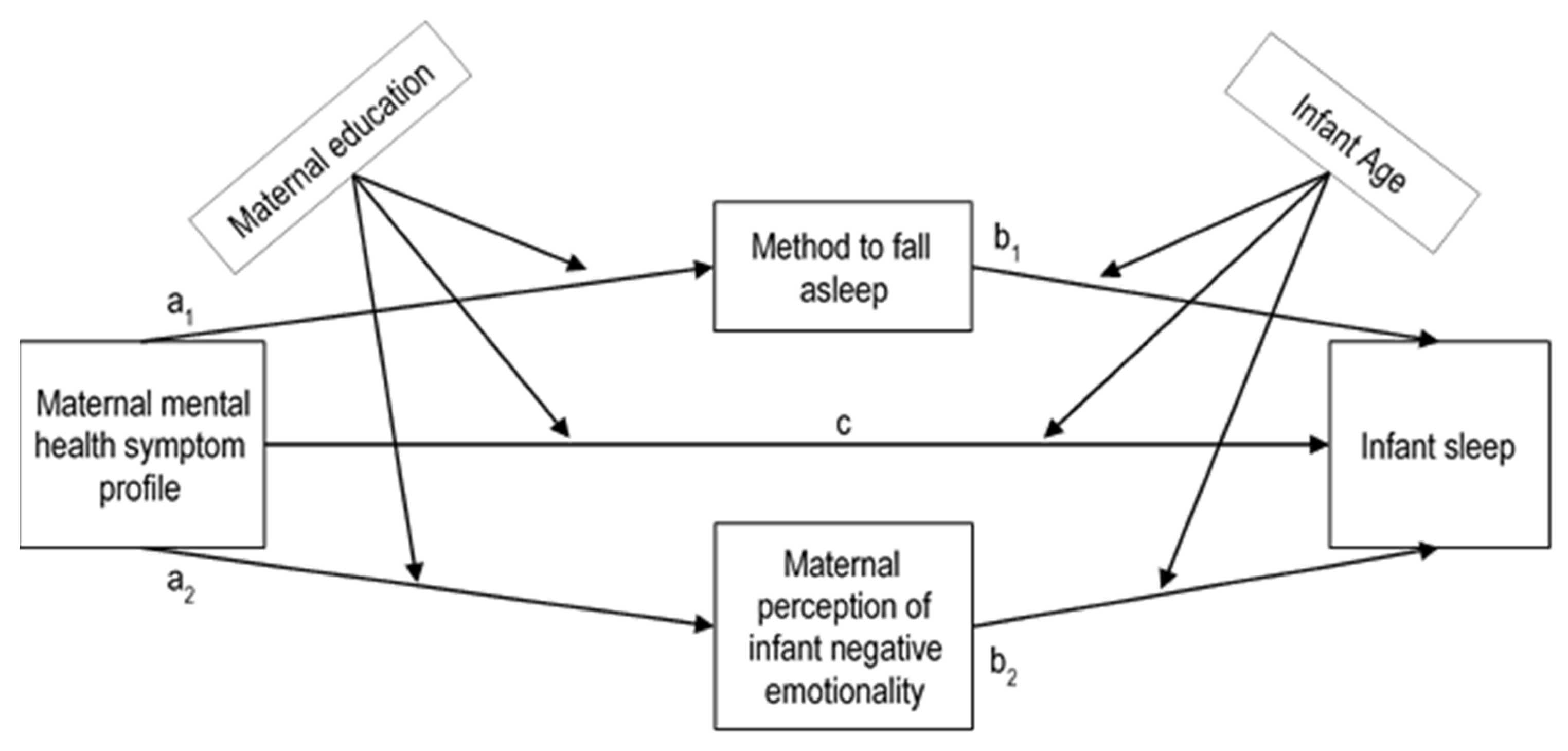
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Associations between Maternal Mental Health Symptoms and Infant Sleep Problems
3.3. Maternal Mental Health Symptom Profiles
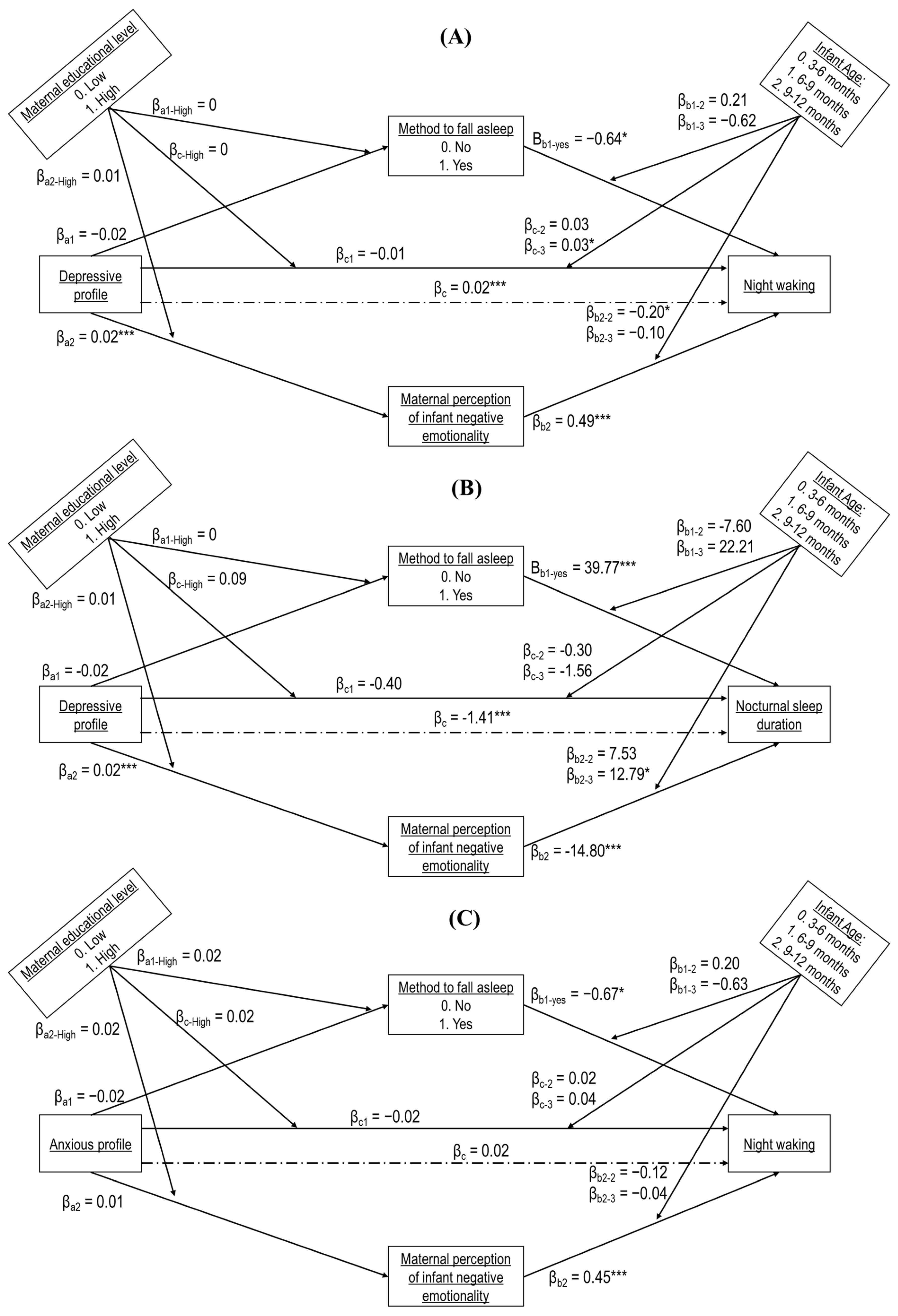
3.4. Associations of Maternal Mental Health Symptom Profiles to Infant Sleep Problems
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gustafsson, E. Les nuits et les pleurs des bébés. In La Science Au-Dessus du Berceau: La Recherche Au Service Des 0 à 6 Ans; Max Milo: Paris, France, 2020. [Google Scholar]
- Williamson, A.A.; Mindell, J.A.; Hiscock, H.; Quach, J. Child sleep behaviors and sleep problems from infancy to school-age. Sleep Med. 2019, 63, 5–8. [Google Scholar] [CrossRef]
- Byars, K.C.; Yolton, K.; Rausch, J.; Lanphear, B.; Beebe, D.W. Prevalence, patterns, and persistence of sleep problems in the first 3 years of life. Pediatrics 2012, 129, e276–e284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teti, D.M.; Crosby, B. Maternal depressive symptoms, dysfunctional cognitions, and infant night waking: The role of maternal nighttime behavior. Child Dev. 2012, 83, 939–953. [Google Scholar] [CrossRef]
- Cook, F.; Conway, L.; Gartland, D.; Giallo, R.; Keys, E.; Brown, S.A. Profiles and predictors of infant sleep problems across the first year. J. Dev. Behav. Pediatr. 2020, 41, 104–116. [Google Scholar] [CrossRef]
- Spruyt, K. A review of developmental consequences of poor sleep in childhood. Sleep Med. 2019, 60, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Kahn, A.; Mozin, M.J.; Rebuffat, E.; Sottiaux, M.; Muller, M.F. Milk intolerance in children with persistent sleeplessness: A prospective double-blind crossover evaluation. Pediatrics 1989, 84, 595–603. [Google Scholar] [CrossRef]
- Sadeh, A.; Tikotzky, L.; Scher, A. Parenting and infant sleep. Sleep Med. Rev. 2010, 14, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal depression: A systematic review of prevalence and incidence. Obstet. Gynecol. 2005, 106, 1071–1083. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef]
- Dennis, C.-L.; Falah-Hassani, K.; Shiri, R. Prevalence of antenatal and postnatal anxiety: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 210, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Grekin, R.; O’Hara, M.W. Prevalence and risk factors of postpartum posttraumatic stress disorder: A meta-analysis. Clin. Psychol. Rev. 2014, 34, 389–401. [Google Scholar] [CrossRef]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. The prevalence of posttraumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. J. Affect. Disord. 2017, 208, 634–647. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Ayers, S.; Wright, D.B.; Thornton, A. Development of a measure of postpartum PTSD: The City Birth Trauma Scale. Front. Psychiatry 2018, 9, 409. [Google Scholar] [CrossRef] [Green Version]
- Castro Dias, C.; Figueiredo, B. Mother’s prenatal and postpartum depression symptoms and infant’s sleep problems at 6 months. Infant Ment. Health J. 2020, 41, 614–627. [Google Scholar] [CrossRef]
- Petzoldt, J.; Wittchen, H.U.; Einsle, F.; Martini, J. Maternal anxiety versus depressive disorders: Specific relations to infants’ crying, feeding and sleeping problems. Child Care Health Dev. 2016, 42, 231–245. [Google Scholar] [CrossRef]
- Warren, S.L.; Gunnar, M.R.; Kagan, J.; Anders, T.F.; Simmens, S.J.; Rones, M.; Wease, S.; Aron, E.; Dahl, R.E.; Sroufe, A.L. Maternal panic disorder: Infant temperament, neurophysiology, and parenting behaviors. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 814–825. [Google Scholar] [CrossRef]
- Garthus-Niegel, S.; Horsch, A.; Bickle Graz, M.; Martini, J.; von Soest, T.; Weidner, K.; Eberhard-Gran, M. The prospective relationship between postpartum PTSD and child sleep: A 2-year follow-up study. J. Affect. Disord. 2018, 241, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Sadeh, A.; Anders, T.F. Infant sleep problems: Origins, assessment, interventions. Infant Ment. Health J. 1993, 14, 17–34. [Google Scholar] [CrossRef]
- Parade, S.H.; Wong, K.; Belair, R.; Dickstein, S.; Seifer, R. Infant sleep moderates the effect of infant temperament on maternal depressive symptoms, maternal sensitivity, and family functioning. Infant Behav. Dev. 2019, 57, 101343. [Google Scholar] [CrossRef]
- Field, T. Infant sleep problems and interventions: A review. Infant Behav. Dev. 2017, 47, 40–53. [Google Scholar] [CrossRef]
- Morrell, J.; Steele, H. The role of attachment security, temperament, maternal perception, and care-giving behavior in persistent infant sleeping problems. Infant Ment. Health J. 2003, 24, 447–468. [Google Scholar] [CrossRef]
- Burdayron, R.; Butler, B.P.; Béliveau, M.-J.; Dubois-Comtois, K.; Pennestri, M.-H. Perception of infant sleep problems: The role of negative affectivity and maternal depression. J. Clin. Sleep Med. 2021, 17, 1279–1285. [Google Scholar] [CrossRef]
- Dekel, S.; Ein-Dor, T.; Dishy, G.A.; Mayopoulos, P.A. Beyond postpartum depression: Posttraumatic stress-depressive response following childbirth. Arch. Women’s Ment. Health 2020, 23, 557–564. [Google Scholar] [CrossRef]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. Depression, anxiety, PTSD and comorbidity in perinatal women in Turkey: A longitudinal population-based study. Midwifery 2017, 55, 29–37. [Google Scholar] [CrossRef]
- Agius, A.; Xuereb, R.B.; Carrick-Sen, D.; Sultana, R.; Rankin, J. The co-existence of depression, anxiety and post-traumatic stress symptoms in the perinatal period: A systematic review. Midwifery 2016, 36, 70–79. [Google Scholar] [CrossRef]
- Gilbert, L.; Sandoz, V.; Quansah, D.Y.; Puder, J.; Horsch, A. Prospective associations between maternal depression and infant sleep in women with gestational diabetes mellitus. Front. Psychol. 2022, 13, 926315. [Google Scholar] [CrossRef]
- Sandoz, V.; Hingray, C.; Stuijfzand, S.; Lacroix, A.; El Hage, W.; Horsch, A. Measurement and conceptualization of maternal PTSD following childbirth: Psychometric properties of the City Birth Trauma Scale—French version (City BiTS-F). Psychol. Trauma Theory Res. Pract. Policy 2021, 14, 696–704. [Google Scholar] [CrossRef]
- Sadeh, A. A brief screening questionnaire for infant sleep problems: Validation and findings for an Internet sample. Pediatrics 2004, 113, e570–e577. [Google Scholar] [CrossRef] [Green Version]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P.; Translation, I.T.F.f.; Cultural, A. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [Green Version]
- Putnam, S.P.; Helbig, A.L.; Gartstein, M.A.; Rothbart, M.K.; Leerkes, E. Development and Assessment of Short and Very Short Forms of the Infant Behavior Questionnaire–Revised. J. Personal. Assess. 2014, 96, 445–458. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guedeney, N.; Fermanian, J. Validation study of the French version of the Edinburgh Postnatal Depression Scale (EPDS): New results about use and psychometric properties. Eur. Psychiatry 1998, 13, 83–89. [Google Scholar] [CrossRef]
- Sandoz, V.; Stuijfzand, S.; Lacroix, A.; Deforges, C.; Quillet Diop, M.; Ehlert, U.; Rubo, M.; Messerli-Bürgy, N.; Horsch, A. The Lausanne Infant Crying Stress Paradigm: Validation of an early postpartum stress paradigm with women at low- vs. high-risk of childbirth-related posttraumatic stress disorder. J. Pers. Med. 2021, 11, 472. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Bocéréan, C.; Dupret, E. A validation study of the Hospital Anxiety and Depression Scale (HADS) in a large sample of French employees. BMC Psychiatry 2014, 14, 354. [Google Scholar] [CrossRef] [Green Version]
- Horsch, A.; Vial, Y.; Favrod, C.; Morisod Harari, M.; Blackwell, S.E.; Watson, P.; Iyadurai, L.; Bonsall, M.B.; Holmes, E.A. Reducing intrusive traumatic memories after emergency caesarean section: A proof-of-principle randomized controlled study. Behav. Res. Ther. 2017, 94, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Sandoz, V.; Horsch, A. Dataset of The Distinct Influence of Different Maternal Mental Health Symptom Profiles on Infant Sleep During the First Year Postpartum: A Cross-Sectional Survey. 2021. Available online:. Available online: https://zenodo.org/record/5070945#.YsOb8IRByUk (accessed on 4 May 2022).
- Barrett, P. Structural equation modelling: Adjudging model fit. Personal. Individ. Differ. 2007, 42, 815–824. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Sobel, M.E. Asymptotic Confidence Intervals for Indirect Effects in Structural Equation Models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Thoemmes, F.; MacKinnon, D.P.; Reiser, M.R. Power Analysis for Complex Mediational Designs Using Monte Carlo Methods. Struct. Equ. Model. Multidiscip. J. 2010, 17, 510–534. [Google Scholar] [CrossRef]
- Davies, J.; Slade, P.; Wright, I.; Stewart, P. Posttraumatic stress symptoms following childbirth and mothers’ perceptions of their infants. Infant Ment. Health J. 2008, 29, 537–554. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.E.; Ayers, S.; Quigley, M.A.; Stein, A.; Alderdice, F. Prevalence and factors associated with postpartum posttraumatic stress in a population-based maternity survey in England. J. Affect. Disord. 2020, 279, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Sechi, C.; Vismara, L.; Rollè, L.; Prino, L.E.; Lucarelli, L. First-Time Mothers’ and Fathers’ Developmental Changes in the Perception of Their Daughters’ and Sons’ Temperament: Its Association With Parents’ Mental Health. Front. Psychol. 2020, 11, 02066. [Google Scholar] [CrossRef]
- Cornish, A.M.; McMahon, C.A.; Ungerer, J.A.; Barnett, B.; Kowalenko, N.; Tennant, C. Maternal depression and the experience of parenting in the second postnatal year. J. Reprod. Infant Psychol. 2006, 24, 121–132. [Google Scholar] [CrossRef]
- McMahon, C.; Barnett, B.; Kowalenko, N.; Tennant, C.; Don, N. Postnatal Depression, Anxiety and Unsettled Infant Behaviour. Aust. N. Z. J. Psychiatry 2001, 35, 581–588. [Google Scholar] [CrossRef]
- Sadeh, A.; Flint-Ofir, E.; Tirosh, T.; Tikotzky, L. Infant sleep and parental sleep-related cognitions. J. Fam. Psychol. JFP J. Div. Fam. Psychol. Am. Psychol. Assoc. 2007, 21, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.M.T.; France, K.G.; Blampied, N.M. The consolidation of infants’ nocturnal sleep across the first year of life. Sleep Med. Rev. 2011, 15, 211–220. [Google Scholar] [CrossRef]
- Thirion, M.; Challamel, M.-J. Le Sommeil, Le Rêve Et L’enfant; Albin Michel: Paris, France, 2011. [Google Scholar]
- Magarey, A.; Kavian, F.; Scott, J.A.; Markow, K.; Daniels, L. Feeding mode of Australian infants in the first 12 months of life: An assessment against national breastfeeding indicators. J. Hum. Lact. 2015, 32, NP95–NP104. [Google Scholar] [CrossRef] [Green Version]
- Nakić Radoš, S.; Matijaš, M.; Anđelinović, M.; Čartolovni, A.; Ayers, S. The role of posttraumatic stress and depression symptoms in mother-infant bonding. J. Affect. Disord. 2020, 268, 134–140. [Google Scholar] [CrossRef]
- Quante, M.; Hong, B.; von Ash, T.; Yu, X.; Kaplan, E.R.; Rueschman, M.; Jackson, C.L.; Haneuse, S.; Davison, K.; Taveras, E.M.; et al. Associations between parent-reported and objectively measured sleep duration and timing in infants at age 6 months. Sleep 2021, 44, zsaa217. [Google Scholar] [CrossRef]
- Castro Dias, C.; Figueiredo, B. Unidirectional and bidirectional links between maternal depression symptoms and infant sleep problems. J. Sleep Res. 2021, 30, e13363. [Google Scholar] [CrossRef]
- Lam, P.; Hiscock, H.; Wake, M. Outcomes of infant sleep problems: A longitudinal study of sleep, behavior, and maternal well-being. Pediatrics 2003, 111, e203–e207. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Variables | Participants (n = 410) | |
|---|---|---|
| M (SD) | n (%) | |
| Maternal age | 30.20 (4.36) | |
| Educational level | ||
| No education | 2 (0.5) | |
| Compulsory education | 25 (6.1) | |
| Post-compulsory education (e.g., apprenticeship) | 103 (25.1) | |
| University of Applied Science or University Diploma of Technology Degree | 88 (21.5) | |
| University | 192 (46.8) | |
| Marital status | ||
| Single | 14 (3.4) | |
| In a couple relationship | 389 (94.9) | |
| Separated, divorced, or widowed | 7 (1.7) | |
| EPDS total score | 9.05 (6.76) | |
| HADS-A total score | 7.84 (4.26) | |
| City BiTS total score | 13.12 (10.81) | |
| Infant gender | ||
| Female | 212 (51.7) | |
| Male | 198 (48.3) | |
| Weeks of gestation | 39.11 (1.90) | |
| Infant age | ||
| ≥3 months to <6 months | 147 (35.9) | |
| ≥6 months to <9 months | 133 (32.4) | |
| ≥9 months to <12 months | 130 (31.7) | |
| Nocturnal sleep duration (min) | 611.04 (85.985) | |
| Missing data | 1 (0.2) | |
| Night waking | 1.44 (1.59) | |
| Method of falling asleep | ||
| While being fed | 90 (22) | |
| While being rocked | 74 (18) | |
| While being held | 22 (5.4) | |
| Alone in the crib | 177 (43.2) | |
| In the crib with parental presence | 47 (11.5) | |
| IBQ-NEG | 3.36 (1.10) | |
| Model | Predictor | Dependent Variable | n | β | R2 | F | p |
|---|---|---|---|---|---|---|---|
| 1 | EPDS | Night waking | 410 | 0.03 | 0.019 | 8.08 | 0.005 |
| 2 | EPDS | Nocturnal sleep duration | 409 | −2.51 | 0.039 | 16.54 | <0.001 |
| 3 | HADS-A | Night waking | 410 | 0.04 | 0.011 | 4.49 | 0.035 |
| 4 | HADS-A | Nocturnal sleep duration | 409 | −2.59 | 0.016 | 6.77 | 0.010 |
| 5 | City BiTS | Night waking | 410 | 0.01 | 0.004 | 1.60 | 0.207 |
| 6 | City BiTS | Nocturnal sleep duration | 409 | −0.80 | 0.010 | 4.17 | 0.042 |
| Items | Depressive Profile | Birth Trauma Profile | Anxious Profile |
|---|---|---|---|
| EPDS | |||
| 1. Being able to laugh and see the funny side of things. | 0.70 | ||
| 2. Looking forward with enjoyment to things. | 0.62 | ||
| 3. Blaming oneself unnecessarily when things went wrong. | 0.51 | ||
| 4. Being anxious or worried for no good reason. | 0.65 | ||
| 5. Feeling scared or panicky for no very good reason. | 0.66 | ||
| 6. Things have been getting on top of oneself. | 0.53 | ||
| 7. Being so unhappy that one have had difficulty sleeping. | 0.51 | 0.44 | |
| 8. Feeling sad or miserable. | 0.70 | ||
| 9. Being so unhappy that one has been crying. | 0.65 | ||
| 10. The thought of harming oneself has occurred. | 0.49 | ||
| HADS-A | |||
| 1. Feeling tense or angry. | 0.64 | ||
| 2. Feeling scared like something might happen to oneself. | 0.64 | ||
| 3. Worrying. | 0.66 | ||
| 4. Sitting restfully doing nothing and feeling calm. | 0.41 | ||
| 5. Feeling scared and having knots in one’s stomach. | 0.64 | ||
| 6. Feeling restless and finding it difficult to stay in place. | |||
| 7. Often feeling panicky. | 0.71 | ||
| City BiTS: birth-related symptoms | |||
| 1. Recurrent unwanted memories of the birth. | 0.71 | ||
| 2. Bad dreams or nightmares about the birth. | 0.49 | ||
| 3. Flashbacks to the birth and/or reliving the experience. | 0.49 | ||
| 4. Getting upset when reminded of the birth. | 0.79 | ||
| 5. Feeling tense or anxious when reminded of the birth. | 0.80 | ||
| 6. Trying to avoid thinking about the birth. | 0.77 | ||
| 7. Trying to avoid things that remind me of the birth. | 0.70 | ||
| 8. Not able to remember details of the birth. | |||
| 9. Blaming myself or others for what happened during the birth. | 0.62 | ||
| 10. Feeling strong negative emotions about the birth. | 0.70 | ||
| City BiTS: General symptoms | |||
| 11. Feeling negative about myself or thinking something awful will happen. | 0.45 | 0.48 | |
| 12. Lost interest in activities that were important to me. | 0.65 | ||
| 13. Feeling detached from other people. | 0.69 | ||
| 14. Not able to feel positive emotions. | 0.70 | ||
| 15. Feeling irritable or aggressive. | 0.74 | ||
| 16. Feeling self-destructive or acting recklessly. | 0.50 | ||
| 17. Feeling tense and on edge. | 0.73 | ||
| 18. Feeling jumpy or easily startled. | |||
| 19. Problems concentrating. | 0.60 | ||
| 20. Not sleeping well … not due to the baby’s sleep pattern. | 0.45 | ||
| Cronbach α, 95% CI | 0.94, [0.93, 0.95] | 0.87, [0.87, 0.90] | 0.91, [0.89, 0.92] |
| Independent Variable | Dependent Variable | Mediator | Covariate | Moderator | ACME, 95% CI | p | Power Monte Carlo (Sobel) |
|---|---|---|---|---|---|---|---|
| Model 1 | |||||||
| Depressive profile | Night waking | IBQ-NEG | Method of falling asleep | Infant age: ≥3 months to <6 months | 0.013, [0.006, 0.024] | <0.001 | 0.97 (0.82) |
| Depressive profile | Night waking | IBQ-NEG | Method of falling asleep | Infant age: ≥6 months to <9 months | 0.006, [0.001, 0.014] | 0.02 | 0.61 (0.47) |
| Depressive profile | Night waking | IBQ-NEG | Method of falling asleep | Infant age: ≥9 months to <12 months | 0.009, [0.001, 0.024] | 0.028 | 0.60 (0.48) |
| Model 2 | |||||||
| Depressive profile | Night waking | IBQ-NEG | Method of falling asleep | Low educational level | 0.007, [0.002, 0.015] | 0.004 | 0.73 (0.58) |
| Depressive profile | Night waking | IBQ-NEG | Method of falling asleep | High educational level | 0.009, [0.004, 0.017] | <0.001 | 0.98 (0.87) |
| Model 3 | |||||||
| Depressive profile | Nocturnal sleep duration | IBQ-NEG | Method of falling asleep | Infant age: ≥6 months to <9 months | −0.296, [−0.677, −0.067] | 0.012 | 0.57 (0.44) |
| Model 4 | |||||||
| Anxious profile | Night waking | IBQ-NEG | Method of falling asleep | Infant age: ≥3 months to <6 months | 0.013, [0.004, 0.026] | <0.001 | 0.70 (0.55) |
| Model 5 | |||||||
| Anxious profile | Night waking | IBQ-NEG | Method of falling asleep | High educational level | 0.009, [0.001, 0.021] | 0.032 | 0.50 (0.48) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sandoz, V.; Lacroix, A.; Stuijfzand, S.; Bickle Graz, M.; Horsch, A. Maternal Mental Health Symptom Profiles and Infant Sleep: A Cross-Sectional Survey. Diagnostics 2022, 12, 1625. https://doi.org/10.3390/diagnostics12071625
Sandoz V, Lacroix A, Stuijfzand S, Bickle Graz M, Horsch A. Maternal Mental Health Symptom Profiles and Infant Sleep: A Cross-Sectional Survey. Diagnostics. 2022; 12(7):1625. https://doi.org/10.3390/diagnostics12071625
Chicago/Turabian StyleSandoz, Vania, Alain Lacroix, Suzannah Stuijfzand, Myriam Bickle Graz, and Antje Horsch. 2022. "Maternal Mental Health Symptom Profiles and Infant Sleep: A Cross-Sectional Survey" Diagnostics 12, no. 7: 1625. https://doi.org/10.3390/diagnostics12071625
APA StyleSandoz, V., Lacroix, A., Stuijfzand, S., Bickle Graz, M., & Horsch, A. (2022). Maternal Mental Health Symptom Profiles and Infant Sleep: A Cross-Sectional Survey. Diagnostics, 12(7), 1625. https://doi.org/10.3390/diagnostics12071625