
Increased Levels of Plasma Alzheimer’s Disease Biomarkers and Their Associations with Brain Structural Changes and Carotid Intima-Media Thickness in Cognitively Normal Obstructive Sleep Apnea Patients


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Neuropsychological Assessments and Carotid IMT Measurement
2.3. Blood Samples and Assessment of Plasma AD Biomarkers (Aβ-40, Aβ-42, T-tau)
2.4. MRI Data Acquisition
Image Acquisition
2.5. Image Preprocessing
2.6. Statistical Analyses
2.6.1. Analyses of Demographic Data, Plasma Biomarkers, Clinical Assessments, and Neuropsychological Testing
2.6.2. Voxel-Based Morphometry Analysis
3. Results
3.1. Baseline Clinical Characteristics of OSA Patients and Controls
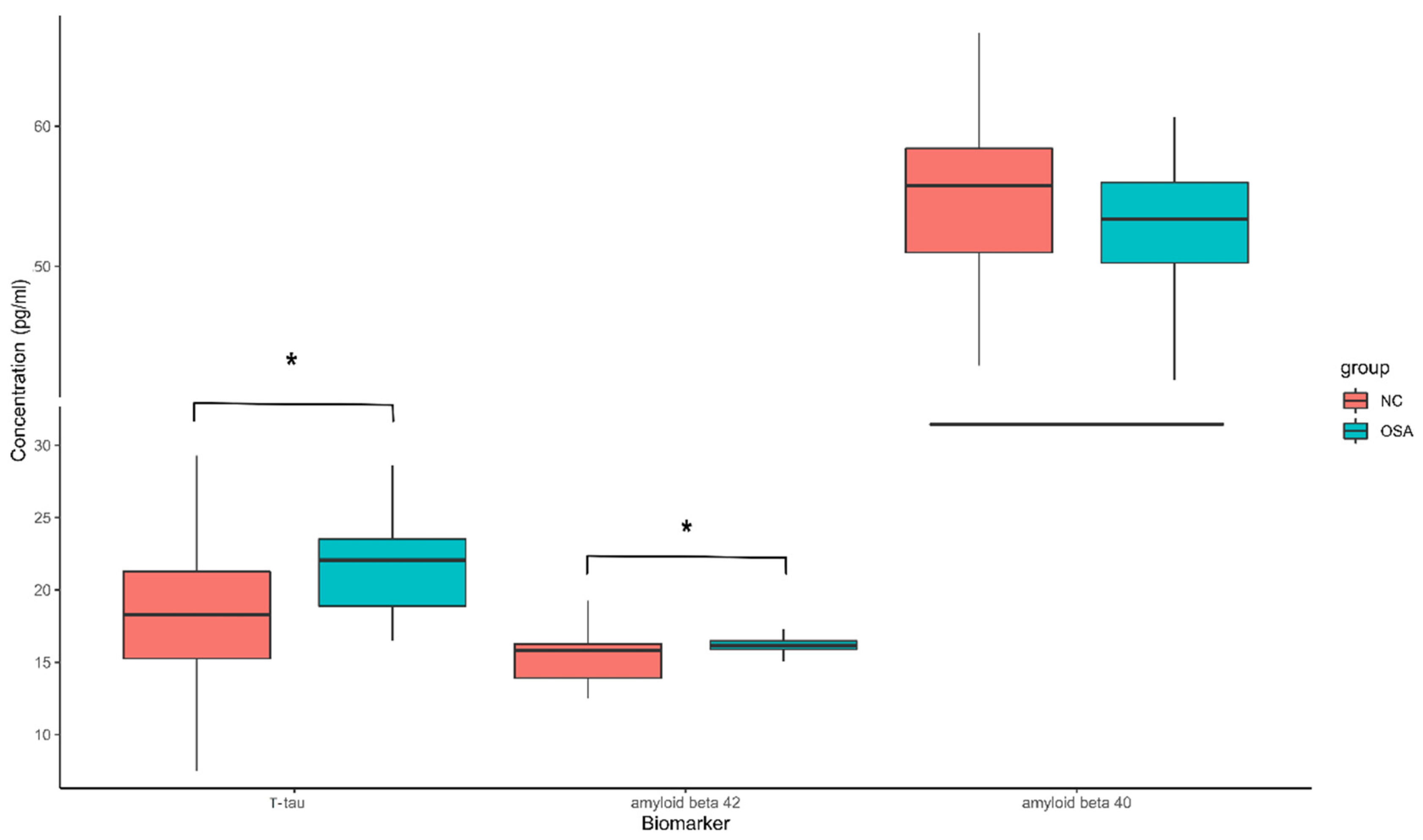
3.2. Plasma Biomarkers between OSA Patients and Controls
3.3. Comparison of Regional GMV between OSA Patients and Controls
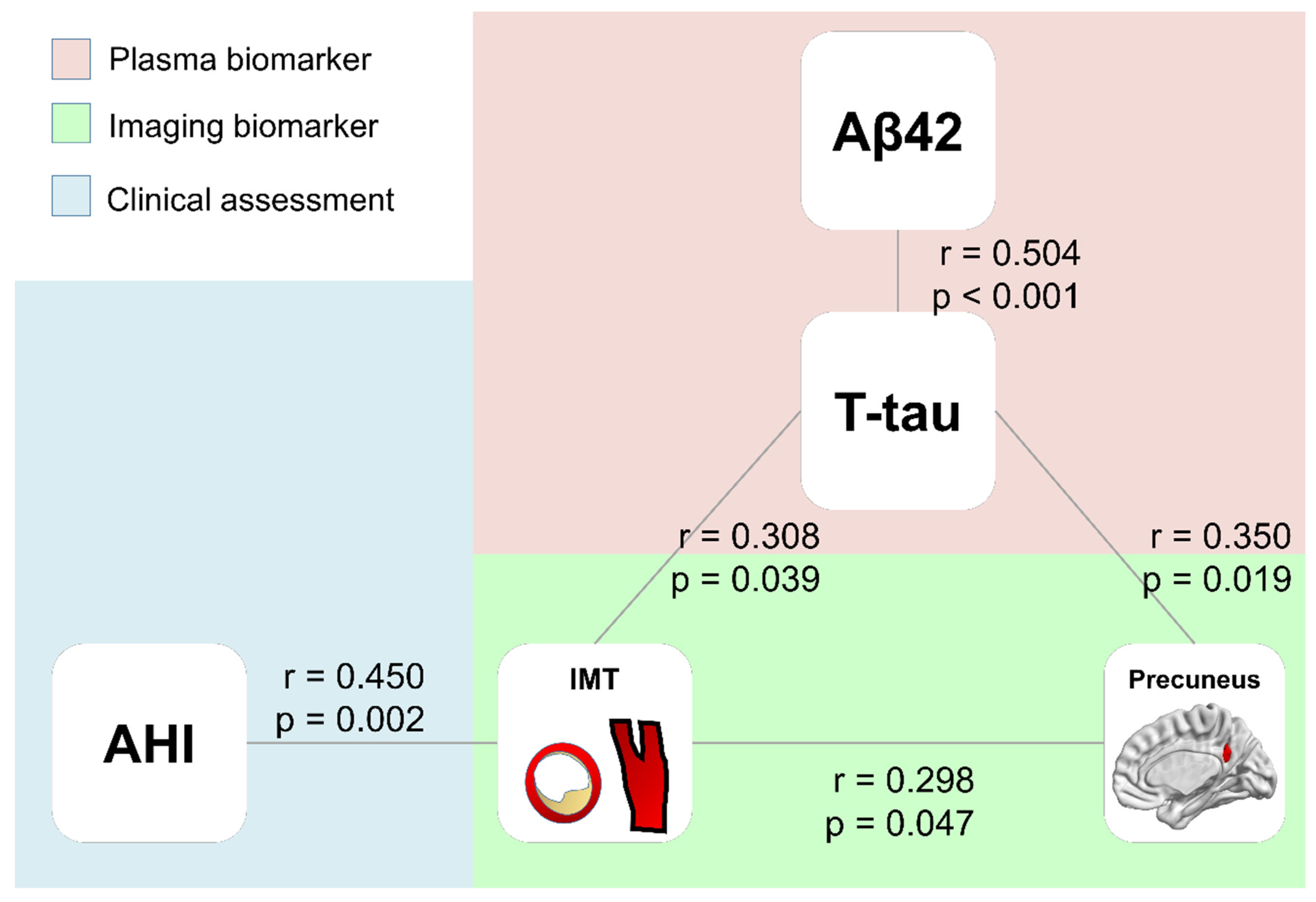
3.4. Correlations between Plasma Biomarkers, Clinical Parameters, and Volumes of the Right Precuneus
3.5. Correlations between Cognitive Function and Plasma Biomarkers, Clinical Parameters, and Volumes of Right Precuneus
4. Discussion
5. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Malhotra, A.; White, D.P. Obstructive sleep apnoea. Lancet 2002, 360, 237–245. [Google Scholar] [CrossRef]
- Spira, A.P.; Yager, C.; Brandt, J.; Smith, G.S.; Zhou, Y.; Mathur, A.; Kumar, A.; Brasic, J.R.; Wong, D.F.; Wu, M.N. Objectively Measured Sleep and beta-amyloid Burden in Older Adults: A Pilot Study. SAGE Open Med. 2014, 2, 2050312114546520. [Google Scholar] [CrossRef] [PubMed]
- Yun, C.H.; Lee, H.Y.; Lee, S.K.; Kim, H.; Seo, H.S.; Bang, S.A.; Kim, S.E.; Greve, D.N.; Au, R.; Shin, C.; et al. Amyloid Burden in Obstructive Sleep Apnea. J. Alzheimers Dis. 2017, 59, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Blennow, K.; de Leon, M.J.; Zetterberg, H. Alzheimer’s disease. Lancet 2006, 368, 387–403. [Google Scholar] [CrossRef]
- Bubu, O.M.; Pirraglia, E.; Andrade, A.G.; Sharma, R.A.; Gimenez-Badia, S.; Umasabor-Bubu, O.Q.; Hogan, M.M.; Shim, A.M.; Mukhtar, F.; Sharma, N.; et al. Obstructive sleep apnea and longitudinal Alzheimer’s disease biomarker changes. Sleep 2019, 42, zsz048. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Lu, X.; Zhang, L.; Shu, H.; Gu, L.; Wang, Z.; Gao, L.; Zhu, J.; Zhang, H.; Zhou, D.; et al. Potential Value of Plasma Amyloid-beta, Total Tau, and Neurofilament Light for Identification of Early Alzheimer’s Disease. ACS Chem. Neurosci. 2019, 10, 3479–3485. [Google Scholar] [CrossRef] [PubMed]
- Yaggi, H.K.; Concato, J.; Kernan, W.N.; Lichtman, J.H.; Brass, L.M.; Mohsenin, V. Obstructive sleep apnea as a risk factor for stroke and death. N. Engl. J. Med. 2005, 353, 2034–2041. [Google Scholar] [CrossRef] [Green Version]
- Yeghiazarians, Y.; Jneid, H.; Tietjens, J.R.; Redline, S.; Brown, D.L.; El-Sherif, N.; Mehra, R.; Bozkurt, B.; Ndumele, C.E.; Somers, V.K. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e56–e67. [Google Scholar] [CrossRef]
- Chang, Y.T.; Lin, H.C.; Chang, W.N.; Tsai, N.W.; Huang, C.C.; Wang, H.C.; Kung, C.T.; Su, Y.J.; Lin, W.C.; Cheng, B.C.; et al. Impact of inflammation and oxidative stress on carotid intima-media thickness in obstructive sleep apnea patients without metabolic syndrome. J. Sleep Res. 2017, 26, 151–158. [Google Scholar] [CrossRef]
- Ciccone, M.M.; Scicchitano, P.; Zito, A.; Cortese, F.; Boninfante, B.; Falcone, V.A.; Quaranta, V.N.; Ventura, V.A.; Zucano, A.; Di Serio, F.; et al. Correlation between inflammatory markers of atherosclerosis and carotid intima-media thickness in Obstructive Sleep Apnea. Molecules 2014, 19, 1651–1662. [Google Scholar] [CrossRef]
- Nelson, A.R.; Sweeney, M.D.; Sagare, A.P.; Zlokovic, B.V. Neurovascular dysfunction and neurodegeneration in dementia and Alzheimer’s disease. Biochim. Biophys. Acta 2016, 1862, 887–900. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Chen, L.; Chen, T.; Li, L.; Dai, J.; Lui, S.; Huang, X.; Sweeney, J.A.; Gong, Q. A Meta-analysis of Voxel-based Brain Morphometry Studies in Obstructive Sleep Apnea. Sci. Rep. 2017, 7, 10095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeung, A.W.K. Morphometric and functional connectivity changes in the brain of patients with obstructive sleep apnea: A meta-analysis. J. Sleep Res. 2019, 28, e12857. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar] [PubMed]
- Wechsler, D. Wechsler Memory Scale-(WMS-III) Chinese Version: Administration and Scoring Manual; The Chinese Behavioral Science Corporation: Taibei, Taiwan, 2005. [Google Scholar]
- Lin, K.N.; Wang, P.N.; Liu, H.C.; Teng, E.L. Cognitive Abilities Screening Instrument, Chinese Version 2.0 (CASI C-2.0): Administration and clinical application. Acta Neurol. Taiwan 2012, 21, 180–189. [Google Scholar]
- Lin, C.H.; Yang, S.Y.; Horng, H.E.; Yang, C.C.; Chieh, J.J.; Chen, H.H.; Liu, B.H.; Chiu, M.J. Plasma alpha-synuclein predicts cognitive decline in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2017, 88, 818–824. [Google Scholar] [CrossRef]
- Yang, S.Y.; Chiu, M.J.; Lin, C.H.; Horng, H.E.; Yang, C.C.; Chieh, J.J.; Chen, H.H.; Liu, B.H. Development of an ultra-high sensitive immunoassay with plasma biomarker for differentiating Parkinson disease dementia from Parkinson disease using antibody functionalized magnetic nanoparticles. J. Nanobiotechnol. 2016, 14, 41. [Google Scholar] [CrossRef] [Green Version]
- Teunissen, C.E.; Chiu, M.J.; Yang, C.C.; Yang, S.Y.; Scheltens, P.; Zetterberg, H.; Blennow, K. Plasma Amyloid-beta (Abeta42) Correlates with Cerebrospinal Fluid Abeta42 in Alzheimer’s Disease. J. Alzheimers Dis. 2018, 62, 1857–1863. [Google Scholar] [CrossRef]
- Yang, S.Y.; Chiu, M.J.; Chen, T.F.; Lin, C.H.; Jeng, J.S.; Tang, S.C.; Lee, Y.F.; Yang, C.C.; Liu, B.H.; Chen, H.H.; et al. Analytical performance of reagent for assaying tau protein in human plasma and feasibility study screening neurodegenerative diseases. Sci. Rep. 2017, 7, 9304. [Google Scholar] [CrossRef] [Green Version]
- Ju, Y.E.; Finn, M.B.; Sutphen, C.L.; Herries, E.M.; Jerome, G.M.; Ladenson, J.H.; Crimmins, D.L.; Fagan, A.M.; Holtzman, D.M. Obstructive sleep apnea decreases central nervous system-derived proteins in the cerebrospinal fluid. Ann. Neurol. 2016, 80, 154–159. [Google Scholar] [CrossRef] [Green Version]
- Kheirandish-Gozal, L.; Philby, M.F.; Alonso-Alvarez, M.L.; Teran-Santos, J.; Gozal, D. Biomarkers of Alzheimer Disease in Children with Obstructive Sleep Apnea: Effect of Adenotonsillectomy. Sleep 2016, 39, 1225–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, R.A.; Varga, A.W.; Bubu, O.M.; Pirraglia, E.; Kam, K.; Parekh, A.; Wohlleber, M.; Miller, M.D.; Andrade, A.; Lewis, C.; et al. Obstructive Sleep Apnea Severity Affects Amyloid Burden in Cognitively Normal Elderly. A Longitudinal Study. Am. J. Respir. Crit. Care Med. 2018, 197, 933–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, S.Y.; Chiu, M.J.; Chen, T.F.; Horng, H.E. Detection of Plasma Biomarkers Using Immunomagnetic Reduction: A Promising Method for the Early Diagnosis of Alzheimer’s Disease. Neurol. Ther. 2017, 6, 37–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bu, X.L.; Liu, Y.H.; Wang, Q.H.; Jiao, S.S.; Zeng, F.; Yao, X.Q.; Gao, D.; Chen, J.C.; Wang, Y.J. Serum amyloid-beta levels are increased in patients with obstructive sleep apnea syndrome. Sci. Rep. 2015, 5, 13917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, A.; Kaneko, N.; Villemagne, V.L.; Kato, T.; Doecke, J.; Dore, V.; Fowler, C.; Li, Q.X.; Martins, R.; Rowe, C.; et al. High performance plasma amyloid-beta biomarkers for Alzheimer’s disease. Nature 2018, 554, 249–254. [Google Scholar] [CrossRef]
- Chen, Z.; Mengel, D.; Keshavan, A.; Rissman, R.A.; Billinton, A.; Perkinton, M.; Percival-Alwyn, J.; Schultz, A.; Properzi, M.; Johnson, K.; et al. Learnings about the complexity of extracellular tau aid development of a blood-based screen for Alzheimer’s disease. Alzheimers Dement. 2019, 15, 487–496. [Google Scholar] [CrossRef]
- Ovod, V.; Ramsey, K.N.; Mawuenyega, K.G.; Bollinger, J.G.; Hicks, T.; Schneider, T.; Sullivan, M.; Paumier, K.; Holtzman, D.M.; Morris, J.C.; et al. Amyloid beta concentrations and stable isotope labeling kinetics of human plasma specific to central nervous system amyloidosis. Alzheimers Dement. 2017, 13, 841–849. [Google Scholar] [CrossRef]
- Bu, X.L.; Xiang, Y.; Jin, W.S.; Wang, J.; Shen, L.L.; Huang, Z.L.; Zhang, K.; Liu, Y.H.; Zeng, F.; Liu, J.H.; et al. Blood-derived amyloid-beta protein induces Alzheimer’s disease pathologies. Mol. Psychiatry 2018, 23, 1948–1956. [Google Scholar] [CrossRef]
- Wang, Y.R.; Wang, Q.H.; Zhang, T.; Liu, Y.H.; Yao, X.Q.; Zeng, F.; Li, J.; Zhou, F.Y.; Wang, L.; Yan, J.C.; et al. Associations Between Hepatic Functions and Plasma Amyloid-Beta Levels-Implications for the Capacity of Liver in Peripheral Amyloid-Beta Clearance. Mol. Neurobiol. 2017, 54, 2338–2344. [Google Scholar] [CrossRef]
- Xiang, Y.; Bu, X.L.; Liu, Y.H.; Zhu, C.; Shen, L.L.; Jiao, S.S.; Zhu, X.Y.; Giunta, B.; Tan, J.; Song, W.H.; et al. Physiological amyloid-beta clearance in the periphery and its therapeutic potential for Alzheimer’s disease. Acta Neuropathol. 2015, 130, 487–499. [Google Scholar] [CrossRef] [Green Version]
- Utevsky, A.V.; Smith, D.V.; Huettel, S.A. Precuneus is a functional core of the default-mode network. J. Neurosci. 2014, 34, 932–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castronovo, V.; Canessa, N.; Strambi, L.F.; Aloia, M.S.; Consonni, M.; Marelli, S.; Iadanza, A.; Bruschi, A.; Falini, A.; Cappa, S.F. Brain activation changes before and after PAP treatment in obstructive sleep apnea. Sleep 2009, 32, 1161–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatouleh, R.H.; Hammam, E.; Lundblad, L.C.; Macey, P.M.; McKenzie, D.K.; Henderson, L.A.; Macefield, V.G. Functional and structural changes in the brain associated with the increase in muscle sympathetic nerve activity in obstructive sleep apnoea. Neuroimage Clin. 2014, 6, 275–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baril, A.A.; Gagnon, K.; Brayet, P.; Montplaisir, J.; De Beaumont, L.; Carrier, J.; Lafond, C.; L’Heureux, F.; Gagnon, J.F.; Gosselin, N. Gray Matter Hypertrophy and Thickening with Obstructive Sleep Apnea in Middle-aged and Older Adults. Am. J. Respir. Crit. Care Med. 2017, 195, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- Cross, N.E.; Memarian, N.; Duffy, S.L.; Paquola, C.; LaMonica, H.; D’Rozario, A.; Lewis, S.J.G.; Hickie, I.B.; Grunstein, R.R.; Naismith, S.L. Structural brain correlates of obstructive sleep apnoea in older adults at risk for dementia. Eur. Respir. J. 2018, 52, 1800740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.C.; Huang, C.C.; Chen, H.L.; Chou, K.H.; Chen, P.C.; Tsai, N.W.; Chen, M.H.; Friedman, M.; Lin, H.C.; Lu, C.H. Longitudinal brain structural alterations and systemic inflammation in obstructive sleep apnea before and after surgical treatment. J. Transl. Med. 2016, 14, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Tang, S.; Lyu, X.; Yang, C.; Chen, X. Structural and functional brain alterations in obstructive sleep apnea: A multimodal meta-analysis. Sleep Med. 2019, 54, 195–204. [Google Scholar] [CrossRef]
- Benzinger, T.L.; Blazey, T.; Jack, C.R., Jr.; Koeppe, R.A.; Su, Y.; Xiong, C.; Raichle, M.E.; Snyder, A.Z.; Ances, B.M.; Bateman, R.J.; et al. Regional variability of imaging biomarkers in autosomal dominant Alzheimer’s disease. Proc. Natl. Acad. Sci. USA 2013, 110, E4502–E4509. [Google Scholar] [CrossRef] [Green Version]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartres-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; Ewers, M.; Franzmeier, N.; Kempermann, G.; Kremen, W.S.; et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement. 2020, 16, 1305–1311. [Google Scholar] [CrossRef]
- Andre, C.; Rehel, S.; Kuhn, E.; Landeau, B.; Moulinet, I.; Touron, E.; Ourry, V.; Le Du, G.; Mezenge, F.; Tomadesso, C.; et al. Association of Sleep-Disordered Breathing With Alzheimer Disease Biomarkers in Community-Dwelling Older Adults: A Secondary Analysis of a Randomized Clinical Trial. JAMA Neurol. 2020, 77, 716–724. [Google Scholar] [CrossRef]
- Bubu, O.M.; Andrade, A.G.; Umasabor-Bubu, O.Q.; Hogan, M.M.; Turner, A.D.; de Leon, M.J.; Ogedegbe, G.; Ayappa, I.; Jean-Louis, G.G.; Jackson, M.L.; et al. Obstructive sleep apnea, cognition and Alzheimer’s disease: A systematic review integrating three decades of multidisciplinary research. Sleep Med. Rev. 2020, 50, 101250. [Google Scholar] [CrossRef] [PubMed]
- Pegueroles, J.; Vilaplana, E.; Montal, V.; Sampedro, F.; Alcolea, D.; Carmona-Iragui, M.; Clarimon, J.; Blesa, R.; Lleo, A.; Fortea, J.; et al. Longitudinal brain structural changes in preclinical Alzheimer’s disease. Alzheimers Dement. 2017, 13, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.J.; Sattler, J.M.; Lopez, S.J. Age effects on Wechsler Adult Intelligence Scale-III subtests. Arch. Clin. Neuropsychol. 2000, 15, 311–317. [Google Scholar] [CrossRef]
- Elkana, O.; Soffer, S.; Eisikovits, O.R.; Oren, N.; Bezalel, V.; Ash, E.L. WAIS Information Subtest as an indicator of crystallized cognitive abilities and brain reserve among highly educated older adults: A three-year longitudinal study. Appl. Neuropsychol. Adult 2020, 27, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Rosenzweig, I.; Glasser, M.; Polsek, D.; Leschziner, G.D.; Williams, S.C.; Morrell, M.J. Sleep apnoea and the brain: A complex relationship. Lancet Respir. Med. 2015, 3, 404–414. [Google Scholar] [CrossRef] [Green Version]
- Mahley, R.W. Apolipoprotein E: From cardiovascular disease to neurodegenerative disorders. J. Mol. Med. 2016, 94, 739–746. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Demographics and Plasma Biomarker | OSA (n = 30) | Control (n = 34) | p Value |
|---|---|---|---|
| Age (year) | 41.93 ± 1.65 | 43.21 ± 2.25 | 0.65 |
| Sex (M, F) | 27:3 | 17 ± 17 | 0.001 * |
| BMI | 26.18 ± 0.52 | 24.83 ± 0.54 | 0.08 |
| T-tau (pg/mL) | 21.43 ± 0.55 | 18.27 ± 0.85 | 0.025 * |
| Aβ42 (pg/mL) | 16.17 ± 0.12 | 15.37 ± 0.26 | 0.041 * |
| Aβ40 (pg/mL) | 53.00 ± 0.90 | 54.61 ± 1.25 | 0.414 |
| Aβ42/Aβ40 | 0.30 ± 0.04 | 0.29 ± 0.08 | 0.219 |
| Polysomnography parameters and IMT of CCA # | |||
| AHI | 41.93 ± 4.33 | 2.68 ± 0.29 | <0.001 * |
| ODI | 32.75 ± 4.22 | 0.91 ± 0.21 | <0.001 * |
| O2 < 90% (% per night) | 8.47 ± 1.44 | 0.44 ± 0.28 | <0.001 * |
| Average O2 | 95.00 ± 0.27 | 97.06 ± 0.19 | <0.001 * |
| Snoring index | 374.00 ± 33.82 | 233.62 ± 56.32 | 0.052 |
| IMT | 0.65 ± 0.12 | 0.54 ± 0.07 | 0.003 * |
| Neuro-psychological assessments Attention Function | |||
| Digit span | 10.27 ± 2.57 | 11.53 ± 2.97 | 0.112 |
| Attention | 7.60 ± 0.72 | 7.74 ± 0.51 | 0.843 |
| Orientation | 17.93 ± 0.37 | 17.94 ± 0.24 | 0.332 |
| Executive Function | |||
| Digit symbol coding | 10.87 ± 2.30 | 11.32 ± 2.04 | 0.943 |
| Arithmetic | 10.77 ± 2.24 | 10.53 ± 2.31 | 0.590 |
| Abstract thinking | 9.93 ± 1.26 | 10.03 ± 1.66 | 0.879 |
| Memory Function | |||
| Short-term memory | 10.40 ± 1.34 | 10.33 ± 1.34 | 0.738 |
| Long-term memory | 9.87 ± 0.51 | 9.94 ± 0.34 | 0.510 |
| Information | 10.80 ± 3.02 | 11.21 ± 3.31 | 0.131 |
| Speech and Language | |||
| Comprehension | 10.83 ± 2.45 | 11.12 ± 2.63 | 0.435 |
| Language | 9.85 ± 0.35 | 9.85 ± 0.36 | 0.693 |
| Semantic fluency | 8.80 ± 1.71 | 8.59 ± 1.78 | 0.884 |
| Visuospatial Function | |||
| Picture completion | 11.50 ± 2.40 | 10.68 ± 2.67 | 0.504 |
| Block design | 11.37 ± 2.55 | 10.41 ± 3.00 | 0.555 |
| Drawing | 9.97 ± 0.18 | 9.94 ± 0.24 | 0.276 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-S.; Chen, M.-H.; Wang, P.-M.; Lu, C.-H.; Chen, H.-L.; Lin, W.-C. Increased Levels of Plasma Alzheimer’s Disease Biomarkers and Their Associations with Brain Structural Changes and Carotid Intima-Media Thickness in Cognitively Normal Obstructive Sleep Apnea Patients. Diagnostics 2022, 12, 1522. https://doi.org/10.3390/diagnostics12071522
Chen Y-S, Chen M-H, Wang P-M, Lu C-H, Chen H-L, Lin W-C. Increased Levels of Plasma Alzheimer’s Disease Biomarkers and Their Associations with Brain Structural Changes and Carotid Intima-Media Thickness in Cognitively Normal Obstructive Sleep Apnea Patients. Diagnostics. 2022; 12(7):1522. https://doi.org/10.3390/diagnostics12071522
Chicago/Turabian StyleChen, Yueh-Sheng, Meng-Hsiang Chen, Pei-Ming Wang, Cheng-Hsien Lu, Hsiu-Ling Chen, and Wei-Che Lin. 2022. "Increased Levels of Plasma Alzheimer’s Disease Biomarkers and Their Associations with Brain Structural Changes and Carotid Intima-Media Thickness in Cognitively Normal Obstructive Sleep Apnea Patients" Diagnostics 12, no. 7: 1522. https://doi.org/10.3390/diagnostics12071522
APA StyleChen, Y.-S., Chen, M.-H., Wang, P.-M., Lu, C.-H., Chen, H.-L., & Lin, W.-C. (2022). Increased Levels of Plasma Alzheimer’s Disease Biomarkers and Their Associations with Brain Structural Changes and Carotid Intima-Media Thickness in Cognitively Normal Obstructive Sleep Apnea Patients. Diagnostics, 12(7), 1522. https://doi.org/10.3390/diagnostics12071522