1. Introduction
Pressure injury (PI) is a refractory skin disease that seriously affects the health of patients and threatens lives [
1]. Therefore, its early diagnosis and treatment are very important. With the development of medical technology, early treatment has become possible in clinical work. In this aspect, the National Pressure Injury Advisory Panel (NPIAP) changed the terminology of “Pressure Ulcer” to “Pressure Injury” in 2016, to emphasize the existence of early PI before ulcer formation [
2]. Stage 1 is the earliest stage of PI (early PI), while non-blanchable erythema is the diagnosis indicator in the transparent disc method, and this condition is mainly caused by intradermal hemorrhage and can be distinguished from the BE caused by hyperemia [
3].
Although the transparent disc method is not an ideal detection method, and may even cause secondary damage due to excessive pressure, there is no better alternative method at present. In transparent disc method, fingers or transparent disk method are used to gently press the area of erythema. This method is widely utilized in clinical settings because of its convenience [
4]. However, the process of applying light pressure to the erythema is not clearly defined. This affects the results of inspections, as the pressure exerted by the estimator will vary from person to person, leading to the omission of some epidemiological statistics. In addition, the prevalence and incidence found in these statistical studies were lower than the actual prevalence of PI [
5]. In clinical settings, although a pressure of 150 mmHg was reported, this was just based on clinical experience and lacked sufficient evidence [
6]. For this reason, the appropriate pressure to use in the transparent disc method should be scientifically verified and determined. Furthermore, for either early PI or BE, a process of the development or disappearance of the wound area occurs. During this period, whether the changes in redness or erythema will affect the results of diagnosis via the transparent disc method is also an issue that should be explored.
In the present study, we verified the uncertainty of the degree of ‘light pressure’ through human observations. Moreover, animal models of BE and early PI were established. A pressure attachment device was made to simulate the pressure of the transparent disc method, and a spectrophotometer and Dermo-camera were used to measure and observe the fading of erythema under different pressures throughout the process and determine the appropriate pressure in order to improve the results of the transparent disc method.
3. Results
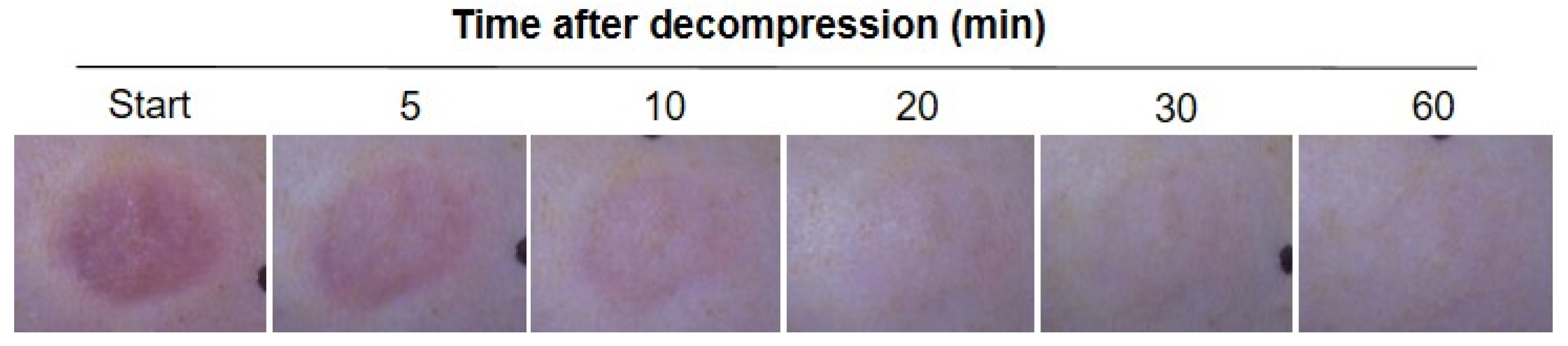
To establish the appropriate pressure to use in the transparent disc method for BE animal models, we first made continuous observations of skin BE color changes based on serial digital pictures, as shown in
Figure 1. After decompression, erythema was clearly observed at the starting point and remained visible until 5 min. With the passing of time, the erythema gradually faded over 10 min after decompression. As shown in
Figure 1, the erythema completely disappeared at 1 h.
3.1. Establish the Appropriate Pressure for the Transparent Disc Method
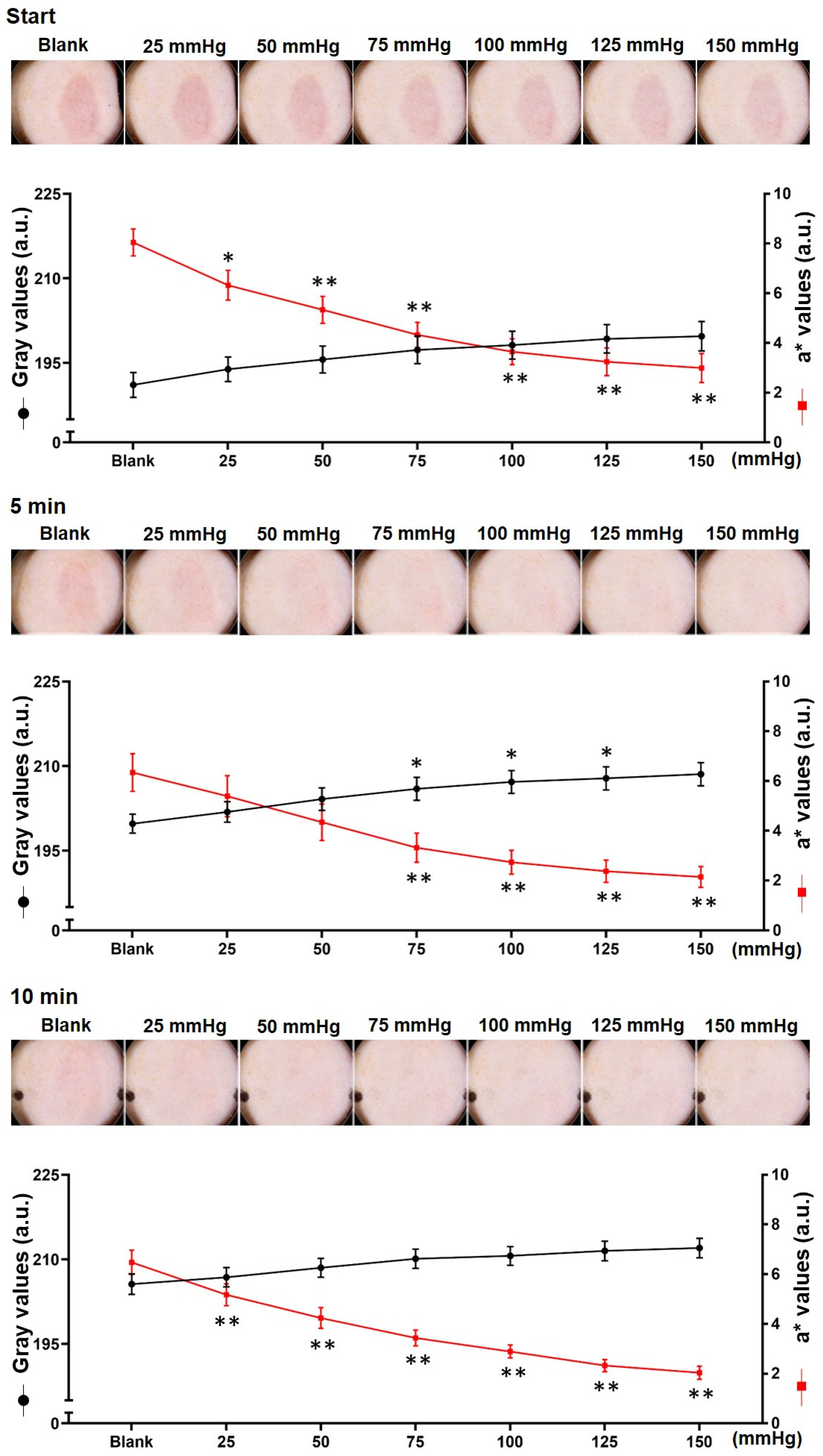
After decompression, we took pictures of BE using the Dermo-camera at the start and after, 5 and 10 min (
Figure 2, top panel). After decompression, the residual erythema was still obvious despite the applied pressure of 150 mmHg, and the surrounding skin showed obvious signs of fading. The erythema faded significantly when a pressure of 50 mmHg was applied at 5 and 10 min after decompression, and the erythema disappeared under the applied pressure of 100 mmHg.
The gray and a* values of the macroscopic images of erythema were measured (
Figure 2, bottom panel).
The gray value of erythema tended to increase three times: from 191.1 ± 5.8 to 199.7 ± 6.9 at the start, from 199.8 ± 4.4 to 208.6 ± 5.4 at 5 min, and a final significant increase at 100 mmHg (p < 0.01 vs. blank). At 10 min after decompression, it increased from 205.6 ± 4.8 to 212 ± 4.6.
The a* value of BE decreased from 8 ± 1.4 to 3 ± 1.5 at the start, from 6.3 ± 2.0 to 2.1 ± 1.1 at 5 min, and from 6.5 ± 1.3 to 2.0 ± 0.7 at 10 min. When the pressure was 50 mmHg, the three time periods were remarkably reduced (p < 0.01 vs. blank).
As shown in
Figure 2, bottom, the erythema of BE disappeared rapidly after decompression, while the gray value increased from 191.1 ± 5.8 at the start after decompression to 199.8 ± 4.4 at 5 min (
p < 0.05 vs. start), and increased even more from 10 min to approximately 205.6 ± 4.8 (
p < 0.01 vs. start).
3.2. Analysis of Pressure for Early PI as Determined Using Transparent Disc Method
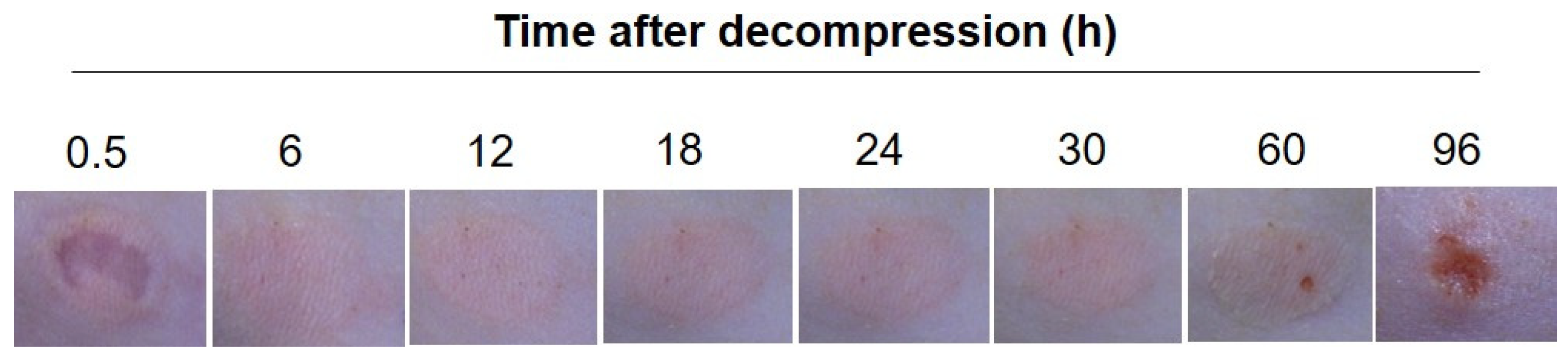
The erythema of PI was visible until 24 h after decompression. A slight increase or decrease was observed during the period. At 30 h after decompression, the erythema began to show punctate erosion and an ulcer formed by 96 h (
Figure 3).
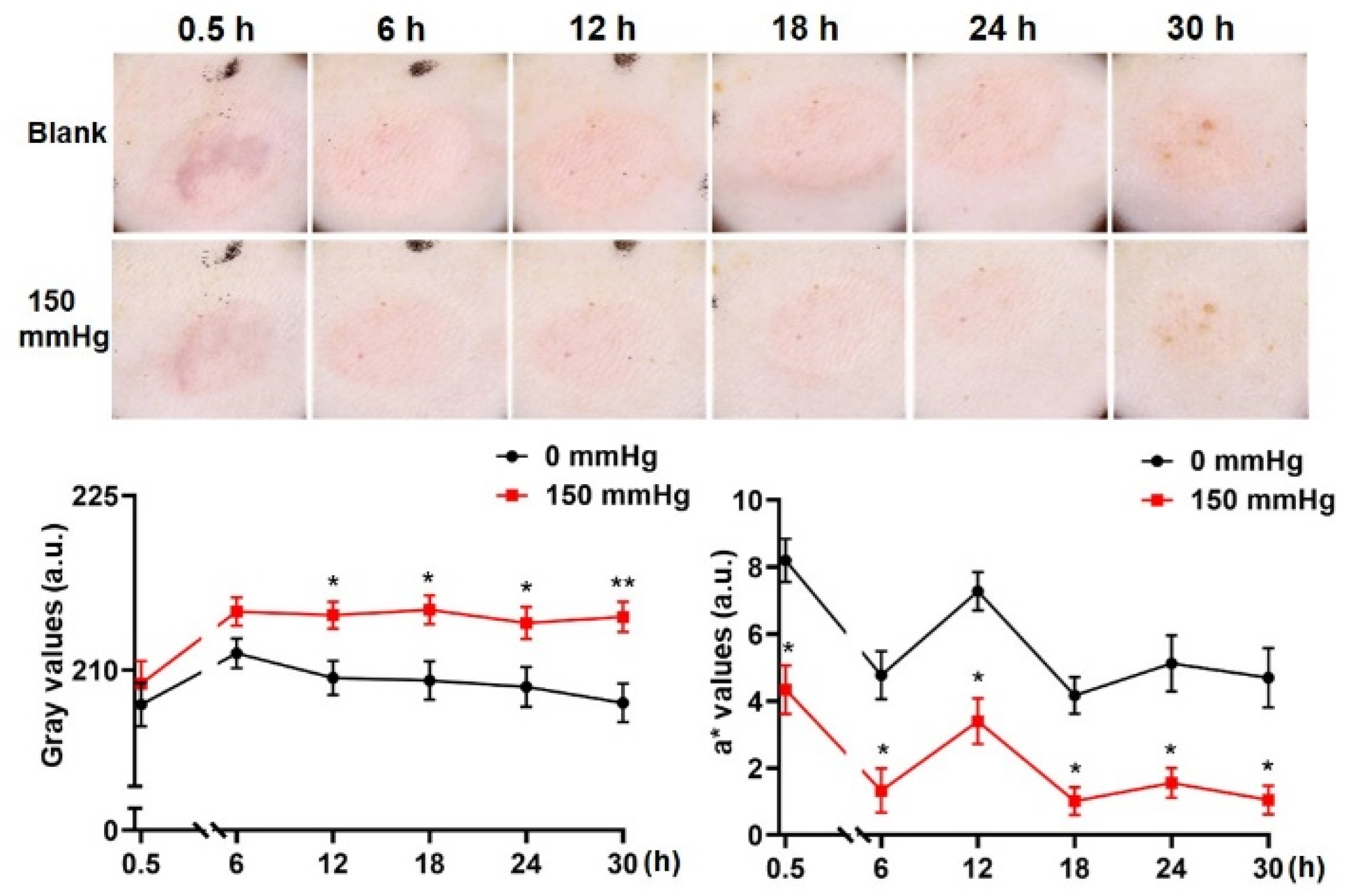
When pressure was applied, non-blanchable erythema was observed at 0.5, 6, 12, 24 and 30 h after decompression, although all instances were alleviated. However, the erythema faded significantly 18 h after decompression (
Figure 4).
When the pressure was applied, the gray value of erythema was respectively decompressed from 207 ± 4.9 (0.5 h) to, 211.4 ± 3.4 (6 h), 209.3 ± 3.9 (12 h), 209.1 ± 4.4 (18 h), 208.6 ± 4.5 (24 h) and 207.2 ± 4.4 (30 h) and increased to 208.8 ± 5.1 (0.5 h), 215 ± 3.2 (6 h), 214.7 ± 3.0 (12 h, p < 0.05 vs. blank), 215.2 ± 3.3 (18 h, p < 0.05 vs. blank), 214.1 ± 3.6 (24 h, p < 0.05 vs. blank) and 214.6 ± 3.4 (30 h, p < 0.01 vs. blank).
The a* value ranged from 8.2 ± 1.7 (0.5 h) to, 4.8 ± 1.9 (6 h), 7.3 ± 1.5 (12 h,
p < 0.05 vs. 0 mmHg), 4.2 ± 1.5 (18 h), 5.1 ± 2.2 (24 h) and 4.7 ± 2.3 (30 h), then reduced to 4.3 ± 1.9 (0.5 h,
p < 0.05 vs. blank), 1.3 ± 1.8 (6 h,
p < 0.05 vs. blank), 3.4 ± 1.8 (12 h,
p < 0.05 vs. blank), 1.0 ± 1.1 (18 h,
p < 0.05 vs. blank), 1.6 ± 1.2 (24 h,
p < 0.05 vs. blank) and 1.1 ± 1.1 (30 h,
p < 0.05 vs. blank) (
Figure 4, bottom).
3.3. Observation of the Variations of Erythema When the Transparent Disc Was Pressed
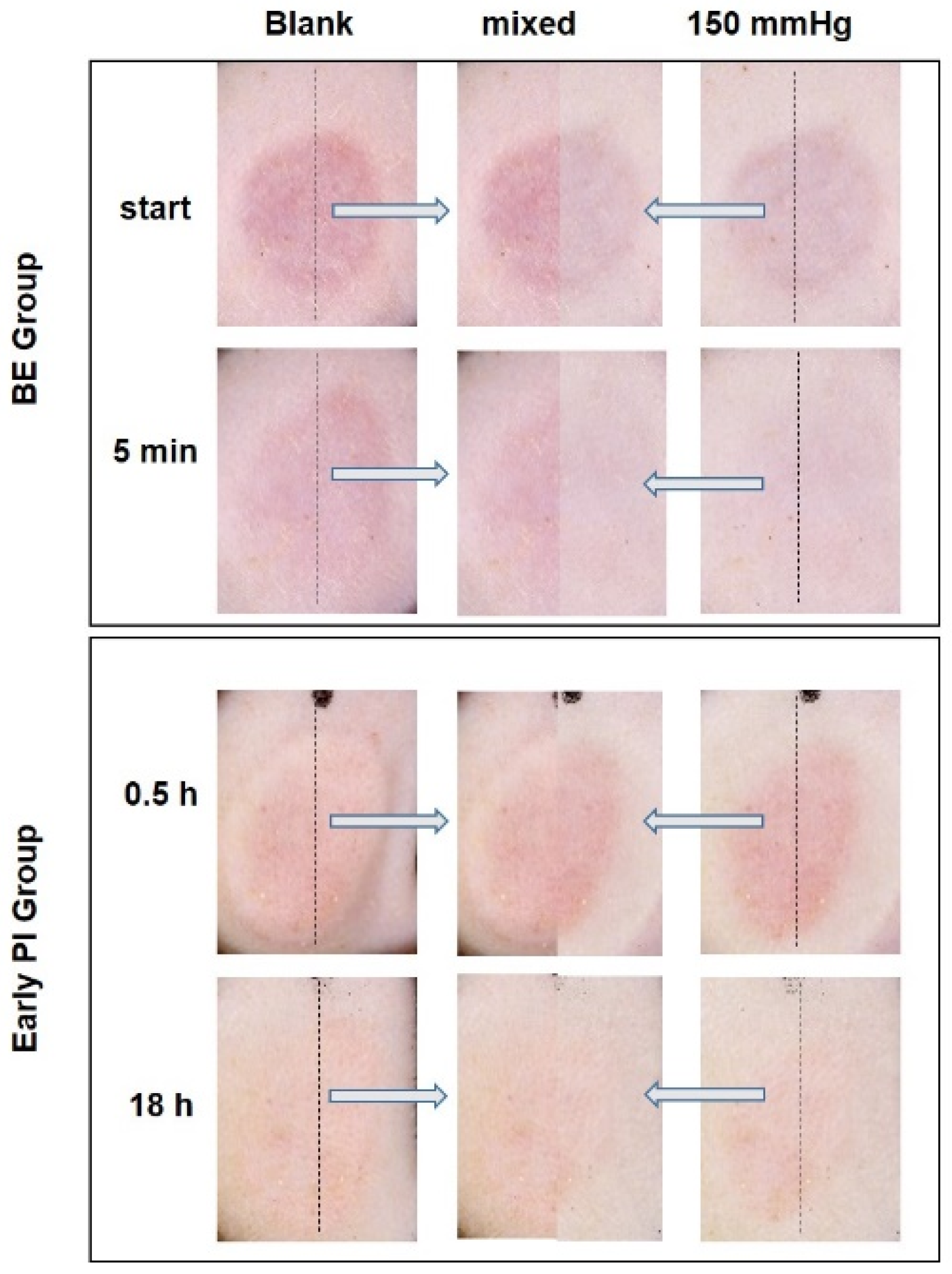
After decompression, BE remained when the transparent disc was applied, and it was visually non-blanchable (
Figure 5, top), although the a* value indicated that the degree of reduction in the level of blanching was obvious (
Figure 2, bottom). By contrast, the erythema of the early PI was lightest at 18 h after decompression (
Figure 4) decreased significantly when the transparent disc was applied, and was visually blanchable (
Figure 5).
4. Discussion
The transparent disc method is an indicator of early PI diagnosis and is widely used in clinical settings [
1]. However, in the present clinical diagnosis, no uniform standard is used for the pressure applied in the transparent disc method, and it varies from person to person. This condition significantly affects the results and consistency of clinical diagnosis [
4]. In our preliminary study, we also found that the pressure applied in the transparent disc method varied from person to person according to their gender and body position (
Supplemental Figure S1).
To explore the appropriate pressure to use in the transparent disc method, we performed tests by using BE models. The results obtained before and after pressure was applied showed that when the pressure was set at 50 mmHg, the erythema visibly faded in each period after decompression. Quantitative analysis showed that the gray values were statistically significant when the pressure was 100 mmHg. Close to the maximal values of fading were obtained when the pressure was 150 mmHg. Therefore, the pressure applied in the transparent disc method should be set at 50 mmHg (macroscopic observation and a* value) or 100 mmHg (gray value). The measurements of the gray value at the erythema and a* value of the spectrophotometer can demonstrate the degree of fading, and the a* value is more sensitive. It seems that the pressure observed to be used in the transparent disc method immediately after BE decompression was inappropriate, because the residual erythema was worse. There was obvious fading of BE within a short period of time. This finding can be applied for use in clinical observations.
Furthermore, we also constructed an early PI model. When applying a pressure of 150 mmHg to the skin, the erythema at each time period showed an obvious residual effect, which meets the definition of it being non-blanchable. This phenomenon was similar to that observed at 18 h after decompression, and the erythema was obviously weakened when pressed, similar to BE.
The transparent disc method was first used by dermatologists to distinguish skin hyperemia and hemorrhage [
9], and later used for the early diagnosis of PI [
10]. The observation methods used include the finger and transparent disk method. These can be performed by lightly pressing on the erythema area with either a finger or a transparent disc. If the erythema does not fade, the non-blanchable erythema seen in early PI is considered [
11,
12]. A previous study that compared the two methods found no obvious difference between the two transparent disc methods [
4].
A diagnosis of early PI is made using the transparent disc method, which is widely used because of its simplicity. Nevertheless, the degree of light pressure that should be used has not yet been determined, which certainly affects the accuracy of this method. Therefore, whether early PI is included in the overall incidence rate has become an important issue that needs to be addressed [
1]. Considering the omission of some epidemiological statistics, the prevalence and incidence rates are lower than the actual prevalence of PI. Kaltenthaler [
5] calculated and compared the prevalence and incidence of PI in the UK, the USA and Canada, finding that many studies exclude early PI from their calculation, leading to significant differences in PI epidemiological statistics. The prevalence rates of PI were reported to be as low as 3% in Italy and Germany, while the rates observed in the UK and the Netherlands as high as 20%. A possible reason for this discrepancy may have been the inclusion of early PI in the statistics rather than the quality of nursing care [
13]. This study revealed a high prevalence of pressure damage (18.6%) in contrast to the published DoH figure of 6.7% [
14]. In this study, the authors ignored stage 1 damage, resulting in a prevalence of 10.1%. Considering the variations in the methodologies and the lack of consensus on a definition of pressure damage and the population surveyed, the standardization of the transparent disc method needs to be conducted urgently to determine the degree of light pressure to be applied.
Our study simulated the transparent disk method; the results obtained were in accordance with the definition of light pressure. However, macroscopic observations have some limitations. For example, the estimators cannot be used for comparison before and after and are also unreliable and hard to quantify [
15]. Furthermore, we used a Dermo-camera to measure the gray values of the images and a spectrophotometer to measure the a* values. Based on previous clinical experience, the evaluator set the pressure to 150 mmHg for the transparent disc method [
6]. In our animal experiments, the gray value and a* values showed that the pressure was in the range of 50–100 mmHg. In order to reduce secondary damage caused by inspections, pressures below 100 mmHg are more appropriate than 150 mmHg.
In human observations, the definition of light pressure has remarkable discrepancies from person to person. While the pressure applied varied from person to person, the pressure applied to most volunteers was below 20 mmHg, and our research results showed that it should be above 50 mmHg for the transparent disc method to be effective. We know that the blood hydrostatic pressure of peripheral circulation in the physiological state is 35 mmHg, and external pressure exceeding this will completely block the blood supply. However, the pathological state of early PI is different. In our preliminary experiment, the results showed that the a* value of the erythema was close to the lowest under a pressure of 150 mmHg, indicating that the transparent disc method has the best effect when observing PI erythema at a pressure close to 150 mmHg. At the same time, the vulnerability of early PI in the pathological state should be considered, and the pressure used in the transparent disc method should be reduced as much as possible. It is not known whether the rapid application of a pressure of 50–100 mmHg in a short time by the transparent disc method will also cause damage. A previous in vitro study showed that tissue exposed to 50 mmHg of pressure for 4 h still maintained a fiber bundle structure and capillaries of varying caliber. However, after being exposed to a pressure of 170 mmHg for 4 h, the tissue structure became significantly different [
16]. This results demonstrated that the application of 50–100 mmHg of pressure may cause little to no harm.
The results obtained from the volunteers further indicated that the specific pressure used should be specified in order to prevent false negatives caused by the application of insufficient pressure, thereby affecting the diagnosis of early PI.
Nevertheless, the transparent disc method is limited to use in qualitative examinations and cannot meet clinical needs. It should be developed into a quantitative examination in order to evaluate cases of early PI more accurately in the future. The Dermo-camera can be used as an objective instrument in clinical examinations. We found that its use in combination with the transparent disc method is able to determine the pressure applied less effectively than the use of the spectrophotometer alone. Therefore, the Dermo-camera should be used to observe and record the fading of erythema under a specified level of pressure, further enhancing the accuracy of the pressure transparent disc method. Nevertheless, the Dermo-camera is an expensive device. Therefore, cheap devices need to be developed for use in the future.
In addition, some exceptions can be noted in our clinical observations. The erythema in early PI can be neither non-blanchable or blanchable, depending upon the severity of the disease [
17], due to the overlapping histological changes seen in normal, blanchable and non-blanchable states [
18]. This study also showed that the erythema seen in early PI was visually blanchable during the deterioration process. This phenomenon may be caused by a reduction in hyperemia and congestion. Similarly, BE shows visual non-blanchable changes, combined with an obvious reduction in and disappearance of erythema within a short period of time, which is consistent with the clinical manifestations of congestion and the results of our previous research [
7], indicating that congestion may also occur in BE. Therefore, in addition to the routine use of the transparent disc method in clinical settings, if time permits, we also recommend observing the erythema at 5 min or 10 min after the first observation to compare the level of fading before and after the procedure. Our research showed that obvious fading should be placed in the category of congestion erythema. This setting requires the use of a corresponding recording device, it is difficult to achieve consistency solely by the evaluator’s memory.
However, in this experiment we mainly utilized animal models to simulate PI and carry out the transparent disc method. Our results may not reflect the PI situation in humans. Furthermore, we did not perform a pathologic analysis, this should be performed in further studies. We also need to set up a more rigid rule to distinguish the various degrees of symptoms in our further study.
Lastly, the Casio camera used in this study are devices designed for dermatologists for clinical observations. The price is high for clinical applications in places where PI is common, such as hospitals, nursing care facilities for the elderly, and home care. Therefore, a more convenient and cheaper device should be developed.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}