
Automated Detection, Segmentation, and Classification of Pericardial Effusions on Chest CT Using a Deep Convolutional Neural Network

 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Materials and Methods
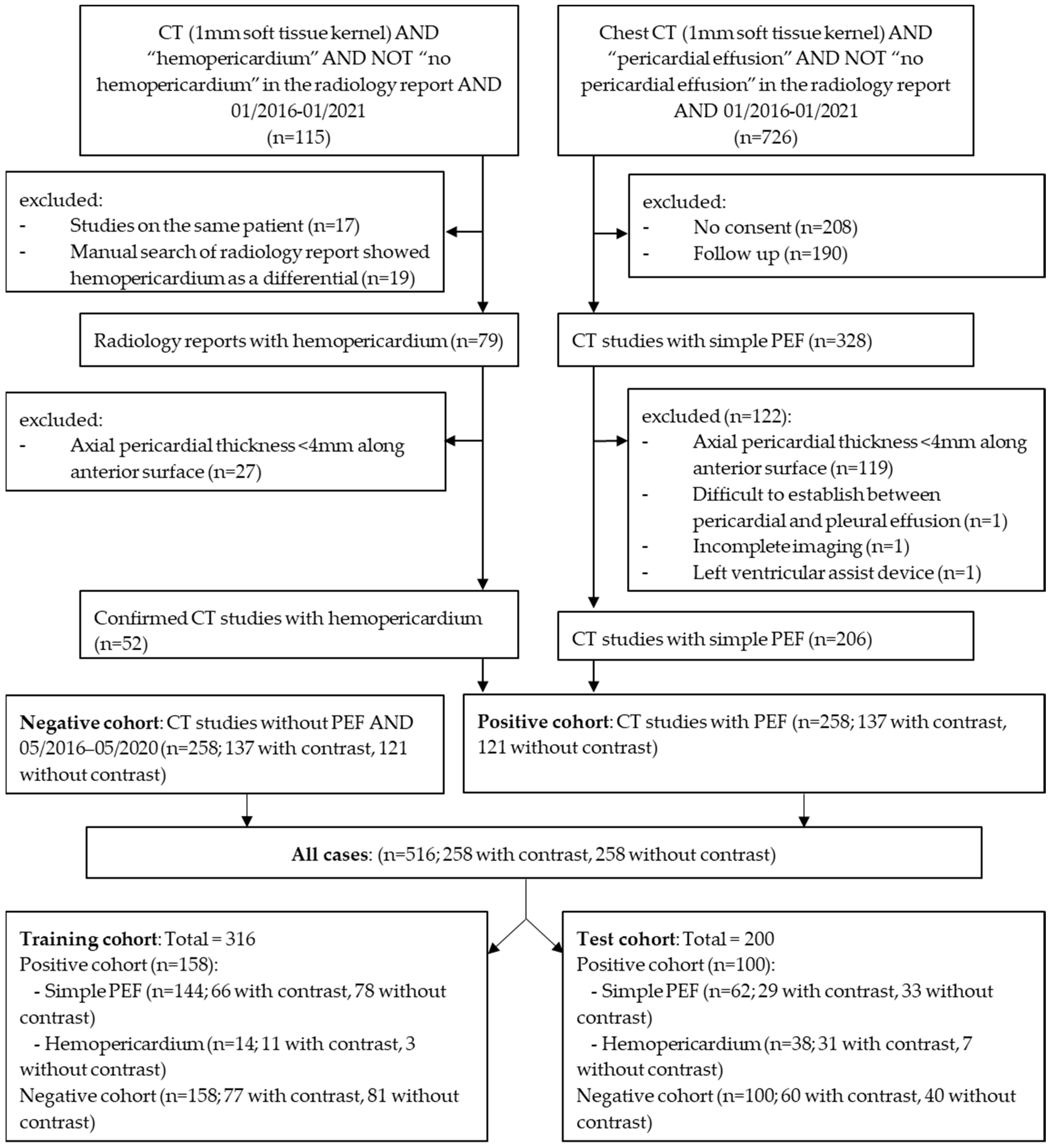
2.1. Study Population
2.2. Image Acquisition Parameters
2.3. Segmentation
2.4. Model Training, Validation, and Testing
2.5. Hardware and Software
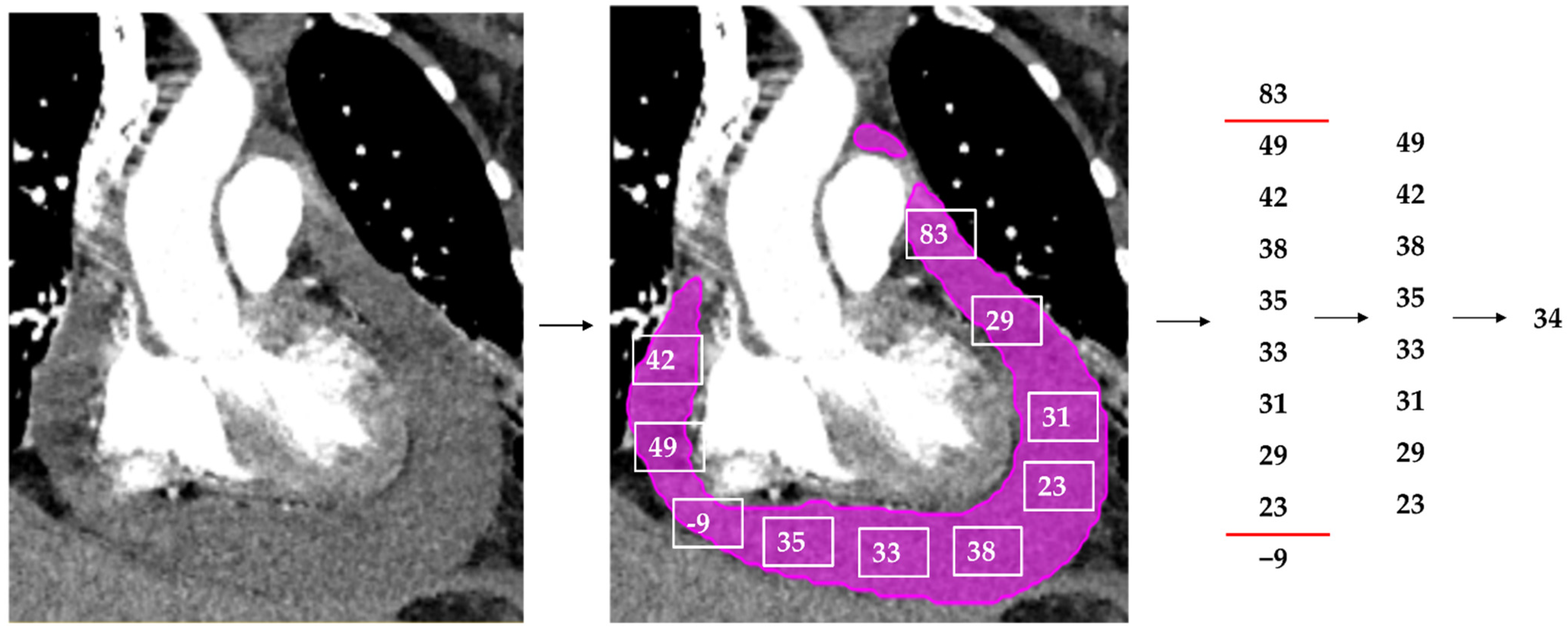
2.6. Classification of Hemopericardium
2.7. The Model’s Output
2.8. External Data Set
2.9. Statistical Analyses
2.10. Publicly Available Data
3. Results
3.1. Study Population
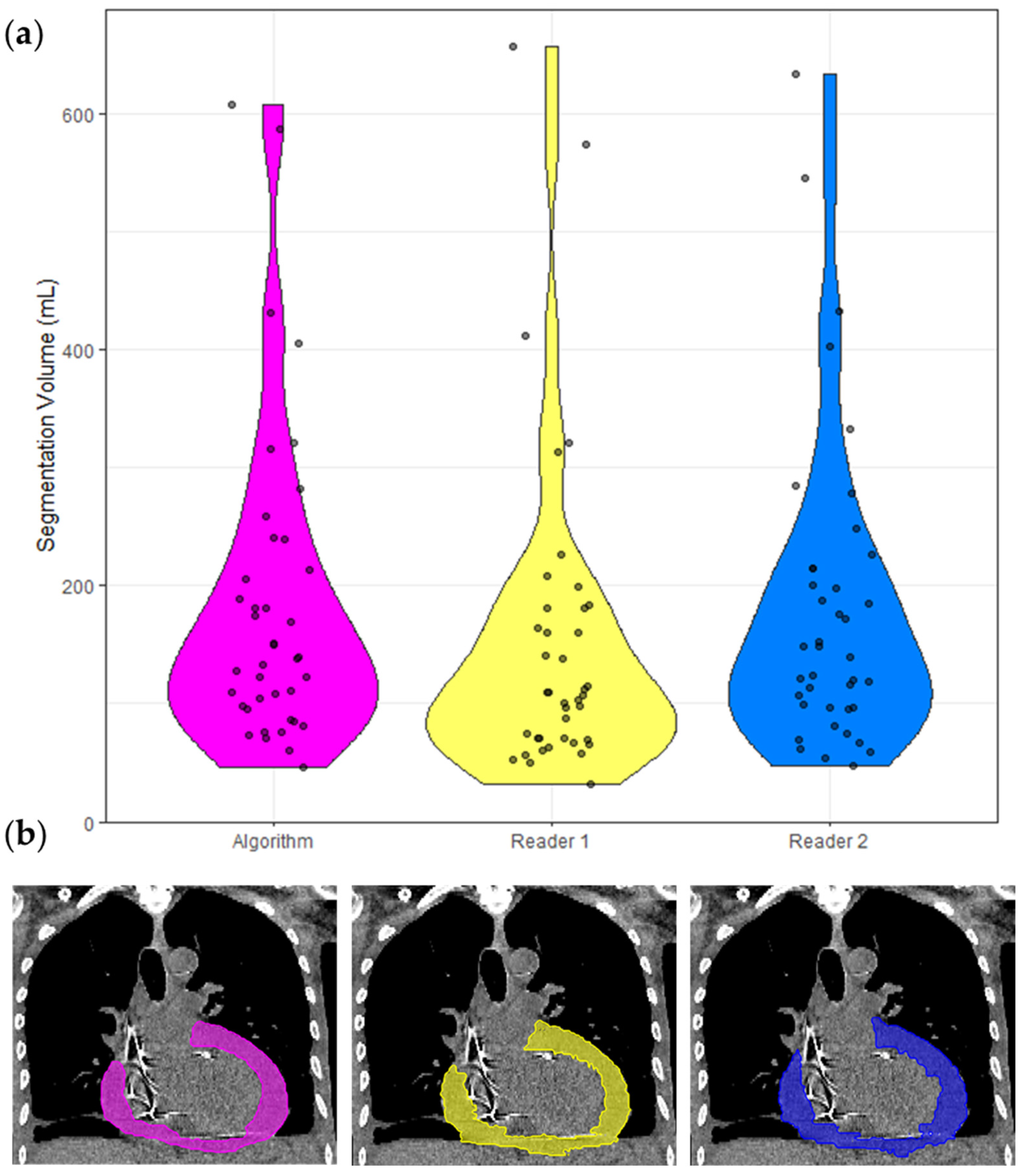
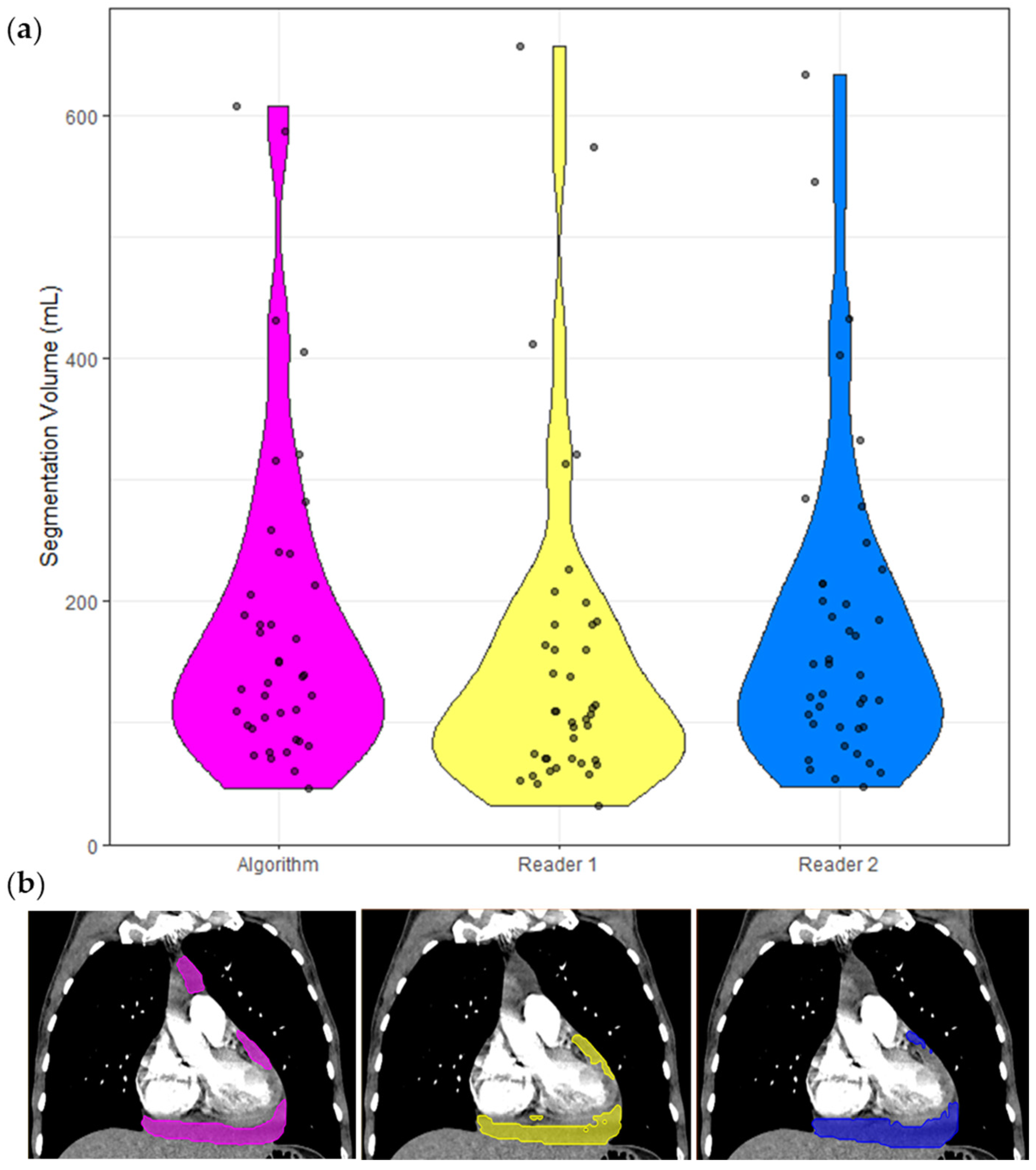
3.2. Inter-Reader Versus Reference-Prediction
3.3. Model Performance and Effect of Confounding Factors
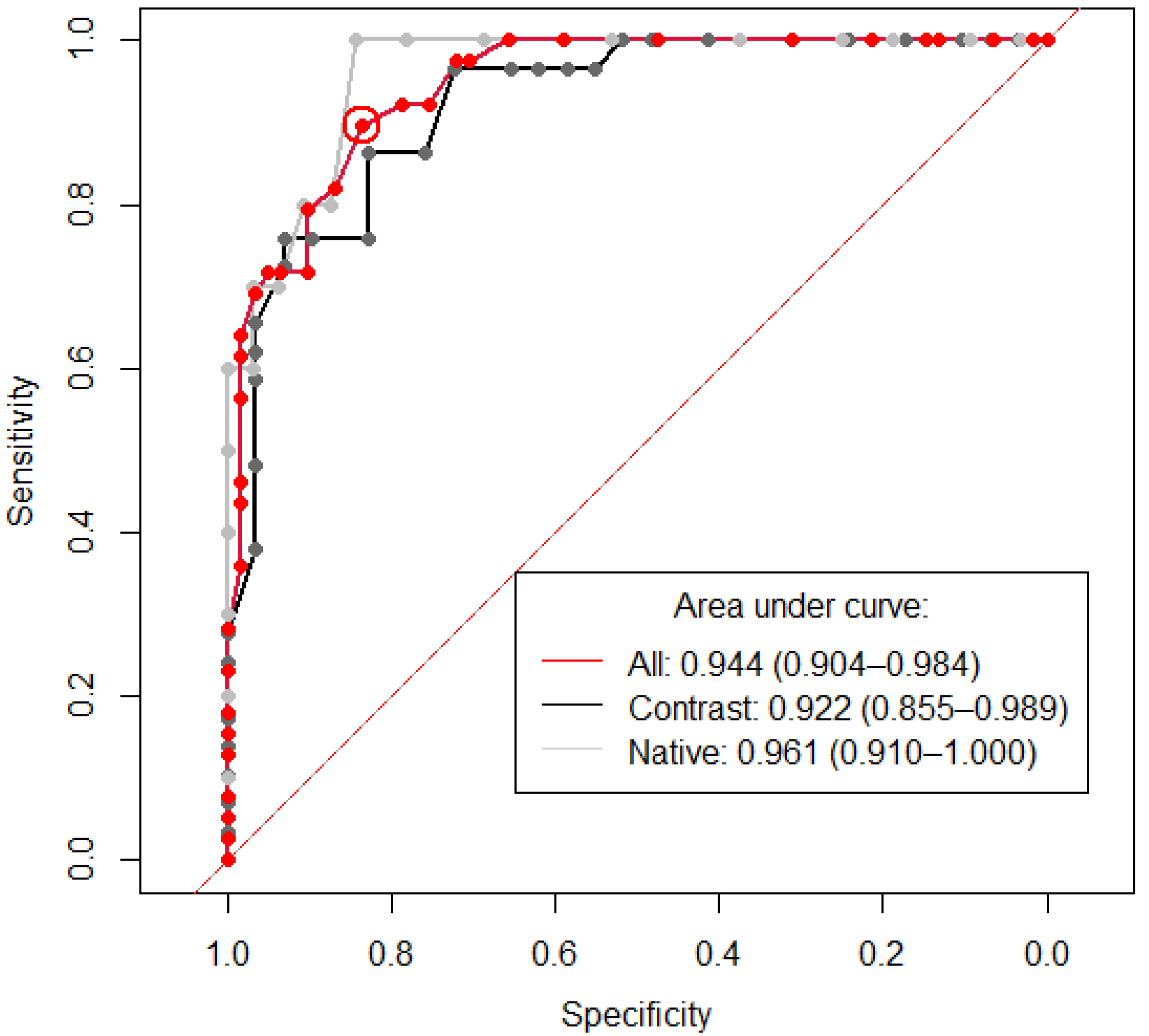
3.4. Detection of Pericardial Effusion
3.5. Hemopericardium Classification
3.6. External Validation
4. Discussion
Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Statistical Analysis of Volume Difference (Reference Minus Model) | Statistical Analysis of Detection Rate Comparison | Statistical Analysis of Dice Coefficient Comparison |
|---|---|---|---|
| Contrast administration (n = 57/60) compared to non-contrast (n = 43) | p = 0.109 | p = 0.506 | p = 0.908 |
| Reference volume of <50mL (n = 11) compared to >50mL (n = 89) | p = 0.474 | p = 0.140 | p = 0.086 |
| Presence of hemopericardium (n = 39) compared to PEF (n = 61) | p = 0.032 | p = 0.015 | p = 0.097 |
| Presence of pleural effusion (n = 62) compared to no pleural effusion (n = 37) | p = 0.123 | p = 0.218 | p = 0.116 |
| Disease (combined post op, visible tumor, trauma, visible infection) (n = 62) compared to no visible disease (n = 38) | p = 0.445 | p = 0.297 | p = 0.061 |
| Post operative (n = 26) versus non post operative images (n = 74) | p = 0.618 | p = 0.460 | p = 0.115 |
| Visible tumor (n = 12) compared to no tumor in image (n = 88) | p = 0.291 | p = 0.361 | p = 0.979 |
| Visible tumor located in mediastinum (n = 7) compared to no tumor (n = 88) | p = 0.116 | p = 0.646 | p = 0.706 |
| Visible tumor located in chest (n = 5) compared to no tumor (n = 88) | p = 0.858 | p = 0.364 | p = 0.615 |
| Trauma (n = 6) compared to no trauma (n = 94) | p = 0.313 | p = 0.530 | p = 0.971 |
| Visible presence of infection (n = 27) compared to no visible infection (n = 73) | p = 0.727 | p = 0.399 | p = 0.951 |
References
- Smith-Bindman, R.; Kwan, M.L.; Marlow, E.; Theis, M.K.; Bolch, W.; Cheng, S.Y.; Bowles, E.J.A.; Duncan, J.R.; Greenlee, R.T.; Kushi, L.H.; et al. Trends in Use of Medical Imaging in US Health Care Systems and in Ontario, Canada, 2000–2016. JAMA 2019, 322, 843–856. [Google Scholar] [CrossRef]
- Munden, R.F.; Carter, B.W.; Chiles, C.; MacMahon, H.; Black, W.C.; Ko, J.P.; McAdams, H.P.; Rossi, S.E.; Leung, A.N.; Boiselle, P.M.; et al. Managing Incidental Findings on Thoracic CT: Mediastinal and Cardiovascular Findings. A White Paper of the ACR Incidental Findings Committee. J. Am. Coll. Radiol. 2018, 15, 1087–1096. [Google Scholar] [CrossRef]
- Klein, A.L.; Abbara, S.; Agler, D.A.; Appleton, C.P.; Asher, C.R.; Hoit, B.; Hung, J.; Garcia, M.J.; Kronzon, I.; Oh, J.K.; et al. American Society of Echocardiography Clinical Recommendations for Multimodality Cardiovascular Imaging of Patients with Pericardial Disease. J. Am. Soc. Echocardiogr. 2013, 26, 965–1012.e15. [Google Scholar] [CrossRef]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Barón-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C.; et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2015, 36, 2921–2964. [Google Scholar] [CrossRef]
- Choy, G.; Kröpil, P.; Scherer, A.; El-Sherief, A.H.; Chung, J.; Rojas, C.A.; Abbara, S. Pertinent reportable incidental cardiac findings on chest CT without electrocardiography gating: Review of 268 consecutive cases. Acta Radiol. 2013, 54, 396–400. [Google Scholar] [CrossRef]
- Vakamudi, S.; Ho, N.; Cremer, P.C. Pericardial Effusions: Causes, Diagnosis, and Management. Prog. Cardiovasc. Dis. 2017, 59, 380–388. [Google Scholar] [CrossRef]
- Alter, P.; Figiel, J.; Rupp, T.P.; Bachmann, G.F.; Maisch, B.; Rominger, M.B. MR, CT, and PET imaging in pericardial disease. Heart Fail. Rev. 2012, 18, 289–306. [Google Scholar] [CrossRef]
- Ebert, L.; Dobay, A.; Franckenberg, S.; Thali, M.; Decker, S.; Ford, J. Image segmentation of post-mortem computed tomography data in forensic imaging: Methods and applications. Forensic Imaging 2021, 28, 200483. [Google Scholar] [CrossRef]
- Cossu, A.; Rother, M.D.M.; Kusmirek, J.E.; Meyer, C.A.; Kanne, J.P. Imaging Early Postoperative Complications of Cardiothoracic Surgery. Radiol. Clin. N. Am. 2020, 58, 133–150. [Google Scholar] [CrossRef]
- Azarbal, A.; LeWinter, M.M. Pericardial Effusion. Cardiol. Clin. 2017, 35, 515–524. [Google Scholar] [CrossRef]
- Yao, J.; Bliton, J.; Summers, R.M. Automatic Segmentation and Measurement of Pleural Effusions on CT. IEEE Trans. Biomed. Eng. 2013, 60, 1834–1840. [Google Scholar] [CrossRef] [Green Version]
- Weikert, T.; D’Antonoli, T.A.; Bremerich, J.; Stieltjes, B.; Sommer, G.; Sauter, A.W. Evaluation of an AI-Powered Lung Nodule Algorithm for Detection and 3D Segmentation of Primary Lung Tumors. Contrast Media Mol. Imaging 2019, 2019, 1545747. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Using artificial intelligence to detect COVID-19 and community-acquired pneumonia based on pulmonary CT: Evaluation of the diagnostic accuracy. Radiology 2020, 296, E65–E71. [Google Scholar] [CrossRef]
- van Velzen, S.G.M.; Lessmann, N.; Velthuis, B.K.; Bank, I.E.M.; Bongard, D.V.D.; Leiner, T.; de Jong, P.A.; Veldhuis, W.B.; Correa, A.; Terry, J.G.; et al. Deep Learning for Automatic Calcium Scoring in CT: Validation Using Multiple Cardiac CT and Chest CT Protocols. Radiology 2020, 295, 66–79. [Google Scholar] [CrossRef]
- Ebert, L.C.; Heimer, J.; Schweitzer, W.; Sieberth, T.; Leipner, A.; Thali, M.; Ampanozi, G. Automatic detection of hemorrhagic pericardial effusion on PMCT using deep learning–A feasibility study. Forensic Sci. Med. Pathol. 2017, 13, 426–431. [Google Scholar] [CrossRef]
- Liu, J.; Cai, J.; Chellamuthu, K.; Bagheri, M.; Lu, L.; Summer, R.M. Summers, Cascaded coarse-to-fine convolutional neural networks for pericardial effusion localization and segmentation on CT scans. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 1092–1095. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional networks for biomedical image segmentation. In Medical Image Computing and Computer-Assisted Intervention 2015; Navab, N., Hornegger, J., Wells, W.M., Frangi, A.F., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar] [CrossRef] [Green Version]
- Isensee, F.; Jaeger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation. Nat. Methods 2020, 18, 203–211. [Google Scholar] [CrossRef]
- Rivera, S.C.; Liu, X.; Chan, A.-W.; Denniston, A.K.; Calvert, M.J.; Darzi, A.; Holmes, C.; Yau, C.; Moher, D.; Ashrafian, H.; et al. Guidelines for clinical trial protocols for interventions involving artificial intelligence: The SPIRIT-AI extension. Nat. Med. 2020, 26, 1351–1363. [Google Scholar] [CrossRef]
- Mongan, J.; Moy, L.; Kahn, C.E. Checklist for Artificial Intelligence in Medical Imaging (CLAIM): A Guide for Authors and Reviewers. Radiol. Artif. Intell. 2020, 2, e200029. [Google Scholar] [CrossRef] [Green Version]
- Hofmanninger, J.; Prayer, F.; Pan, J.; Röhrich, S.; Prosch, H.; Langs, G. Automatic lung segmentation in routine imaging is primarily a data diversity problem, not a methodology problem. Eur. Radiol. Exp. 2020, 4, 50. [Google Scholar] [CrossRef]
- Flach, P.M.; Gascho, D.; Schweitzer, W.; Ruder, T.D.; Berger, N.; Ross, S.G.; Thali, M.J.; Ampanozi, G. Imaging in forensic radiology: An illustrated guide for postmortem computed tomography technique and protocols. Forensic Sci. Med. Pathol. 2014, 10, 583–606. [Google Scholar] [CrossRef] [Green Version]
- Ebert, L.C.; Ampanozi, G.; Ruder, T.; Hatch, G.; Thali, M.J.; Germerott, T. CT based volume measurement and estimation in cases of pericardial effusion. J. Forensic Leg. Med. 2012, 19, 126–131. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development for R; RStudio Team: Boston, MA, USA, 2020; Available online: https://rstudio.com/ (accessed on 26 October 2021).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; Available online: https://ggplot2.tidyverse.org (accessed on 5 January 2022).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Wilder-Smith, A.J.; Yang, S. Automated Detection, Segmentation and Classification of Pericardial Effusions on Chest CT Using a Deep Convolutional Neural Network. 2022. Available online: https://zenodo.org/record/6384747#.YmC8RdNByUk (accessed on 1 April 2022).
- Çetin, M.S.; Çetin, E.H.Ö.; Özdemir, M.; Topaloğlu, S.; Aras, D.; Temizhan, A.; Aydoğdu, S. Effectiveness of computed tomography attenuation values in characterization of pericardial effusion. Anatol. J. Cardiol. 2017, 17, 322–327. [Google Scholar] [CrossRef]
- Wahid, M.F.; Hossain, A.A. Classification of Diabetic Retinopathy from OCT Images using Deep Convolutional Neural Network with BiLSTM and SVM. In Proceedings of the 2021 12th International Conference on Computing Communication and Networking Technologies (ICCCNT), Kharagpur, India, 6–8 July 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Hassan, M.M.; Gumaei, A.; Aloi, G.; Fortino, G.; Zhou, M. A Smartphone-Enabled Fall Detection Framework for Elderly People in Connected Home Healthcare. IEEE Netw. 2019, 33, 58–63. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, J.; Lan, F. Dynamic hand gesture recognition based on short-term sampling neural networks. IEEE/CAA J. Autom. Sin. 2020, 8, 110–120. [Google Scholar] [CrossRef]
- Ay, Y.; Ay, N.K. Diagnostic value of transthoracic echocardiography and computerized tomography for surgically confirmed late tamponade after cardiac surgery. J. Card. Surg. 2019, 34, 1486–1491. [Google Scholar] [CrossRef]
- Gruettner, J.; Fink, C.; Walter, T.; Meyer, M.; Apfaltrer, P.; Schoepf, U.J.; Saur, J.; Sueselbeck, T.; Traunwieser, D.; Takx, R.; et al. Coronary computed tomography and triple rule out CT in patients with acute chest pain and an intermediate cardiac risk profile. Part 1: Impact on patient management. Eur. J. Radiol. 2013, 82, 100–105. [Google Scholar] [CrossRef]
- Ma, W.; Liu, J.; Zeng, Y.; Chen, S.; Ye, S.; Lan, L.; Liu, Q.; Weig, H.-J. Causes of moderate to large pericardial effusion requiring pericardiocentesis in 140 Han Chinese patients. Herz 2011, 37, 183–187. [Google Scholar] [CrossRef]

| Design | Parameters |
|---|---|
| Image preprocessing | Image downsampling to 1 × 1 × 1 mm3 |
| Hard-/Software | Matlab R2018b and Python 3.7 on a workstation with a consumer-grade graphic processor unit (Nvidia RTX 2080Ti). |
| Optimizer | SGD with Nesterov momentum (µ = 0.99) |
| Learning rate | Poly-learning rate schedule (initial 0.01) |
| Data augmentation | Gaussian noise and blur, brightness, contrast, simulation of low resolution, gamma correction and mirroring |
| Loss function | Dice and cross-entropy |
| Training procedure | 1000 epochs × 250 minibatches, foreground oversampling |
| Inference procedure | Sliding window with half-patch size overlap. Gaussian patch center weighting |
| Architecture template | Encoder-decoder with skip connection, instance normalization, leaky ReLU, deep supervision |
| Intensity normalization | Global dataset percentile clipping, z-score with global foreground mean and s.d. |
| Image resampling strategy | In-plane with third-order spline, out- of-plan with nearest neighbor |
| Annotation resampling strategy | Nearest neighbor interpolation to original spatial resolution |
| Image target spacing | Lowest resolution axis tenth percentile |
| Patch size | (128, 128, 128) |
| Batch size | 2 |
| Ensemble selection | 3D U-Net according to cross-validation performance |
| Positive Cohort | Negative Cohort | Significance | |
|---|---|---|---|
| Mean age | 63.1 | 55.9 | p < 0.001 |
| Sex (male) | n = 66 | n = 57 | p = 0.193 |
| Inter-Reader | Reference-Prediction | |
|---|---|---|
| PEF volume | Reader 1: 152.92 ± 134.85 mL | Reader 1: 152.92 ± 134.85 mL |
| Reader 2: 181.04 ± 131.55 mL | Prediction: 184.20 ± 132.19 mL | |
| (p = 0.105) | (p = 0.062) | |
| Correlation coefficient | r2 = 0.930 | r2 = 0.925 |
| Dice coefficient | 0.69 ± 0.10, median = 0.69 | 0.73 ± 0.10, median = 0.74 |
| Reference-Prediction | Significance | |
|---|---|---|
| PEF volume | Reference: 198.20 ± 159.78 mL | p = 0.875 |
| Prediction: 201.50 ± 160.93 | ||
| Correlation coefficient | r2 = 0.929 | N/A |
| Dice coefficient | 0.75 ± 0.01, median = 0.76 | N/A |
| Effect of confounding factors assessed with Dice coefficient: | ||
| Contrast administration | Contrast: 0.74 ± 0.19, median = 0.77 | p = 0.908 |
| No contrast: 0.75 ± 0.09, median = 0.76 | ||
| PEF size (>50 mL vs. >50 mL) | <50 mL: 0.67 ± 0.17, median = 0.74 | p = 0.086 |
| >50 mL: 0.75 ± 0.10, median = 0.77 | ||
| Hemopericardium presence | Hemopericardium: 0.72 ± 0.13, median = 0.73 | p = 0.097 |
| No hemopericardium: 0.76 ± 0.09, median = 0.78 | ||
| Pleural effusion presence | Pleural effusion: 0.73 ± 0.12, median = 0.74 | p = 0.116 |
| No pleural effusion: 0.77 ± 0.08, median = 0.79 | ||
| Other radiologically identified chest pathology | Visible pathology: 0.73 ± 0.12, median = 0.74 | p = 0.061 |
| No visible pathology: 0.77 ± 0.09, median = 0.78 | ||
| Hemopericardium | Simple PEF | Significance | |
|---|---|---|---|
| Hounsfield unit (HU) | 36.10 ± 9.72, median = 36 | 19.20 ± 5.52, median = 18 | p < 0.001 |
| Affect of contrast on Hounsfield unit: | |||
| Presence of contrast | 36.86 ± 9.65, median = 36 | 20.97 ± 6.35, median = 19 | p < 0.001 |
| No contrast | 33.99 ± 10.08, median = 35 | 17.59 ± 4.12, median = 17 | p < 0.001 |
| Autopsy-Reference | Reference-Prediction | Autopsy-Prediction | |
|---|---|---|---|
| PEF volume | Autopsy: 488.33 ± 232.41 mL | Reference: 515.26 ± 216.67 mL | Autopsy: 488.33 ± 232.41 mL |
| Reference: 515.26 ± 216.67 mL | Prediction: 301.69 ± 118.92 mL | Prediction: 301.69 ± 118.92 mL | |
| (p = 0.283) | (p < 0.001) | (p = 0.019) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilder-Smith, A.J.; Yang, S.; Weikert, T.; Bremerich, J.; Haaf, P.; Segeroth, M.; Ebert, L.C.; Sauter, A.; Sexauer, R. Automated Detection, Segmentation, and Classification of Pericardial Effusions on Chest CT Using a Deep Convolutional Neural Network. Diagnostics 2022, 12, 1045. https://doi.org/10.3390/diagnostics12051045
Wilder-Smith AJ, Yang S, Weikert T, Bremerich J, Haaf P, Segeroth M, Ebert LC, Sauter A, Sexauer R. Automated Detection, Segmentation, and Classification of Pericardial Effusions on Chest CT Using a Deep Convolutional Neural Network. Diagnostics. 2022; 12(5):1045. https://doi.org/10.3390/diagnostics12051045
Chicago/Turabian StyleWilder-Smith, Adrian Jonathan, Shan Yang, Thomas Weikert, Jens Bremerich, Philip Haaf, Martin Segeroth, Lars C. Ebert, Alexander Sauter, and Raphael Sexauer. 2022. "Automated Detection, Segmentation, and Classification of Pericardial Effusions on Chest CT Using a Deep Convolutional Neural Network" Diagnostics 12, no. 5: 1045. https://doi.org/10.3390/diagnostics12051045
APA StyleWilder-Smith, A. J., Yang, S., Weikert, T., Bremerich, J., Haaf, P., Segeroth, M., Ebert, L. C., Sauter, A., & Sexauer, R. (2022). Automated Detection, Segmentation, and Classification of Pericardial Effusions on Chest CT Using a Deep Convolutional Neural Network. Diagnostics, 12(5), 1045. https://doi.org/10.3390/diagnostics12051045