
Quantifying and Statistically Modeling Residual Pneumoperitoneum after Robotic-Assisted Laparoscopic Prostatectomy: A Prospective, Single-Center, Observational Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Surgery
2.3. Parameters
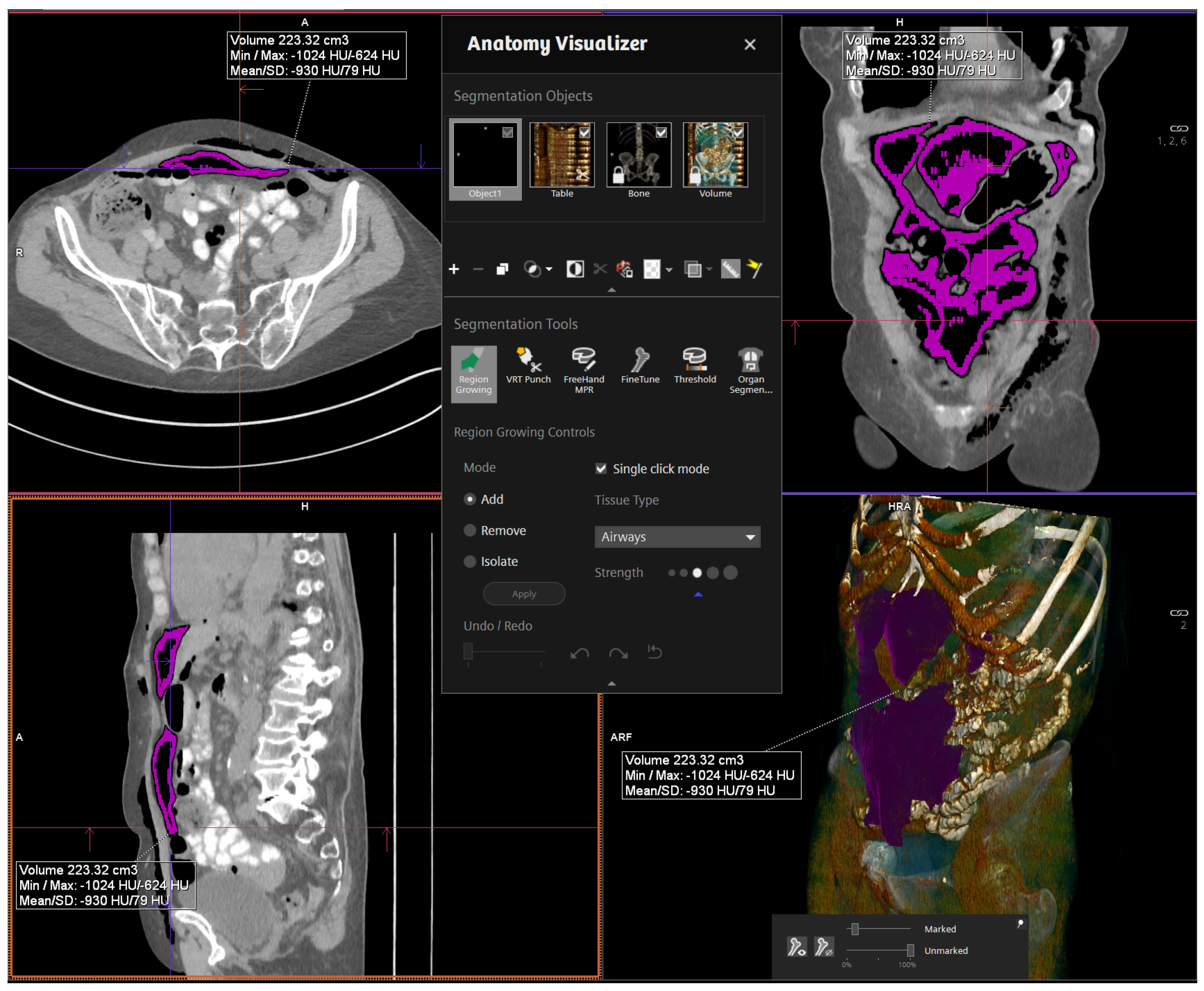
2.4. CT Parameters, RPP Measurement, and Data Management
3. Results
3.1. Demographic Data
3.2. Radiographic Assessment of Residual Pneumoperitoneum
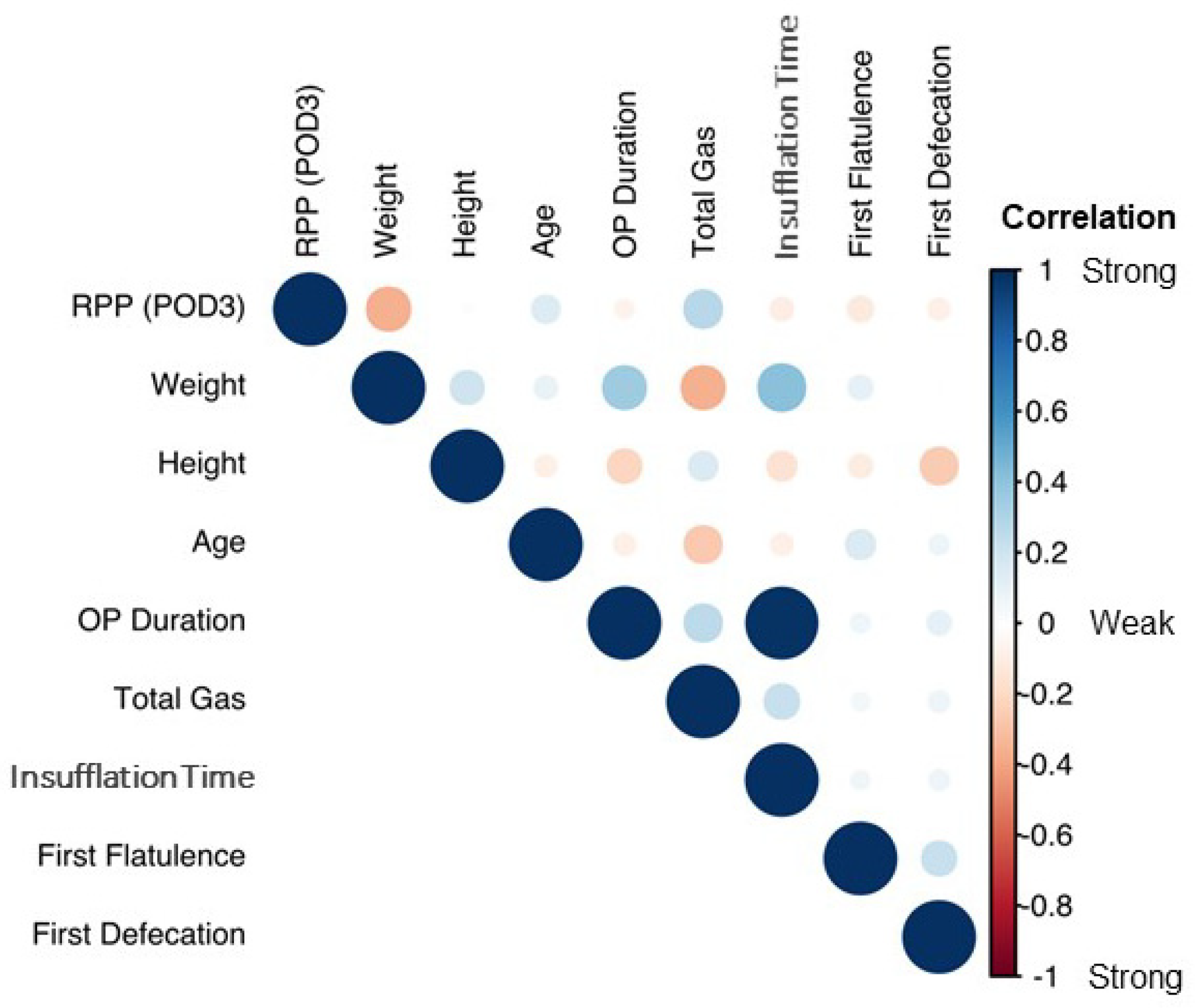
3.3. RPP Correlation with Demographic and Operative Data
3.4. Generating and Understanding a Predictive Model for RPP
4. Discussion
4.1. Description of RPP and Correlation to Demographics
4.2. Statistical Formula
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- van der Ploeg, A.P.T.; Ayez, N.; Akkersdijk, G.P.; van Rossem, C.C.; de Rooij, P.D. Postoperative pain after lobectomy: Robot-assisted, video-assisted and open thoracic surgery. J. Robot. Surg. 2020, 14, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Püschel, A.; Schafmayer, C.; Groß, J. Robot-assisted techniques in vascular and endovascular surgery. Langenbeck Arch. Surg. 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sciarra, A.; Frisenda, M.; Maggi, M.; Magliocca, F.M.; Ciardi, A.; Panebianco, V.; De Berardinis, E.; Salciccia, S.; Di Pierro, G.B.; Gentilucci, A.; et al. Prospective comparative trial on nerve-sparing radical prostatectomy using a robot-assisted versus laparoscopic technique: Expectation versus satisfaction and impact on surgical margins. Cent. Eur. J. Urol. 2021, 74, 169–177. [Google Scholar] [CrossRef]
- Maggard-Gibbons, M.; Girgis, M.; Ye, L.; Shenoy, R.; Mederos, M.; Childers, C.P.; Tang, A.; Mak, S.; Begashaw, M.; Booth, M.S.; et al. Robot-Assisted Procedures in General Surgery: Cholecystectomy, Inguinal and Ventral Hernia Repairs; BJS Open: Washington, DC, USA, 2020. [Google Scholar]
- Caglià, P.; Tracia, A.; Buffone, A.; Amodeo, L.; Tracia, L.; Amodeo, C.; Veroux, M. Physiopathology and clinical considerations of laparoscopic surgery in the elderly. Int. J. Surg. 2016, 33 (Suppl. 1), S97–S102. [Google Scholar] [CrossRef] [PubMed]
- Sabzi Sarvestani, A.; Zamiri, M. Residual Pneumoperitoneum Volume and Postlaparoscopic Cholecystectomy Pain. Anesthesiol. Pain Med. 2014, 4, e17366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanley, I.R.; Laurence, A.S.; Hill, J.C. Disappearance of intraperitoneal gas following gynaecological laparoscopy. Anaesthesia 2002, 57, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Gans, S.L.; Pols, M.A.; Stoker, J.; Boermeester, M.A. Guideline for the diagnostic pathway in patients with acute abdominal pain. Dig. Surg. 2015, 32, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Gelman, A. Prior distributions for variance parameters in hierarchical models (comment on article by Browne and Draper). Bayesian Anal. 2006, 1, 515–534. [Google Scholar] [CrossRef]
- Kruschke, J.K.; Liddell, T.M. The Bayesian New Statistics: Hypothesis testing, estimation, meta-analysis, and power analysis from a Bayesian perspective. Psychon. Bull. Rev. 2018, 25, 178–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Shrimpton, P.C.; Hillier, M.C.; Lewis, M.A.; Dunn, M. National survey of doses from CT in the UK: 2003. Br. J. Radiol. 2006, 79, 968–980. [Google Scholar] [CrossRef] [PubMed]
- Bürkner, P.-C. brms: An R Package for Bayesian Multilevel Models. J. Stat. Softw. 2017, 80, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Gelman, A.; Rubin, D.B.; Carlin, J.B.; Stern, H. Bayesian Data Analysis, 1st ed.; Taylor and Francis: London, UK, 1995. [Google Scholar] [CrossRef]
- Socea, B.; Bogaciu, C.; Carâp, A.; Nica, A.; Smaranda, A.; Băleanu, V.; Virgil Davitoiu, D.; Bratu, O.; Constantin, V. Pneumoperitoneum diagnosed using ultrasonography—A narrative review of the literature. Res. Sci. 2019, 1, 219. [Google Scholar]
- Hindman, N.M.; Kang, S.; Parikh, M.S. Common postoperative findings unique to laparoscopic surgery. Radiographics 2014, 34, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Elbiss, H.M.; Abu-Zidan, F.M. Bowel injury following gynecological laparoscopic surgery. Afr. Health Sci. 2017, 17, 1237–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, E.Y.; Yoo, J.H.; Rodrigues, A.J.J.; Utiyama, E.M.; Birolini, D.; Rasslan, S. A computerized tomography scan method for calculating the hernia sac and abdominal cavity volume in complex large incisional hernia with loss of domain. Hernia 2010, 14, 63–69. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Mean | SD | Median | IQR | |
|---|---|---|---|---|---|
| Age | 31 | 66.2 | 6.7 | 67 | 62–70.5 |
| Weight (kg) | 31 | 83.3 | 12.4 | 83 | 75.5–90.5 |
| Height (cm) | 31 | 177.2 | 6.1 | 178 | 173–180.5 |
| BMI | 31 | 26.6 | 4.1 | 26.0 | 24.1–29.2 |
| OP Duration (min) | 31 | 302.4 | 43.4 | 306 | 270–328 |
| Total Gas (mL) | 29 | 971,448 | 426,203 | 941,000 | 775,000–1,242,000 |
| Insufflation Time (min) | 30 | 278.9 | 42.3 | 276.5 | 255–304.2 |
| RPP POD 3 (mL) | 31 | 37.6 | 61.8 | 9.6 | 3.9–31.8 |
| RPP POD 5 (mL) | 28 | 19.8 | 48.1 | 1.4 | 0.2–5.6 |
| RPP POD 7 (mL) | 29 | 10.1 | 25.8 | 0.1 | 0.0–1.5 |
| Postoperative Day | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|
| Normal Weight Patient (RPP in mL) | |||||
| Upper limit (97.5%) | 2500.95 | 1523.20 | 856.85 | 573.02 | 411.99 |
| Lower limit (2.5%) | 0.05 | 0 | 0 | 0 | 0 |
| Overweight Patient (RPP in mL) | |||||
| Upper limit (97.5%) | 1271.42 | 748.61 | 472.70 | 315.49 | 219.31 |
| Lower limit (2.5%) | 0.02 | 0 | 0 | 0 | 0 |
| Obese Patient (RPP in mL) | |||||
| Upper limit (97.5%) | 154.94 | 87.48 | 45.96 | 29.52 | 24.46 |
| Lower limit (2.5%) | 0 | 0 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramakrishnan, V.M.; Niemann, T.; Maletzki, P.; Guenther, E.; Bujaroska, T.; Labulo, O.; Li, Z.; Slieker, J.; Kubik-Huch, R.A.; Lehmann, K.; et al. Quantifying and Statistically Modeling Residual Pneumoperitoneum after Robotic-Assisted Laparoscopic Prostatectomy: A Prospective, Single-Center, Observational Study. Diagnostics 2022, 12, 785. https://doi.org/10.3390/diagnostics12040785
Ramakrishnan VM, Niemann T, Maletzki P, Guenther E, Bujaroska T, Labulo O, Li Z, Slieker J, Kubik-Huch RA, Lehmann K, et al. Quantifying and Statistically Modeling Residual Pneumoperitoneum after Robotic-Assisted Laparoscopic Prostatectomy: A Prospective, Single-Center, Observational Study. Diagnostics. 2022; 12(4):785. https://doi.org/10.3390/diagnostics12040785
Chicago/Turabian StyleRamakrishnan, Venkat M., Tilo Niemann, Philipp Maletzki, Edward Guenther, Teodora Bujaroska, Olanrewaju Labulo, Zhufeng Li, Juliette Slieker, Rahel A. Kubik-Huch, Kurt Lehmann, and et al. 2022. "Quantifying and Statistically Modeling Residual Pneumoperitoneum after Robotic-Assisted Laparoscopic Prostatectomy: A Prospective, Single-Center, Observational Study" Diagnostics 12, no. 4: 785. https://doi.org/10.3390/diagnostics12040785
APA StyleRamakrishnan, V. M., Niemann, T., Maletzki, P., Guenther, E., Bujaroska, T., Labulo, O., Li, Z., Slieker, J., Kubik-Huch, R. A., Lehmann, K., Nocito, A., & Hefermehl, L. J. (2022). Quantifying and Statistically Modeling Residual Pneumoperitoneum after Robotic-Assisted Laparoscopic Prostatectomy: A Prospective, Single-Center, Observational Study. Diagnostics, 12(4), 785. https://doi.org/10.3390/diagnostics12040785