Diagnostics Literacy Advocacy Model for Vulnerable Populations

{kind=link}
Abstract
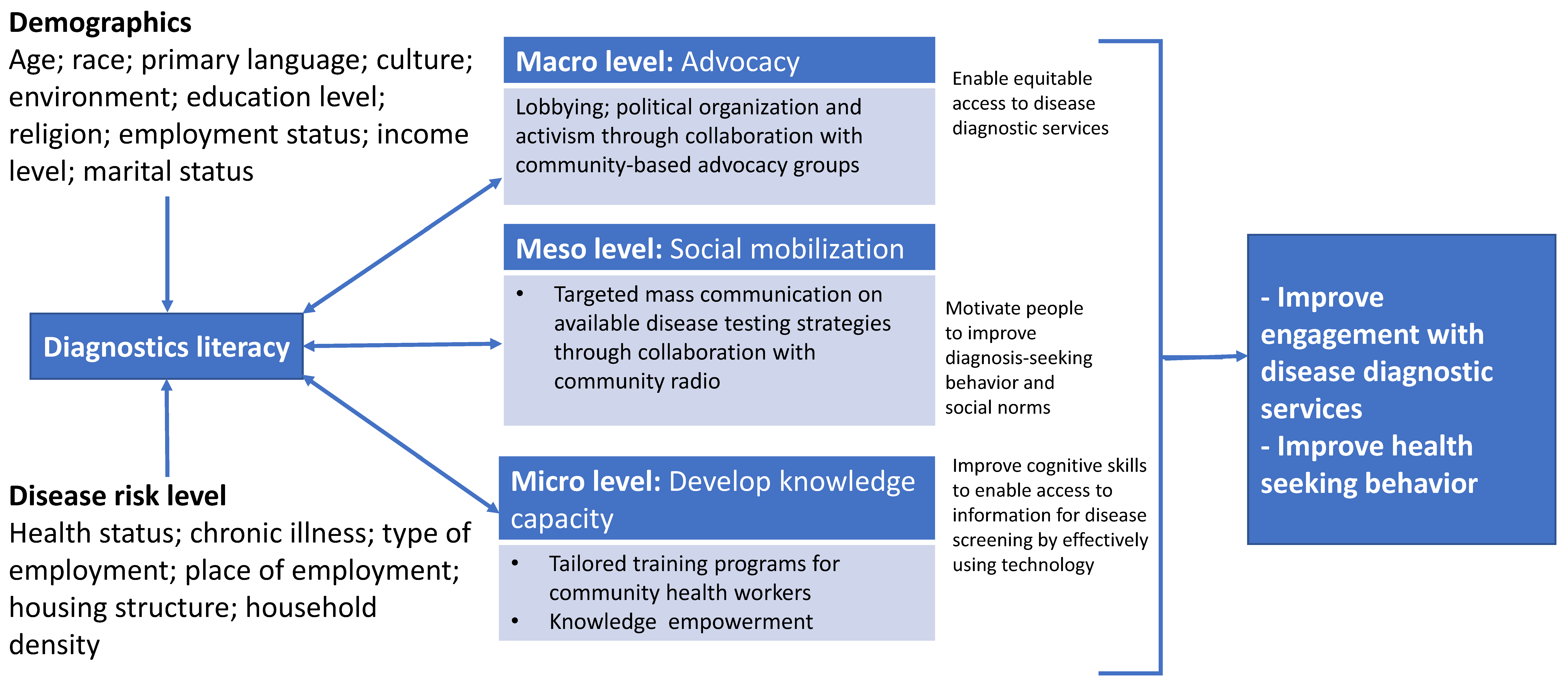
:- 1.
- Macro level—Advocacy
- Conduct a key stakeholder workshop and invite all relevant community leaders, policy makers and implementers.
- Establish a disease diagnostics advocacy group comprising diagnostics experts, health promotion experts and health experts.
- Develop and implement tailored disease testing and linkage-to-care advocacy programs for different population groups.
- 2.
- Meso level—Social mobilization
- Create social media platforms that inform societies about the importance of regular and rapid disease testing, with information about linkage-to-care to remove physical barriers that traditionally impede access to disease testing support and resources.
- Collaborate with religious leaders to develop faith-based diagnostic advocacy programs to help influence health-seeking behaviors and increase engagement with disease testing and linkage-to-care services.
- Develop local newspaper, TV and radio station based diagnostic advocacy programs.
- 3.
- Micro level—Develop knowledge capacity
- Educate health workers during a training program on disease diagnostics literacy. The curriculum could be delivered using a learning management system linked app.
- Incorporate diagnostic literacy as part of school-based health education services. Edutainment could be used as a public health communication intervention to improve diagnostic literacy through music, jingles, poetry, dramas and puppetry.
- Incorporate diagnostics literacy as part of community-based health education services.
Funding
Acknowledgments
Conflicts of Interest
References
- International Union for Health Promotion and Education. COVID-19 Response for the African Region and India. Available online: https://www.iuhpe.org/images/IUHPE/News/Final-Report_Phase1_IUHPE-Support-to-COVID-19-Response-in-Africa-1.pdf (accessed on 30 January 2022).
- Sheikhzadeh, E.; Eissa, S.; Ismail, A.; Zourob, M. Diagnostic techniques for COVID-19 and new developments. Talanta 2020, 220, 121392. [Google Scholar] [CrossRef] [PubMed]
- Fleming, K.A.; Horton, S.; Wilson, M.L.; Atun, R.; Destigter, K.; Flanigan, J.; Sayed, S.; Adam, P.; Aguilar, B.; Andronikou, S.; et al. The Lancet Commission on diagnostics: Transforming access to diagnostics. Lancet 2021, 398, 1997–2050. [Google Scholar] [CrossRef]
- Goto, E.; Ishikawa, H.; Okuhara, T.; Kiuchi, T. Relationship of health literacy with utilization of health-care services in a general Japanese population. Prev. Med. Rep. 2019, 14, 100811. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine of the National Academies. Health Literacy: A Prescription to End Confusion; The National Academic Press: Washington, DC, USA, 2004. [Google Scholar]
- Videto, D.M.; Dake, J.A. Promoting Health Literacy Through Defining and Measuring Quality School Health Education. Health Promot. Pract. 2019, 20, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Rudd, R.E. Improving Americans’ Health Literacy. N. Engl. J. Med. 2010, 363, 2283–2285. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mashamba-Thompson, T.P. Diagnostics Literacy Advocacy Model for Vulnerable Populations. Diagnostics 2022, 12, 716. https://doi.org/10.3390/diagnostics12030716
Mashamba-Thompson TP. Diagnostics Literacy Advocacy Model for Vulnerable Populations. Diagnostics. 2022; 12(3):716. https://doi.org/10.3390/diagnostics12030716
Chicago/Turabian StyleMashamba-Thompson, Tivani P. 2022. "Diagnostics Literacy Advocacy Model for Vulnerable Populations" Diagnostics 12, no. 3: 716. https://doi.org/10.3390/diagnostics12030716
APA StyleMashamba-Thompson, T. P. (2022). Diagnostics Literacy Advocacy Model for Vulnerable Populations. Diagnostics, 12(3), 716. https://doi.org/10.3390/diagnostics12030716