
Loss of Single-Stranded DNA Binding Protein 2 Expression Is Associated with Aggressiveness and Poor Overall Survival in Patients with Invasive Breast Carcinoma

 , , , , , , and
, , , , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Tumor Samples
2.2. Tissue Microarray (TMA) Construction
2.3. Immunohistochemical (IHC) Staining
2.4. Interpretation of IHC Staining and Molecular Subtypes
2.5. Statistical Analysis
3. Results
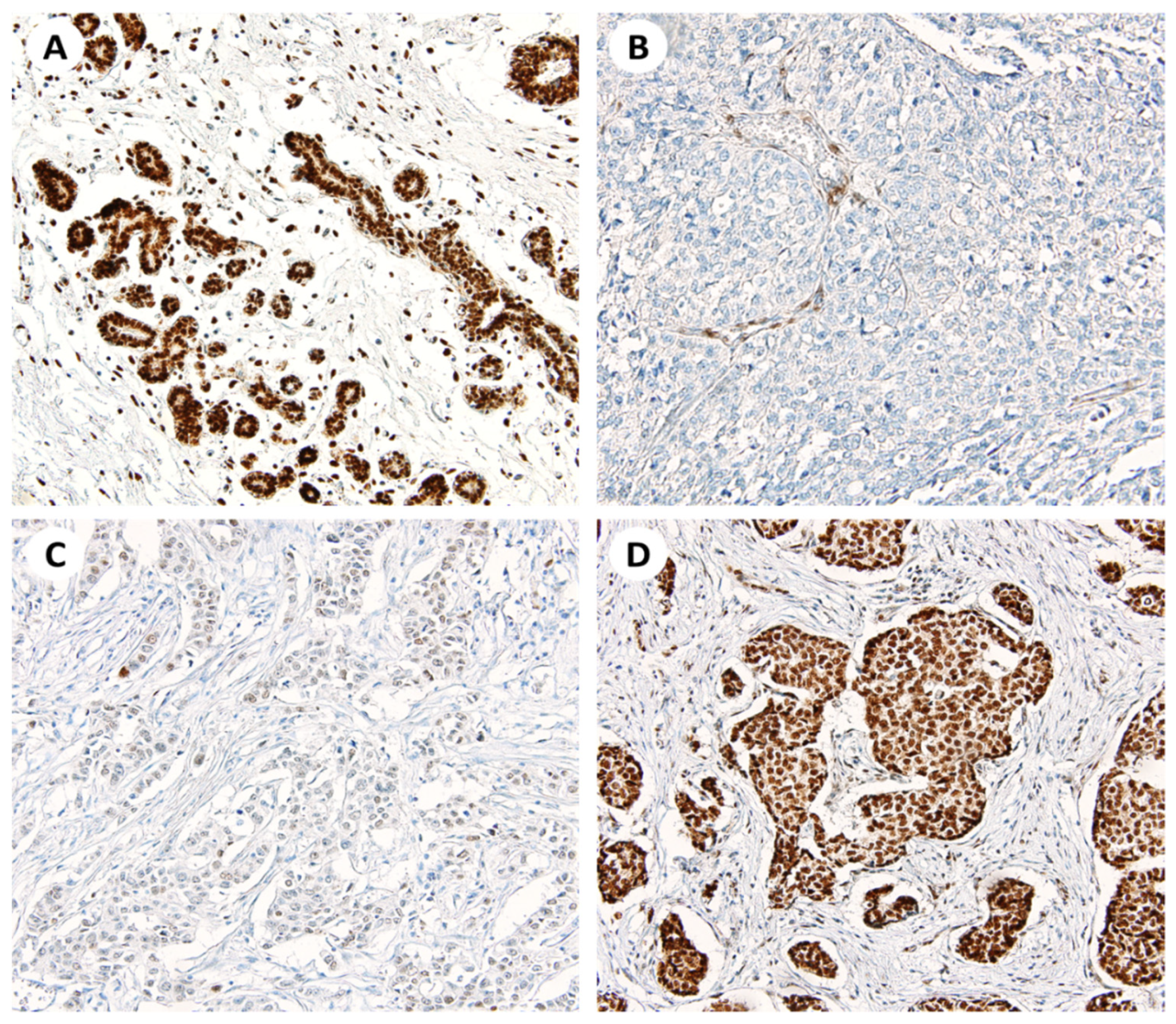
3.1. Patterns of SSBP2 Expression
3.2. Correlations between Nuclear SSBP2 Expression and Clinicopathological Parameters
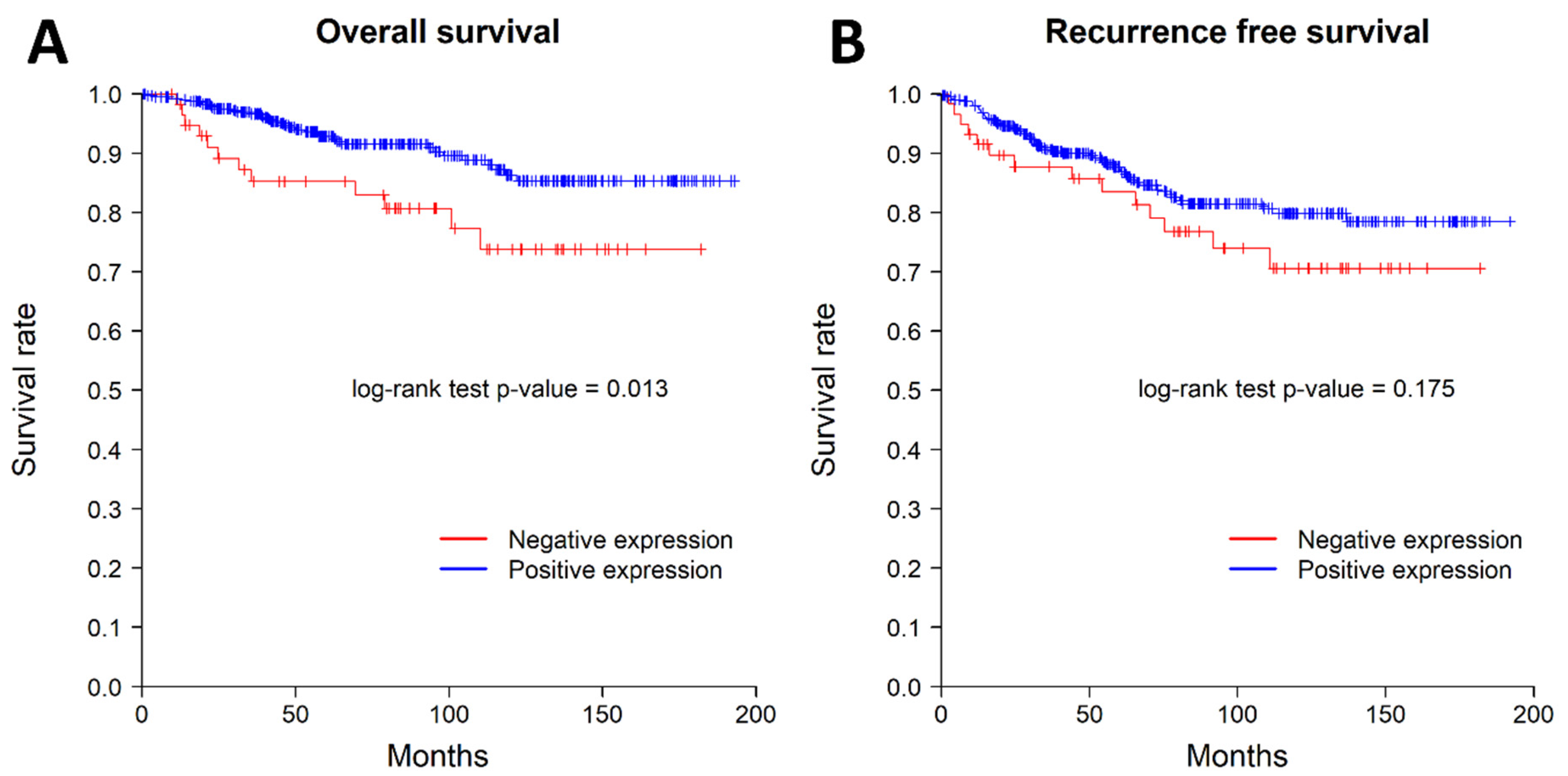
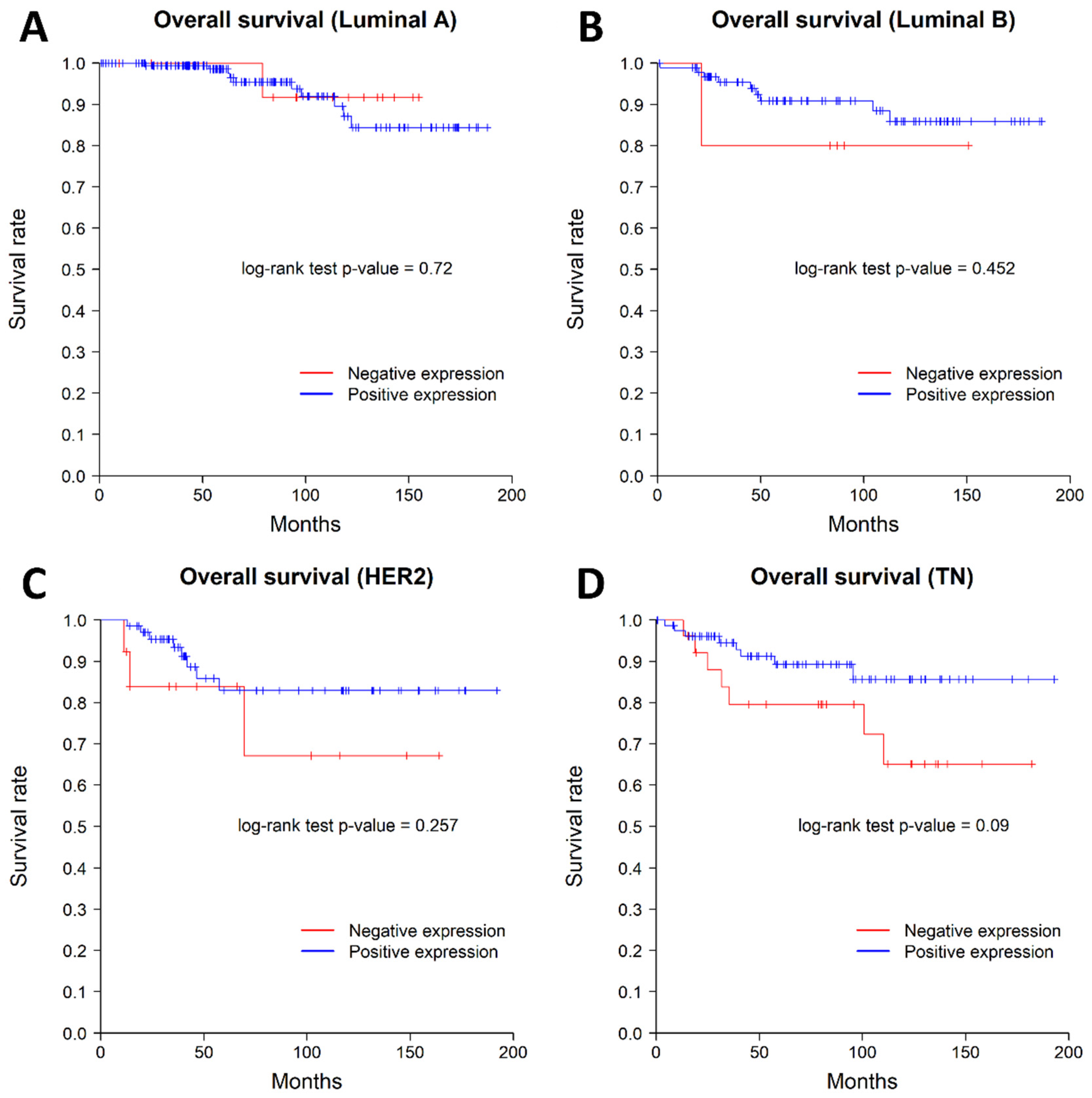
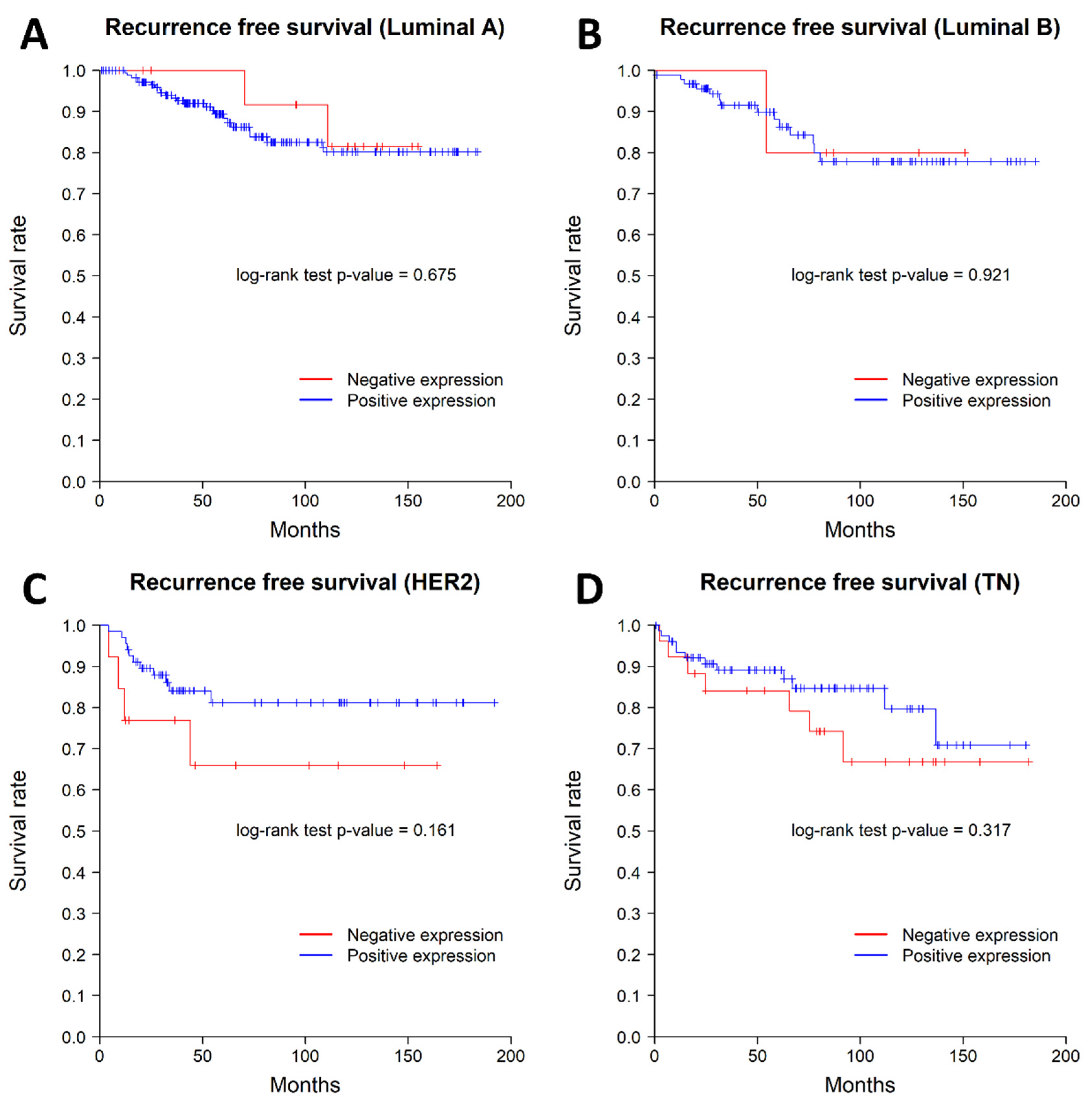
3.3. Correlations between Nuclear SSBP2 Expression and Patient Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Jang, S.M.; Ahn, H.; Sim, J.; Yi, K.; Chung, Y.; Han, H.; Rehman, A.; Chung, M.S.; Jang, K.; et al. Clinicopathological Significance of Dual-Specificity Protein Phosphatase 4 Expression in Invasive Ductal Carcinoma of the Breast. J. Breast Cancer 2015, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Jezierska, A.; Motyl, T. Matrix Metalloproteinase-2 Involvement in Breast. Med. Sci. Monit. 2009, 15, RA32-40. [Google Scholar] [PubMed]
- Bertolo, C.; Guerrero, D.; Vicente, F.; Cordoba, A.; Esteller, M.; Ropero, S.; Guillen-Grima, F.; Martinez-Peñuela, J.M.; Lera, J.M. Differences and Molecular Immunohistochemical Parameters in the Subtypes of Infiltrating Ductal Breast Cancer. Am. J. Clin. Pathol. 2008, 130, 414–424. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Th?rlimann, B.; Senn, H.-J.; Albain, K.S.; Andr?, F.; Bergh, J.; et al. Personalizing the Treatment of Women with Early Breast Cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Wang, Y.; Klumpp, S.; Amin, H.M.; Liang, H.; Li, J.; Estrov, Z.; Zweidler-McKay, P.; Brandt, S.J.; Agulnick, A.; Nagarajan, L. SSBP2 Is an in Vivo Tumor Suppressor and Regulator of LDB1 Stability. Oncogene 2010, 29, 3044–3053. [Google Scholar] [CrossRef]
- Li, J.; Kurasawa, Y.; Wang, Y.; Clise-Dwyer, K.; Klumpp, S.A.; Liang, H.; Tailor, R.C.; Raymond, A.C.; Estrov, Z.; Brandt, S.J.; et al. Requirement for Ssbp2 in Hematopoietic Stem Cell Maintenance and Stress Response. J. Immunol. 2014, 193, 4654–4662. [Google Scholar] [CrossRef]
- Nishioka, N.; Nagano, S.; Nakayama, R.; Kiyonari, H.; Ijiri, T.; Taniguchi, K.; Shawlot, W.; Hayashizaki, Y.; Westphal, H.; Behringer, R.R.; et al. Ssdp1 Regulates Head Morphogenesis of Mouse Embryos by Activating the Lim1-Ldb1 Complex. Development 2005, 132, 2535–2546. [Google Scholar] [CrossRef]
- Zhu, M.; Jiang, B.; Zuo, H.; Wang, X.; Ge, H.; Huang, Z. LIM-Domain-Binding Protein 1 Mediates Cell Proliferation and Drug Resistance in Colorectal Cancer. Front. Surg. 2022, 8, 790380. [Google Scholar] [CrossRef]
- Liang, H.; Samanta, S.; Nagarajan, L. SSBP2, a Candidate Tumor Suppressor Gene, Induces Growth Arrest and Differentiation of Myeloid Leukemia Cells. Oncogene 2005, 24, 2625–2634. [Google Scholar] [CrossRef]
- Liu, J.-W.; Nagpal, J.K.; Sun, W.; Lee, J.; Kim, M.S.; Ostrow, K.L.; Zhou, S.; Jeronimo, C.; Henrique, R.; Van Criekinge, W.; et al. SsDNA-Binding Protein 2 Is Frequently Hypermethylated and Suppresses Cell Growth in Human Prostate Cancer. Clin. Cancer Res. 2008, 14, 3754–3760. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Decker, P.A.; Rice, T.; McCoy, L.S.; Smirnov, I.; Patoka, J.S.; Hansen, H.M.; Wiemels, J.L.; Tihan, T.; Prados, M.D.; et al. SSBP2 Variants Are Associated with Survival in Glioblastoma Patients. Clin. Cancer Res. 2012, 18, 3154–3162. [Google Scholar] [CrossRef]
- Kim, H.; Kim, Y.; Chung, Y.; Abdul, R.; Sim, J.; Ahn, H.; Shin, S.-J.; Paik, S.S.; Kim, H.J.; Jang, K.; et al. Single-Stranded DNA Binding Protein 2 Expression Is Associated with Patient Survival in Hepatocellular Carcinoma. BMC Cancer 2018, 18, 1244. [Google Scholar] [CrossRef] [PubMed]
- Bang, S.; Kim, H.; Jang, K.; Paik, S.S.; Shin, S.-J. The Loss of Nuclear Expression of Single-Stranded DNA Binding Protein 2 of Gastric Adenocarcinoma and Its Prognostic Role: Analysis of Molecular Subtype. PLoS ONE 2020, 15, e0236896. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.; Kim, H.; Bang, S.; Jang, K.; Paik, S.S.; Shin, S.-J. Nuclear Expression Loss of SSBP2 Is Associated with Poor Prognostic Factors in Colorectal Adenocarcinoma. Diagnostics 2020, 10, 1097. [Google Scholar] [CrossRef]
- Kim, H.; Kim, Y.; Bang, S.; Park, S.; Jee, S.; Sim, J.; Shin, S.-J.; Paik, S.S.; Jang, K. Low Expression of Single-Stranded DNA Binding Protein 2 (SSBP2) Predicts Unfavourable Postoperative Outcomes in Patients with Clear Cell Renal Cell Carcinoma. In Vivo 2020, 34, 101–107. [Google Scholar] [CrossRef]
- Feeley, L.P.; Mulligan, A.M.; Pinnaduwage, D.; Bull, S.B.; Andrulis, I.L. Distinguishing Luminal Breast Cancer Subtypes by Ki67, Progesterone Receptor or TP53 Status Provides Prognostic Information. Mod. Pathol. 2014, 27, 554–561. [Google Scholar] [CrossRef]
- Fairman, J.; Wang, R.; Liang, H.; Zhao, L.; Saltman, D.; Liang, J.; Nagarajan, L. Translocations and Deletions of 5q13.1 in Myelodysplasia and Acute Myelogenous Leukemia: Evidence for a Novel Critical Locus. Blood 1996, 88, 2259–2266. [Google Scholar] [CrossRef]
- Castro, P.; Liang, H.; Liang, J.C.; Nagarajan, L. A Novel, Evolutionarily Conserved Gene Family with Putative Sequence-Specific Single-Stranded DNA-Binding Activity. Genomics 2002, 80, 78–85. [Google Scholar] [CrossRef]
- Haryono, S.J.; Datasena, I.G.B.; Santosa, W.B.; Mulyarahardja, R.; Sari, K. A Pilot Genome-Wide Association Study of Breast Cancer Susceptibility Loci in Indonesia. Asian Pacific J. Cancer Prev. 2015, 16, 2231–2235. [Google Scholar] [CrossRef]
- Huang, Y.; Chang, X.; Lee, J.; Cho, Y.G.; Zhong, X.; Park, I.-S.; Liu, J.-W.; Califano, J.A.; Ratovitski, E.A.; Sidransky, D.; et al. Cigarette Smoke Induces Promoter Methylation of Single-Stranded DNA-Binding Protein 2 in Human Esophageal Squamous Cell Carcinoma. Int. J. Cancer 2011, 128, 2261–2273. [Google Scholar] [CrossRef] [PubMed]
- Brait, M.; Maldonado, L.; Noordhuis, M.; Begum, S.; Loyo, M.; Poeta, M.L.; Barbosa, A.; Fazio, V.M.; Angioli, R.; Rabitti, C.; et al. Association of Promoter Methylation of VGF and PGP9.5 with Ovarian Cancer Progression. PLoS ONE 2013, 8, e70878. [Google Scholar] [CrossRef]
- Kagohara, L.T.; Schussel, J.L.; Subbannayya, T.; Sahasrabuddhe, N.; Lebron, C.; Brait, M.; Maldonado, L.; Valle, B.L.; Pirini, F.; Jahuira, M.; et al. Global and Gene-Specific DNA Methylation Pattern Discriminates Cholecystitis from Gallbladder Cancer Patients in Chile. Future Oncol. 2015, 11, 233–249. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristics | Value (%) |
|---|---|
| Age (years, median, mean ± SD) | 51, 52.9 ± 11.1 |
| Size | |
| ≤2 cm | 226 (46.0%) |
| >2 cm | 265 (54.0%) |
| Histological grade | |
| G1 | 104 (21.2%) |
| G2 | 225 (45.8%) |
| G3 | 162 (33.0%) |
| pT stage | |
| T1 | 226 (46.0%) |
| T2 | 223 (45.4%) |
| T3 | 28 (5.7%) |
| T4 | 14 (2.9%) |
| pN stage | |
| N0 | 307 (62.5%) |
| N1 | 108 (22.0%) |
| N2 | 41 (8.4%) |
| N3 | 35 (7.1%) |
| AJCC stage | |
| I | 183 (37.3%) |
| II | 207 (42.2%) |
| III | 92 (18.7%) |
| IV | 9 (1.8%) |
| LN metastasis | |
| Negative | 307 (62.5%) |
| Positive | 184 (37.5%) |
| Distant metastasis | |
| Negative | 482 (98.2%) |
| Positive | 9 (1.8%) |
| ER status | |
| Negative | 192 (39.1%) |
| Positive | 299 (60.9%) |
| PR status | |
| Negative | 199 (40.5%) |
| Positive | 292 (59.5%) |
| HER2 status | |
| Negative | 338 (68.9%) |
| Positive | 153 (31.1%) |
| Molecular subtype | |
| Luminal A | 200 (40.7%) |
| Luminal B | 108 (22.0%) |
| HER2 | 76 (15.5%) |
| TNBC | 107 (21.8%) |
| Parameter | SSBP2 Expression | p Value | ||
|---|---|---|---|---|
| Positive (n = 430) No. (%) | Negative (n = 61) No. (%) | |||
| Age (years, mean ± SD) | 0.427 † | |||
| 52.7 ± 10.9 | 54 ± 12.1 | |||
| Size | <0.001 | |||
| ≤2 cm | 210 (48.8%) | 16 (26.2%) | ||
| >2 cm | 220 (51.2%) | 45 (73.8%) | ||
| Histological grade | 0.016 * | |||
| G1 | 95 (22.1%) | 9 (14.8%) | ||
| G2 | 202 (47.0%) | 23 (37.7%) | ||
| G3 | 133 (30.9%) | 29 (47.5%) | ||
| pT stage | 0.001 * | |||
| T1 | 213 (49.6%) | 13 (21.3%) | ||
| T2 | 182 (42.3%) | 41 (67.2%) | ||
| T3 | 25 (5.8%) | 3 (4.9%) | ||
| T4 | 10 (2.3%) | 4 (6.6%) | ||
| pN stage | 0.958 * | |||
| N0 | 269 (62.6%) | 38 (62.3%) | ||
| N1 | 94 (21.9%) | 14 (23.3%) | ||
| N2 | 37 (8.6%) | 4 (6.6%) | ||
| N3 | 30 (7.0%) | 5 (8.2%) | ||
| AJCC stage | 0.053 * | |||
| I | 170 (39.5%) | 13 (21.3%) | ||
| II | 172 (40.0%) | 35 (57.4%) | ||
| III | 81 (18.8%) | 11 (18.0%) | ||
| IV | 7 (1.6%) | 2 (3.3%) | ||
| LN metastasis | 0.968 | |||
| Negative | 269 (62.6%) | 38 (62.3%) | ||
| Positive | 161 (37.4%) | 23 (37.7%) | ||
| Distant metastasis | 0.368 | |||
| Negative | 423 (98.4%) | 59 (96.7%) | ||
| Positive | 7 (1.6%) | 2 (3.3%) | ||
| ER status | <0.001 | |||
| Negative | 152 (35.3%) | 39 (63.9%) | ||
| Positive | 278 (64.7%) | 22 (36.1%) | ||
| PR status | 0.233 | |||
| Negative | 170 (39.5%) | 29 (47.5%) | ||
| Positive | 260 (60.5%) | 32 (52.5%) | ||
| HER2 status | 0.374 | |||
| Negative | 293 (68.1%) | 45 (73.8%) | ||
| Positive | 137 (31.9%) | 16 (26.2%) | ||
| Molecular subtype | <0.001 | |||
| Luminal A | 183 (42.6%) | 17 (27.9%) | ||
| Luminal B | 95 (22.1%) | 5 (8.2%) | ||
| HER2 | 71 (16.5%) | 13 (21.3%) | ||
| TNBC | 81 (18.8%) | 26 (42.6%) | ||
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age (per 1 year) | 0.994 | 0.967–1.021 | 0.648 | 0.995 | 0.968–1.023 | 0.723 |
| Histological grade 3 (vs. 1, 2) | 2.48 | 1.398–4.4 | 0.002 | 1.578 | 0.832–2.994 | 0.163 |
| pT stage 3, 4 (vs. 1, 2) | 2.701 | 1.262–5.783 | 0.01 | 1.853 | 0.819–4.192 | 0.139 |
| ER status positive (vs. negative) | 0.466 | 0.262–0.829 | 0.009 | 0.627 | 0.324–1.213 | 0.166 |
| HER2 status positive (vs. negative) | 1.519 | 0.847–2.723 | 0.161 | 1.35 | 0.742–2.457 | 0.326 |
| LN metastasis positive (vs. negative) | 2.483 | 1.378–4.474 | 0.002 | 2.228 | 1.205–4.12 | 0.011 |
| SSBP2 status negative (vs. positive) | 2.242 | 1.162–4.325 | 0.016 | 1.942 | 0.97–3.89 | 0.061 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.; Jee, S.; Son, H.; Cha, H.; Bang, S.; Kim, H.; Shin, S.-J.; Cha, C.; Chung, M.S.; Myung, J.; et al. Loss of Single-Stranded DNA Binding Protein 2 Expression Is Associated with Aggressiveness and Poor Overall Survival in Patients with Invasive Breast Carcinoma. Diagnostics 2022, 12, 487. https://doi.org/10.3390/diagnostics12020487
Park H, Jee S, Son H, Cha H, Bang S, Kim H, Shin S-J, Cha C, Chung MS, Myung J, et al. Loss of Single-Stranded DNA Binding Protein 2 Expression Is Associated with Aggressiveness and Poor Overall Survival in Patients with Invasive Breast Carcinoma. Diagnostics. 2022; 12(2):487. https://doi.org/10.3390/diagnostics12020487
Chicago/Turabian StylePark, Hosub, Seungyun Jee, Hwangkyu Son, Hyebin Cha, Seongsik Bang, Hyunsung Kim, Su-Jin Shin, Chihwan Cha, Min Sung Chung, Jaekyung Myung, and et al. 2022. "Loss of Single-Stranded DNA Binding Protein 2 Expression Is Associated with Aggressiveness and Poor Overall Survival in Patients with Invasive Breast Carcinoma" Diagnostics 12, no. 2: 487. https://doi.org/10.3390/diagnostics12020487
APA StylePark, H., Jee, S., Son, H., Cha, H., Bang, S., Kim, H., Shin, S.-J., Cha, C., Chung, M. S., Myung, J., & Paik, S. S. (2022). Loss of Single-Stranded DNA Binding Protein 2 Expression Is Associated with Aggressiveness and Poor Overall Survival in Patients with Invasive Breast Carcinoma. Diagnostics, 12(2), 487. https://doi.org/10.3390/diagnostics12020487