
Sudden Sensorineural Hearing Loss in the COVID-19 Pandemic: A Systematic Review and Meta-Analysis

 ,
, 
 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Electronic Database Search
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
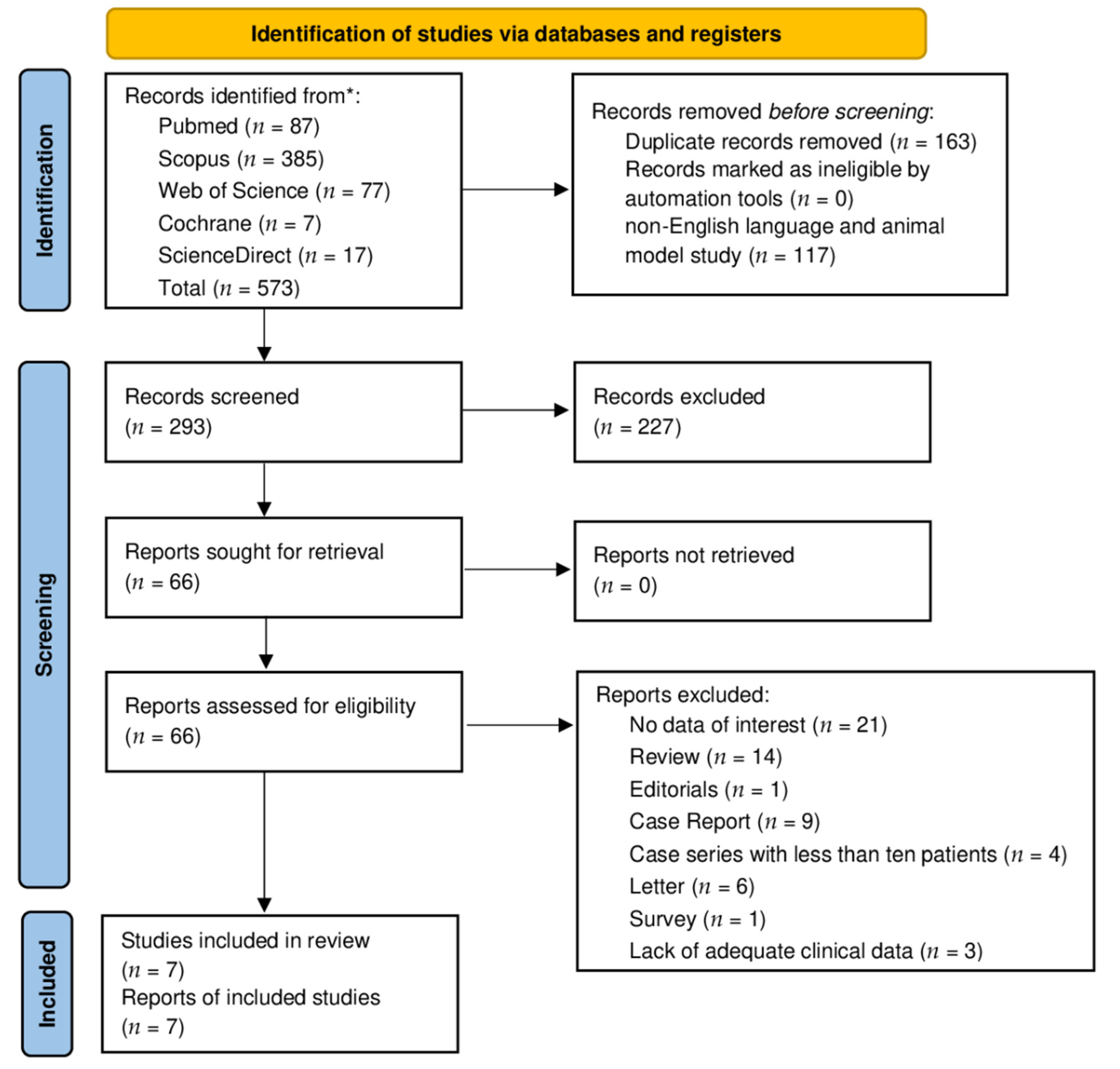
3.1. Retrieving Studies
3.2. Quality Assessment
3.3. Qualitative Synthesis
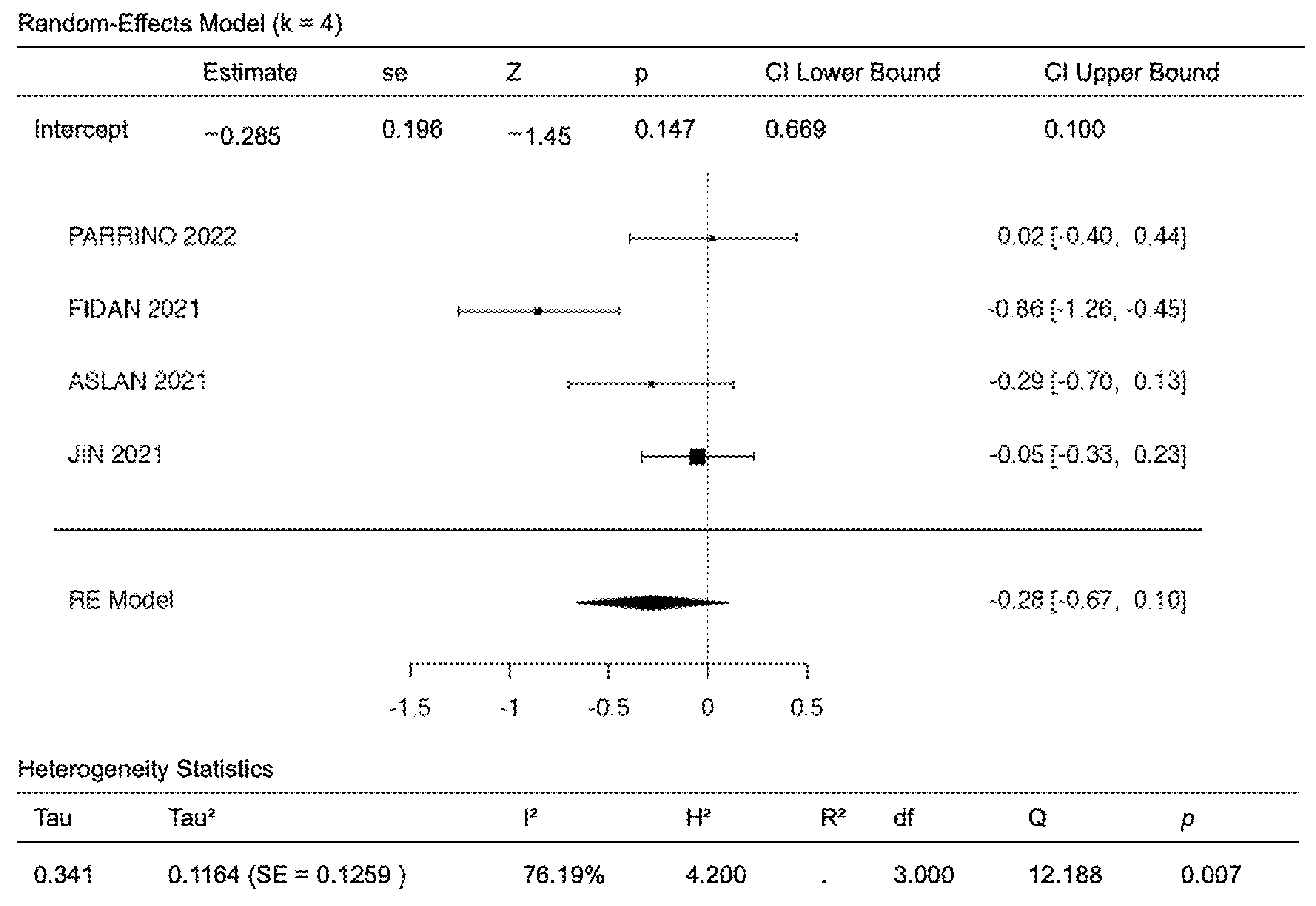
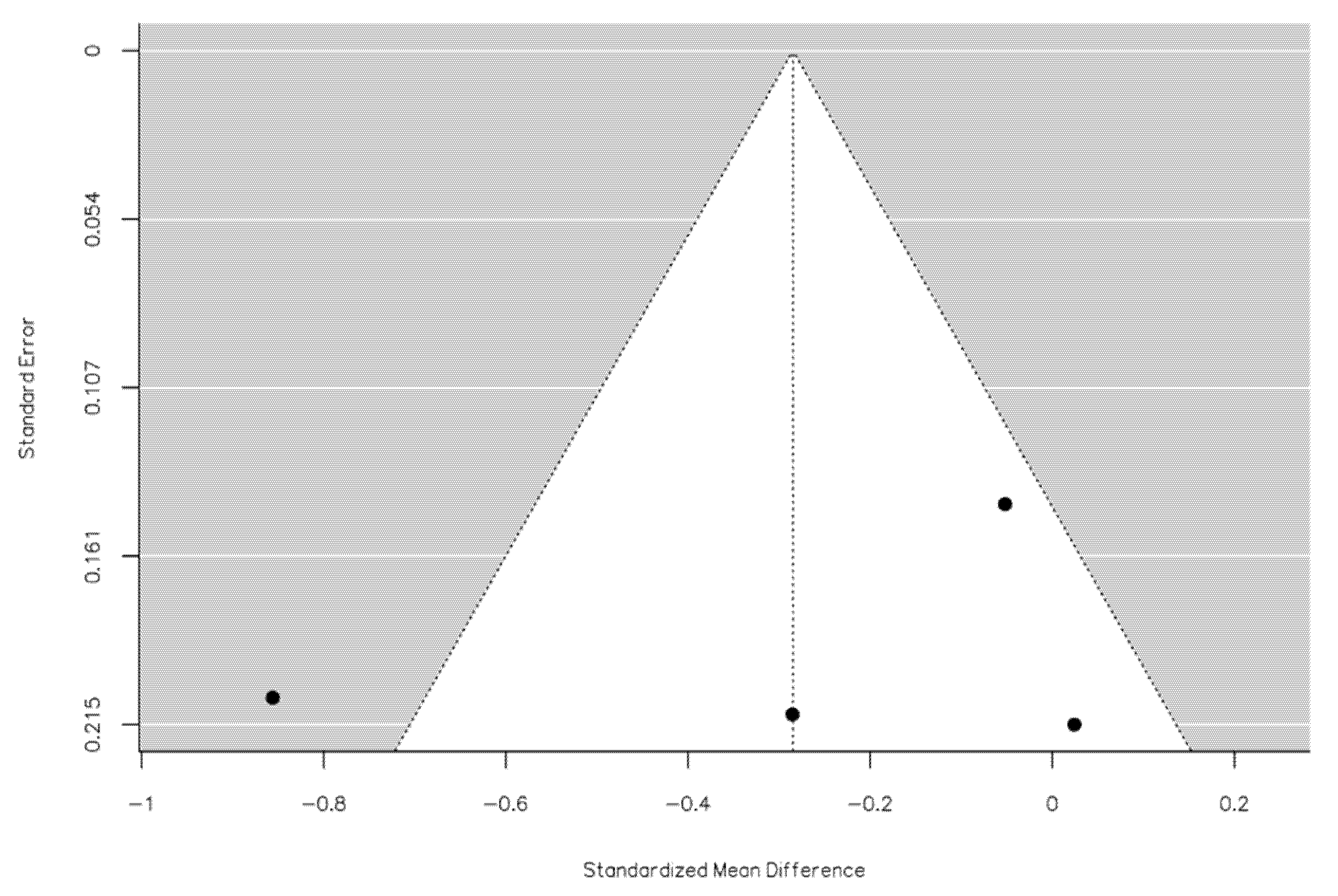
3.4. Quantitative Analysis
4. Discussion
4.1. Audio-Vestibular Symptoms in COVID-19: Hypotheses on Patho-Physiology
4.2. Incidence of Audiological Symptoms during the Pandemic Period
4.3. Demographics and Clinical Features of SSNHL Cases during the Pandemic Period
4.4. Clinical Features of SSNHL in COVID-19 Patients
4.5. SSNHL Treatment, Outcome, and Follow-up in the Pandemic Scenario
4.6. Quality of Evidence on SSNHL during COVID-19 Pandemic
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chandrasekhar, S.S.; Tsai Do, B.S.; Schwartz, S.R.; Bontempo, L.J.; Faucett, E.A.; Finestone, S.A.; Hollingsworth, D.B.; Kelley, D.M.; Kmucha, S.T.; Moonis, G.; et al. Clinical Practice Guideline: Sudden Hearing Loss (Update) Executive Summary. Otolaryngol. Neck Surg. 2019, 161, 195–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, T.H.; Harris, J.P. Incidence of Sudden Sensorineural Hearing Loss. Otol. Neurotol. 2013, 34, 1586–1589. [Google Scholar] [CrossRef] [PubMed]
- Chern, A.; Famuyide, A.O.; Moonis, G.; Lalwani, A.K. Bilateral Sudden Sensorineural Hearing Loss and Intralabyrinthine Hemorrhage in a Patient With COVID-19. Otol. Neurotol. 2021, 42, e10–e14. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19). Available online: https://covid19.who.int/ (accessed on 29 July 2022).
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683. [Google Scholar] [CrossRef] [Green Version]
- Almufarrij, I.; Uus, K.; Munro, K.J. Does coronavirus affect the audio-vestibular system? A rapid systematic review. Int. J. Audiol. 2020, 59, 487–491. [Google Scholar] [CrossRef]
- Koumpa, F.S.; Forde, C.T.; Manjaly, J.G. Sudden irreversible hearing loss post COVID-19. BMJ Case Rep. 2020, 13, e238419. [Google Scholar] [CrossRef]
- Sriwijitalai, W.; Wiwanitkit, V. Hearing loss and COVID-19: A note. Am. J. Otolaryngol. 2020, 41, 102473. [Google Scholar] [CrossRef]
- Viola, P.; Ralli, M.; Pisani, D.; Malanga, D.; Sculco, D.; Messina, L.; Laria, C.; Aragona, T.; Leopardi, G.; Ursini, F.; et al. Tinnitus and equilibrium disorders in COVID-19 patients: Preliminary results. Eur. Arch. Otorhinolaryngol. 2021, 278, 3725–3730. [Google Scholar] [CrossRef]
- Mustafa, M.W.M. Audiological profile of asymptomatic COVID-19 PCR-positive cases. Am. J. Otolaryngol. 2020, 41, 102483. [Google Scholar] [CrossRef]
- Frazier, K.M.; Hooper, J.E.; Mostafa, H.H.; Stewart, C.M. SARS-CoV-2 Virus Isolated From the Mastoid and Middle Ear: Implications for COVID-19 Precautions During Ear Surgery. JAMA Otolaryngol. Neck Surg. 2020, 146, 964. [Google Scholar] [CrossRef]
- Ricciardiello, F.; Pisani, D.; Viola, P.; Cristiano, E.; Scarpa, A.; Giannone, A.; Longo, G.; Russo, G.; Bocchetti, M.; Coppola, C.; et al. Sudden Sensorineural Hearing Loss in Mild COVID-19: Case Series and Analysis of the Literature. Audiol. Res. 2021, 11, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Degen, C.; Lenarz, T.; Willenborg, K. Acute Profound Sensorineural Hearing Loss After COVID-19 Pneumonia. Mayo Clin. Proc. 2020, 95, 1801–1803. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Rocke, J.; France, K.; Izzat, S. Sudden sensorineural hearing loss in COVID-19: A case series from the Wrightington, Wigan and Leigh Teaching Hospitals, United Kingdom. Med. J. Malays. 2021, 76, 55–59. [Google Scholar]
- Chari, D.A.; Parikh, A.; Kozin, E.D.; Reed, M.; Jung, D.H. Impact of COVID-19 on Presentation of Sudden Sensorineural Hearing Loss at a Single Institution. Otolaryngol. Neck Surg. 2021, 165, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.H.; Young, Y.H. Evolution of incidence of audiovestibular disorders during the pandemic COVID-19 period. Eur. Arch. Otorhinolaryngol. 2022, 279, 3341–3345. [Google Scholar] [CrossRef]
- Parrino, D.; Frosolini, A.; Toninato, D.; Matarazzo, A.; Marioni, G.; de Filippis, C. Sudden hearing loss and vestibular disorders during and before COVID-19 pandemic: An audiology tertiary referral centre experience. Am. J. Otolaryngol. 2022, 43, 103241. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 29 July 2022).
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- The Jamovi Project (Version 2.3). Available online: https://www.jamovi.org (accessed on 29 July 2022).
- R Core Team: A Language and Environment for Statistical Computing. (Version 4.1). Available online: https://cran.r-project.org (accessed on 29 July 2022).
- Fidan, V.; Akin, O.; Koyuncu, H. Rised sudden sensorineural hearing loss during COVID-19 widespread. Am. J. Otolaryngol. 2021, 42, 102996. [Google Scholar] [CrossRef]
- Tsuda, T.; Hanada, Y.; Wada, K.; Fujiwara, E.; Takeda, K.; Nishimura, H. Efficacy of Intratympanic Glucocorticoid Steroid Administration Therapy as an Initial Treatment for Idiopathic Sudden Sensorineural Hearing Loss During the COVID-19 Pandemic. Ear Nose Throat J. 2021, 1455613211032534. [Google Scholar] [CrossRef]
- Yaseen, N.K.; Al-Ani, R.M.; Ali Rashid, R. COVID-19-related sudden sensorineural hearing loss. Qatar Med. J. 2021, 2021, 58. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Fan, K.; Tan, S.; Liu, S.; Wang, Y.; Yu, S. Analysis of the characteristics of outpatient and emergency diseases in the department of otolaryngology during the “COVID-19” pandemic. Sci. Prog. 2021, 104, 003685042110363. [Google Scholar] [CrossRef] [PubMed]
- Aslan, M.; Çiçek, M.T. Can isolated sudden sensorineural hearing loss (SSNHL) and idiopathic acute facial paralysis (Bell’s palsy) be symptoms of COVID-19? Am. J. Otolaryngol. 2021, 42, 103129. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.K.; Das, S.; Lenka, S. Sudden Sensorineural Hearing Loss among COVID-19 Patients-Our Experiences at an Indian Teaching Hospital. Siriraj Med. J. 2021, 72, 77–83. [Google Scholar] [CrossRef]
- Cohen, B.E.; Durstenfeld, A.; Roehm, P.C. Viral Causes of Hearing Loss: A Review for Hearing Health Professionals. Trends Hear 2014, 18, 233121651454136. [Google Scholar] [CrossRef]
- Schraff, S.A.; Schleiss, M.R.; Brown, D.K.; Meinzen-Derr, J.; Choi, K.Y.; Greinwald, J.H.; Choo, D.I. Macrophage inflammatory proteins in cytomegalovirus-related inner ear injury. Otolaryngol. Neck Surg. 2007, 137, 612–618. [Google Scholar] [CrossRef]
- Lindsay, J.R.; Davey, P.R.; Ward, P.H. LXVII Inner Ear Pathology in Deafness Due to Mumps. Ann. Otol. Rhinol. Laryngol. 1960, 69, 918–935. [Google Scholar] [CrossRef]
- Töndury, G.; Smith, D.W. Fetal rubella pathology. J. Pediatr. 1966, 68, 867–879. [Google Scholar] [CrossRef]
- Sweeney, C.J. NOSOLOGICAL ENTITIES?: Ramsay Hunt syndrome. J. Neurol. Neurosurg. Psychiatry 2001, 71, 149–154. [Google Scholar] [CrossRef]
- Parrino, D.; Brescia, G.; Trimarchi, M.V.; Tealdo, G.; Sasset, L.; Cattelan, A.M.; Bovo, R.; Marioni, G. Cochlear-Vestibular Impairment due to West Nile Virus Infection. Ann. Otol. Rhinol. Laryngol. 2019, 128, 1198–1202. [Google Scholar] [CrossRef]
- Krajewska, J.; Krajewski, W.; Zub, K.; Zatoński, T. COVID-19 in otolaryngologist practice: A review of current knowledge. Eur. Arch. Otorhinolaryngol. 2020, 277, 1885–1897. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Galougahi, M.; Naeini, A.S.; Raad, N.; Mikaniki, N.; Ghorbani, J. Vertigo and hearing loss during the COVID-19 pandemic—Is there an association? Acta Otorhinolaryngol. Ital. 2020, 40, 463–465. [Google Scholar] [CrossRef] [PubMed]
- Chirakkal, P.; Al Hail, A.N.; Zada, N.; Vijayakumar, D.S. COVID-19 and Tinnitus. Ear Nose Throat J. 2021, 100, 160S–162S. [Google Scholar] [CrossRef] [PubMed]
- Almufarrij, I.; Munro, K.J. One year on: An updated systematic review of SARS-CoV-2, COVID-19 and audio-vestibular symptoms. Int. J. Audiol. 2021, 60, 935–945. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, S.; Bello Alvarez, M.; Mungul, S.; Hari, K. Otologic dysfunction in patients with COVID-19: A systematic review. Laryngoscope Investig. Otolaryngol. 2020, 5, 1192–1196. [Google Scholar] [CrossRef]
- Jafari, Z.; Kolb, B.E.; Mohajerani, M.H. Hearing Loss, Tinnitus, and Dizziness in COVID-19: A Systematic Review and Meta-Analysis. Can. J. Neurol. Sci. 2022, 49, 184–195. [Google Scholar] [CrossRef]
- Uranaka, T.; Kashio, A.; Ueha, R.; Sato, T.; Bing, H.; Ying, G.; Kinoshita, M.; Kondo, K.; Yamasoba, T. Expression of Ace2, Tmprss2, and Furin in mouse ear tissue. Laryngoscope 2021, 131, E2013–E2017. [Google Scholar] [CrossRef]
- Tan, W.J. Noise-induced cochlear inflammation. World J. Otorhinolaryngol. 2013, 3, 89. [Google Scholar] [CrossRef]
- Vallamkondu, J.; John, A.; Wani, W.Y.; Ramadevi, S.P.; Jella, K.K.; Reddy, P.H.; Kandimalla, R. SARS-CoV-2 pathophysiology and assessment of coronaviruses in CNS diseases with a focus on therapeutic targets. Biochim. Biophys. Acta BBA-Mol. Basis Dis. 2020, 1866, 165889. [Google Scholar] [CrossRef]
- Karia, R.; Nagraj, S.; Gupta, I.; Barua, A.; Kaur, N.; Singh, H. Hydroxychloroquine: A review of its safety and efficacy in COVID-19. J. Fam. Med. Prim. Care 2021, 10, 1124. [Google Scholar] [CrossRef]
- Saunders, G.H.; Beukes, E.; Uus, K.; Armitage, C.J.; Kelly, J.; Munro, K.J. Shedding Light on SARS-CoV-2, COVID-19, COVID-19 Vaccination, and Auditory Symptoms: Causality or Spurious Conjunction? Front. Public Health 2022, 10, 837513. [Google Scholar] [CrossRef] [PubMed]
- Riccaboni, M.; Verginer, L.; Naudet, F. The impact of the COVID-19 pandemic on scientific research in the life sciences. PLoS ONE 2022, 17, e0263001. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, K.M.; Favre, N.M.; Kuo, C.C.; Carr, M.M. Systematic Review of Sensorineural Hearing Loss Associated With COVID-19 Infection. Cureus 2021, 13, e19757. [Google Scholar] [CrossRef] [PubMed]
- Umashankar, A.; Prakash, P.; Prabhu, P. Sudden Sensorineural Hearing Loss Post Coronavirus Disease: A Systematic Review of Case Reports. Indian J. Otolaryngol. Head Neck Surg. 2021, 74 (Suppl. S2), 1–8. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Wang, J.; Sun, J.; Zhu, K. COVID-19 and Sudden Sensorineural Hearing Loss: A Systematic Review. Front. Neurol. 2022, 13, 883749. [Google Scholar] [CrossRef]
- Shadbolt, N.; Brett, A.; Chen, M.; Marion, G.; McKendrick, I.J.; Panovska-Griffiths, J.; Pellis, L.; Reeve, R.; Swallow, B. The challenges of data in future pandemics. Epidemics 2022, 40, 100612. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author; Year | Study Type | Country | PYP Pre-PYP (Month/Year) | Purpose | Results | PYP Visits | PYP N SSNHL Cases (Incidence) | Pre-PYP N Visits | Pre-PYP N SSNHL (Incidence) | Quality [19] |
|---|---|---|---|---|---|---|---|---|---|---|
| Parrino et al. [17]; 2022 | ORS | Italy | 03/20–02/21 03/19–02/20 | To assess the impact of COVID-19 on SSNHL and vestibular disorders. | SSNHL during the pandemic seemed worse in terms of PTA with a higher incidence of associated vestibular involvement. | 2761 | 34 (1.23%) | 3446 | 27 (0.78%) | Good |
| Fidan et al. [23]; 2021 | ORS | Turkey | 04/20–09/20 04/19–09/19 | To measure the incidence of SSNHL presenting at a clinic during the pandemic and pre-pandemic period. | Increased incidence of SSNHL during the COVID-19 widespread compared to the same interval of the prior year. | NR | 68 (8.5/100’000) | NR | 41 (5.2/100’000) | Fair |
| Aslan et al. [27]; 2021 | OPS | Turkey | 04/20–04/21 01/19–01/20 | To evaluate the relationship of SSNHL and Bell’s palsy in COVID-19 patients. | No relationship between COVID-19 and cases of SSNHL and Bell’s palsy was observed. | NR | 42 | NR | 49 | Fair |
| Tsuda et al. [24]; 2021 | ORCCS | Japan | 04/20–03/20 NR | To compare the efficacy of ITS and IVS therapy as initial treatment for SSNHL during the COVID-19 pandemic. | ITS administration can be considered as the first line of treatment for SSNHL in the context of widespread COVID-19. | NR | 68 | NR | NR | Fair |
| Yaseen et al. [25]; 2021 | ORS | Iraq | 12/20–06/21 NR | To assess the demographic, clinical, and treatment outcomes of SSNHL in COVID-19 subjects. | Majority of COVID-19-related SSNHL cases presented within 1 week of onset, with bilateral outnumbering unilateral cases. Tinnitus was the most common associated symptom. Steroid treatment achieved improvement in 50% of the cases. | NR | 26 | NR | NR | Fair |
| Swain et al. [28]; 2021 | OPS | India | 03/20–08/20 NR | To investigate the incidence of SSNHL in COVID-19 patients. | Patients with COVID-19 infections have a chance of hearing loss. | NR | 16 | NR | NR | Poor |
| Jin et al. [26]; 2021 | ORS | China | 02/20–04/20 2017–2020 | To evaluate the impact of COVID-19 on ENT diseases. | COVID-19 may cause tinnitus or sudden deafness for people with or without vascular disease. | NR | 73 | NR | 140 | Fair |
| Author; Year | Mean Age ± Standard Deviation at Onset (Years) | Sex (M/F, No. Cases) | Associated Symptoms (No. Cases) | Mean PTA (dB) ± Standard Deviation | PYP Treatment (No. Cases) | Mean PTA (dB) ± Standard Deviation after Treatment | Recovery/No Recovery (No. Cases) | MRI Findings (No. Cases) | No. Cases SARS-CoV-2 +/Total |
|---|---|---|---|---|---|---|---|---|---|
| Parrino et al. [17]; 2022 | 56.2 ± 18.5 | 22/20 | D (15) | 61.2 ± 24.4 | OS (27); IVS (10); OS + ITS (1) | 50.4 ± 25.6 | 22/12 | NR | 2/5 |
| Fidan et al. [23]; 2021 | 51.7 ± 18.6 | 37/31 | NR | NR | OS | NR | NR | NR | 39/68 |
| Aslan et al. [27]; 2021 | 45.95 ± 15.61 | 29/13 | NR | NR | NR | NR | 22/20 | NR | 0/42 |
| Tsuda et al. [24]; 2021 | 62.18 ± 15.06 | 34/34 | D (11) | 68.77 ± 23.32 | IVS (46); ITS (22); HOT (salvage therapy) (7) | NR | NR | NR | NR |
| Yaseen et al. [25]; 2021 | 39.23 ± 11.88 | 6/20 | D (11); T (25) | 50.91 ± 11.78 | OS; OS + ITS | 40.24 ± 15.69 | 21/4 | No abnormalities | 26/26 * |
| Swain et al. [28]; 2021 | 48.42 ± NR | 11/5 | D (3); T (5) | NR | OS | NR | 9/7 | Cochlear enhancement (10/16) | 16/16 * |
| Jin et al. [26]; 2021 | 58 ± 14.18 | 42/31 | NR | NR | NR | NR | NR | NR | NR |
| Author; Year | Mean Age ± Standard Deviation at Onset (Years) | Sex (M/F, No. Cases) | Associated Symptoms (No. Cases) | Mean PTA (dB) ± Standard Deviation | Treatment (No. Cases) | Mean PTA (dB) ± Standard Deviation after Treatment | Recovery/No Recovery (No. Cases) |
|---|---|---|---|---|---|---|---|
| Parrino et al. [17]; 2022 | 55.8 ± 14.2 | 29/16 | 10 V (10) | 51.9 ± 28.4 | IVS (18); OS (21); OS + ITS (3) | 43.1 ± 26.4 | 19/8 |
| Fidan et al. [23]; 2021 | 67.2 ± 16.9 | 22/19 | NR | NR | OS | NR | NR |
| Aslan et al. [27]; 2021 | 50.73 ± 17.41 | 32/17 | NR | NR | NR | NR | 25/24 |
| Jin et al. [26]; 2021 | 58.75 ± 14.53 | 73/67 | NR | NR | NR | NR | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frosolini, A.; Franz, L.; Daloiso, A.; de Filippis, C.; Marioni, G. Sudden Sensorineural Hearing Loss in the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 3139. https://doi.org/10.3390/diagnostics12123139
Frosolini A, Franz L, Daloiso A, de Filippis C, Marioni G. Sudden Sensorineural Hearing Loss in the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(12):3139. https://doi.org/10.3390/diagnostics12123139
Chicago/Turabian StyleFrosolini, Andrea, Leonardo Franz, Antonio Daloiso, Cosimo de Filippis, and Gino Marioni. 2022. "Sudden Sensorineural Hearing Loss in the COVID-19 Pandemic: A Systematic Review and Meta-Analysis" Diagnostics 12, no. 12: 3139. https://doi.org/10.3390/diagnostics12123139
APA StyleFrosolini, A., Franz, L., Daloiso, A., de Filippis, C., & Marioni, G. (2022). Sudden Sensorineural Hearing Loss in the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Diagnostics, 12(12), 3139. https://doi.org/10.3390/diagnostics12123139