

Predicting Progression of Kidney Injury Based on Elastography Ultrasound and Radiomics Signatures
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
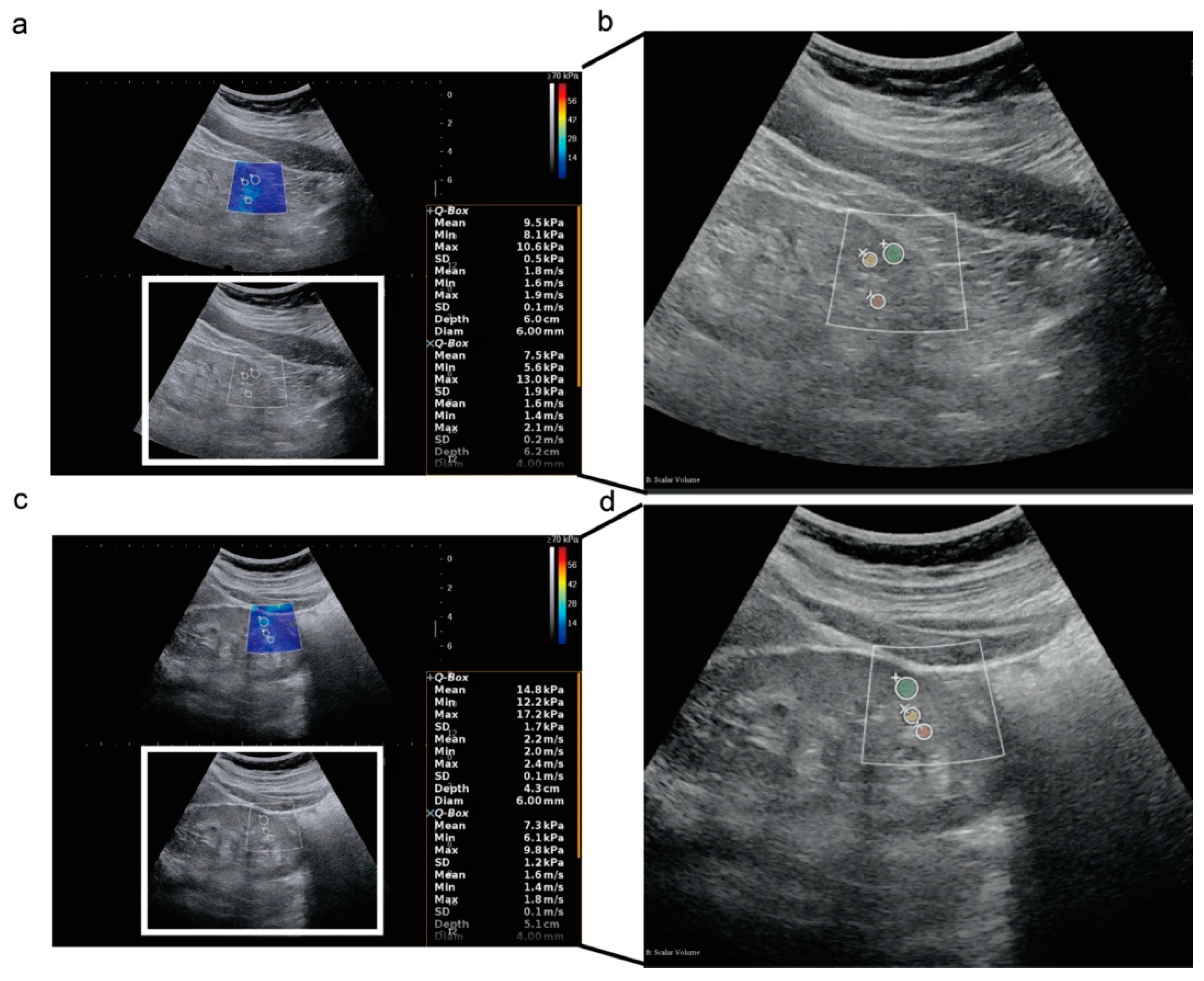
2.2. Clinical, Pathological, and Ultrasound Index
2.3. Radiomics Signature Extraction from Ultrasound
2.4. Cox Regression, Machine Learning, and Deep Learning Modeling
2.5. Statistical Analysis
3. Results
3.1. Baseline of the Study Population
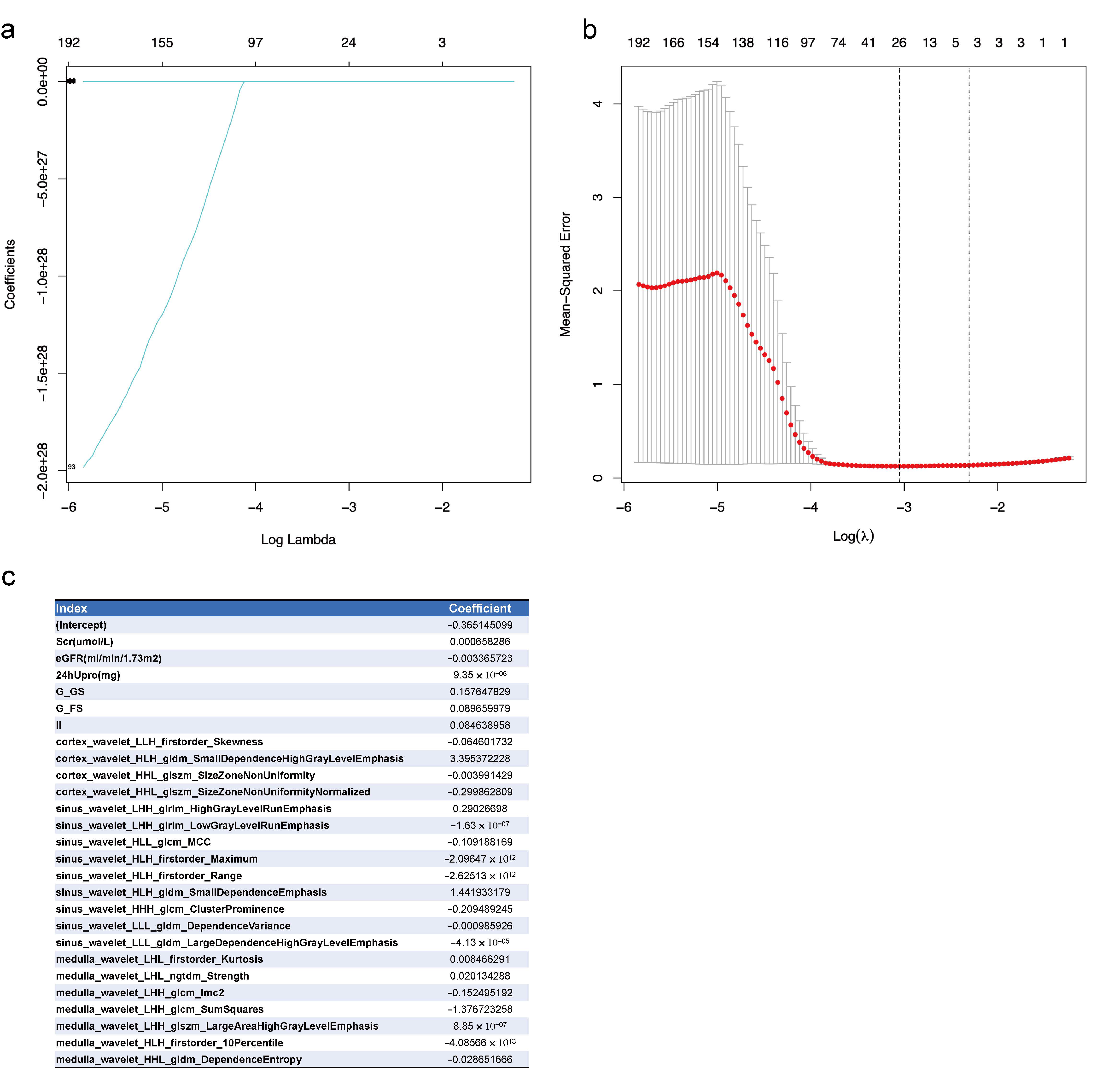
3.2. Feature Selections for CKD Prognosis by Lasso Regression
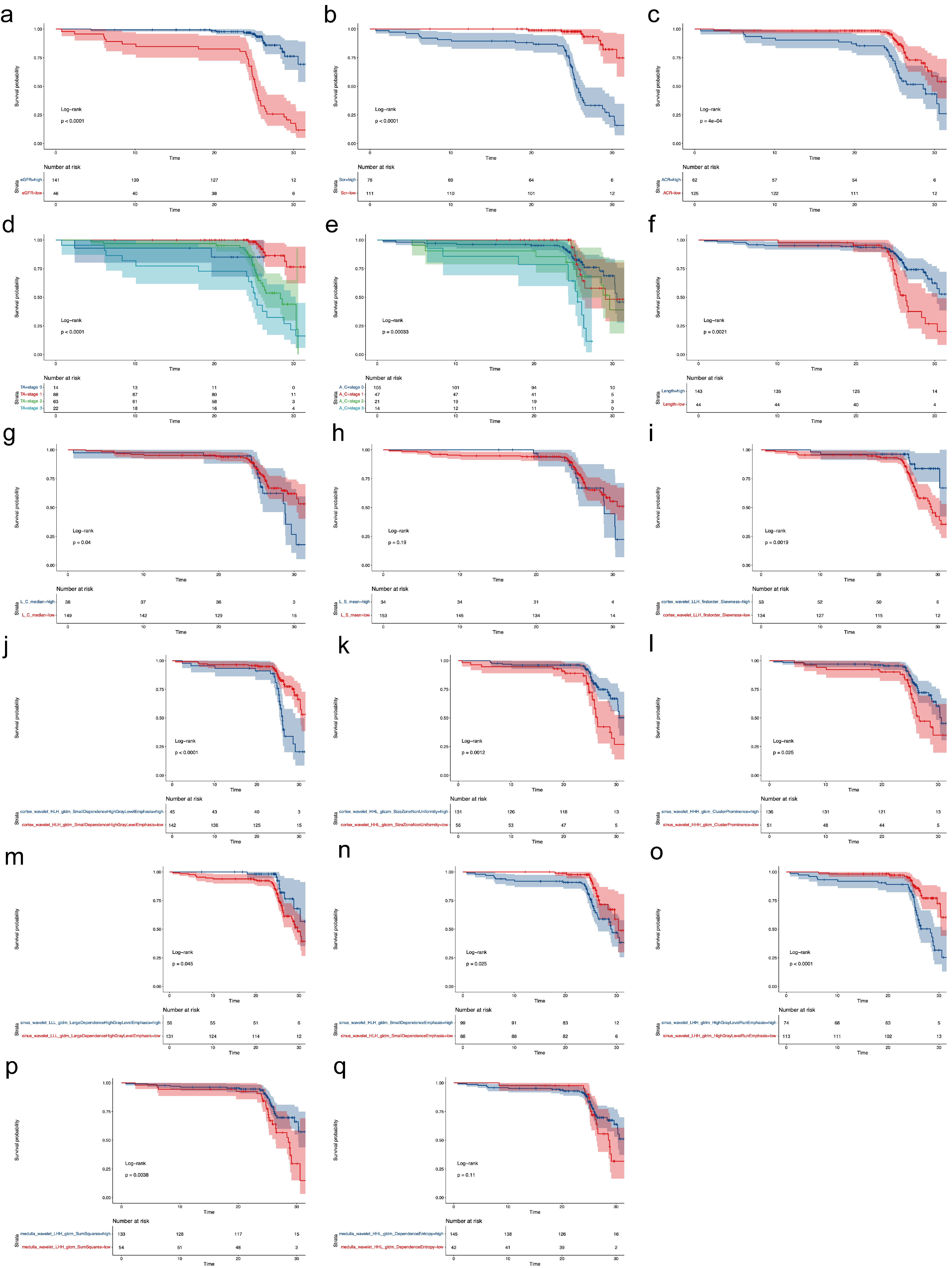
3.3. Cox regression for CKD Prognosis
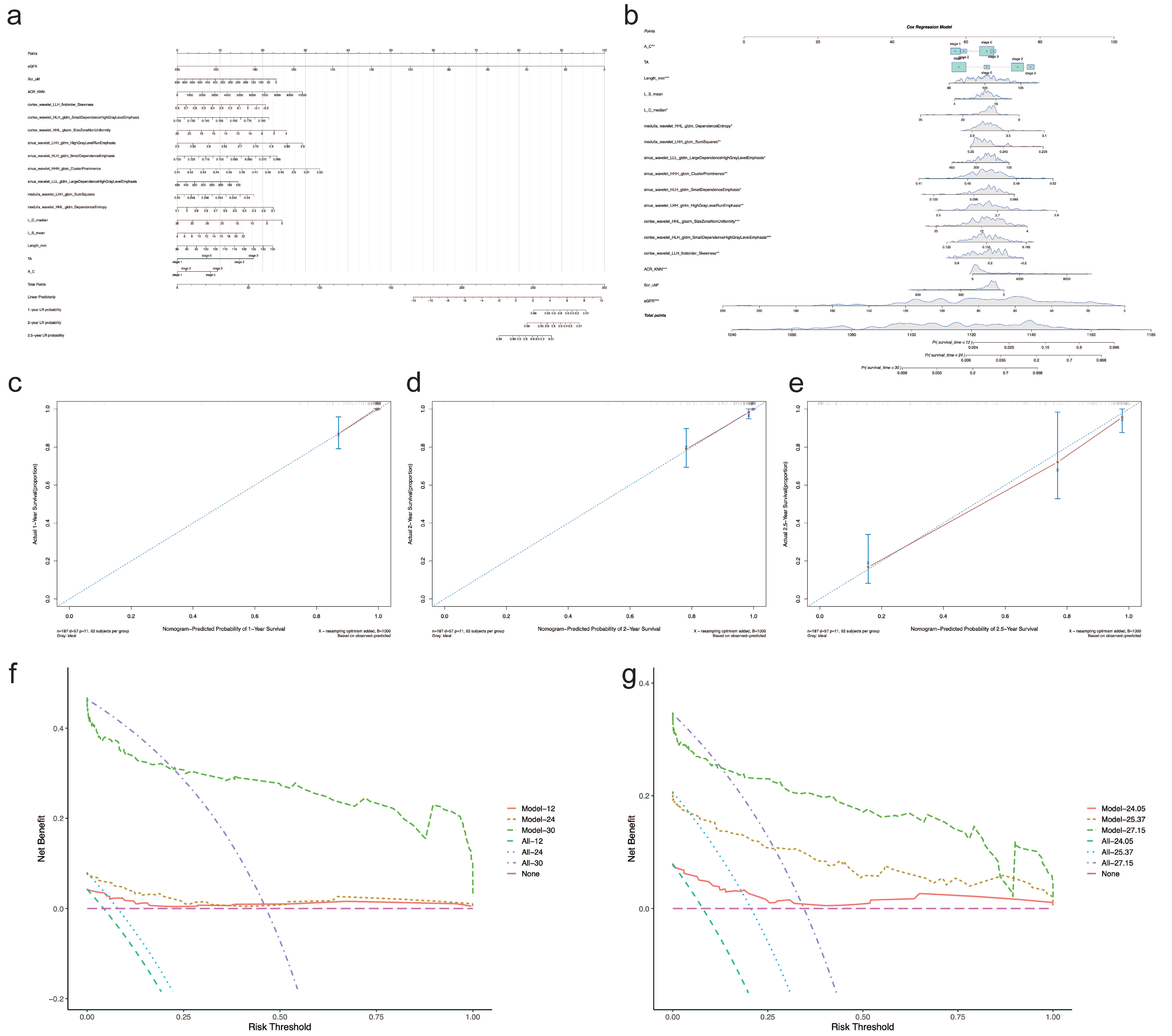
3.4. Nomogram for CKD Prognosis
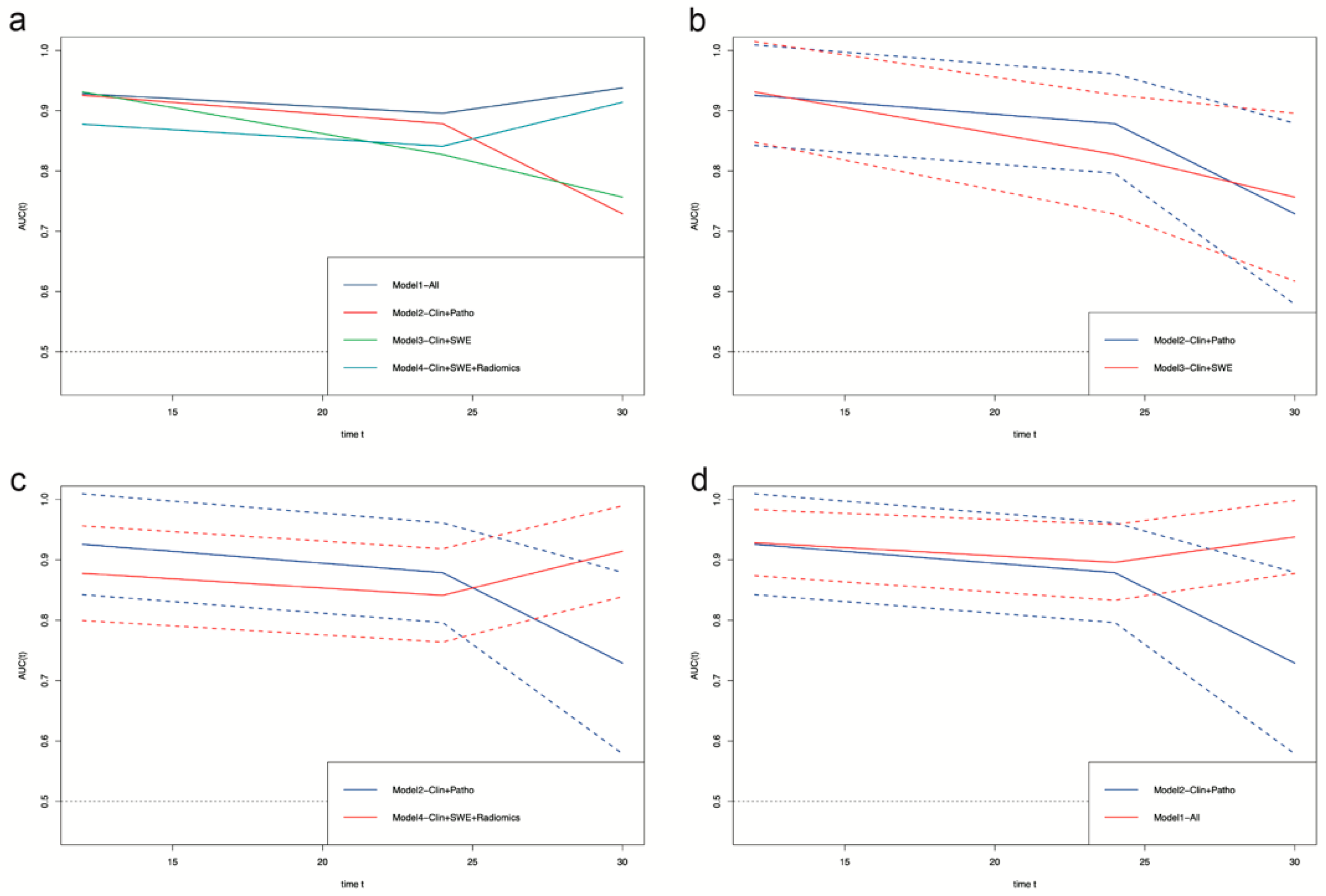
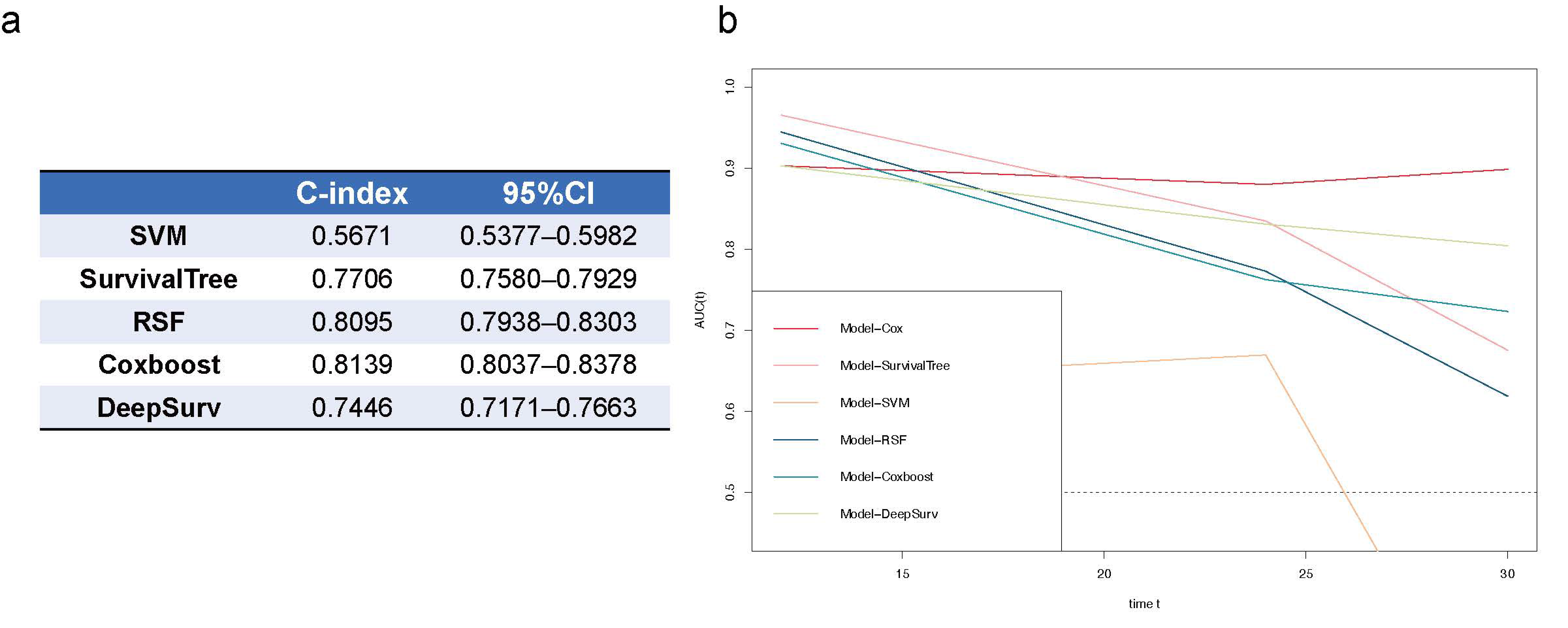
3.5. Predicting Models for CKD Prognosis Using Machine Learning and Deep Learning
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collaboration GBDCKD. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Elshahat, S.; Cockwell, P.; Maxwell, A.P.; Griffin, M.; O’Brien, T.; O’Neill, C. The impact of chronic kidney disease on developed countries from a health economics perspective: A systematic scoping review. PLoS ONE 2020, 15, e0230512. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ortega, M.; Rayego-Mateos, S.; Lamas, S.; Ortiz, A.; Rodrigues-Diez, R.R. Targeting the progression of chronic kidney disease. Nat. Rev. Nephrol. 2020, 16, 269–288. [Google Scholar] [CrossRef] [PubMed]
- Beenken, A.; Barasch, J.M.; Gharavi, A.G. Not all proteinuria is created equal. J. Clin. Investig. 2020, 130, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Bedin, M.; Boyer, O.; Servais, A.; Li, Y.; Villoing-Gaudé, L.; Tête, M.J.; Cambier, A.; Hogan, J.; Baudouin, V.; Krid, S.; et al. Human C-terminal CUBN variants associate with chronic proteinuria and normal renal function. J. Clin. Investig. 2020, 130, 335–344. [Google Scholar] [CrossRef]
- Singla, R.K.; Kadatz, M.; Rohling, R.; Nguan, C. Kidney Ultrasound for Nephrologists: A Review. Kidney Med. 2022, 4, 100464. [Google Scholar] [CrossRef]
- Yoon, H.; Lee, Y.S.; Lim, B.J.; Han, K.; Shin, H.J.; Kim, M.J.; Lee, M.J. Renal elasticity and perfusion changes associated with fibrosis on ultrasonography in a rabbit model of obstructive uropathy. Eur. Radiol. 2020, 30, 1986–1996. [Google Scholar] [CrossRef]
- Leong, S.S.; Wong, J.H.D.; Md Shah, M.N.; Vijayananthan, A.; Jalalonmuhali, M.; Chow, T.K.; Sharif, N.H.M.; Ng, K.H. Shear wave elastography accurately detects chronic changes in renal histopathology. Nephrology 2021, 26, 38–45. [Google Scholar] [CrossRef]
- Shiina, T.; Nightingale, K.R.; Palmeri, M.L.; Hall, T.J.; Bamber, J.C.; Barr, R.G.; Castera, L.; Choi, B.I.; Chou, Y.H.; Cosgrove, D.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: Basic principles and terminology. Ultrasound Med. Biol. 2015, 41, 1126–1147. [Google Scholar] [CrossRef]
- Maksuti, E.; Bini, F.; Fiorentini, S.; Blasi, G.; Urban, M.W.; Marinozzi, F.; Larsson, M. Influence of wall thickness and diameter on arterial shear wave elastography: A phantom and finite element study. Phys. Med. Biol. 2017, 62, 2694–2718. [Google Scholar] [CrossRef]
- Lim, W.T.H.; Ooi, E.H.; Foo, J.J.; Foo, J.J.; Ng, K.H.; Wong, J.; Leong, S.S. Shear Wave Elastography: A Review on the Confounding Factors and Their Potential Mitigation in Detecting Chronic Kidney Disease. Ultrasound Med. Biol. 2021, 47, 2033–2047. [Google Scholar] [CrossRef]
- Alnazer, I.; Bourdon, P.; Urruty, T.; Falou, O.; Khalil, M.; Shahin, A.; Fernandez-Maloigne, C. Recent advances in medical image processing for the evaluation of chronic kidney disease. Med. Image Anal. 2021, 69, 101960. [Google Scholar] [CrossRef]
- Kagiyama, N.; Shrestha, S.; Cho, J.S.; Khalil, M.; Singh, Y.; Challa, A.; Casaclang-Verzosa, G.; Sengupta, P.P. A low-cost texture-based pipeline for predicting myocardial tissue remodeling and fibrosis using cardiac ultrasound. EBioMedicine 2020, 54, 102726. [Google Scholar] [CrossRef]
- Li, W.; Huang, Y.; Zhuang, B.W.; Liu, G.J.; Hu, H.T.; Li, X.; Liang, J.Y.; Wang, Z.; Huang, X.W.; Zhang, C.Q.; et al. Multiparametric ultrasomics of significant liver fibrosis: A machine learning-based analysis. Eur. Radiol. 2019, 29, 1496–1506. [Google Scholar] [CrossRef]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Dahly, D.L.; Damen, J.A.A.; Debray, T.P.A.; et al. Prediction models for diagnosis and prognosis of COVID-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef]
- Li, M.D.; Cheng, M.Q.; Chen, L.D.; Hu, H.T.; Zhang, J.C.; Ruan, S.M.; Huang, H.; Kuang, M.; Lu, M.D.; Li, W.; et al. Reproducibility of radiomics features from ultrasound images: Influence of image acquisition and processing. Eur. Radiol. 2022, 32, 5843–5851. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef]
- Van Belle, V.; Pelckmans, K.; Van Huffel, S.; Suykens, J.A. Improved performance on high-dimensional survival data by application of Survival-SVM. Bioinformatics 2011, 27, 87–94. [Google Scholar] [CrossRef]
- Berrar, D.; Sturgeon, B.; Bradbury, I.; Downes, C.S.; Dubitzky, W. Survival trees for analyzing clinical outcome in lung adenocarcinomas based on gene expression profiles: Identification of neogenin and diacylglycerol kinase alpha expression as critical factors. J. Comput. Biol. 2005, 12, 534–544. [Google Scholar] [CrossRef]
- Mogensen, U.B.; Ishwaran, H.; Gerds, T.A. Evaluating Random Forests for Survival Analysis using Prediction Error Curves. J. Stat. Softw. 2012, 50, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Binder, H.; Allignol, A.; Schumacher, M.; Beyersmann, J. Boosting for high-dimensional time-to-event data with competing risks. Bioinformatics 2009, 25, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Jiang, T.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med. Res. Methodol. 2018, 18, 24. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; et al. National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef]
- Anonymous. Summary of Recommendation Statements. Kidney Int. Suppl. 2013, 3, 5–14. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Marsh, J.; Stevens, L.A.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Expressing the Modification of Diet in Renal Disease Study equation for estimating glomerular filtration rate with standardized serum creatinine values. Clin. Chem. 2007, 53, 766–772. [Google Scholar] [CrossRef]
- Hansen, K.L.; Nielsen, M.B.; Ewertsen, C. Ultrasonography of the Kidney: A Pictorial Review. Diagnostics 2015, 6, 2. [Google Scholar] [CrossRef]
- Sethi, S.; D’Agati, V.D.; Nast, C.C.; Fogo, A.B.; De Vriese, A.S.; Markowitz, G.S.; Glassock, R.J.; Fervenza, F.C.; Seshan, S.V.; Rule, A.; et al. A proposal for standardized grading of chronic changes in native kidney biopsy specimens. Kidney Int. 2017, 91, 787–789. [Google Scholar] [CrossRef]
- Srivastava, A.; Palsson, R.; Kaze, A.D.; Chen, M.E.; Palacios, P.; Sabbisetti, V.; Betensky, R.A.; Steinman, T.I.; Thadhani, R.I.; McMahon, G.M.; et al. The Prognostic Value of Histopathologic Lesions in Native Kidney Biopsy Specimens: Results from the Boston Kidney Biopsy Cohort Study. J. Am. Soc. Nephrol. 2018, 29, 2213–2224. [Google Scholar] [CrossRef]
- Liu, P.; Quinn, R.R.; Lam, N.N.; Al-Wahsh, H.; Sood, M.M.; Tangri, N.; Tonelli, M.; Ravani, P. Progression and Regression of Chronic Kidney Disease by Age Among Adults in a Population-Based Cohort in Alberta, Canada. JAMA Netw. Open 2021, 4, e2112828. [Google Scholar] [CrossRef]
- Vatcheva, K.P.; Lee, M.; McCormick, J.B.; Vatcheva, K.P.; Lee, M.; McCormick, J.B.; Rahbar, M.H. Multicollinearity in Regression Analyses Conducted in Epidemiologic Studies. Epidemiology 2016, 6, 227. [Google Scholar] [CrossRef] [PubMed]
- Hocking, R.R. Methods and Applications of Linear Models, 3rd ed.; Wiley: New York, NY, USA, 2013; pp. 142–178. [Google Scholar]
- Liu, Q.; Wang, Z. Diagnostic value of real-time shear wave elastography in children with chronic kidney disease. Clin. Hemorheol. Microcirc. 2021, 77, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, P.; Bane, O.; Hectors, S.J.; Gordic, S.; Berger, M.; Delaney, V.; Salem, F.; Lewis, S.; Menon, M.; Taouli, B. Magnetic resonance elastography vs. point shear wave ultrasound elastography for the assessment of renal allograft dysfunction. Eur. J. Radiol. 2020, 126, 108949. [Google Scholar] [CrossRef] [PubMed]
- Radulescu, D.; Peride, I.; Petcu, L.C.; Niculae, A.; Checherita, I.A. Supersonic Shear Wave Ultrasonography for Assessing Tissue Stiffness in Native Kidney. Ultrasound Med. Biol. 2018, 44, 2556–2568. [Google Scholar] [CrossRef]
- Amador, C.; Urban, M.W.; Chen, S.; Chen, Q.; An, K.N.; Greenleaf, J.F. Shear elastic modulus estimation from indentation and SDUV on gelatin phantoms. IEEE Trans Biomed. Eng. 2011, 58, 1706–1714. [Google Scholar] [CrossRef]
- Amador, C.; Urban, M.; Kinnick, R.; Chen, S.; Greenleaf, J.F. In vivo swine kidney viscoelasticity during acute gradual decrease in renal blood flow: Pilot study. Rev. Ing Biomed. 2013, 7, 68–78. [Google Scholar]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Yoshimasu, Y.; Kasai, Y.; Furuichi, Y.; Itoi, T. Viscoelasticity Measurement in Rat Livers Using Shear-Wave US Elastography. Ultrasound Med. Biol. 2018, 44, 2018–2024. [Google Scholar] [CrossRef]
- Gennisson, J.L.; Grenier, N.; Combe, C.; Tanter, M. Supersonic shear wave elastography of in vivo pig kidney: Influence of blood pressure, urinary pressure and tissue anisotropy. Ultrasound Med. Biol. 2012, 38, 1559–1567. [Google Scholar] [CrossRef]
- Humphreys, B.D. Mechanisms of Renal Fibrosis. Annu. Rev. Physiol. 2018, 80, 309–326. [Google Scholar] [CrossRef]
- Kattan, M.W. Comparison of Cox regression with other methods for determining prediction models and nomograms. J. Urol. 2003, 170, S6–S9, discussion S10. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 187) | CKD fo_1~2 (n = 130) | CKD fo_3~5 (n = 57) | p Value | |
| Age(year) | 45.00 (32.00–59.00) | 40.00 (30.00–40.00) | 52.00 (38.50–52.00) | <0.001 |
| Sex (male%) | 105 (56.1%) | 67 (63.80%) | 38 (36.20%) | 0.055 |
| BMI (kg/m2) | 24.30 (21.96–27.16) | 24.19 (21.98–24.19) | 24.80 (21.80–24.80) | 0.426 |
| SBP (mmHg) | 141.00 (121.00–165.00) | 135.50 (119.00–135.50) | 157.00 (128.00–157.00) | 0.003 |
| DBP (mmHg) | 77.50 (70.00–85.75) | 77.50 (67.75–77.50) | 77.00 (72.00–77.00) | 0.362 |
| eGFR (MDRD) (mL/min/1.73 m2) | 73.35 (51.96–101.88) | 86.55 (69.04–86.55) | 39.01 (24.94–39.01) | <0.001 |
| Scr (μmol/L) | 92.00 (68.00–131.00) | 81.00 (62.00–81.00) | 165.00 (117.50–165.00) | <0.001 |
| BUN (mmol/L) | 5.50 (4.23–7.38) | 4.70 (3.90–4.70) | 7.90 (5.80–7.90) | <0.001 |
| UA (μmol/L) | 363.50 (299.50–412.50) | 351.50 (281.25–351.50) | 389.00 (343.00–389.00) | 0.001 |
| Alb (g/L) | 35.60 (29.95–41.05) | 36.45 (29.11–36.45) | 35.00 (30.25–35.00) | 0.612 |
| 24hUpro (mg) | 1454.40 (624.60–3397.15) | 1119.15 (583.40–1119.15) | 2493.00 (1186.80–2493.00) | <0.001 |
| ACR (mg/g) | 565.95 (253.03–1788.85) | 421.85 (193.65–421.85) | 1084.40 (441.00–1084.40) | <0.001 |
| Pathological Changes | Total (n = 187) | CKD fo_1~2 (n = 130) | CKD fo_3~5 (n = 57) | p Value |
| G_G_Sclerosis (%) | 20.00% (5.88–43.75%) | 12.77% (0.00–28.57%) | 46.67% (25.83–62.02%) | <0.001 |
| G_FS_Sclerosis (%) | 0.00% (0.00–7.69%) | 0.00% (0.00–6.47%) | 3.23% (0.00–11.81%) | 0.042 |
| G_Crescents (%) | 0.00% (0.00–3.33%) | 0.00% (0.0–3.54%) | 0.00% (0.00–4.41%) | 0.959 |
| G_Fibrinoid necrosis (%) | 0.00% (0.00–0.00%) | 0.00% (0.00%–0.00%) | 0.00% (0.00–0.00%) | 0.290 |
| Mesengial matrix hyperplasia | <0.001 | |||
| 0 | 17 (9.10%) | 10 (58.80%) | 7 (41.20%) | |
| 1 | 140 (74.90%) | 105 (75.00%) | 35 (25.00%) | |
| 2 | 20 (10.70%) | 14 (70.00%) | 6 (30.00%) | |
| 3 | 10 (5.30%) | 1 (10.00%) | 9 (90.00%) | |
| Mesangial hypercellularity | 0.096 | |||
| 0 | 30 (16.00%) | 19 (63.30%) | 11 (36.70%) | |
| 1 | 134 (71.70%) | 99 (73.90%) | 35 (26.10%) | |
| 2 | 22 (11.80%) | 12 (54.50%) | 10 (45.50%) | |
| 3 | 1 (0.50%) | 0 (0.00%) | 1 (100.00%) | |
| Intra–capillary proliferation | 0.069 | |||
| 0 | 144 (77.00%) | 102 (70.80%) | 42 (29.20%) | |
| 1 | 2 (1.10%) | 1 (50.00%) | 1 (50.00%) | |
| 2 | 41 (21.90%) | 27 (65.90%) | 14 (34.10%) | |
| 3 | 0 (0.00%) | 0 (0.00%) | 0 (0.00%) | |
| Capillary wall hyalinosis | 0.738 | |||
| 0 | 114 (61.00%) | 82 (71.90%) | 32 (28.10%) | |
| 1 | 49 (26.20%) | 31 (63.30%) | 18 (36.70%) | |
| 2 | 21 (11.20%) | 15 (71.40%) | 6 (28.60%) | |
| 3 | 3 (1.60%) | 2 (66.70%) | 1 (33.30%) | |
| Tubular atrophy | <0.001 | |||
| 0 | 14 (7.50%) | 12 (85.70%) | 2 (14.30%) | |
| 1 | 88 (47.10%) | 78 (88.60%) | 10 (11.40%) | |
| 2 | 63 (33.70%) | 37 (58.70%) | 26 (41.30%) | |
| 3 | 22 (11.80%) | 3 (13.60%) | 19 (86.40%) | |
| Interstitial inflammation | <0.001 | |||
| 0 | 14 (7.50%) | 13 (92.90%) | 1 (7.10%) | |
| 1 | 91 (48.70%) | 82 (90.10%) | 9 (9.90%) | |
| 2 | 60 (32.10%) | 33 (55.00%) | 27 (45.00%) | |
| 3 | 22 (11.80%) | 2 (9.10%) | 20 (90.90%) | |
| Interstitial fibrosis | <0.001 | |||
| 0 | 13 (7.00%) | 12 (92.30%) | 1 (7.70%) | |
| 1 | 92 (49.20%) | 81 (88.00%) | 11 (12.00%) | |
| 2 | 61 (32.60%) | 34 (55.70%) | 27 (44.30%) | |
| 3 | 21 (11.20%) | 3 (14.30%) | 18 (85.70%) | |
| Artery/arteriole intima thickening | 0.114 | |||
| 0 | 79 (42.20%) | 59 (74.70%) | 20 (25.30%) | |
| 1 | 39 (20.90%) | 30 (76.90%) | 9 (23.10%) | |
| 2 | 59 (31.60%) | 34 (57.60%) | 25 (42.40%) | |
| 3 | 10 (5.30%) | 7 (70.00%) | 3 (30.00%) | |
| Artery/arteriole hyalinosis | <0.001 | |||
| 0 | 105 (56.10%) | 81 (77.10%) | 24 (22.90%) | |
| 1 | 47 (25.10%) | 35 (74.50%) | 12 (25.50%) | |
| 2 | 21 (11.20%) | 10 (47.60%) | 11 (52.40%) | |
| 3 | 14 (7.50%) | 4 (28.60%) | 10 (71.40%) | |
| Grade of chronic changes | <0.001 | |||
| Minimal (0–1) | 10 (5.30%) | 10 (100.00%) | 0 (0.00%) | |
| Mild (2–4) | 66 (35.30%) | 59 (89.40%) | 7 (10.60%) | |
| Moderate (5–7) | 61 (32.60%) | 47 (77.00%) | 14 (23.00%) | |
| Severe (≥8) | 50 (26.70%) | 14 (28.00%) | 36 (72.00%) | |
| Ultrasound | Total (n = 187) | CKD fo_1~2 (n = 130) | CKD fo_3~5 (n = 57) | p Value |
| L_C_mean (kPa) | 10.60 (9.50–12.50) | 10.35 (9.30–11.95) | 10.80 (9.65–13.30) | 0.126 |
| L_C_median (kPa) | 10.60 (9.20–12.60) | 10.50 (9.18–12.10) | 10.80 (9.30–13.40) | 0.174 |
| L_M_mean (kPa) | 6.50 (5.50–8.20) | 6.45 (5.28–8.13) | 6.80 (5.70–8.70) | 0.128 |
| L_M_median (kPa) | 6.50 (5.30–8.40) | 6.35 (5.20–8.40) | 6.90 (5.80–8.75) | 0.124 |
| L_S_mean (kPa) | 13.40 (12.10–14.80) | 13.10 (11.90–14.58) | 13.80 (11.85–15.25) | 0.305 |
| L_S_median (kPa) | 13.40 (11.90–14.90) | 13.10 (11.70–14.60) | 13.90 (11.80–15.35) | 0.235 |
| Length (mm) | 106.00 (99.00–112.00) | 106.00 (101.00–112.25) | 103.00 (95.50–110.00) | 0.037 |
| Width (mm) | 45.00 (42.00–49.00) | 45.00 (42.00–48.00) | 45.00 (40.50–49.00) | 0.904 |
| Thickness (mm) | 43.40 (39.00–46.50) | 44.00 (40.30–47.00) | 42.00 (38.50–45.50) | 0.093 |
| Kidney volume (cm3) | 201.35 (173.04–238.66) | 205.95 (179.58–239.10) | 188.93 (158.01–237.50) | 0.159 |
| Parameters | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| HR (95%CI) | p Value | HR (95%CI) | p Value | ||
| Clinical Index | Age (year) | 0.953 (0.904–1.003) | 0.066 | ||
| SBP (mmHg) | 1.002 (0.995–1.009) | 0.613 | |||
| eGFR (mL/min/1.73 m2) | 0.865 (0.806–0.93) | <0.001 | 0.927 (0.9–0.955) | <0.001 | |
| Scr (μmol/L) | 0.978 (0.965–0.992) | 0.002 | 0.994 (0.989–0.999) | 0.013 | |
| BUN (mmol/L) | 1.195 (0.957–1.492) | 0.116 | |||
| UA (μmol/L) | 0.997 (0.987–1.006) | 0.504 | |||
| 24hUpro (mg) | 0.999998 (0.999767–1.000229) | 0.985 | |||
| ACR (mg/g) | 1.001 (1.001–1.002) | <0.001 | 1.000489 (1.000247–1.001) | <0.001 | |
| Pathological Changes | G_GS (%) | 7.53 (0.311–182.252) | 0.214 | ||
| G_FS (%) | 5.63 (0.152–209.022) | 0.349 | |||
| M_M (1) | 39.261 (1.175–1311.474) | 0.040 | |||
| M_M (2) | 0.669 (0.009–52.184) | 0.857 | |||
| M_M (3) | 6.067 (0.268–137.282) | 0.257 | |||
| TA (1) | 0.002 (0.000009–0.649) | 0.035 | 0.316 (0.038–2.602) | 0.284 | |
| TA (2) | 6.465 (0.018–2293.191) | 0.533 | 3.584 (0.435–29.553) | 0.236 | |
| TA (3) | 1.524 (0.000111–20913.596) | 0.931 | 6.173 (0.553–68.902) | 0.139 | |
| II (1) | 0.348 (2.614 × 10–27–4.638 × 1025) | 0.973 | |||
| II (2) | 15,636.424 (1.029 × 10–22–2.374 × 1030) | 0.754 | |||
| II (3) | 5.148 (2.995 × 10–26–8.847 × 1026) | 0.958 | |||
| IF (1) | 5677.54 (3.1539 × 10–23–1.022 × 1030) | 0.779 | |||
| IF (2) | 0.29 (1.641 × 10–27–5.126 × 1025) | 0.968 | |||
| IF (3) | 55,447.23 (2.382 × 10–22–1.290 × 1031) | 0.724 | |||
| A_C (1) | 0.092 (0.010–0.806) | 0.031 | 0.273 (0.109–0.682) | 0.005 | |
| A_C (2) | 0.122 (0.016–0.922) | 0.041 | 0.385 (0.122–1.217) | 0.104 | |
| A_C (3) | 7.482 (0.883–63.383) | 0.065 | 1.317 (0.464–3.741) | 0.605 | |
| Grade of chronic changes (1) | 17,027.838 (9.106 × 10–35–3.184 × 1042) | 0.828 | |||
| Grade of chronic changes (2) | 152.155 (8.861 × 10–37–2.613 × 1040) | 0.911 | |||
| Grade of chronic changes (3) | 6.777 (3.582 × 10–38–1.282 × 1039) | 0.966 | |||
| Ultrasound Parameters | L_C_mean (kPa) | 0.281 (0.073–1.08) | 0.065 | ||
| L_C_median (kPa) | 3.236 (0.945–11.076) | 0.061 | 0.890 (0.796–0.994) | 0.039 | |
| L_M_mean (kPa) | 1.457 (0.329–6.452) | 0.620 | |||
| L_M_median (kPa) | 0.569 (0.143–2.263) | 0.423 | |||
| L_S_mean (kPa) | 3.024 (0.875–10.449) | 0.080 | 1.154 (0.971–1.371) | 0.104 | |
| L_S_median (kPa) | 0.444 (0.159–1.243) | 0.122 | |||
| Length (mm) | 1.267 (1.117–1.437) | <0.001 | 1.077 (1.034–1.122) | <0.001 | |
| Kidney_volume (cm2) | 0.995 (0.977–1.014) | 0.625 | |||
| Ultrasound Radiomics | cortex_wavelet_LLH_firstorder_Skewness | 0.000363 (0.000002–0.056) | 0.002 | 0.032 (0.003–0.311) | 0.003 |
| cortex_wavelet_HLH_gldm_ SmallDependenceHighGrayLevelEmphasis | 2.005 × 1066 (1.482 × 1029–2.714 × 10103) | <0.001 | 7.876 × 1023 (1.672 × 1011–3.709 × 1036) | <0.001 | |
| cortex_wavelet_HHL_glszm_ SizeZoneNonUniformity | 0.704 (0.536–0.925) | 0.012 | 0.789 (0.691–0.902) | 0.001 | |
| cortex_wavelet_HHL_glszm_ SizeZoneNonUniformityNormalized | 1811.003 (0.000122–2.698 × 1010) | 0.373 | |||
| sinus_wavelet_LHH_glrlm_ HighGrayLevelRunEmphasis | 916,226,561.138 (300.893–2.790 × 1015) | 0.007 | 206,763.534 (38.345–1.115 × 1010) | 0.005 | |
| sinus_wavelet_LHH_glrlm_ LowGrayLevelRunEmphasis | a | ||||
| sinus_wavelet_HLL_glcm_MCC | 129.179 (0.002–7,675,218.559) | 0.386 | |||
| sinus_wavelet_HLH_gldm_ SmallDependenceEmphasis | 5.848 × 10–45 (7.627 × 10–77–4.483 × 10–13) | 0.007 | 7.163 × 10–25 (4.143 × 10–44–0.000012) | 0.014 | |
| sinus_wavelet_HHH_glcm_ClusterProminence | 1.774 × 1046 (9.389 × 1011–3.350 × 1080) | 0.008 | 9.179 × 1021 (55,633,770.994–1.514 × 1036) | 0.002 | |
| sinus_wavelet_LLL_gldm_ DependenceVariance | 0.773 (0.184–3.243) | 0.725 | |||
| sinus_wavelet_LLL_gldm_ LargeDependenceHighGrayLevelEmphasis | 0.985 (0.972–0.998) | 0.023 | 0.993 (0.987–0.999) | 0.022 | |
| medulla_wavelet_LHL_firstorder_Kurtosis | 1.800 (0.793–4.086) | 0.160 | |||
| medulla_wavelet_LHL_ngtdm_Strength | 1.685 (0.491–5.789) | 0.407 | |||
| medulla_wavelet_LHH_glcm_Imc2 | 5580.503 (0–3.695 × 1011) | 0.348 | |||
| medulla_wavelet_LHH_glcm_SumSquares | 0 (0–5.364 × 10–220) | <0.001 | 5.146 × 10–119 (2.670 × 10–202–9.917 × 10–36) | 0.005 | |
| medulla_wavelet_LHH_glszm_ LargeAreaHighGrayLevelEmphasis | 1.002 (0.999769–1.004) | 0.082 | |||
| medulla_wavelet_HHL_gldm_ DependenceEntropy | 0.001 (0.000003–0.615) | 0.034 | 0.024 (0.001–0.691) | 0.030 | |
| Cox Regression Model | L.R.Chisq | p-Value |
|---|---|---|
| Model-Clin + Patho vs. Model-Clin + SWE | 7.2347 | 0.1240 |
| Model-Clin + Patho vs. Model-Clin + SWE + Radiomics | 27.0800 | 0.0001 |
| Model-Clin + Patho vs. Model-All | 63.9548 | <0.0001 |
| Model-Clin + SWE + Radiomics vs. Model-All | 36.8748 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, M.; Tang, L.; Yang, W.; Xu, Y.; Che, X.; Zhou, Y.; Shao, X.; Zhou, W.; Zhang, M.; Li, G.; et al. Predicting Progression of Kidney Injury Based on Elastography Ultrasound and Radiomics Signatures. Diagnostics 2022, 12, 2678. https://doi.org/10.3390/diagnostics12112678
Zhu M, Tang L, Yang W, Xu Y, Che X, Zhou Y, Shao X, Zhou W, Zhang M, Li G, et al. Predicting Progression of Kidney Injury Based on Elastography Ultrasound and Radiomics Signatures. Diagnostics. 2022; 12(11):2678. https://doi.org/10.3390/diagnostics12112678
Chicago/Turabian StyleZhu, Minyan, Lumin Tang, Wenqi Yang, Yao Xu, Xiajing Che, Yin Zhou, Xinghua Shao, Wenyan Zhou, Minfang Zhang, Guanghan Li, and et al. 2022. "Predicting Progression of Kidney Injury Based on Elastography Ultrasound and Radiomics Signatures" Diagnostics 12, no. 11: 2678. https://doi.org/10.3390/diagnostics12112678
APA StyleZhu, M., Tang, L., Yang, W., Xu, Y., Che, X., Zhou, Y., Shao, X., Zhou, W., Zhang, M., Li, G., Zheng, M., Wang, Q., Li, H., & Mou, S. (2022). Predicting Progression of Kidney Injury Based on Elastography Ultrasound and Radiomics Signatures. Diagnostics, 12(11), 2678. https://doi.org/10.3390/diagnostics12112678