
Abdominal and Pelvic Floor Activity Related to Respiratory Diaphragmatic Activity in Subjects with and without Non-Specific Low Back Pain


 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Demographic Variables
2.2. Non-Specific Low Back Pain
2.3. Ultrasound Measurements
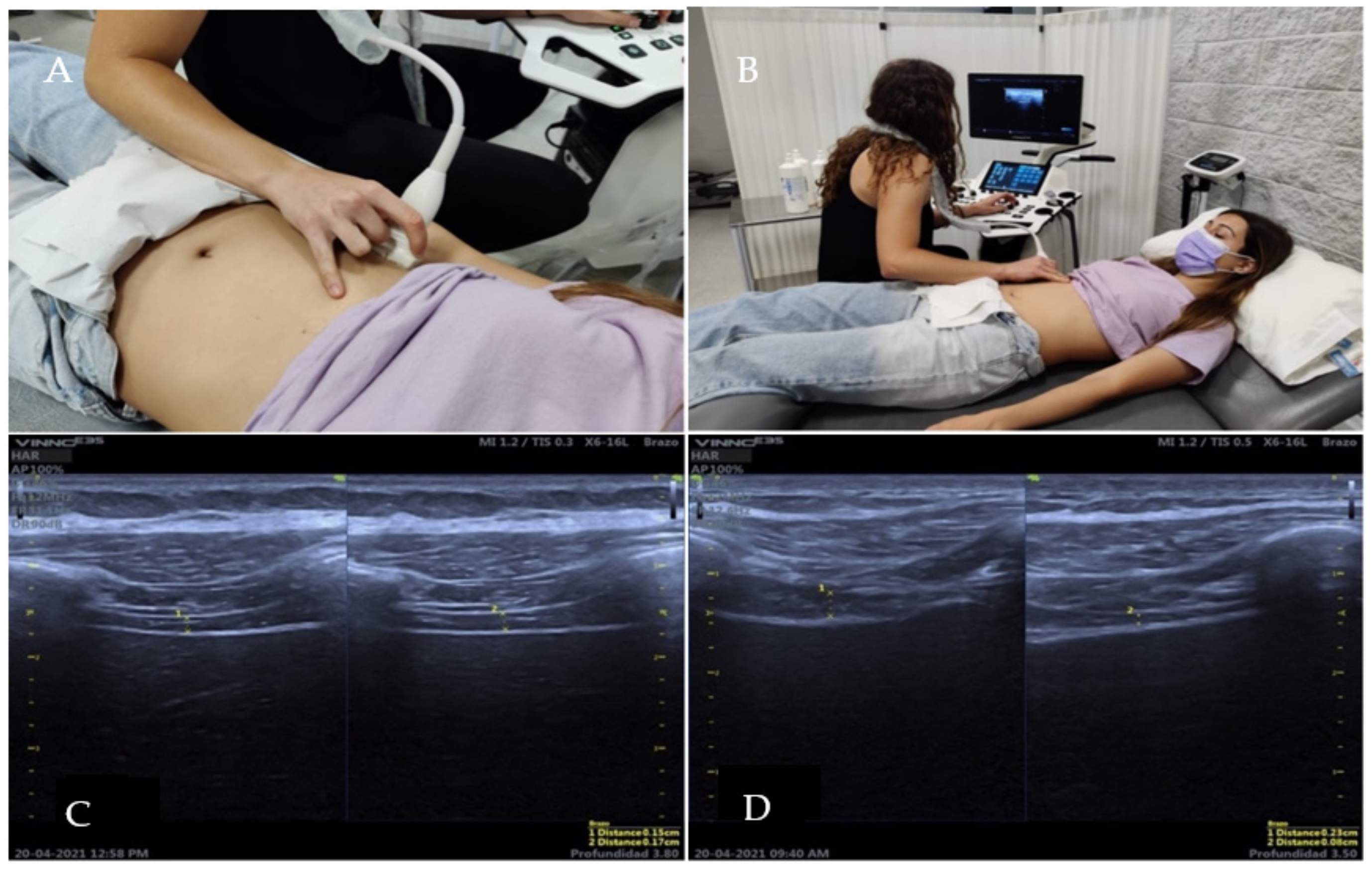
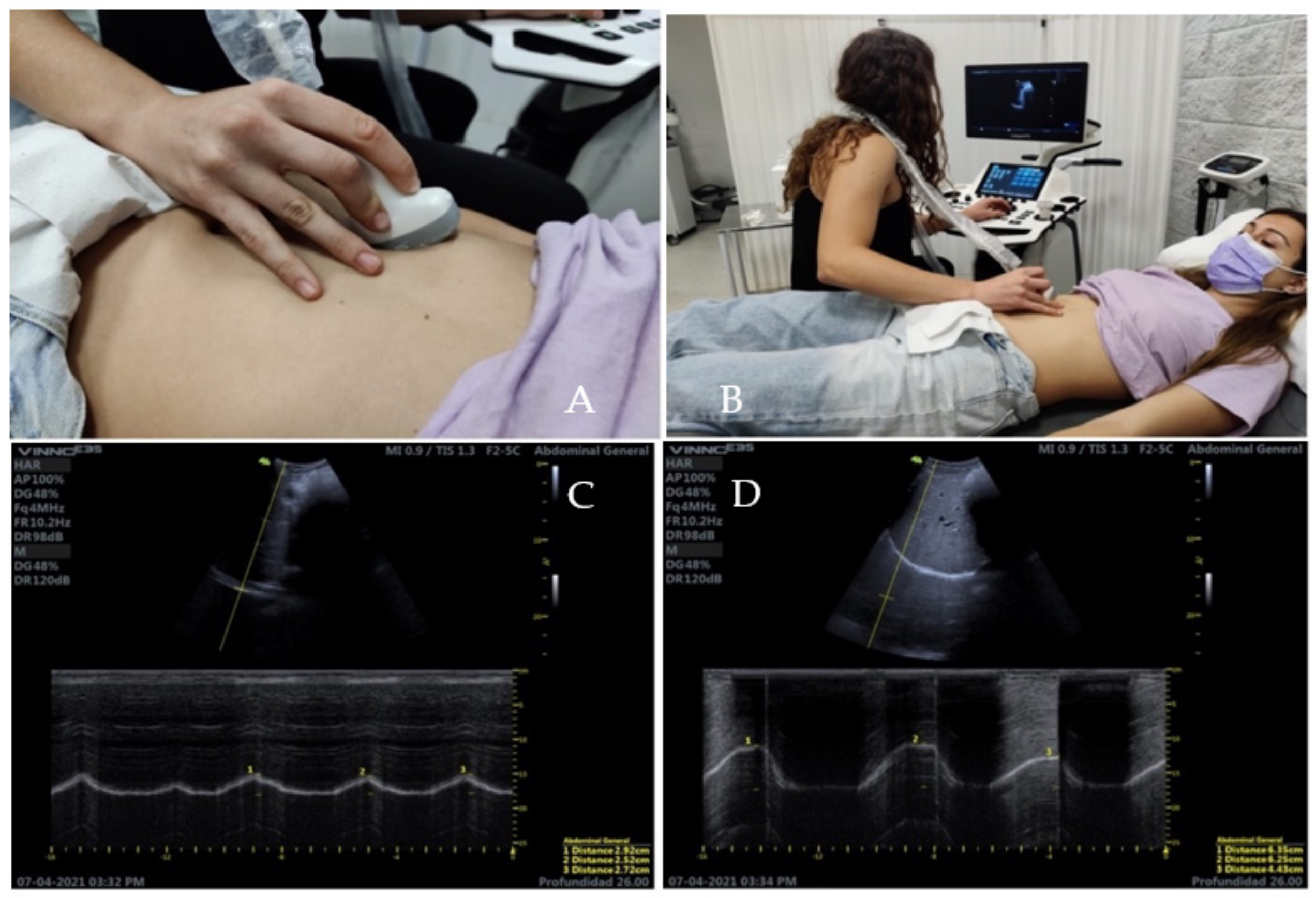
2.4. Ultrasound Measurement of the Diaphragm
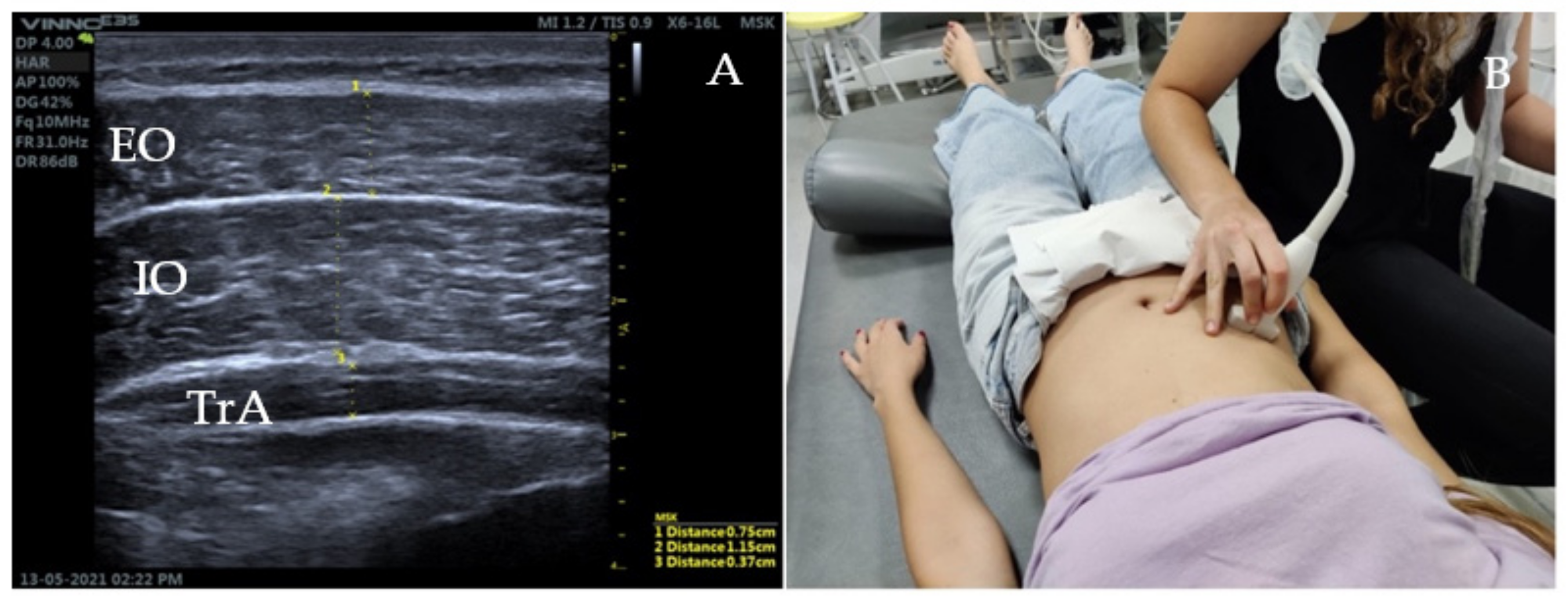
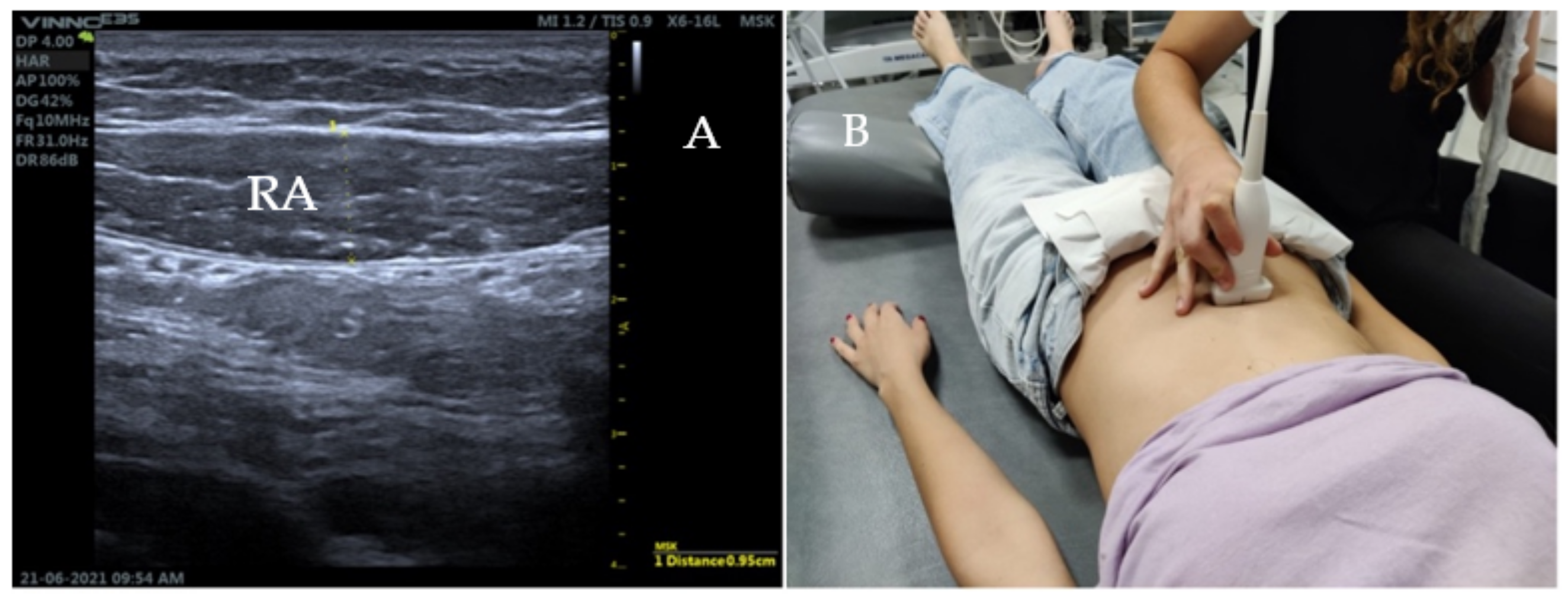
2.5. Ultrasound Measurement of the Abdominal Wall
2.6. Ultrasound Measurement of the Pelvic Floor
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Teyhen, D. Rehabilitative Ultrasound Imaging Symposium San Antonio, TX, 8–10 May 2006. J. Orthop. Sports Phys. Ther. 2006, 36, A1–A3. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Carnero, S.; Calvo-Lobo, C.; Garrido-Marin, A.; Arias-Buría, J. Correction: 2nd Rehabilitative Ultrasound Imaging Symposium in Physical Therapy, Madrid, Spain, 3–5 June 2016. Br. J. Sports Med. 2018, 52 (Suppl. S2), A1–A6. [Google Scholar] [CrossRef]
- Whittaker, J.L.; Teyhen, D.S.; Elliott, J.M.; Cook, K.; Langevin, H.M.; Dahl, H.H.; Stokes, M. Rehabilitative Ultrasound Imaging: Understanding the Technology and Its Applications. J. Orthop. Sports Phys. Ther. 2007, 37, 434–449. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, F.M.; Fernández, C.; Cordero, A.; Muriel, A.; González-Luján, L. Real MTG Del. Non-specific low back pain in primary care in the Spanish National Health Service: A prospective study on clinical outcomes and determinants of management. BMC Health Serv. Res. 2006, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bordoni, B.; Marelli, F.; Bordoni, G. A review of analgesic and emotive breathing: A multidisciplinary approach. J. Multidiscip. Healthc. 2016, 9, 97–102. [Google Scholar] [CrossRef] [PubMed]
- De Troyer, A. Mechanical role of the abdominal muscles in relation to posture. Respir. Physiol. 1983, 53, 341–353. [Google Scholar] [CrossRef]
- Broyles, J.M.; Schuenke, M.D.; Patel, S.R.; Vail, C.M.; Broyles, H.V.; Dellon, A.L. Defining the Anatomy of the Tendinous Intersections of the Rectus Abdominis Muscle and Their Clinical Implications in Functional Muscle Neurotization. Ann. Plast. Surg. 2018, 80, 50–53. [Google Scholar] [CrossRef]
- Fan, C.; Fede, C.; Gaudreault, N.; Porzionato, A.; Macchi, V.; De Caro, R.; Stecco, C. Anatomical and functional relationships between external abdominal oblique muscle and posterior layer of thoracolumbar fascia. Clin. Anat. 2018, 31, 1092–1098. [Google Scholar] [CrossRef]
- Calvo-Lobo, C.; Almazán-Polo, J.; Becerro-De-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Palomo-López, P.; Rodríguez-Sanz, D.; López-López, D. Ultrasonography comparison of diaphragm thickness and excursion between athletes with and without lumbopelvic pain. Phys. Ther. Sport 2019, 37, 128–137. [Google Scholar] [CrossRef]
- Vostatek, P.; Novák, D.; Rychnovský, T.; Rychnovská, Š. Diaphragm postural function analysis using magnetic resonance imaging. PLoS ONE 2013, 8, e56724. [Google Scholar] [CrossRef]
- Kottner, J.; Audigé, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for reporting reliability and agreement studies (GRRAS) were proposed. J. Clin. Epidemiol. 2011, 64, 96–106. [Google Scholar] [CrossRef]
- Zou, G.Y. Sample size formulas for estimating intraclass correlation coefficients with precision and assurance. Stat. Med. 2012, 31, 3972–3981. [Google Scholar] [CrossRef]
- Ferrari, G.; De Filippi, G.; Elia, F.; Panero, F.; Volpicelli, G.; Aprà, F. Diaphragm ultrasound as a new index of discontinuation from mechanical ventilation. Crit. Ultrasound. J. 2014, 6, 1–6. [Google Scholar] [CrossRef]
- Sarwal, A.; Walker, F.O.; Cartwright, M.S.; Sarwal, A.; Walker, F.O.; Cartwright, M.S. Neuromuscular ultrasound for evaluation of the diaphragm. Muscle Nerve 2013, 4, 319–329. [Google Scholar] [CrossRef]
- Harper, C.J.; Shahgholi, L.; Cieslak, K.; Hellyer, N.J.; Strommen, J.A.; Boon, A.J. Variability in Diaphragm Motion During Normal Breathing, Assessed With B-Mode Ultrasound. J. Orthop. Sports Phys. Ther. 2013, 43, 927–931. [Google Scholar] [CrossRef]
- Testa, A.; Soldati, G.; Giannuzzi, R.; Berardi, S.; Portale, G.; Gentiloni Silveri, N. Ultrasound M-Mode Assessment of Diaphragmatic Kinetics by Anterior Transverse Scanning in Healthy Subjects. Ultrasound. Med. Biol. 2011, 37, 44–52. [Google Scholar] [CrossRef]
- Fayssoil, A.; Behin, A.; Ogna, A.; Mompoint, D.; Amthor, H.; Clair, B.; Laforet, P.; Mansart, A.; Prigent, H.; Orlikowski, D.; et al. Diaphragm: Pathophysiology and Ultrasound Imaging in Neuromuscular Disorders. J. Neuromuscul. Dis. 2018, 5, 1–10. [Google Scholar] [CrossRef]
- Wilson, A.; Hides, J.A.; Blizzard, L.; Callisaya, M.; Cooper, A.; Srikanth, V.K.; Winzenberg, T. Measuring ultrasound images of abdominal and lumbar multifidus muscles in older adults: A reliability study. Man Ther. 2015, 23, 114–119. [Google Scholar] [CrossRef]
- Teyhen, D.S.; Gill, N.W.; Whittaker, J.L.; Henry, S.M.; Hides, J.A.; Hodges, P. Rehabilitative ultrasound imaging of the abdominal muscles. J. Orthop. Sports Phys. Ther. 2007, 37, 450–466. [Google Scholar] [CrossRef]
- Lovegrove, R.C.J. Dynamic Evaluation of Female Pelvic Floor Muscle Function Using 2D Ultrasound and Image Processing Methods. Ph.D. Thesis, University of Southampton, Southampton, UK, 2010. [Google Scholar]
- Whittaker, J.L. Ultrasound Imaging of the Abdominal Muscles and Bladder: Implications for the Clinical Assessment of Individuals with Lumbopelvic Pain. Ph.D. Thesis, University of Southampton, Southampton, UK, 2012. [Google Scholar]
- Ludbrook, J. Advantages of permutation (randomization) tests in clinical and experimental pharmacology and physiology. Clin. Exp. Pharmacol. Physiol. 1994, 21, 673–686. [Google Scholar] [CrossRef]
- Hodges, P.; Richardson, C. Inefficient muscular stabilization of the lumbar spine associated with low back pain: A motor control evaluation of transversus abdominis. Spine 1996, 21, 2640–2650. [Google Scholar] [CrossRef]
- Ferreira, P.H.; Ferreira, M.L.; Maher, C.G.; Refshauge, K.; Herbert, R.D.; Hodges, P.W. Changes in recruitment of transversus abdominis correlate with disability in people with chronic low back pain. Br. J. Sport Med. 2010, 44, 1166–1172. [Google Scholar] [CrossRef]
- Pulkovski, N.; Mannion, A.F.; Caporaso, F.; Toma, V.; Gubler, D.; Helbling, D.; Sprott, H. Ultrasound assessment of transversus abdominis muscle contraction ratio during abdominal hollowing: A useful tool to distinguish between patients with chronic low back pain and healthy controls? Eur. Spine J. 2012, 21 (Suppl. S6), S750–S759. [Google Scholar] [CrossRef]
- Ehsani, F.; Sahebi, N.; Shanbehzadeh, S.; Arab, A.M.; ShahAli, S. Stabilization exercise affects function of transverse abdominis and pelvic floor muscles in women with postpartum lumbo-pelvic pain: A double-blinded randomized clinical trial study. Int. Urogynecol. J. 2020, 31, 197–204. [Google Scholar] [CrossRef]
- Ehsani, F.; Arab, A.M.; Assadi, H.; Karimi, N.; Shanbehzadeh, S. Evaluation of pelvic floor muscles activity with and without abdominal maneuvers in subjects with and without low back pain. J. Back Musculoskelet. Rehabil. 2016, 29, 241–247. [Google Scholar] [CrossRef]
- Kocjan, J.; Gzik-Zroska, B.; Nowakowska, K.; Burkacki, M.; Suchoń, S.; Michnik, R.; Czyżewski, D.; Adamek, M. Impact of diaphragm function parameters on balance maintenance. PLoS ONE 2018, 13, e0208697. [Google Scholar] [CrossRef]
- Kolář, P.; Šulc, J.; Kynčl, M.; Šanda, J.; Čakrt, O.; Andel, R.; Kumagai, K.; Kobesová, A. Postural function of the diaphragm in persons with and without chronic low back pain. J. Orthop. Sports Phys. Ther. 2012, 42, 352–362. [Google Scholar] [CrossRef]
- Mohan, V.; Paungmali, A.; Sitilerpisan, P.; Hashim, U.F.; Mazlan, M.B.; Nasuha, T.N. Respiratory characteristics of individuals with non-specific low back pain: A cross-sectional study. Nurs. Health Sci. 2018, 20, 224–230. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| With Pain | Without Pain | ||
|---|---|---|---|
| n | 23 | 31 | |
| Age | 21 [21, 22.5] | 21 [21, 22] | |
| Gender, n (%) | Men | 10 (43.5) | 12 (38.7) |
| Women | 13 (56.5) | 19 (61.3) | |
| Height (meters) | 1.67 [1.65, 1.75] | 1.67 [1.65, 1.78] | |
| Weight (kg) | 62 [55, 72] | 61 [57, 75] | |
| BMI (Body Mass Index) | 21.48 [20.16, 22.94] | 22.04 [20.75, 23.7] | |
| Sport, n (%) | Dance and fitness | 0 (0.0) | 1 (3.2) |
| Cardio | 1 (4.3) | 0 (0.0) | |
| Mountain Cycling | 1 (4.3) | 0 (0.0) | |
| Running | 1 (4.3) | 0 (0.0) | |
| Crossfit | 1 (4.3) | 1 (3.2) | |
| Strength and cardio | 0 (0.0) | 1 (3.2) | |
| Football | 1 (4.3) | 1 (3.2) | |
| Gym | 5 (21.7) | 9 (29.0) | |
| Gym and athletics | 0 (0.0) | 1 (3.2) | |
| Gym and climbing | 1 (4.3) | 0 (0.0) | |
| Gym and spinning | 0 (0.0) | 1 (3.2) | |
| Does not play sports | 8 (34.8) | 3 (9.7) | |
| Padel | 0 (0.0) | 1 (3.2) | |
| Rugby | 0 (0.0) | 1 (3.2) | |
| Running and crossfit | 0 (0.0) | 1 (3.2) | |
| Running and bodybuilding | 0 (0.0) | 2 (6.5) | |
| Route | 1 (4.3) | 0 (0.0) | |
| Softball | 1 (4.3) | 0 (0.0) | |
| Triathlon | 1 (4.3) | 8 (25.8) | |
| Yoga and running | 1 (4.3) | 0 (0.0) | |
| Frequency, n (%) | 1x per week | 0 (0.0) | 1 (3.2) |
| 2x per week | 2 (8.7) | 1 (3.2) | |
| 3x per week | 7 (30.4) | 5 (16.1) | |
| 4x per week | 4 (17.4) | 7 (22.6) | |
| 5x per week | 0 (0.0) | 5 (16.1) | |
| 6x per week | 1 (4.3) | 7 (22.6) | |
| 7x per week | 1 (4.3) | 1 (3.2) | |
| No data | 8 (34.8) | 4 (12.9) | |
| Non-specific Low Back Pain, n (%) | No | 0 (0.0) | 31 (100.0) |
| Yes | 23 (100.0) | 0 (0.0) | |
| VNS | 5.57 ± 1.53 | No data | |
| With Pain | Without Pain | p a | Difference (95%CI) | r (95% CI) | |
|---|---|---|---|---|---|
| 23 | 31 | ||||
| Diaphragmatic thickness TV: inspiration | 0.17 [0.13, 0.20] | 0.14 [0.12, 0.16] | <0.001 | 0.02 (0, 0.05) | 0.26 (0.026, 0.477) |
| Diaphragmatic thickness TV: respiration | 0.14 [0.10, 0.16] | 0.12 [0.10, 0.14] | <0.001 | 0.02 (0, 0.04) | 0.242 (0.019, 0.535) |
| Diaphragmatic thickness FV: inspiration | 0.28 [0.23, 0.35] | 0.26 [0.20, 0.31] | <0.001 | 0.04 (−0.01, 0.09) | 0.207 (0.022, 0.454) |
| Diaphragmatic thickness FV: respiration | 0.13 [0.11, 0.16] | 0.14 [0.11, 0.16] | 1 | 0 (−0.02, 0.02) | 0.034 (0.007, 0.279) |
| DTF TV | 0.21 [0.16, 0.30] | 0.20 [0.14, 0.25] | <0.001 | 0.024 (−0.031, 0.081) | 0.136 (0.004, 0.374) |
| DTF FV | 1.09 [0.77, 1.51] | 0.75 [0.57, 1.33] | <0.001 | 0.236 (−0.047, 0.5) | 0.217 (0.02, 0.449) |
| Diaphragmatic excursion TV | 1.59 [1.38, 2.33] | 1.61 [1.29, 2.21] | 1 | 0.08 (−0.27, 0.42) | 0.072 (0.008, 0.36) |
| Diaphragmatic excursion FV | 4.37 [3.47, 5.12] | 4.38 [3.71, 5.25] | 1 | −0.092 (−0.75, 0.65) | 0.031 (0.002, 0.402) |
| Pelvic floor excursion | 2.83 [2.64, 3.52] | 2.97 [2.44, 3.24] | <0.001 | −0.08 (−0.25, 0.02) | 0.202 (0.013, 0.469) |
| Transverse abdominis thickness R | 2.61 [2.34, 3.12] | 2.49 [2.23, 3.02] | 1 | −0.02 (−0.08, 0.04) | 0.095 (0.007, 0.354) |
| External oblique thickness R | 3.01 [2.72, 3.78] | 3.04 [2.68, 3.42] | <0.001 | 0.01 (−0.09, 0.13) | 0.019 (0.005, 0.311) |
| Internal oblique thickness R | 2.56 [2.29, 3.23] | 2.73 [2.35, 2.99] | 1 | 0.01 (−0.14, 0.16) | 0.026 (0.006, 0.264) |
| Rectus abdominis thickness R | 0.17 [0.14, 0.22] | 0.18 [0.14, 0.21] | 1 | 0.03 (−0.12, 0.19) | 0.056 (0.005, 0.385) |
| ICC 95%CI | |
|---|---|
| Observer 1: Diaphragm VC inspiration | 0.876 (0.813, 0.922) |
| Observer 1: Diaphragm VC expiration | 0.819 (0.732, 0.884) |
| Observer 1: Diaphragm VF inspiration | 0.787 (0.688, 0.863) |
| Observer 1: Diaphragm VF expiration | 0.759 (0.651, 0.844) |
| Observer 2: Diaphragm VC inspiration | 0.763 (0.656, 0.846) |
| Observer 2: Diaphragm VC expiration | 0.788 (0.689, 0.864) |
| Observer 2: Diaphragm VF inspiration | 0.631 (0.489, 0.752) |
| Observer 2: Diaphragm VF expiration | 0.763 (0.657, 0.847) |
| ICC 95% CI | |
|---|---|
| Diaphragm VC inspiration | 0.375 (0.116, 0.585) |
| Diaphragm VC expiration | 0.481 (0.246, 0.663) |
| Diaphragm VF inspiration | 0.245 (−0.024, 0.482) |
| Diaphragm VF expiration | 0.5 (0.267, 0.678) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sicilia-Gomez, C.; Fernández-Carnero, S.; Martin-Perez, A.; Cuenca-Zaldívar, N.; Naranjo-Cinto, F.; Pecos-Martín, D.; Cervera-Cano, M.; Nunez-Nagy, S. Abdominal and Pelvic Floor Activity Related to Respiratory Diaphragmatic Activity in Subjects with and without Non-Specific Low Back Pain. Diagnostics 2022, 12, 2530. https://doi.org/10.3390/diagnostics12102530
Sicilia-Gomez C, Fernández-Carnero S, Martin-Perez A, Cuenca-Zaldívar N, Naranjo-Cinto F, Pecos-Martín D, Cervera-Cano M, Nunez-Nagy S. Abdominal and Pelvic Floor Activity Related to Respiratory Diaphragmatic Activity in Subjects with and without Non-Specific Low Back Pain. Diagnostics. 2022; 12(10):2530. https://doi.org/10.3390/diagnostics12102530
Chicago/Turabian StyleSicilia-Gomez, Cristina, Samuel Fernández-Carnero, Alicia Martin-Perez, Nicolas Cuenca-Zaldívar, Fermin Naranjo-Cinto, Daniel Pecos-Martín, Maria Cervera-Cano, and Susana Nunez-Nagy. 2022. "Abdominal and Pelvic Floor Activity Related to Respiratory Diaphragmatic Activity in Subjects with and without Non-Specific Low Back Pain" Diagnostics 12, no. 10: 2530. https://doi.org/10.3390/diagnostics12102530
APA StyleSicilia-Gomez, C., Fernández-Carnero, S., Martin-Perez, A., Cuenca-Zaldívar, N., Naranjo-Cinto, F., Pecos-Martín, D., Cervera-Cano, M., & Nunez-Nagy, S. (2022). Abdominal and Pelvic Floor Activity Related to Respiratory Diaphragmatic Activity in Subjects with and without Non-Specific Low Back Pain. Diagnostics, 12(10), 2530. https://doi.org/10.3390/diagnostics12102530