
Clinical Comparison of FD-CT and MS-CT in Aneurysmal Subarachnoid Haemorrhage: A Single Center Experience
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Acquisition and Postprocessing
2.2.1. FD-CT
2.2.2. MS-CT
2.3. Data Evaluation
2.3.1. Image Quality
2.3.2. Qualitative Analysis
2.3.3. Quantitative Analysis
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Image Quality
3.2.1. FD-CT
3.2.2. MS-CT
3.3. Qualitative Analysis
3.3.1. Blood Distribution
3.3.2. External Ventricular Drain Position
3.3.3. Acute Obstructive Hydrocephalus
3.4. Quantitative Analysis
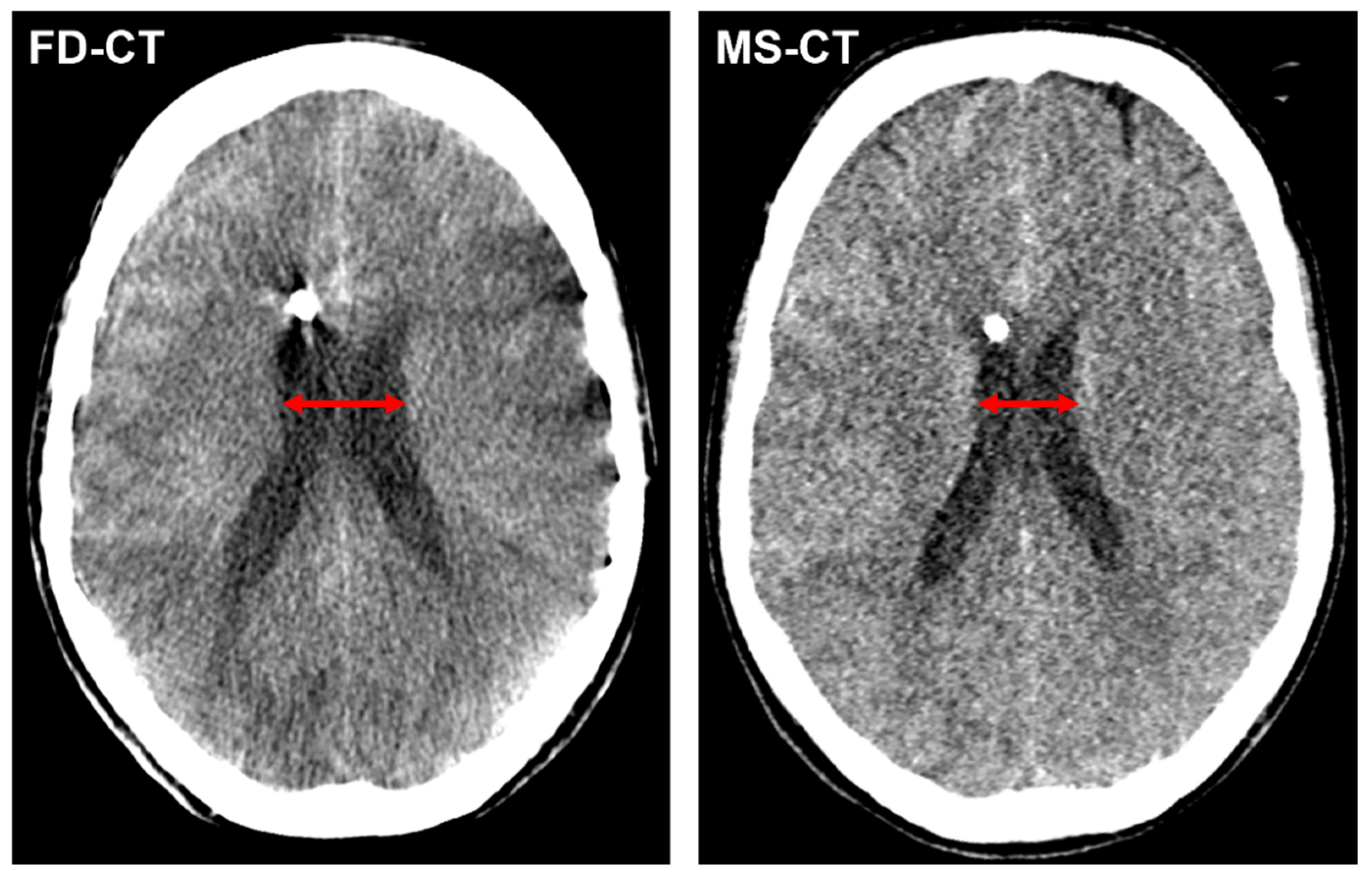
3.4.1. Cella Media Distance
3.4.2. Modified Graeb Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnston, S.C.; Selvin, S.; Gress, D.R. The burden, trends, and demographics of mortality from subarachnoid hemorrhage. Neurology 1998, 50, 1413–1418. [Google Scholar] [CrossRef]
- Petridis, A.K.; Kamp, M.A.; Cornelius, J.F.; Beez, T.; Beseoglu, K.; Turowski, B.; Steiger, H.J. Aneurysmal Subarachnoid Hemorrhage. Dtsch. Arztebl. Int. 2017, 114, 226–236. [Google Scholar] [CrossRef]
- Macdonald, R.L.; Schweizer, T.A. Spontaneous subarachnoid haemorrhage. Lancet 2017, 389, 655–666. [Google Scholar] [CrossRef]
- Neifert, S.N.; Chapman, E.K.; Martini, M.L.; Shuman, W.H.; Schupper, A.J.; Oermann, E.K.; Mocco, J.; Macdonald, R.L. Aneurysmal Subarachnoid Hemorrhage: The Last Decade. Transl. Stroke Res. 2021, 12, 428–446. [Google Scholar] [CrossRef]
- Rinkel, G.J.; Algra, A. Long-term outcomes of patients with aneurysmal subarachnoid haemorrhage. Lancet Neurol. 2011, 10, 349–356. [Google Scholar] [CrossRef]
- Muehlschlegel, S. Subarachnoid Hemorrhage. Contin. Lifelong Learn. Neurol. 2018, 24, 1623–1657. [Google Scholar] [CrossRef]
- Suarez, J.I.; Tarr, R.W.; Selman, W.R. Aneurysmal subarachnoid hemorrhage. N. Engl. J. Med. 2006, 354, 387–396. [Google Scholar] [CrossRef]
- Dubosh, N.M.; Bellolio, M.F.; Rabinstein, A.A.; Edlow, J.A. Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Stroke 2016, 47, 750–755. [Google Scholar] [CrossRef]
- Long, B.; Koyfman, A.; Runyon, M.S. Subarachnoid Hemorrhage: Updates in Diagnosis and Management. Emerg. Med. Clin. North. Am. 2017, 35, 803–824. [Google Scholar] [CrossRef]
- Steiner, T.; Juvela, S.; Unterberg, A.; Jung, C.; Forsting, M.; Rinkel, G. European Stroke Organization guidelines for the management of intracranial aneurysms and subarachnoid haemorrhage. Cerebrovasc. Dis. 2013, 35, 93–112. [Google Scholar] [CrossRef]
- Froehler, M.T. Endovascular treatment of ruptured intracranial aneurysms. Curr. Neurol. Neurosci. Rep. 2013, 13, 326. [Google Scholar] [CrossRef]
- Suarez, J.I. Treatment of ruptured cerebral aneurysms and vasospasm after subarachnoid hemorrhage. Neurosurg. Clin. N. Am. 2006, 17, 57–69. [Google Scholar] [CrossRef]
- Molyneux, A.J.; Kerr, R.S.; Yu, L.M.; Clarke, M.; Sneade, M.; Yarnold, J.A.; Sandercock, P. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005, 366, 809–817. [Google Scholar] [CrossRef]
- Campos, J.K.; Lien, B.V.; Wang, A.S.; Lin, L.M. Advances in endovascular aneurysm management: Coiling and adjunctive devices. Stroke Vasc. Neurol. 2020, 5, 14–21. [Google Scholar] [CrossRef]
- Eden, S.V.; Meurer, W.J.; Sánchez, B.N.; Lisabeth, L.D.; Smith, M.A.; Brown, D.L.; Morgenstern, L.B. Gender and ethnic differences in subarachnoid hemorrhage. Neurology 2008, 71, 731–735. [Google Scholar] [CrossRef]
- Van Gijn, J.; Kerr, R.S.; Rinkel, G.J. Subarachnoid haemorrhage. Lancet 2007, 369, 306–318. [Google Scholar] [CrossRef]
- Germanwala, A.V.; Huang, J.; Tamargo, R.J. Hydrocephalus after aneurysmal subarachnoid hemorrhage. Neurosurg. Clin. N. Am. 2010, 21, 263–270. [Google Scholar] [CrossRef]
- Mehta, V.; Holness, R.O.; Connolly, K.; Walling, S.; Hall, R. Acute hydrocephalus following aneurysmal subarachnoid hemorrhage. Can. J. Neurol. Sci. 1996, 23, 40–45. [Google Scholar] [CrossRef]
- Chen, S.; Luo, J.; Reis, C.; Manaenko, A.; Zhang, J. Hydrocephalus after Subarachnoid Hemorrhage: Pathophysiology, Diagnosis, and Treatment. Biomed. Res. Int. 2017, 2017, 8584753. [Google Scholar] [CrossRef]
- Wilkins, R.H. Cerebral vasospasm. Crit. Rev. Neurobiol. 1990, 6, 51–77. [Google Scholar] [CrossRef]
- Li, K.; Barras, C.D.; Chandra, R.V.; Kok, H.K.; Maingard, J.T.; Carter, N.S.; Russell, J.H.; Lai, L.; Brooks, M.; Asadi, H. A Review of the Management of Cerebral Vasospasm After Aneurysmal Subarachnoid Hemorrhage. World Neurosurg. 2019, 126, 513–527. [Google Scholar] [CrossRef] [PubMed]
- Ciurea, A.V.; Palade, C.; Voinescu, D.; Nica, D.A. Subarachnoid hemorrhage and cerebral vasospasm—Literature review. J. Med. Life 2013, 6, 120–125. [Google Scholar]
- Struffert, T.; Richter, G.; Engelhorn, T.; Doelken, M.; Goelitz, P.; Kalender, W.A.; Ganslandt, O.; Doerfler, A. Visualisation of intracerebral haemorrhage with flat-detector CT compared to multislice CT: Results in 44 cases. Eur. Radiol. 2009, 19, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Struffert, T.; Eyupoglu, I.Y.; Huttner, H.B.; Engelhorn, T.; Doelken, M.; Saake, M.; Ganslandt, O.; Doerfler, A. Clinical evaluation of flat-panel detector compared with multislice computed tomography in 65 patients with acute intracranial hemorrhage: Initial results. Clinical article. J. Neurosurg. 2010, 113, 901–907. [Google Scholar] [CrossRef]
- Morgan, T.C.; Dawson, J.; Spengler, D.; Lees, K.R.; Aldrich, C.; Mishra, N.K.; Lane, K.; Quinn, T.J.; Diener-West, M.; Weir, C.J.; et al. The Modified Graeb Score: An enhanced tool for intraventricular hemorrhage measurement and prediction of functional outcome. Stroke 2013, 44, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Hunt, W.E.; Hess, R.M. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J. Neurosurg. 1968, 28, 14–20. [Google Scholar] [CrossRef]
- Eckert, M.; Gölitz, P.; Lücking, H.; Struffert, T.; Knossalla, F.; Doerfler, A. Optimized Flat-Detector CT in Stroke Imaging: Ready for First-Line Use? Cerebrovasc. Dis. 2017, 43, 9–16. [Google Scholar] [CrossRef]
- Leyhe, J.R.; Tsogkas, I.; Hesse, A.C.; Behme, D.; Schregel, K.; Papageorgiou, I.; Liman, J.; Knauth, M.; Psychogios, M.N. Latest generation of flat detector CT as a peri-interventional diagnostic tool: A comparative study with multidetector CT. J. NeuroInterventional Surg. 2017, 9, 1253–1257. [Google Scholar] [CrossRef]
- Psychogios, M.N.; Buhk, J.H.; Schramm, P.; Xyda, A.; Mohr, A.; Knauth, M. Feasibility of angiographic CT in peri-interventional diagnostic imaging: A comparative study with multidetector CT. AJNR Am. J. Neuroradiol. 2010, 31, 1226–1231. [Google Scholar] [CrossRef]
- Velásquez, C.; Rivero-Garvía, M.; Mayorga-Buiza, M.J.; Cañizares-Méndez, M.L.; Jiménez-Mejías, M.E.; Márquez-Rivas, J. Avoiding pullout complications in external ventricular drains: Technical note. J. Neurosurg. 2017, 126, 1003–1005. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | n |
|---|---|
| male | 139 (33.9%) |
| female | 271 (66.1%) |
| Hunt & Hess grade | |
| 1 | 127 (31%) |
| 2 | 86 (21%) |
| 3 | 71 (17.3%) |
| 4 | 62 (15.1%) |
| 5 | 64 (15.6%) |
| Endovascular treatment approach | |
| coiling | 326 (75.3%) |
| ballon-assisted coiling | 52 (12%) |
| extra-aneurysmal flow-diversion | 25 (5.8%) |
| stent-assisted coiling | 14 (3.2%) |
| intra-aneurysmal flow-diversion | 12 (2.8%) |
| extra-aneurysmal flow-diversion plus coiling | 4 (0.9%) |
| Aneurysm location | |
| anterior communicating artery | 157 (36.3%) |
| internal carotid artery | 110 (25.4%) |
| middle cerebral artery | 45 (10.4%) |
| basilar artery | 42 (9.7%) |
| posterior inferior cerebellar artery | 27 (6.2%) |
| anterior cerebral artery | 24 (5.5.%) |
| vertebral artery | 15 (3.5%) |
| posterior cerebral artery | 11 (2.5%) |
| anterior inferior cerebellar artery | 2 (0.5%) |
| IQ | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| nFD-CT | 0 | 8 | 20 | 56 | 326 |
| nMS-CT | 0 | 7 | 21 | 52 | 330 |
| nFD-CT | nMS-CT | |
|---|---|---|
| SAH | 401 | 401 |
| ICH | 94 | 94 |
| IVH | 309 | 281 |
| EVDcorrect | 299 | 290 |
| AOH | 290 | 290 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eisenhut, F.; Heidelbach, C.; Heynold, E.; Manhart, M.; Struffert, T.; Brandner, S.; Doerfler, A.; Lang, S. Clinical Comparison of FD-CT and MS-CT in Aneurysmal Subarachnoid Haemorrhage: A Single Center Experience. Diagnostics 2022, 12, 2443. https://doi.org/10.3390/diagnostics12102443
Eisenhut F, Heidelbach C, Heynold E, Manhart M, Struffert T, Brandner S, Doerfler A, Lang S. Clinical Comparison of FD-CT and MS-CT in Aneurysmal Subarachnoid Haemorrhage: A Single Center Experience. Diagnostics. 2022; 12(10):2443. https://doi.org/10.3390/diagnostics12102443
Chicago/Turabian StyleEisenhut, Felix, Cornelius Heidelbach, Elisabeth Heynold, Michael Manhart, Tobias Struffert, Sebastian Brandner, Arnd Doerfler, and Stefan Lang. 2022. "Clinical Comparison of FD-CT and MS-CT in Aneurysmal Subarachnoid Haemorrhage: A Single Center Experience" Diagnostics 12, no. 10: 2443. https://doi.org/10.3390/diagnostics12102443
APA StyleEisenhut, F., Heidelbach, C., Heynold, E., Manhart, M., Struffert, T., Brandner, S., Doerfler, A., & Lang, S. (2022). Clinical Comparison of FD-CT and MS-CT in Aneurysmal Subarachnoid Haemorrhage: A Single Center Experience. Diagnostics, 12(10), 2443. https://doi.org/10.3390/diagnostics12102443