
AI Denoising Significantly Improves Image Quality in Whole-Body Low-Dose Computed Tomography Staging

 , , ,
, , , 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population, and Radiation Dose
2.2. Image Acquisition and Reconstruction Parameters
2.3. Image Quality Analysis
2.3.1. Subjective Image Quality
2.3.2. Objective Image Quality
2.4. Statistical Analysis
3. Results
3.1. Study Population and Radiation Dose
3.2. Image Quality Analysis
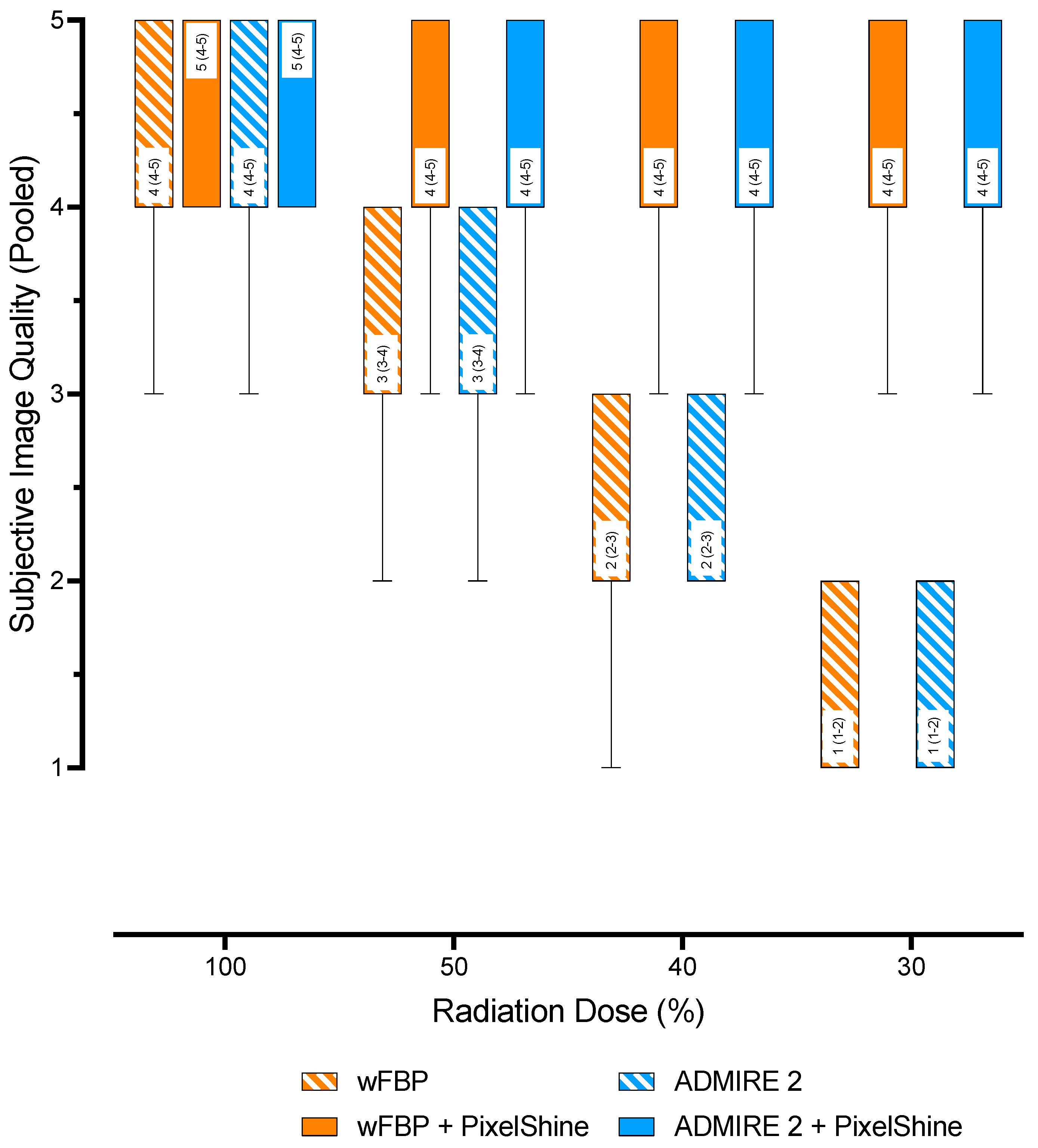
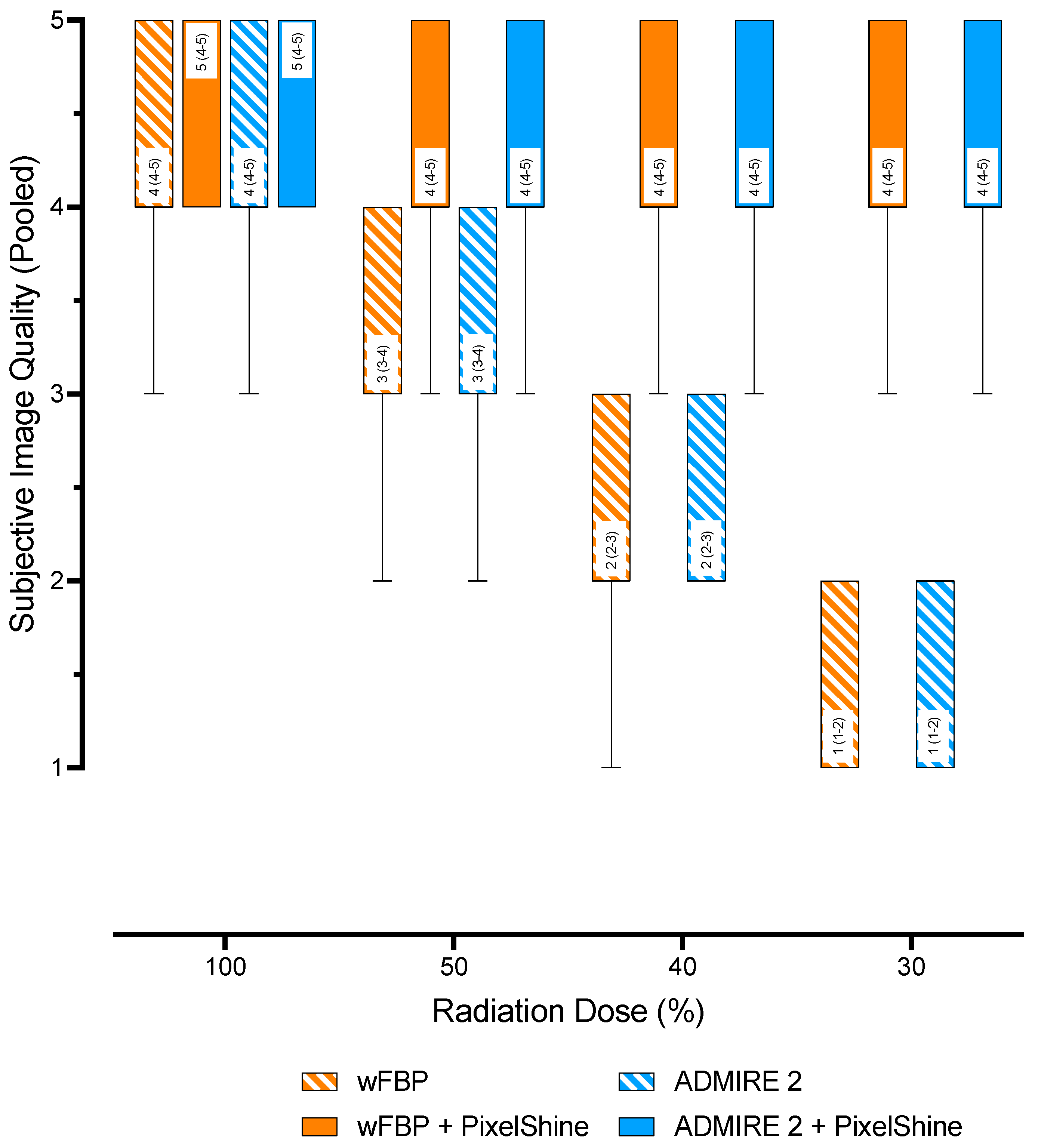
3.2.1. Subjective Image Quality
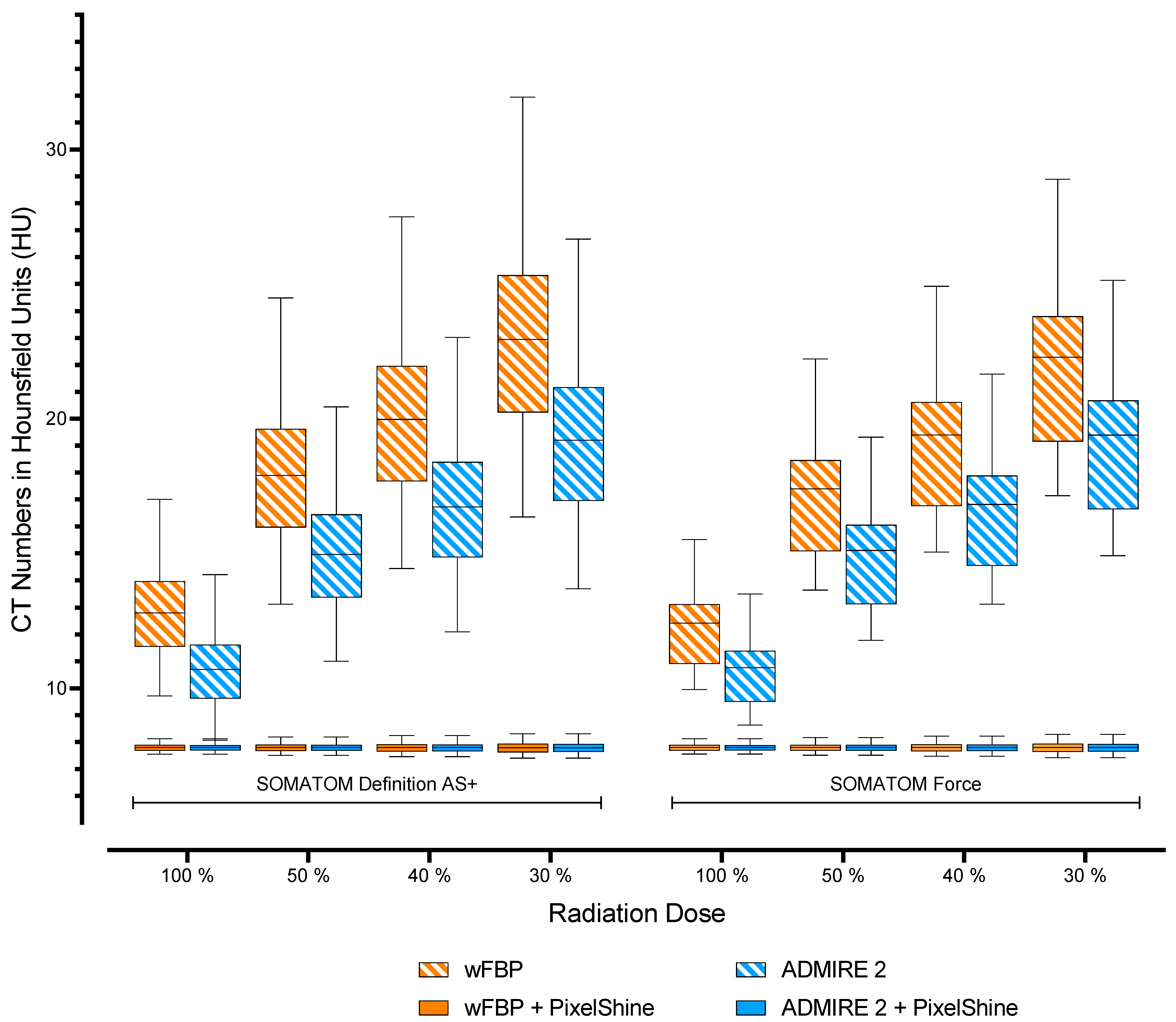
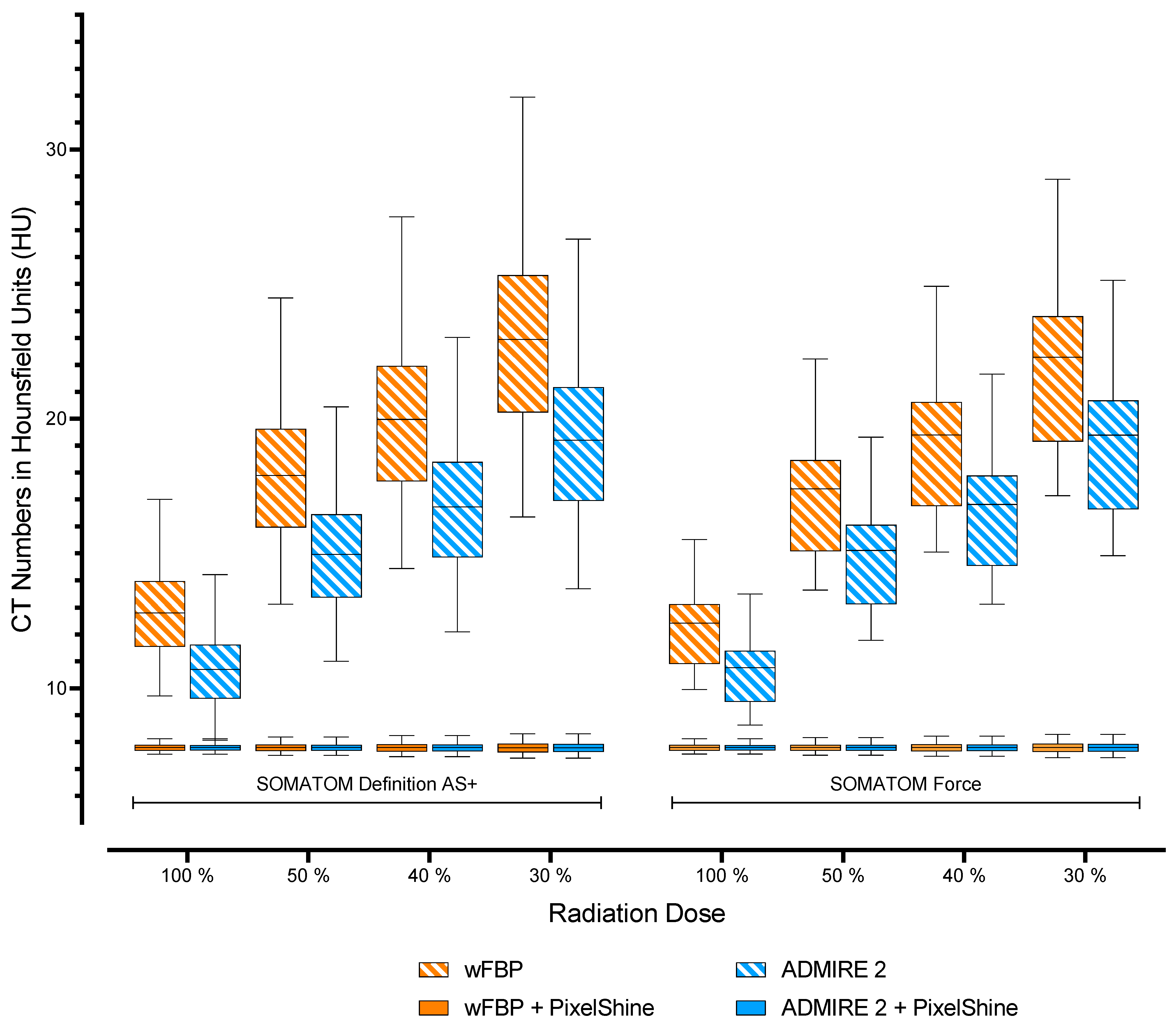
3.2.2. Objective Image Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zondervan, R.L.; Hahn, P.F.; Sadow, C.A.; Liu, B.; Lee, S.I. Frequent Body CT Scanning of Young Adults: Indications, Outcomes, and Risk for Radiation-Induced Cancer. J. Am. Coll. Radiol. 2011, 8, 501–507. [Google Scholar] [CrossRef]
- Trugenberger-Schnabel, A.; Merchel, D.; Löbke-Reinl, A.; Peter, J. Environmental Radioactivity and Radiation Exposure Annual Report 2018; Bundesministerium für Umwelt, Naturschutz und nukleare Sicherheit (BMU): Bonn, Germany, 2018. [Google Scholar]
- Brenner, D.J.; Hall, E.J. Computed Tomography—An Increasing Source of Radiation Exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- De González, A.B.; Mahesh, M.; Kim, K.-P.; Bhargavan, M.; Lewis, R.; Mettler, F.; Land, C. Projected Cancer Risks From Computed Tomographic Scans Performed in the United States in 2007. Arch. Intern. Med. 2009, 169, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, P.; Sinha, R.; Tumeh, J.W.; Lechowicz, M.J.; Flowers, C. Surveillance Computed Tomography Scans for Patients With Lymphoma: Is the Risk Worth the Benefits? Clin. Lymphoma Myeloma Leuk. 2010, 10, 270–277. [Google Scholar] [CrossRef]
- Shao, Y.-H.; Tsai, K.; Kim, S.; Wu, Y.-J.; Demissie, K. Exposure to Tomographic Scans and Cancer Risks. JNCI Cancer Spectr. 2020, 4, pkz072. [Google Scholar] [CrossRef]
- Fletcher, J.G.; Fidler, J.L.; Venkatesh, S.K.; Hough, D.M.; Takahashi, N.; Yu, L.; Johnson, M.; Leng, S.; Holmes, D.R., III; Carter, R. Observer performance with varying radiation dose and reconstruction methods for detection of hepatic metastases. Radiology 2018, 289, 455–464. [Google Scholar] [CrossRef]
- Karpitschka, M.; Augart, D.; Becker, H.-C.; Reiser, M.; Graser, A. Dose reduction in oncological staging multidetector CT: Effect of iterative reconstruction. Br. J. Radiol. 2013, 86, 20120224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangold, S.; Wichmann, J.L.; Schoepf, U.J.; Poole, Z.B.; Canstein, C.; Varga-Szemes, A.; Caruso, D.; Bamberg, F.; Nikolaou, K.; De Cecco, C.N. Automated tube voltage selection for radiation dose and contrast medium reduction at coronary CT angiography using 3rd generation dual-source CT. Eur. Radiol. 2016, 26, 3608–3616. [Google Scholar] [CrossRef] [PubMed]
- Afat, S.; Brockmann, C.; Nikoubashman, O.; Müller, M.; Thierfelder, K.M.; Brockmann, M.A.; Nikolaou, K.; Wiesmann, M.; Kim, J.H.; Othman, A.E. Diagnostic Accuracy of Simulated Low-Dose Perfusion CT to Detect Cerebral Perfusion Impairment after Aneurysmal Subarachnoid Hemorrhage: A Retrospective Analysis. Radiol. 2018, 287, 643–650. [Google Scholar] [CrossRef] [Green Version]
- Brendlin, A.S.; Winkelmann, M.T.; Do, P.L.; Schwarze, V.; Peisen, F.; Almansour, H.; Bongers, M.N.; Artzner, C.P.; Weiss, J.; Kim, J.H.; et al. Simulated Radiation Dose Reduction in Whole-Body CT on a 3rd Generation Dual-Source Scanner: An Intraindividual Comparison. Diagnostics 2021, 11, 118. [Google Scholar] [CrossRef]
- Steuwe, A.; Weber, M.; Bethge, O.; Sawicki, L.; Antoch, G.; Aissa, J. Einfluss einer neuen deep-learning basierten Rauschunterdrückung für gefilterte Rückprojektionen im Vergleich zu iterativ rekonstruierten Bildern. In Proceedings of the 101. Deutscher Röntgenkongress und 9. Gemeinsamer Kongress der DRG und ÖRG, Leipzig, Germany, 20–23 May 2020; Georg Thieme Verlag KG: Stuttgart, Germany, 2020; Volume 192, p. WISS.5. [Google Scholar]
- Mechlem, K.; Allner, S.; Ehn, S.; Mei, K.; Braig, E.; Münzel, D.; Pfeiffer, F.; Noël, P.B. A post-processing algorithm for spectral CT material selective images using learned dictionaries. Biomed. Phys. Eng. Express 2017, 3, 025009. [Google Scholar] [CrossRef]
- Noda, Y.; Nakamura, F.; Kawamura, T.; Kawai, N.; Kaga, T.; Miyoshi, T.; Kato, H.; Hyodo, F.; Matsuo, M. Deep-learning image-reconstruction algorithm for dual-energy CT angiography with reduced iodine dose: Preliminary results. Clin. Radiol. 2021, 77, e138–e146. [Google Scholar] [CrossRef]
- Diwakar, M.; Kumar, M. A review on CT image noise and its denoising. Biomed. Signal Process. Control. 2018, 42, 73–88. [Google Scholar] [CrossRef]
- Mohammadinejad, P.; Mileto, A.; Yu, L.; Leng, S.; Guimaraes, L.S.; Missert, A.D.; Jensen, C.T.; Gong, H.; McCollough, C.H.; Fletcher, J.G. CT Noise-Reduction Methods for Lower-Dose Scanning: Strengths and Weaknesses of Iterative Reconstruction Algorithms and New Techniques. Radiogr 2021, 41, 1493–1508. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Into Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef] [Green Version]
- Agarwala, S.S.; Eggermont, A.M.M.; O’Day, S.; Zager, J.S. Metastatic melanoma to the liver: A contemporary and comprehensive review of surgical, systemic, and regional therapeutic options. Cancer 2013, 120, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Higaki, T.; Tatsugami, F.; Zhou, J.; Yu, Z.; Akino, N.; Ito, Y.; Iida, M.; Awai, K. Deep Learning–based CT Image Reconstruction: Initial Evaluation Targeting Hypovascular Hepatic Metastases. Radiol. Artif. Intell. 2019, 1, e180011. [Google Scholar] [CrossRef]
- ICRP. The 2007 Recommendations of the International Commission on Radiological Protection. Ann. ICRP 2007, 37, 2–4. [Google Scholar]
- Bongartz, G.; Golding, S.J.; Jurik, A.G.; Leonardi, M.; van Meerten, E.v.P.; Geleijns, J.; Jessen, K.A.; Panzer, W.; Shrimpton, P.C.; Tosi, G.; et al. European Guidelines on Quality Criteria for Computed Tomography; Publications Office of the European Union: Luxembourg, 2000. [Google Scholar]
- Brendlin, A.S.; Reinert, C.P.; Baumgartner, H.; Bongers, M.N.; Thomas, C.; Afat, S.; Springer, F.; Almansour, H. CT in Patients With External Fixation for Complex Lower Extremity Fractures: Impact of Iterative Metal Artifact Reduction Techniques on Metal Artifact Burden and Subjective Quality. Am. J. Roentgenol. 2021, 10, 1–10. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Shin, Y.J.; Chang, W.; Ye, J.C.; Kang, E.; Oh, D.Y.; Lee, Y.J.; Park, J.H.; Kim, Y.H. Low-Dose Abdominal CT Using a Deep Learning-Based Denoising Algorithm: A Comparison with CT Reconstructed with Filtered Back Projection or Iterative Reconstruction Algorithm. Korean J. Radiol. 2020, 21, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.; Min, J.; Ye, J.C. A deep convolutional neural network using directional wavelets for low-dose X-ray CT reconstruction. Med. Phys. 2017, 44, e360–e375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hata, A.; Yanagawa, M.; Yoshida, Y.; Miyata, T.; Tsubamoto, M.; Honda, O.; Tomiyama, N. Combination of Deep Learning–Based Denoising and Iterative Reconstruction for Ultra-Low-Dose CT of the Chest: Image Quality and Lung-RADS Evaluation. Am. J. Roentgenol. 2020, 215, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Yanagawa, M.; Gyobu, T.; Leung, A.N.; Kawai, M.; Kawata, Y.; Sumikawa, H.; Honda, O.; Tomiyama, N. Ultra-low-dose CT of the Lung: Effect of Iterative Reconstruction Techniques on Image Quality. Acad. Radiol. 2014, 21, 695–703. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | Overall | ||||
|---|---|---|---|---|---|---|
| SOMATOM Definition AS+ | Patient characteristics | |||||
| N | 30 | 30 | 60 | |||
| Age | 63 ± 12 | 59 ± 16 | 61 ± 14 | |||
| BMI | 26 ± 3 | 27 ± 2 | 26 ± 3 | |||
| Radiation dose | ||||||
| CTDIvol (mean ± SD) | 4.31 ± 0.95 | 4.46 ± 0.94 | 4.38 ± 0.95 | |||
| DLP (mean ± SD) | 746.63 ± 165.58 | 759.54 ± 168.45 | 753.08 ± 167.15 | |||
| ED (mean ± SD) | ||||||
| 100% mAs | 10.72 ± 2.53 | 11.39 ± 2.53 | 11.05 ± 2.55 | |||
| 50% mAs | 5.36 ± 1.27 | 5.70 ± 1.26 | 5.53 ± 1.28 | |||
| 40% mAs | 4.29 ± 1.01 | 4.56 ± 1.01 | 4.43 ± 1.02 | |||
| 30% mAs | 3.22 ± 0.76 | 3.42 ± 0.76 | 3.32 ± 0.77 | |||
| SOMATOM Force | Patient characteristics | |||||
| N | 30 | 30 | 60 | |||
| Age | 63 ± 12 | 59 ± 16 | 61 ± 14 | |||
| BMI | 26 ± 3 | 27 ± 2 | 26 ± 3 | |||
| Radiation dose | ||||||
| CTDIvol (mean ± SD) | 4.15 ± 0.97 | 4.32 ± 0.97 | 4.22 ± 0.97 | |||
| DLP (mean ± SD) | 714.42 ± 168.85 | 726.78 ± 171.77 | 720.60 ± 170.43 | |||
| ED (mean ± SD) | ||||||
| 100% mAs | 9.17 ± 2.17 | 9.59 ± 2.13 | 9.38 ± 2.16 | |||
| 50% mAs | 4.59 ± 1.08 | 4.79 ± 1.06 | 4.69 ± 1.08 | |||
| 40% mAs | 3.67 ± 0.87 | 3.83 ± 0.85 | 3.75 ± 0.86 | |||
| 30% mAs | 2.75 ± 0.65 | 2.88 ± 0.64 | 2.81 ± 0.65 | |||
| Timepoint 1 | Timepoint 1 | Timepoint 1 vs. 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Rating | Inter-Rater Agreement | Rating | Inter-Rater Agreement | Intra-Rater Reliability | ||||||
| ED | Mode | Median (IQR) | ICC (95% CI) | p | Median (IQR) | ICC (95% CI) | p | ICC (95% CI) | p | |
| SOMATOM Definition AS+ | 100% | wFBP | 4 (4–4) | 0.97 (0.96–0.98) | <0.001 | 4 (3–4) | 0.95 (0.93–0.97) | <0.001 | 0.98 (0.97–0.99) | <0.001 |
| ADMIRE 2 | 4 (4–5) | 0.96 (0.94–0.98) | <0.001 | 4 (4–5) | 0.96 (0.95–0.98) | <0.001 | 0.98 (0.97–0.98) | <0.001 | ||
| wFBP + PS | 4 (4–5) | 0.97 (0.96–0.98) | <0.001 | 4 (4–5) | 0.86 (0.80–0.91) | <0.001 | 0.98 (0.97–0.98) | <0.001 | ||
| ADMIRE 2 + PS | 4 (4–5) | 0.97 (0.95–0.98) | <0.001 | 4 (4–5) | 0.93 (0.90–0.96) | <0.001 | 0.98 (0.98–0.99) | <0.001 | ||
| 50% | wFBP | 3 (3–3) | 0.98 (0.98–0.99) | <0.001 | 3 (2–3) | 0.98 (0.97–0.99) | <0.001 | 0.98 (0.98–0.99) | <0.001 | |
| ADMIRE 2 | 3 (3–4) | 0.98 (0.97–0.99) | <0.001 | 3 (3–4) | 0.97 (0.95–0.98) | <0.001 | 0.98 (0.97–0.99) | <0.001 | ||
| wFBP + PS | 4 (4–5) | 0.94 (0.92–0.96) | <0.001 | 4 (4–5) | 0.89 (0.83–0.93) | <0.001 | 0.94 (0.92–0.96) | <0.001 | ||
| ADMIRE 2 + PS | 4 (4–5) | 0.95 (0.93–0.97) | <0.001 | 4 (4–5) | 0.93 (0.90–0.96) | <0.001 | 0.95 (0.93–0.97) | <0.001 | ||
| 40% | wFBP | 2 (2–2) | 0.98 (0.97–0.99) | <0.001 | 2 (1–2) | 0.97 (0.95–0.98) | <0.001 | 0.99 (0.98–0.99) | <0.001 | |
| ADMIRE 2 | 2 (2–2) | 0.99 (0.98–0.99) | <0.001 | 2 (2–3) | 0.96 (0.94–0.97) | <0.001 | 0.98 (0.97–0.99) | <0.001 | ||
| wFBP + PS | 4 (4–5) | 0.92 (0.89–0.95) | <0.001 | 4 (4–5) | 0.91 (0.87–0.94) | <0.001 | 0.92 (0.88–0.95) | <0.001 | ||
| ADMIRE 2 + PS | 4 (4–5) | 0.95 (0.93–0.97) | <0.001 | 4 (4–5) | 0.95 (0.92–0.96) | <0.001 | 0.95 (0.92–0.96) | <0.001 | ||
| 30% | wFBP | 1 (1–1) | 0.99 (0.98–0.99) | <0.001 | 1 (1-1) | 0.96 (0.94–0.97) | <0.001 | 0.98 (0.97–0.99) | <0.001 | |
| ADMIRE 2 | 1 (1–2) | 0.97 (0.96–0.98) | <0.001 | 1 (1-2) | 0.96 (0.94–0.97) | <0.001 | 0.98 (0.97–0.99) | <0.001 | ||
| wFBP + PS | 4 (4–5) | 0.91 (0.87–0.94) | <0.001 | 4 (4-5) | 0.96 (0.94–0.98) | <0.001 | 0.91 (0.87–0.94) | <0.001 | ||
| ADMIRE 2 + PS | 4 (4–5) | 0.95 (0.92–0.96) | <0.001 | 4 (4-5) | 0.98 (0.97–0.98) | <0.001 | 0.94 (0.92–0.96) | <0.001 | ||
| SOMATOM Force | 100% | wFBP | 4 (4–5) | 0.98 (0.97–0.99) | <0.001 | 4 (4–5) | 0.98 (0.97–0.99) | <0.001 | 0.99 (0.98–0.99) | <0.001 |
| ADMIRE 2 | 5 (4–5) | 0.95 (0.92–0.97) | <0.001 | 5 (4–5) | 0.96 (0.95–0.98) | <0.001 | 0.96 (0.95–0.98) | <0.001 | ||
| wFBP + PS | 5 (4–5) | 0.82 (0.74–0.88) | <0.001 | 5 (4–5) | 0.89 (0.84–0.93) | <0.001 | 0.84 (0.78–0.90) | <0.001 | ||
| ADMIRE 2 + PS | 5 (5–5) | 0.91 (0.86–0.94) | <0.001 | 5 (4–5) | 0.91 (0.87–0.94) | <0.001 | 0.85 (0.79–0.90) | <0.001 | ||
| 50% | wFBP | 3 (3–4) | 0.99 (0.98–0.99) | <0.001 | 3 (3–4) | 0.98 (0.97–0.99) | <0.001 | 0.99 (0.98–0.99) | <0.001 | |
| ADMIRE 2 | 4 (3–4) | 0.96 (0.94–0.97) | <0.001 | 4 (3–4) | 0.95 (0.93–0.97) | <0.001 | 0.97 (0.96–0.98) | <0.001 | ||
| wFBP + PS | 4 (4–5) | 0.92 (0.88–0.95) | <0.001 | 4 (4–5) | 0.91 (0.88–0.94) | <0.001 | 0.84 (0.77–0.89) | <0.001 | ||
| ADMIRE 2 + PS | 4 (4–5) | 0.94 (0.92–0.96) | <0.001 | 4 (4–5) | 0.83 (0.75–0.89) | <0.001 | 0.88 (0.83–0.92) | <0.001 | ||
| 40% | wFBP | 2 (2–3) | 0.99 (0.99–1.00) | <0.001 | 2 (2–3) | 0.98 (0.96–0.98) | <0.001 | 0.99 (0.98–0.99) | <0.001 | |
| ADMIRE 2 | 3 (2–3) | 0.98 (0.97–0.99) | <0.001 | 3 (2–3) | 0.95 (0.92–0.97) | <0.001 | 0.97 (0.96–0.98) | <0.001 | ||
| wFBP + PS | 4 (4–5) | 0.92 (0.88–0.94) | <0.001 | 4 (4–5) | 0.86 (0.80–0.91) | <0.001 | 0.86 (0.80–0.91) | <0.001 | ||
| ADMIRE 2 + PS | 4 (4–5) | 0.93 (0.89–0.95) | <0.001 | 4 (4–5) | 0.9 (0.85–0.93) | <0.001 | 0.85 (0.79–0.90) | <0.001 | ||
| 30% | wFBP | 1 (1–2) | 0.98 (0.97–0.99) | <0.001 | 1 (1–2) | 0.97 (0.96–0.98) | <0.001 | 0.99 (0.99–0.99) | <0.001 | |
| ADMIRE 2 | 2 (1–2) | 0.96 (0.94–0.97) | <0.001 | 2 (1–2) | 0.93 (0.89–0.95) | <0.001 | 0.98 (0.97–0.99) | <0.001 | ||
| wFBP + PS | 4 (4–5) | 0.86 (0.80–0.91) | <0.001 | 4 (4–5) | 0.92 (0.88–0.95) | <0.001 | 0.87 (0.82–0.91) | <0.001 | ||
| ADMIRE 2 + PS | 4 (4–5) | 0.92 (0.88–0.95) | <0.001 | 4 (4–5) | 0.95 (0.92–0.96) | <0.001 | 0.93 (0.90–0.95) | <0.001 | ||
| Variable | B | SE | 95% CI | |t| | p |
|---|---|---|---|---|---|
| Intercept | 1.21 | 0.06 | 1.09–1.33 | 20.1 | <0.001 |
| ED (reference: 30%) | |||||
| 40% | 0.78 | 0.08 | 0.63–0.93 | 10.1 | <0.001 |
| 50% | 1.78 | 0.08 | 1.63–1.93 | 23 | <0.001 |
| 100% | 2.78 | 0.08 | 2.63–2.93 | 35.9 | <0.001 |
| Scanner (reference: SOMATOM Definition AS+) | |||||
| SOMATOM Force | 0.22 | 0.07 | 0.09–0.35 | 3.26 | 0.053 |
| Mode (reference: wFBP) | |||||
| ADMIRE 2 | 0.04 | 0.08 | −0.11–0.2 | 0.58 | 0.564 |
| ADMIRE 2 + PS | 2.88 | 0.08 | 2.72–3.03 | 37.2 | <0.001 |
| wFBP + PS | 3.06 | 0.08 | 2.91–3.21 | 39.6 | <0.001 |
| Rater (reference: Rater 1) | |||||
| Rater 2 | 0.01 | 0.08 | –0.16–0.16 | 0 | >0.999 |
| Rater 3 | 0.01 | 0.08 | –0.16–0.16 | 0 | >0.999 |
| Rater 4 | 0.01 | 0.08 | –0.14–0.17 | 0.15 | 0.882 |
| Rater 5 | 0.01 | 0.08 | –0.16–0.16 | 0 | >0.999 |
| Timepoint (reference: Timepoint 1) | |||||
| Timepoint 2 | 0.03 | 0.07 | –0.1–0.16 | 0.46 | 0.648 |
| Noise | p (Two-Sided, Adjusted) vs. 100% ED | ||||||
|---|---|---|---|---|---|---|---|
| ED | Mode | Mean ± SD | wFBP | ADMIRE 2 | wFBP + PS | ADMIRE 2 + PS | |
| SOMATOM Definition AS+ | 100% | wFBP | 12.85 ± 1.63 | <0.001 | <0.001 | <0.001 | |
| ADMIRE 2 | 10.75 ± 1.36 | <0.001 | <0.001 | <0.001 | |||
| wFBP + PS | 7.8 ± 0.13 | <0.001 | <0.001 | 0.423 | |||
| ADMIRE 2 + PS | 7.8 ± 0.13 | <0.001 | <0.001 | 0.423 | |||
| 50% | wFBP | 17.99 ± 2.51 | <0.001 | <0.001 | <0.001 | <0.001 | |
| ADMIRE 2 | 15.05 ± 2.11 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| wFBP + PS | 7.8 ± 0.15 | <0.001 | <0.001 | 0.936 | 0.943 | ||
| ADMIRE 2 + PS | 7.8 ± 0.15 | <0.001 | <0.001 | 0.860 | 0.991 | ||
| 40% | wFBP | 20.06 ± 2.89 | <0.001 | <0.001 | <0.001 | <0.001 | |
| ADMIRE 2 | 16.78 ± 2.42 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| wFBP + PS | 7.8 ± 0.18 | <0.001 | <0.001 | 0.947 | 0.941 | ||
| ADMIRE 2 + PS | 7.8 ± 0.17 | <0.001 | <0.001 | 0.963 | 0.969 | ||
| 30% | wFBP | 23.07 ± 3.46 | <0.001 | <0.001 | <0.001 | <0.001 | |
| ADMIRE 2 | 19.29 ± 2.89 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| wFBP + PS | 7.8 ± 0.2 | <0.001 | <0.001 | 0.980 | 0.981 | ||
| ADMIRE 2 + PS | 7.8 ± 0.2 | <0.001 | <0.001 | 0.979 | 0.969 | ||
| SOMATOM Force | 100% | wFBP | 12.35 ± 1.57 | <0.001 | <0.001 | <0.001 | <0.001 |
| ADMIRE 2 | 10.73 ± 1.36 | <0.001 | <0.001 | <0.001 | |||
| wFBP + PS | 7.8 ± 0.13 | <0.001 | <0.001 | 0.422 | |||
| ADMIRE 2 + PS | 7.8 ± 0.12 | <0.001 | <0.001 | 0.422 | |||
| 50% | wFBP | 17.29 ± 2.42 | <0.001 | <0.001 | <0.001 | <0.001 | |
| ADMIRE 2 | 15.02 ± 2.11 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| wFBP + PS | 7.8 ± 0.15 | <0.001 | <0.001 | 0.927 | 0.807 | ||
| ADMIRE 2 + PS | 7.8 ± 0.14 | <0.001 | <0.001 | 0.920 | 0.927 | ||
| 40% | wFBP | 19.27 ± 2.78 | <0.001 | <0.001 | <0.001 | <0.001 | |
| ADMIRE 2 | 16.74 ± 2.41 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| wFBP + PS | 7.8 ± 0.17 | <0.001 | <0.001 | 0.930 | 0.868 | ||
| ADMIRE 2 + PS | 7.8 ± 0.17 | <0.001 | <0.001 | 0.936 | 0.895 | ||
| 30% | wFBP | 22.17 ± 3.32 | <0.001 | <0.001 | <0.001 | <0.001 | |
| ADMIRE 2 | 19.26 ± 2.89 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| wFBP + PS | 7.8 ± 0.19 | <0.001 | <0.001 | 0.936 | 0.897 | ||
| ADMIRE 2 + PS | 7.8 ± 0.19 | <0.001 | <0.001 | 0.978 | 0.978 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brendlin, A.S.; Plajer, D.; Chaika, M.; Wrazidlo, R.; Estler, A.; Tsiflikas, I.; Artzner, C.P.; Afat, S.; Bongers, M.N. AI Denoising Significantly Improves Image Quality in Whole-Body Low-Dose Computed Tomography Staging. Diagnostics 2022, 12, 225. https://doi.org/10.3390/diagnostics12010225
Brendlin AS, Plajer D, Chaika M, Wrazidlo R, Estler A, Tsiflikas I, Artzner CP, Afat S, Bongers MN. AI Denoising Significantly Improves Image Quality in Whole-Body Low-Dose Computed Tomography Staging. Diagnostics. 2022; 12(1):225. https://doi.org/10.3390/diagnostics12010225
Chicago/Turabian StyleBrendlin, Andreas S., David Plajer, Maryanna Chaika, Robin Wrazidlo, Arne Estler, Ilias Tsiflikas, Christoph P. Artzner, Saif Afat, and Malte N. Bongers. 2022. "AI Denoising Significantly Improves Image Quality in Whole-Body Low-Dose Computed Tomography Staging" Diagnostics 12, no. 1: 225. https://doi.org/10.3390/diagnostics12010225
APA StyleBrendlin, A. S., Plajer, D., Chaika, M., Wrazidlo, R., Estler, A., Tsiflikas, I., Artzner, C. P., Afat, S., & Bongers, M. N. (2022). AI Denoising Significantly Improves Image Quality in Whole-Body Low-Dose Computed Tomography Staging. Diagnostics, 12(1), 225. https://doi.org/10.3390/diagnostics12010225