
The Prognostic Value of ADAMTS-13 and von Willebrand Factor in COVID-19 Patients: Prospective Evaluation by Care Setting



 , and
, and  on behalf of the CSS COVID-19 Group
on behalf of the CSS COVID-19 Group
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Methodology and Setting
2.2. Sample Preparation and Plasma-Based Determinations
2.3. Data Analysis
3. Results
3.1. Demographic/Clinical Information and Laboratory Data
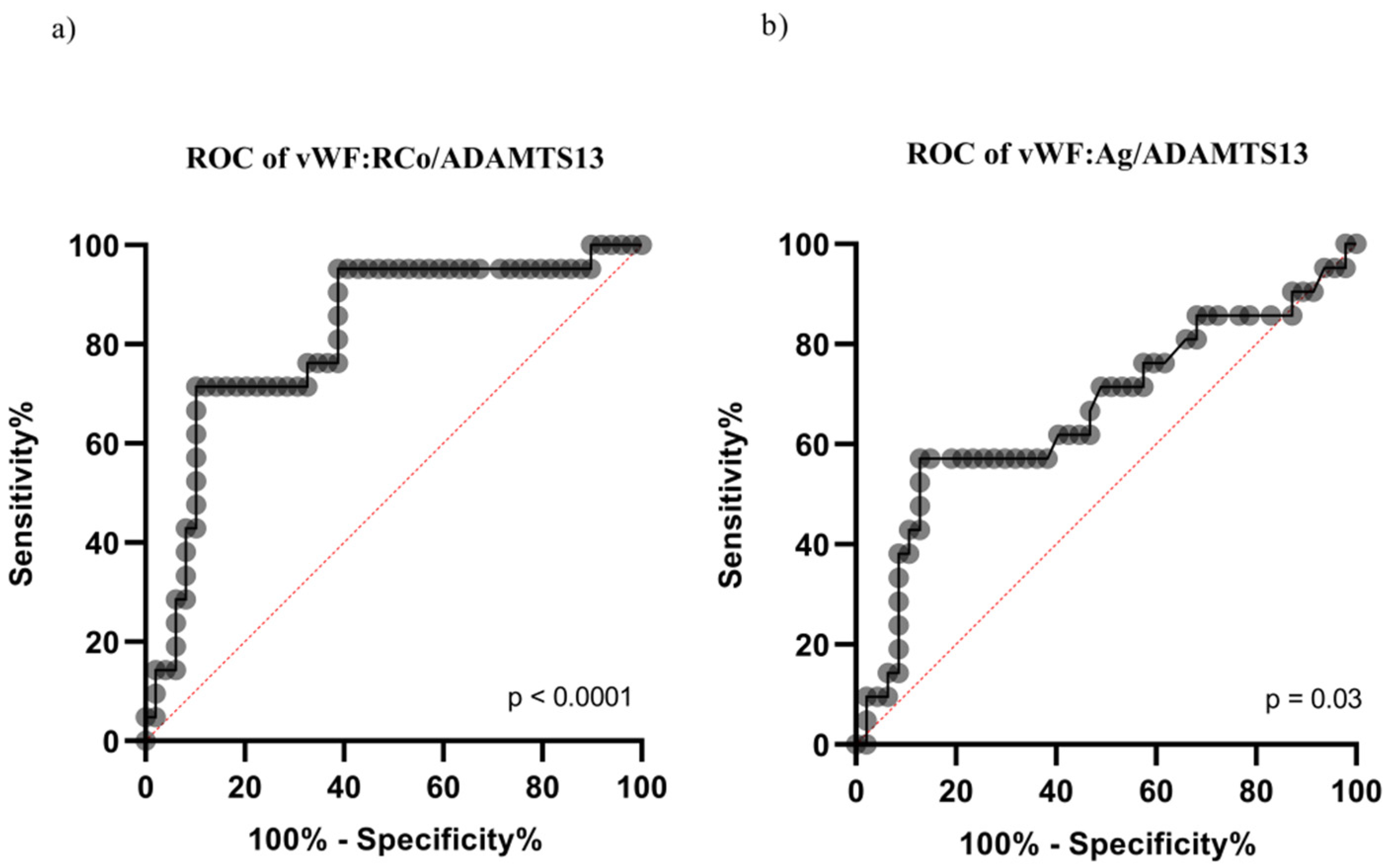
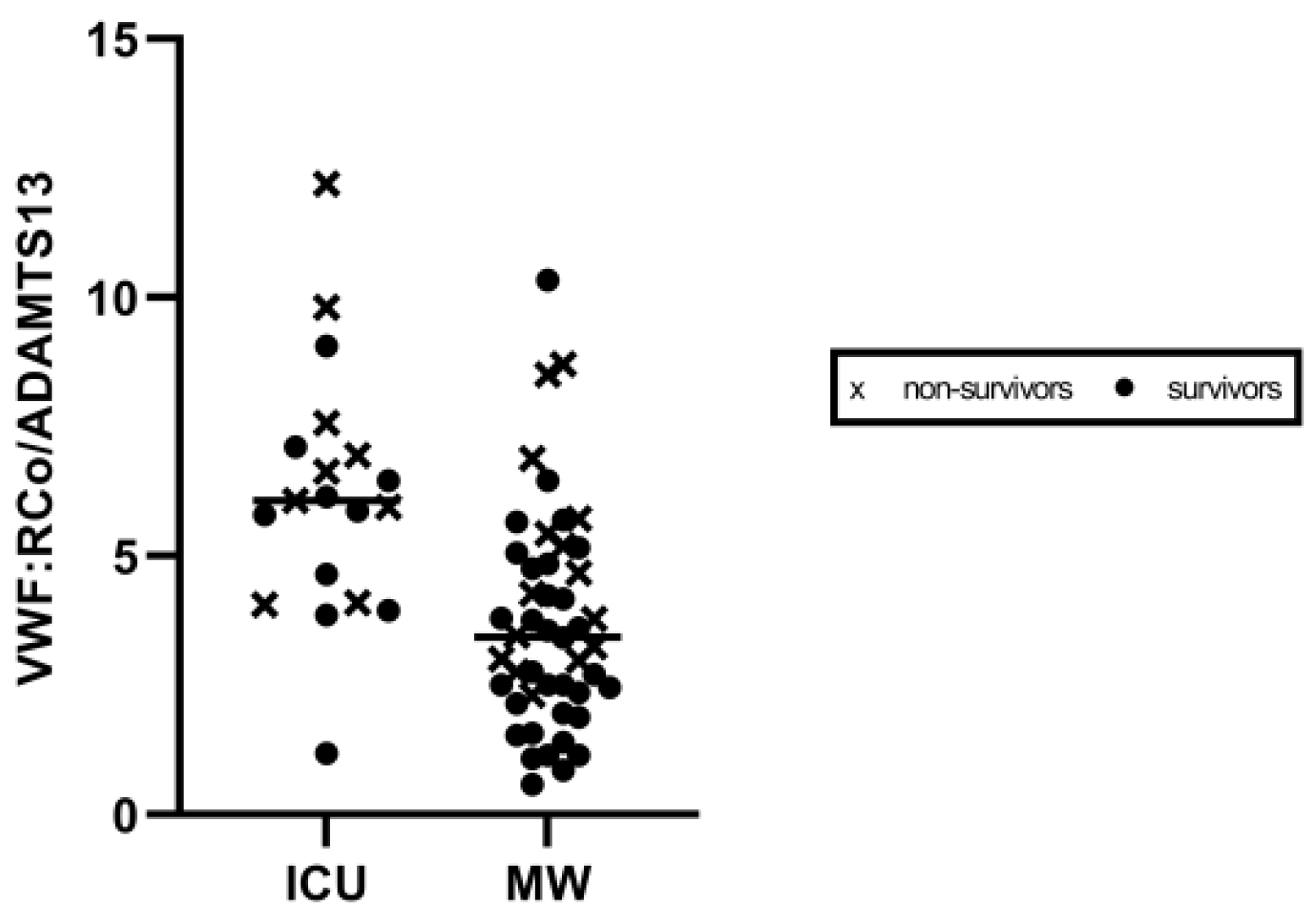
3.2. VWF/ADAMTS-13 Fraction by Care Setting
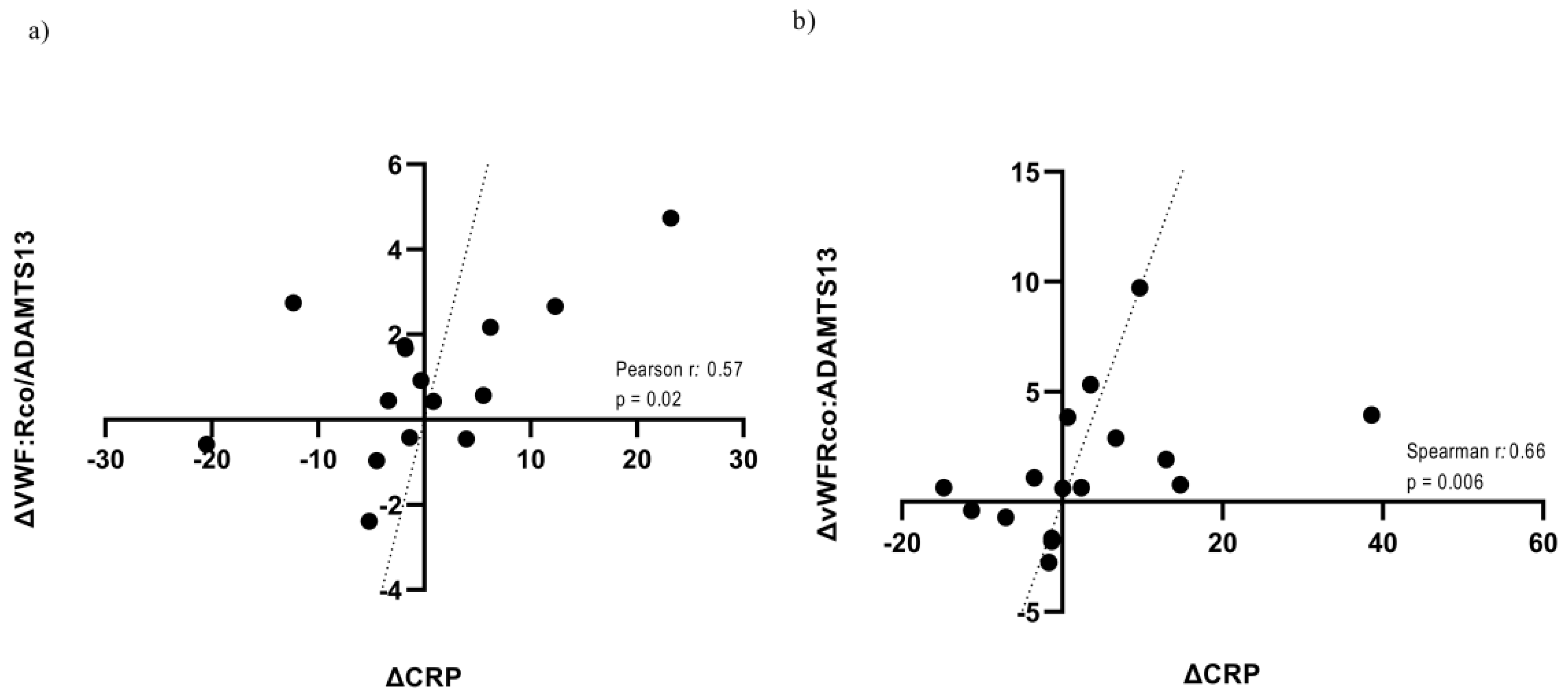
3.3. Correlation between VWF/ADAMTS-13 and Routine Blood Parameters: Data from the Prospective Cohort
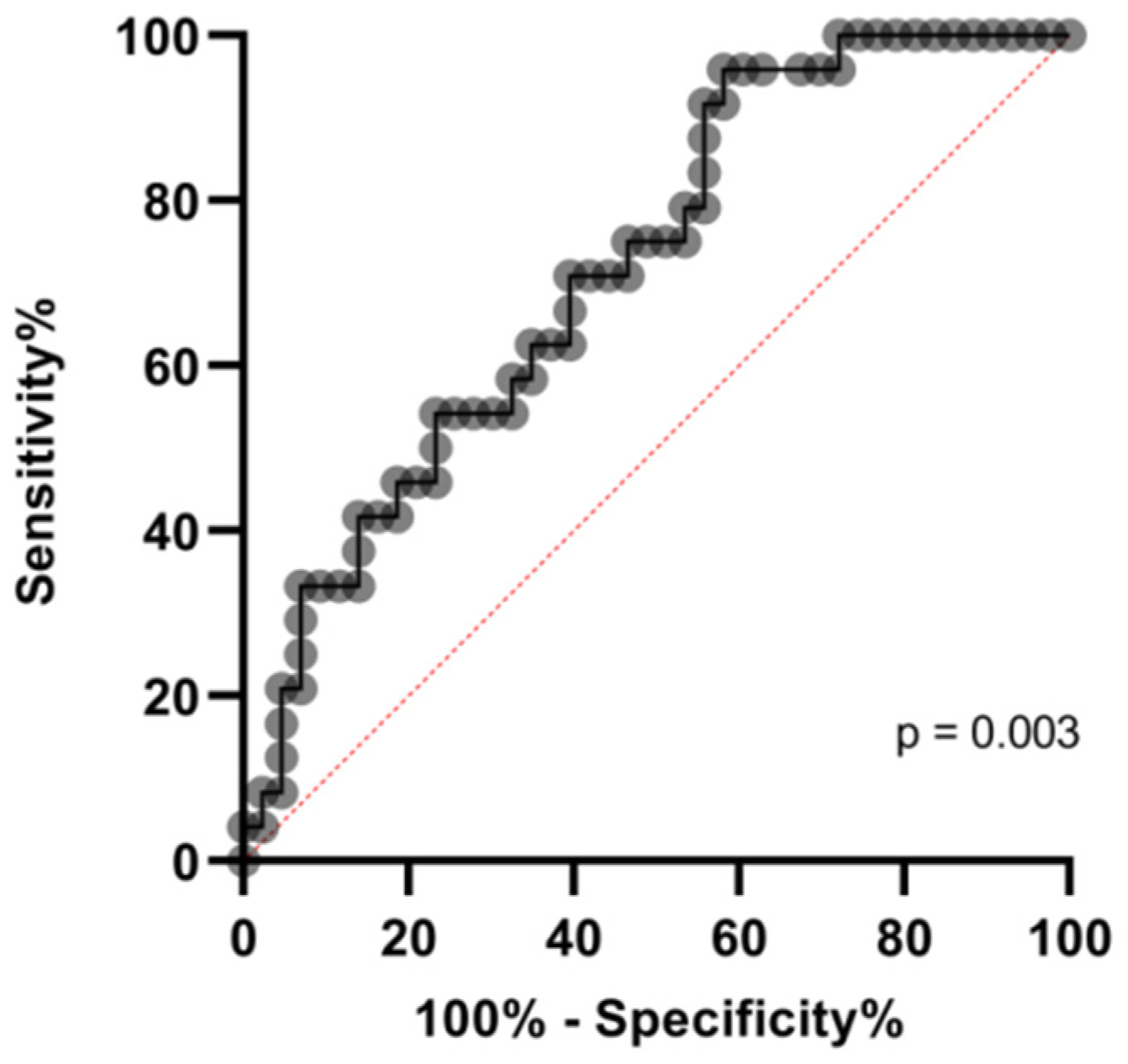
3.4. VWF/ADAMTS-13 and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lippi, G.; Plebani, M. Laboratory abnormalities in patients with COVID-2019 infection. Clin. Chem. Lab. Med. 2020, 5, 1131–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peiró, Ó.M.; Carrasquer, A.; Sánchez-Gimenez, R.; Lal-Trehan, N.; Del-Moral-Ronda, V.; Bonet, G.; Fort-Gallifa, I.; Picó-Plana, E.; Bastón-Paz, N.; Gutiérrez, C.; et al. Biomarkers and short-term prognosis in COVID-19. Biomarkers 2021, 26, 119–126. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Guler, N.; Siddiqui, F.; Fareed, J. Is the Reason of Increased D-Dimer Levels in COVID-19 Because of ACE-2-Induced Apoptosis in Endothelium? Clin. Appl. Thromb. Hemost. 2020, 26. [Google Scholar] [CrossRef] [PubMed]
- Ladikou, E.E.; Sivaloganathan, H.; Milne, K.M.; Arter, W.E.; Ramasamy, R.; Saad, R.; Stoneham, S.M.; Philips, B.; Eziefula, A.C.; Chevassut, T. Von Willebrand factor (vWF): Marker of endothelial damage and thrombotic risk in COVID-19? Clin. Med. 2020, 20, e178–e182. [Google Scholar] [CrossRef] [PubMed]
- Philippe, A.; Chocron, R.; Gendron, N.; Bory, O.; Beauvais, A.; Peron, N.; Khider, L.; Guerin, C.L.; Goudot, G.; Levasseur, F.; et al. Circulating Von Willebrand factor and high molecular weight multimers as markers of endothelial injury predict COVID-19 in-hospital mortality. Angiogenesis 2021, 24, 505–517. [Google Scholar] [CrossRef]
- Perico, L.; Benigni, A.; Casiraghi, F.; Ng, L.; Renia, L.; Remuzzi, G. Immunity, endothelial injury and complement-induced coagulopathy in COVID-19. Nat. Rev. Nephrol. 2021, 17, 46–64. [Google Scholar] [CrossRef]
- Mancini, I.; Baronciani, L.; Artoni, A.; Colpani, P.; Biganzoli, M.; Cozzi, G.; Novembrino, C.; Boscolo Anzoletti, M.; De Zan, V.; Pagliari, M.T.; et al. The ADAMTS13-von Willebrand factor axis in COVID-19 patients. JTH 2021, 19, 513–521. [Google Scholar] [CrossRef]
- Bazzan, M.; Montaruli, B.; Sciascia, S.; Cosseddu, D.; Norbiato, C.; Roccatello, D. Low ADAMTS 13 plasma levels are predictors of mortality in COVID-19 patients. Intern. Emerg. Med. 2020, 15, 861–863. [Google Scholar] [CrossRef]
- Tiscia, G.L.; Favuzzi, G.; De Laurenzo, A.; Cappucci, F.; Fischetti, L.; di Mauro, L.; Miscio, G.; Mirijello, A.; Chinni, E.; Grandone, E.; et al. Reduction of ADAMTS13 Levels Predicts Mortality in SARS-CoV-2 Patients. TH Open 2020, 4, e203–e206. [Google Scholar] [CrossRef]
- Ono, T.; Mimuro, J.; Madoiwa, S.; Soejima, K.; Kashiwakura, Y.; Ishiwata, A.; Takano, K.; Ohmori, T.; Sakata, Y. Severe secondary deficiency of von Willebrand factor-cleaving protease (ADAMTS13) in patients with sepsis-induced disseminated intravascular coagulation: Its correlation with development of renal failure. Blood 2006, 107, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Tiscia, G.L.; Ostuni, A.; Cascavilla, N.; Cappucci, F.; Scalzulli, P.; Battista, C.; Abrescia, A.; Aucella, F.; Buquicchio, C.; Brigante, M.; et al. Validation of PLASMIC score and follow-up data in a cohort of patients with suspected microangiopathies from Southern Italy. J. Thromb. Thrombolysis 2018, 46, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Pascreau, T.; Zia-Chahabi, S.; Zuber, B.; Tcherakian, C.; Farfour, E.; Vasse, M. ADAMTS 13 deficiency is associated with abnormal distribution of von Willebrand factor multimers in patients with COVID-19. Thromb. Res. 2021, 204, 138–240. [Google Scholar] [CrossRef]
- Turecek, P.L.; Peck, R.C.; Rangarajan, S.; Reilly-Stitt, C.; Laffan, M.A.; Kazmi, R.; James, I.; Dushianthan, A.; Schrenk, G.; Gritsch, H.; et al. Recombinant ADAMTS13 reduces abnormally up-regulated von Willebrand factor in plasma from patients with severe COVID-19. Thromb. Res. 2021, 201, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Vasileiadis, I.; Politou, M.; Dimopoulos, S.; Rovina, N.; Kyriakopoulou, M.; Kyriakoudi, A.; Tripodaki, E.S.; Koutsouri, T.; Terpos, E.; Koulouris, N.; et al. Variation of endothelium-related hemostatic factors during sepsis. Microcirculation 2018, 25, e12500. [Google Scholar] [CrossRef] [PubMed]
- Kremer Hovinga, J.A.; Zeerleder, S.; Kessler, P.; Romani de Wit, T.; van Mourik, J.A.; Hack, C.E.; ten Cate, H.; Reitsma, P.H.; Wuillemin, W.A.; Lämmle, B. ADAMTS-13, von Willebrand factor and related parameters in severe sepsis and septic shock. JTH 2007, 5, 2284–2290. [Google Scholar] [CrossRef]
- Levi, M.; Scully, M.; Singer, M. The role of ADAMTS-13 in the coagulopathy of sepsis. JTH 2018, 16, 646–651. [Google Scholar] [CrossRef]
- Wagner, D.D. The Weibel-Palade body: The storage granule for von Willebrand factor and P-selectin. Thromb. Haemost. 1993, 70, 105–110. [Google Scholar] [CrossRef]
- Libby, P.; Lüscher, T. COVID-19 is, in the end, an endothelial disease. Eur. Heart. J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef] [PubMed]
- Escher, R.; Breakey, N.; Lämmle, B. Severe COVID-19 infection associated with endothelial activation. Thromb. Res. 2020, 190, 62. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.X.; Tyagi, T.; Jain, K.; Gu, V.W.; Lee, S.H.; Hwa, J.M.; Kwan, J.M.; Krause, D.S.; Lee, A.I.; Halene, S.; et al. Thrombocytopathy and endotheliopathy: Crucial contributors to COVID-19 thromboinflammation. Nat. Rev. Cardiol. 2021, 18, 194–209. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Favaloro, E.J. D-dimer is Associated with Severity of Coronavirus Disease 2019: A Pooled Analysis. Thromb. Haem. 2020, 120, 876–878. [Google Scholar] [CrossRef] [Green Version]
- Hachim, M.Y.; Hachim, I.Y.; Naeem, K.B.; Hannawi, H.; Salmi, I.A.; Hannawi, S. D-dimer, Troponin, and Urea Level at Presentation with COVID-19 can Predict ICU Admission: A Single Centered Study. Front. Med. 2020, 7, 585003. [Google Scholar] [CrossRef] [PubMed]
- Póvoa, P. C-reactive protein: A valuable marker of sepsis. Intensive Care Med. 2002, 28, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Foley, J.H.; Conway, E.M. Cross Talk Pathways Between Coagulation and Inflammation. Circ. Res. 2016, 118, 1392–1408. [Google Scholar] [CrossRef]
- Camerer, E.; Huang, W.; Coughlin, S.R. Tissue factor- and factor X-dependent activation of protease-activated receptor 2 by factor VIIa. Proc. Natl. Acad. Sci. USA 2000, 97, 5255–5260. [Google Scholar] [CrossRef] [Green Version]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Tassiopoulos, A.K.; Mofakham, S.; Rubano, J.A.; Labropoulos, N.; Bannazadeh, M.; Drakos, P.; Volteas, P.; Cleri, N.A.; Alkadaa, L.N.; Asencio, A.A.; et al. D-Dimer-Driven Anticoagulation Reduces Mortality in Intubated COVID-19 Patients: A Cohort Study with a Propensity-Matched Analysis. Front. Med. 2021, 8, 631335. [Google Scholar] [CrossRef]
- Gragnano, F.; Sperlongano, S.; Golia, E.; Natale, F.; Bianchi, R.; Crisci, M.; Fimiani, F.; Pariggiano, I.; Diana, V.; Carbone, A.; et al. The Role of von Willebrand Factor in Vascular Inflammation: From Pathogenesis to Targeted Therapy. Mediat. Inflamm. 2017, 2017, 5620314. [Google Scholar] [CrossRef]
- Tiwari, N.R.; Phatak, S.; Sharma, V.R.; Agarwal, S.K. COVID-19 and thrombotic microangiopathies. Thromb. Res. 2021, 202, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Aldecoa, C.; Llau, J.V.; Nuvials, X.; Artigas, A. Role of albumin in the preservation of endothelial glycocalyx integrity and the microcirculation: A review. Ann. Intensive Care. 2020, 10, 85. [Google Scholar] [CrossRef] [PubMed]
- Folsom, A.R.; Lutsey, P.L.; Heckbert, S.R.; Cushman, M. Serum albumin and risk of venous thromboembolism. Thromb. Haeost. 2010, 104, 100–104. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.L.; Dubois, M.J.; Navickis, R.J.; Wilkes, M.M. Hypoalbuminemia in acute illness: Is there a rationale for intervention? A meta-analysis of cohort studies and controlled trials. Ann. Surg. 2003, 237, 319–334. [Google Scholar] [CrossRef]
- Kheir, M.; Saleem, F.; Wang, C.; Mann, A.; Chua, J. Higher albumin levels on admission predict better prognosis in patients with confirmed COVID-19. PLoS ONE 2021, 16, e0248358. [Google Scholar] [CrossRef]
- Kendall, H.; Abreu, E.; Cheng, A.L. Serum Albumin Trend Is a Predictor of Mortality in ICU Patients with Sepsis. Biol. Res. Nurs. 2019, 21, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Ramadori, G. Albumin Infusion in Critically Ill COVID-19 Patients: Hemodilution and Anticoagulation. Int. J. Mol. Sci. 2021, 22, 7126. [Google Scholar] [CrossRef]
- Violi, F.; Cangemi, R.; Romiti, G.F.; Ceccarelli, G.; Oliva, A.; Alessandri, F.; Pirro, M.; Pignatelli, P.; Lichtner, M.; Carraro, A.; et al. Is Albumin Predictor of Mortality in COVID-19? Antioxid. Redox Signal. 2021, 35, 39–142. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All, n = 74 | ICU, n = 22 | Medical Ward, n = 52 | p Value |
|---|---|---|---|---|
| Age, years, (IQR) | 68.0 (22.0) | 63.0 (15.2) | 69.0 (19.7) | 0.03 |
| Male, n (%) | 43 (58) | 17 (77) | 26 (50) | 0.02 |
| Deaths, n (%) | 26 (35.0) | 10 (45.5) | 16 (30.7) | 0.19 |
| Invasive ventilation, n (%) | 11 (15) | 11 (50) | 0 (0) | <0.0001 |
| Non-invasive ventilation, n (%) | 30 (40.5) | 11 (50) | 19 (36.5) | 0.31 |
| Diabetes, n (%) | 15 (20) | 6 (27.3) | 9 (17.3) | 0.35 |
| Hypertension, n (%) | 36 (48.5) | 11 (50) | 25 (48) | 0.90 |
| Chronic Kidney Disease, n (%) | 11 (15) | 6 (27.3) | 6 (11.5) | 0.16 |
| Cardiovascular disease, n (%) | 19 (25.5) | 5 (22.7) | 14 (27) | 0.77 |
| No. of co-morbidities, n (%) | ||||
| 0 | 35 (47) | 7 (32) | 18 (34.5) | 0.99 |
| 1 | 22 (29.7) | 6 (27.0) | 16 (31.0) | 0.31 |
| 2 | 14 (19) | 6 (27.0) | 8 (15.5) | 0.33 |
| 3 | 7 (9.5) | 0 | 7 (13.5) | 0.09 |
| 4 | 4 (5.5) | 2 (9.1) | 2 (3.8) | 0.50 |
| 5 | 2 (2.7) | 1 (4.5) | 1 (2) | 0.50 |
| Red Blood Cells, 1012/L, (IQR) | 4.3 (1.3) | 4.4 (1.0) | 4.3 (1.4) | 0.91 |
| White Blood Cells, 109/L, (IQR) | 7.4 (5.6) | 10.6 (6.5) | 5.8 (4.5) | 0.03 |
| Neutrophil-to-Lymphocyte Ratio, (IQR) | 7.4 (15.4) | 23.0 (24.0) | 4.7 (6.6) | <0.0001 |
| Hemoglobin, g/dL, (IQR) | 12.5 (3.9) | 12.6 (3.6) | 12.3 (3.9) | 0.78 |
| Platelet count, 109/L, (IQR) | 242 (152) | 254 (103) | 238 (183) | 0.48 |
| Lactate Dehydrogenase, U/L, (IQR) | 251.5 (240.0) | 556.0 (512.0) | 222.0 (94.5) | <0.0001 |
| C-Reactive Protein, mg/dL, (IQR) | 5.6 (9.0) | 6.5 (11.4) | 4.9 (8.1) | 0.15 |
| Direct bilirubin, mg/dL, (IQR) | 0.1 (0.1) | 0.2 (0.3) | 0.1 (0.1) | 0.0003 |
| Indirect bilirubin, mg/dL, (IQR) | 0.2 (0.2) | 0.2 (0.2) | 0.2 (0.2) | 0.27 |
| Aspartate transaminase, U/L, (IQR) | 34.0 (27.0) | 38.0 (32.5) | 31.0 (24.5) | 0.06 |
| Alanine transaminase, U/L, (IQR) | 31.0 (35.7) | 32.0 (45.5) | 30.0 (30.0) | 0.045 |
| Creatinine, mg/dL, (IQR) | 0.9 (0.9) | 0.7 (0.8) | 1.0 (1.1) | 0.05 |
| Serum albumin, g/dL, (IQR) | 2.4 (0.6) | 2.4 (0.4) | 2.4 (1.2) | 0.87 |
| Prothrombin Time, INR, (IQR) | 1.1 (0.1) | 1.1 (0.2) | 1.1 (0.2) | 0.58 |
| Partial thromboplastin time, s, (IQR) | 24.8 (4.4) | 22.8 (5.0) | 25.3 (4.0) | 0.03 |
| Fibrinogen, mg/dL, (IQR) | 544.0 (351.5) | 462.5 (260.2) | 636.0 (238.5) | 0.0083 |
| D-dimer, ng/mL, (IQR) | 1364.0 (5051.5) | 11,936.0 (31,569.0) | 1069.0 (2258.0) | <0.0001 |
| Factor VIII, %, (IQR) | 117.8 (68.0) | 146.2 (55.8) | 95.2 (61.9) | 0.0032 |
| Variables | All, n = 74 | ICU, n = 22 | Medical Ward, n = 52 | p Value |
|---|---|---|---|---|
| vWF:Ag, U/dL, (IQR) | 223.2 (207.4) | 494.1 (362.8) | 222.8 (30.4) | 0.07 |
| vWF:RCo, U/dL, (IQR) | 324.1 (265.5) | 439.8 (195.3) | 266.5 (196.8) | <0.0001 |
| ADAMTS-13, U/dL, (IQR) | 80.0 (30.0) | 70.0 (20.0) | 80.0 (30.0) | 0.83 |
| vWF:Ag/ADAMTS-13 fraction, (IQR) | 3.1 (4.0) | 5.7 (5.8) | 2.9 (1.8) | 0.03 |
| vWF:RCo/ADAMTS-13 fraction, (IQR) | 4.1 (3.3) | 6.0 (2.6) | 3.4 (2.7) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiscia, G.; Favuzzi, G.; De Laurenzo, A.; Cappucci, F.; Fischetti, L.; Colaizzo, D.; Chinni, E.; Florio, L.; Miscio, G.; Piscitelli, A.P.; et al. The Prognostic Value of ADAMTS-13 and von Willebrand Factor in COVID-19 Patients: Prospective Evaluation by Care Setting. Diagnostics 2021, 11, 1648. https://doi.org/10.3390/diagnostics11091648
Tiscia G, Favuzzi G, De Laurenzo A, Cappucci F, Fischetti L, Colaizzo D, Chinni E, Florio L, Miscio G, Piscitelli AP, et al. The Prognostic Value of ADAMTS-13 and von Willebrand Factor in COVID-19 Patients: Prospective Evaluation by Care Setting. Diagnostics. 2021; 11(9):1648. https://doi.org/10.3390/diagnostics11091648
Chicago/Turabian StyleTiscia, Giovanni, Giovanni Favuzzi, Antonio De Laurenzo, Filomena Cappucci, Lucia Fischetti, Donatella Colaizzo, Elena Chinni, Lucia Florio, Giuseppe Miscio, Angela Pamela Piscitelli, and et al. 2021. "The Prognostic Value of ADAMTS-13 and von Willebrand Factor in COVID-19 Patients: Prospective Evaluation by Care Setting" Diagnostics 11, no. 9: 1648. https://doi.org/10.3390/diagnostics11091648
APA StyleTiscia, G., Favuzzi, G., De Laurenzo, A., Cappucci, F., Fischetti, L., Colaizzo, D., Chinni, E., Florio, L., Miscio, G., Piscitelli, A. P., Mastroianno, M., & Grandone, E., on behalf of the CSS COVID-19 Group. (2021). The Prognostic Value of ADAMTS-13 and von Willebrand Factor in COVID-19 Patients: Prospective Evaluation by Care Setting. Diagnostics, 11(9), 1648. https://doi.org/10.3390/diagnostics11091648