
Percutaneous Core Needle Biopsy Can Efficiently and Safely Diagnose Most Primary Bone Tumors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
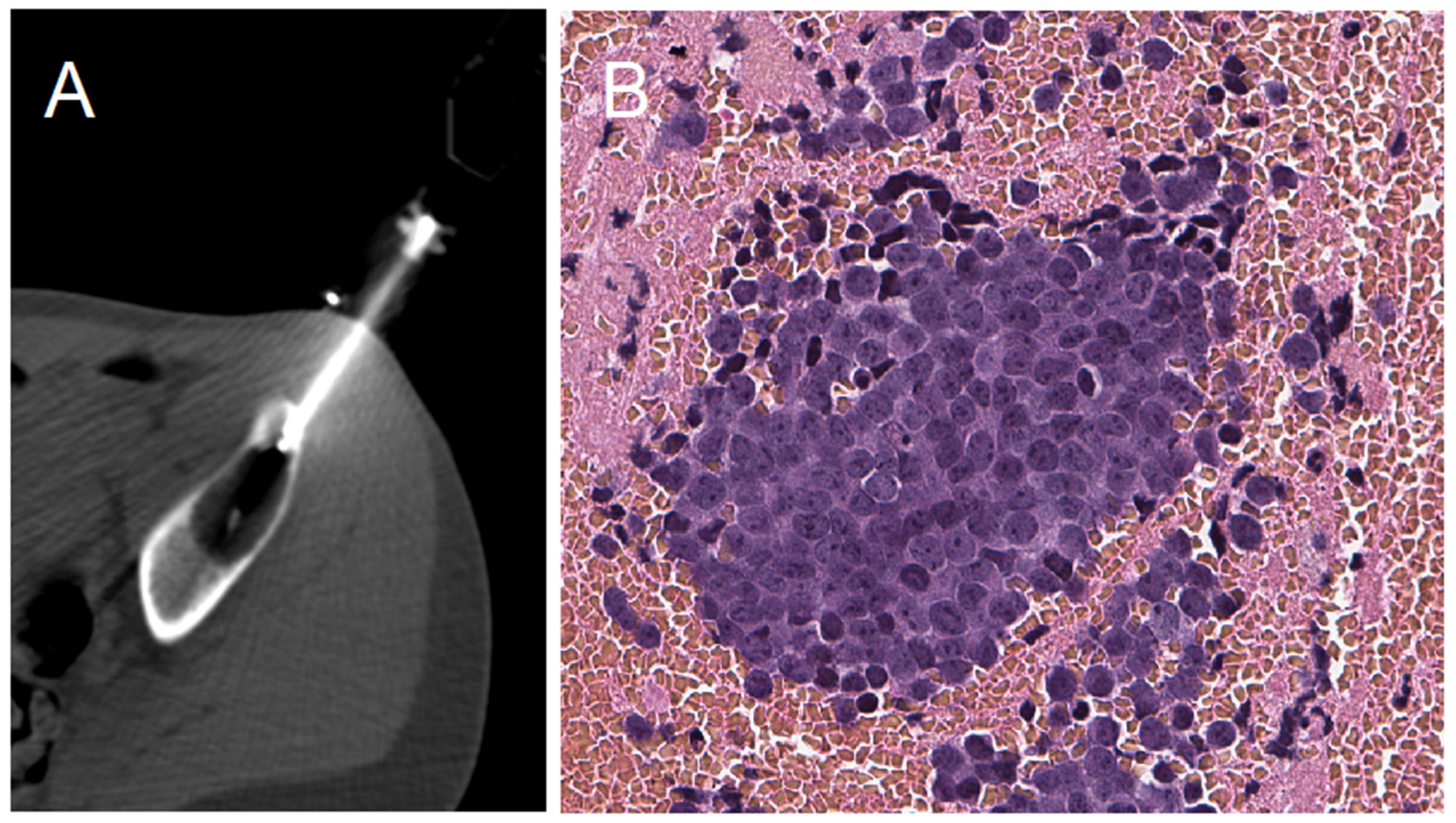
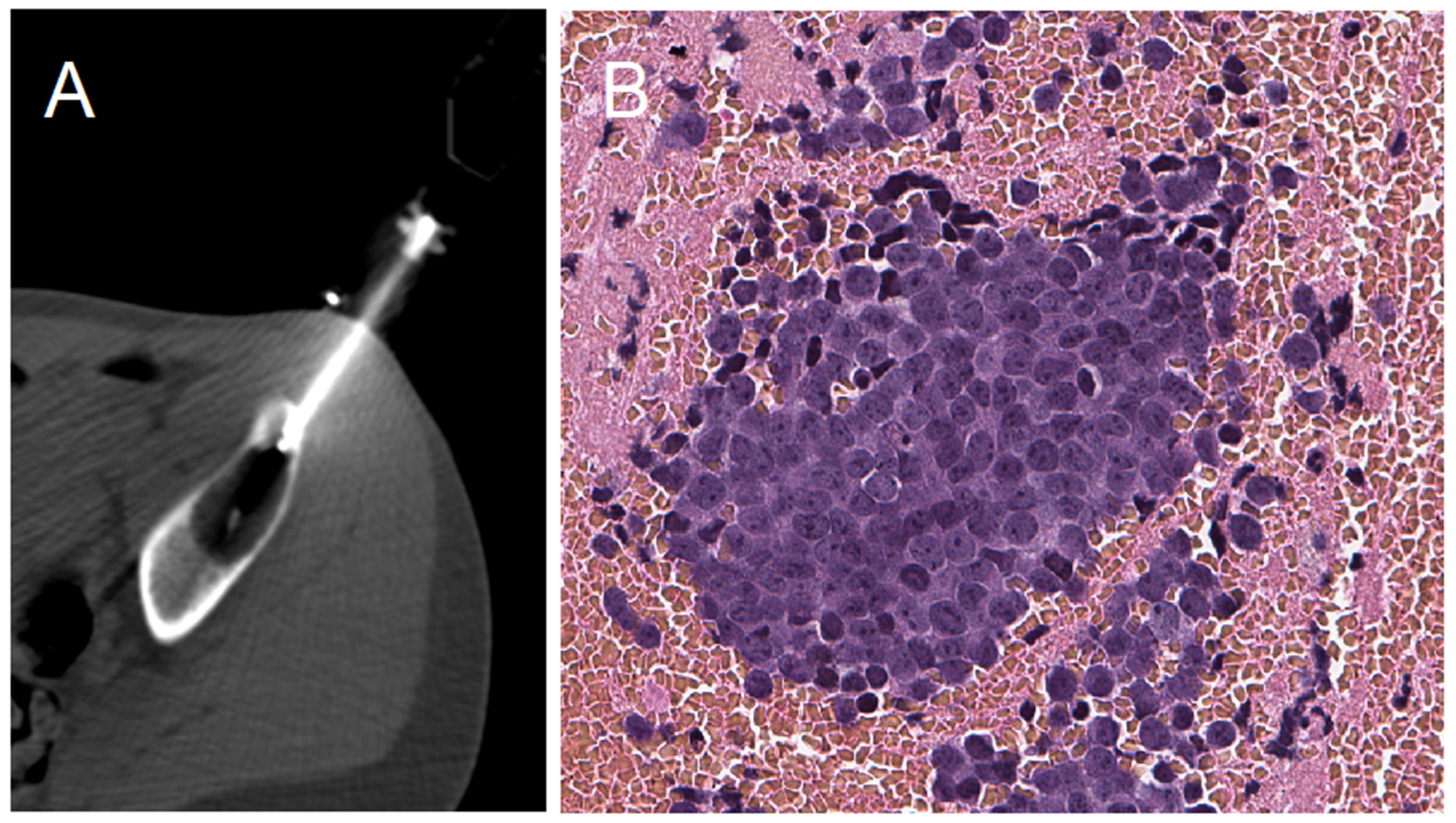
2.2. Biopsy Protocol
2.3. Outcome Measure
2.4. Statistics and Ethics
3. Results
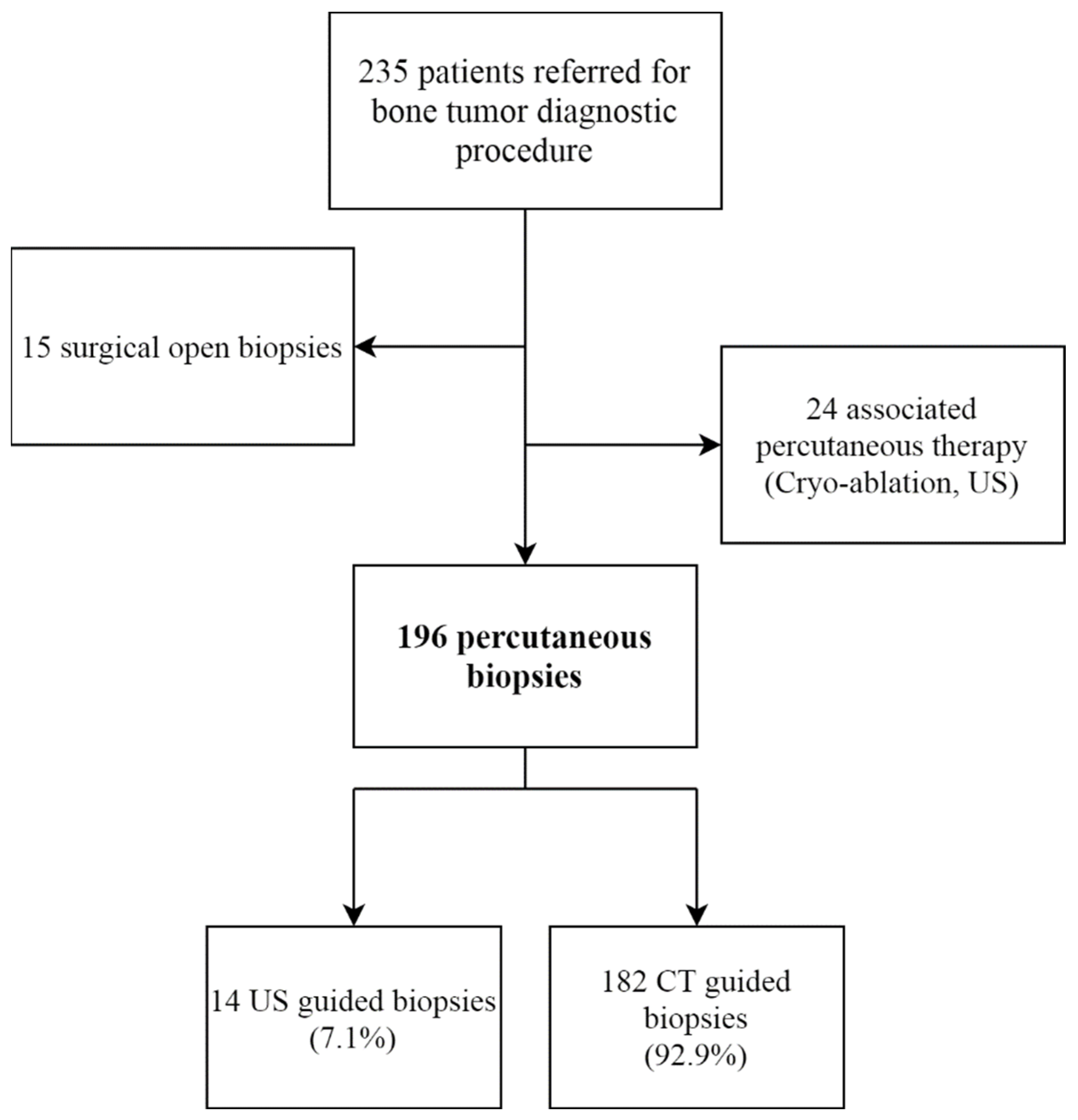
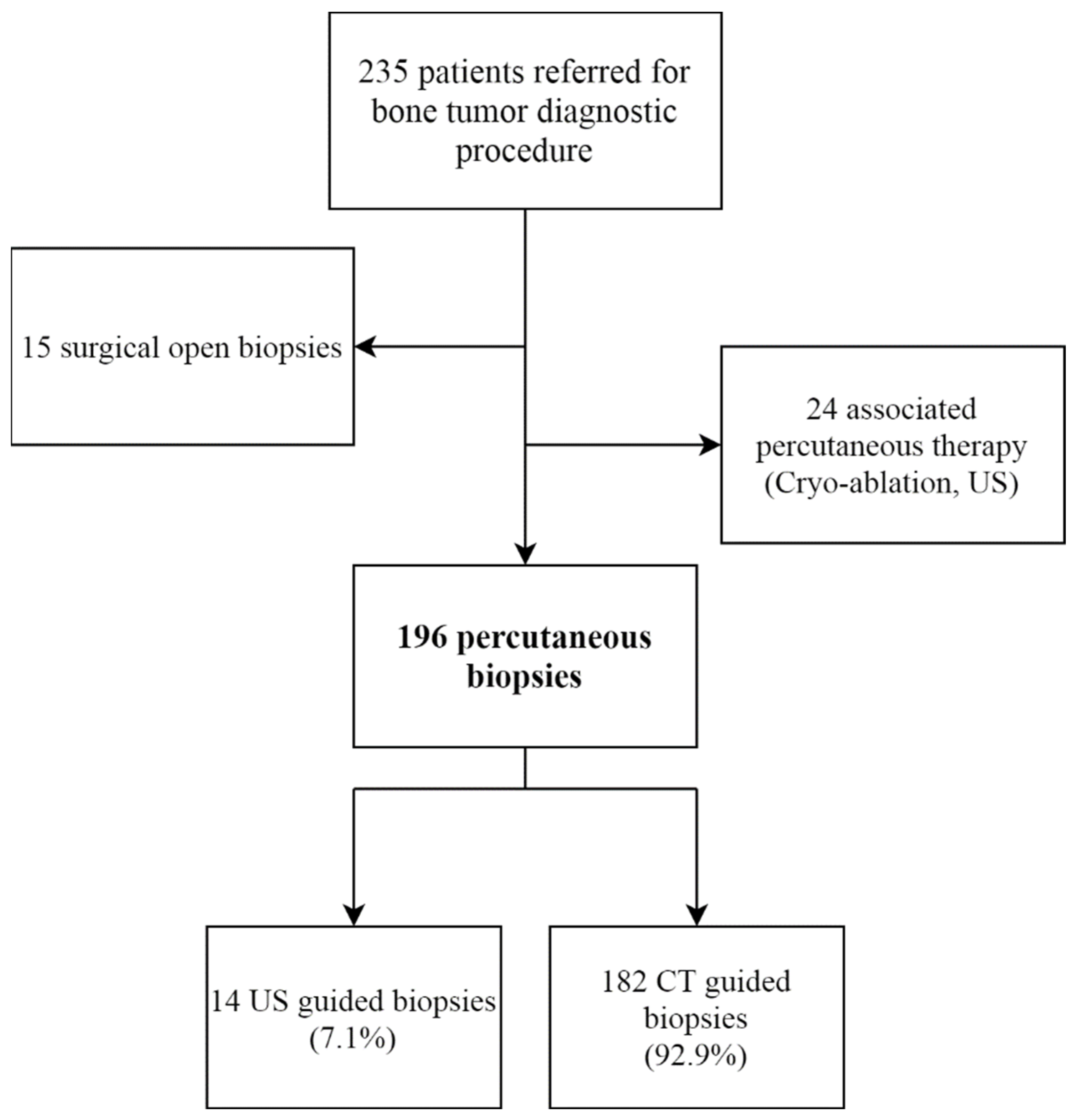
3.1. Study Population
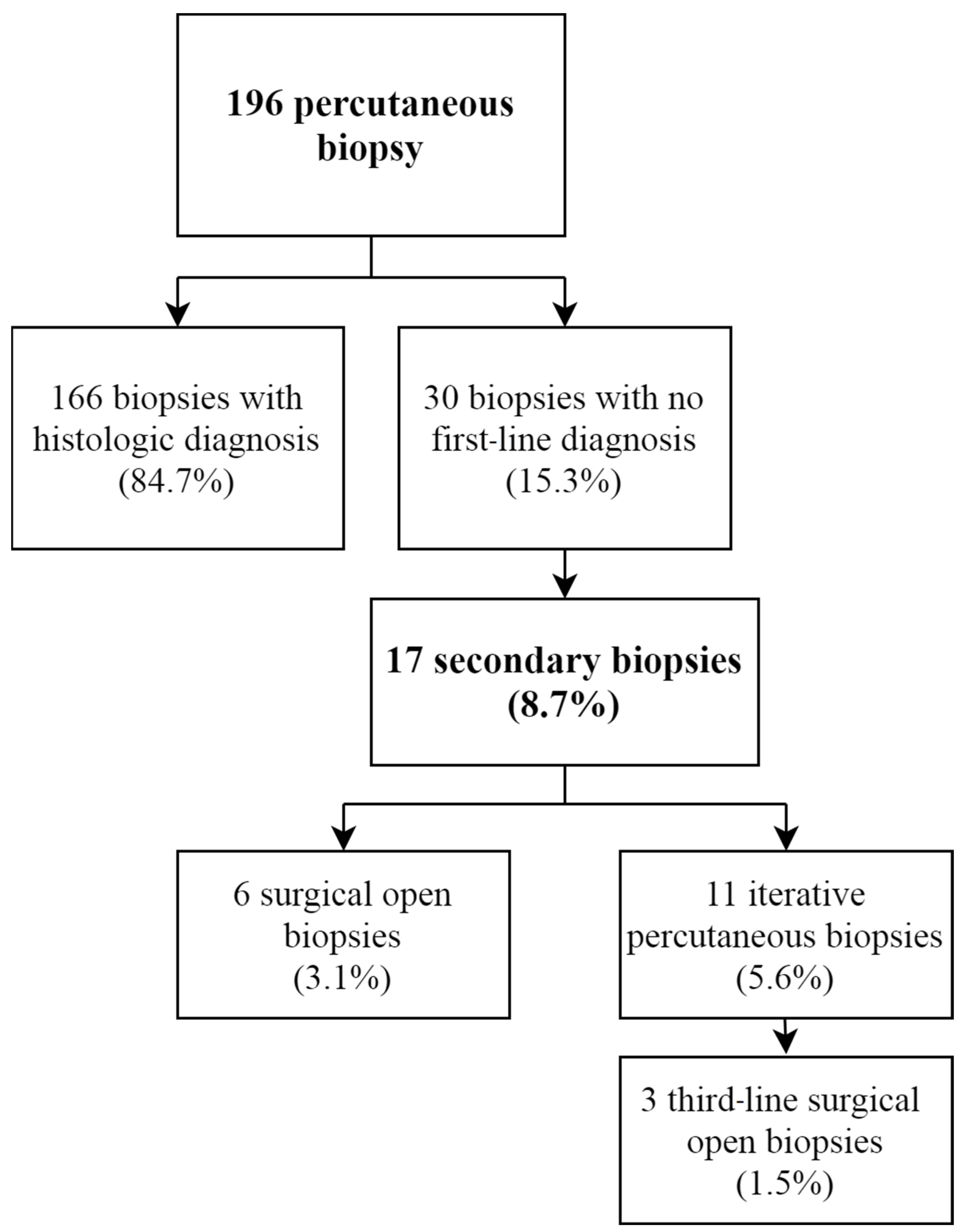
3.2. Diagnostic Yield
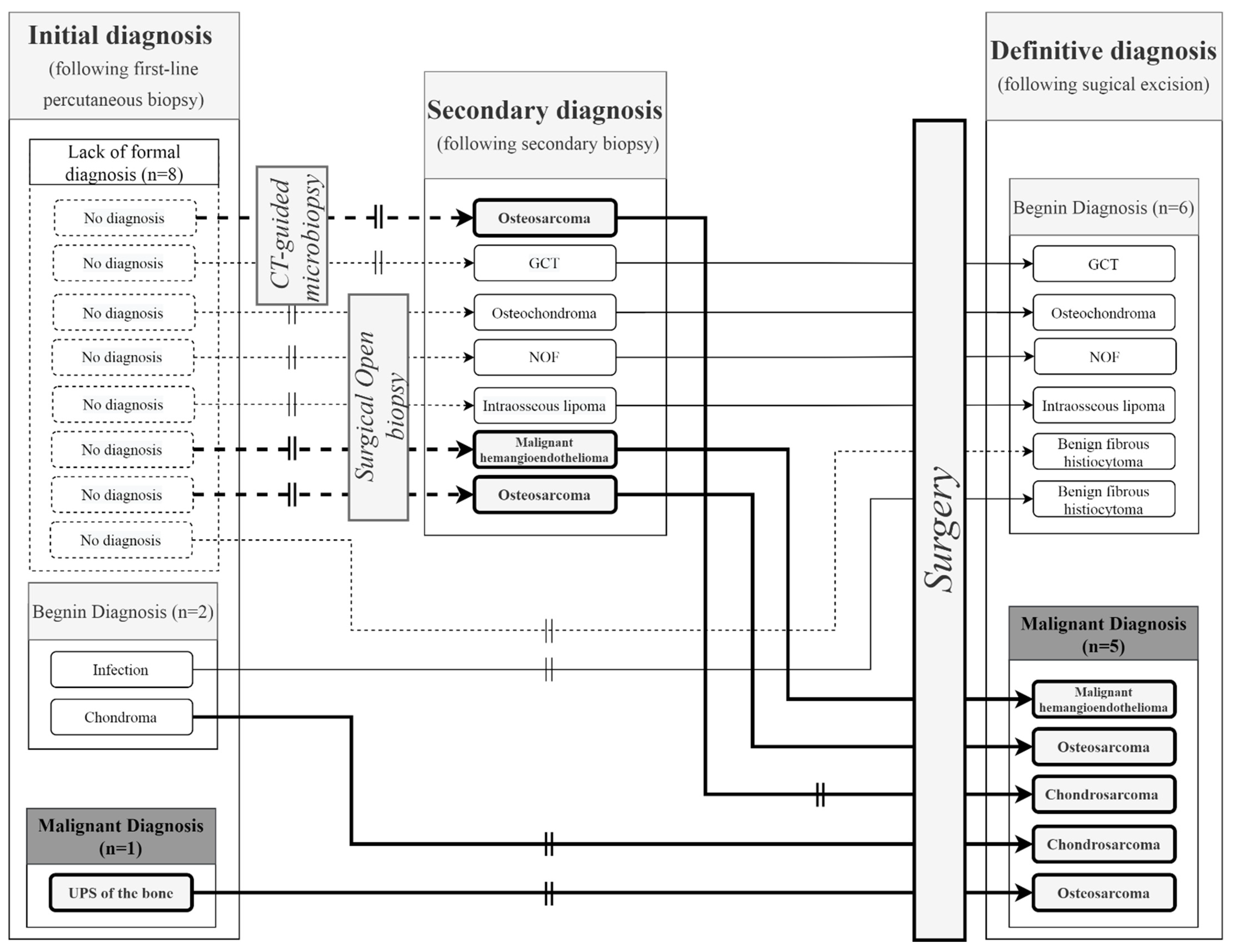
3.3. Diagnostic Accuracy
3.4. Complications
4. Discussion
4.1. Diagnostic Yield
4.2. Diagnostic Accuracy
4.3. Complications
4.4. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Le, H.B.Q.; Lee, S.T.; Munk, P.L. Image-Guided Musculoskeletal Biopsies. Semin. Interv. Radiol. 2010, 27, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Srisawat, P.; Veeraphun, P.; Punyaratabandhu, T.; Chareonvareekul, S.; Songpattanasilpa, T.; Sritanabutr, P.; Pipithkul, S. Comparative Study of Diagnostic Accuracy between Office-Based Closed Needle Biopsy and Open Incisional Biopsy in Patients with Musculoskeletal Sarcomas. J. Med. Assoc. Thai 2014, 97 (Suppl. 2), S30–S38. [Google Scholar] [PubMed]
- Sung, K.-S.; Seo, S.-W.; Shon, M.-S. The Diagnostic Value of Needle Biopsy for Musculoskeletal Lesions. Int. Orthop. 2009, 33, 1701–1706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceraulo, A.; Ouziel, A.; Lavergne, E.; Perrier, L.; Decouvelaere, A.-V.; Chotel, F.; Thiesse, P.; Marec-Berard, P. Percutaneous Guided Biopsy for Diagnosing Suspected Primary Malignant Bone Tumors in Pediatric Patients: A Safe, Accurate, and Cost-Saving Procedure. Pediatr. Radiol. 2017, 47, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Skrzynski, M.C.; Biermann, J.S.; Montag, A.; Simon, M.A. Diagnostic Accuracy and Charge-Savings of Outpatient Core Needle Biopsy Compared with Open Biopsy of Musculoskeletal Tumors. J. Bone Jt. Surg. Am. 1996, 78, 644–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippiadis, D.K.; Charalampopoulos, G.; Mazioti, A.; Keramida, K.; Kelekis, A. Bone and Soft-Tissue Biopsies: What You Need to Know. Semin. Interv. Radiol. 2018, 35, 215–220. [Google Scholar] [CrossRef]
- Rimondi, E.; Rossi, G.; Bartalena, T.; Ciminari, R.; Alberghini, M.; Ruggieri, P.; Errani, C.; Angelini, A.; Calabrò, T.; Abati, C.N.; et al. Percutaneous CT-Guided Biopsy of the Musculoskeletal System: Results of 2027 Cases. Eur. J. Radiol. 2011, 77, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Pouedras, M.; Briand, S.; Crenn, V.; Cassagnau, E.; Gouin, F. Non Image-Guided Core Needle Biopsies Can Be Used Safely to Improve Diagnostic Efficiency for Soft Tissue Tumors. Surg. Oncol. 2021, 37, 101518. [Google Scholar] [CrossRef] [PubMed]
- Galant, C.; Bouvier, C.; Larousserie, F.; Aubert, S.; Audard, V.; Brouchet, A.; Marie, B.; Guinebretière, J.-M.; de Pinieux du Bouexic, G. Diagnostic histologique des tumeurs osseuses: Biopsie chirurgicale ou biopsie percutanée? Recommandations des pathologistes du réseau de référence des tumeurs osseuses (RESOS). Bull. Du Cancer 2018, 105, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Furuta, T.; Johan, M.P.; Sakuda, T.; Ochi, M.; Adachi, N. A Meta-Analysis Supports Core Needle Biopsy by Radiologists for Better Histological Diagnosis in Soft Tissue and Bone Sarcomas. Med. Baltim. 2018, 97, e11567. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Frassica, F.J.; Fayad, L.; Clark, D.P.; Weber, K.L. Analysis of Nondiagnostic Results after Image-Guided Needle Biopsies of Musculoskeletal Lesions. Clin. Orthop. Relat. Res. 2010, 468, 3103–3111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, A.; Fell, T.; Birkenmaier, C.; Fromm, J.; Jansson, V.; Knösel, T.; Dürr, H.R. Relative Sensitivity of Core-Needle Biopsy and Incisional Biopsy in the Diagnosis of Musculoskeletal Sarcomas. Cancers 2021, 13, 1393. [Google Scholar] [CrossRef] [PubMed]
- Sharif, B.; Lindsay, D.; Saifuddin, A. The Role of Imaging in Differentiating Low-Grade and High-Grade Central Chondral Tumours. Eur. J. Radiol. 2021, 137, 109579. [Google Scholar] [CrossRef] [PubMed]
- Roitman, P.D.; Farfalli, G.L.; Ayerza, M.A.; Múscolo, D.L.; Milano, F.E.; Aponte-Tinao, L.A. Is Needle Biopsy Clinically Useful in Preoperative Grading of Central Chondrosarcoma of the Pelvis and Long Bones? Clin. Orthop. Relat. Res. 2017, 475, 808–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegde, V.; Burke, Z.D.C.; Park, H.Y.; Zoller, S.D.; Johansen, D.; Kelley, B.V.; Levine, B.; Motamedi, K.; Federman, N.C.; Seeger, L.L.; et al. Is Core Needle Biopsy Reliable in Differentiating Between Aggressive Benign and Malignant Radiolucent Bone Tumors? Clin. Orthop. Relat. Res. 2018, 476, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Taupin, T.; Decouvelaere, A.-V.; Vaz, G.; Thiesse, P. Accuracy of Core Needle Biopsy for the Diagnosis of Osteosarcoma: A Retrospective Analysis of 73 patients. Diagn. Interv. Imaging 2016, 97, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Mankin, H.J.; Mankin, C.J.; Simon, M.A. The Hazards of the Biopsy, Revisited. Members of the Musculoskeletal Tumor Society. J. Bone Jt. Surg. Am. 1996, 78, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Errani, C.; Traina, F.; Perna, F.; Calamelli, C.; Faldini, C. Current Concepts in the Biopsy of Musculoskeletal Tumors. Sci. World J. 2013, 2013, 538152. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Cohort (n = 196) | |
|---|---|
| Age | 41.9 (8–90) |
| Sex | |
| Female | 106 (54.1%) |
| Male | 90 (45.9%) |
| Performance status | |
| 0 | 154 (78.6%) |
| 1–2 | 37 (18.9%) |
| 3–4 | 5 (2.5%) |
| Localization | |
| Upper limb | 39 (19.9%) |
| Lower limb | 115 (58.7%) |
| Axial skeleton | 42 (21.4%) |
| Biopsy type | |
| Percutaneous guided | |
| Echography | 14 (7.1%) |
| CT | 182 (92.9%) |
| Anesthesiology modality | |
| Local anesthesia | 180 (91.8%) |
| General anesthesia | 16 (8.2%) |
| Sampling Outcome Diagnosis | Final Diagnosis | ||
|---|---|---|---|
| Malignant | Begnin | ||
| Osteosarcoma | 27 (13.8%) | Giant cell tumor | 19 (9.7%) |
| Chondrosarcoma | 27 (13.8%) | No malignancy lesion * | 18 (9.2%) |
| Ewing sarcoma | 20 (10.2%) | Angioma | 7 (3.6%) |
| Lymphoma | 11 (5.6%) | Chondroblastoma | 7 (3.6%) |
| Chordoma | 4 (2.0%) | Osteoid Osteoma | 5 (2.6%) |
| Myeloma or plasmacytoma | 4 (2.0%) | Nonossifying fibroma | 5 (2.6%) |
| High-grade sarcoma (NOS) | 1 (0.5%) | Langerhans cell histiocytosis | 5 (2.6%) |
| Pleomorphic cell sarcoma | 1 (0.5%) | Osteochondroma or osteoma | 4 (2.0%) |
| Adamantinoma | 1 (0.5%) | Fibrous dysplasia | 4 (2.0%) |
| Malignant hemangioendothelioma | 1 (0.5%) | Infection | 3 (1.5%) |
| Simple bone cyst | 3 (1.5%) | ||
| Benign fibrous histiocytoma | 3 (1.5%) | ||
| Chondroma | 2 (1.0%) | ||
| Osteoblastoma | 2 (1.0%) | ||
| Reactive bone changes | 2 (1.0%) | ||
| Paget’s disease | 2 (1.0%) | ||
| Begnin hemangioma | 2 (1.0%) | ||
| Atypic cartilaginous tumor | 1 (0.5%) | ||
| Brown tumor | 1 (0.5%) | ||
| Intra-osseous lipoma | 1 (0.5%) | ||
| Gout tophus | 1 (0.5%) | ||
| Chondrocalcinosis | 1 (0.5%) | ||
| Total | 97(49.5%) | 99 (51.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crenn, V.; Vezole, L.; Bouhamama, A.; Meurgey, A.; Karanian, M.; Marec-Bérard, P.; Gouin, F.; Vaz, G. Percutaneous Core Needle Biopsy Can Efficiently and Safely Diagnose Most Primary Bone Tumors. Diagnostics 2021, 11, 1552. https://doi.org/10.3390/diagnostics11091552
Crenn V, Vezole L, Bouhamama A, Meurgey A, Karanian M, Marec-Bérard P, Gouin F, Vaz G. Percutaneous Core Needle Biopsy Can Efficiently and Safely Diagnose Most Primary Bone Tumors. Diagnostics. 2021; 11(9):1552. https://doi.org/10.3390/diagnostics11091552
Chicago/Turabian StyleCrenn, Vincent, Léonard Vezole, Amine Bouhamama, Alexandra Meurgey, Marie Karanian, Perrine Marec-Bérard, François Gouin, and Gualter Vaz. 2021. "Percutaneous Core Needle Biopsy Can Efficiently and Safely Diagnose Most Primary Bone Tumors" Diagnostics 11, no. 9: 1552. https://doi.org/10.3390/diagnostics11091552
APA StyleCrenn, V., Vezole, L., Bouhamama, A., Meurgey, A., Karanian, M., Marec-Bérard, P., Gouin, F., & Vaz, G. (2021). Percutaneous Core Needle Biopsy Can Efficiently and Safely Diagnose Most Primary Bone Tumors. Diagnostics, 11(9), 1552. https://doi.org/10.3390/diagnostics11091552