
Evidence of SARS-CoV-2 Virus in the Middle Ear of Deceased COVID-19 Patients


 ,
,  ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Sampling
2.3. Virology Analysis for SARS-CoV-2
2.3.1. Antemortem PCR
2.3.2. Tissue Virology Analyses
2.4. Histopathology
2.5. Scanning Electron Microscopy (SEM)
2.6. Transmission Electron Microscopy (TEM)
3. Results
3.1. Virology Analyses
3.2. Histopathology
3.3. SEM
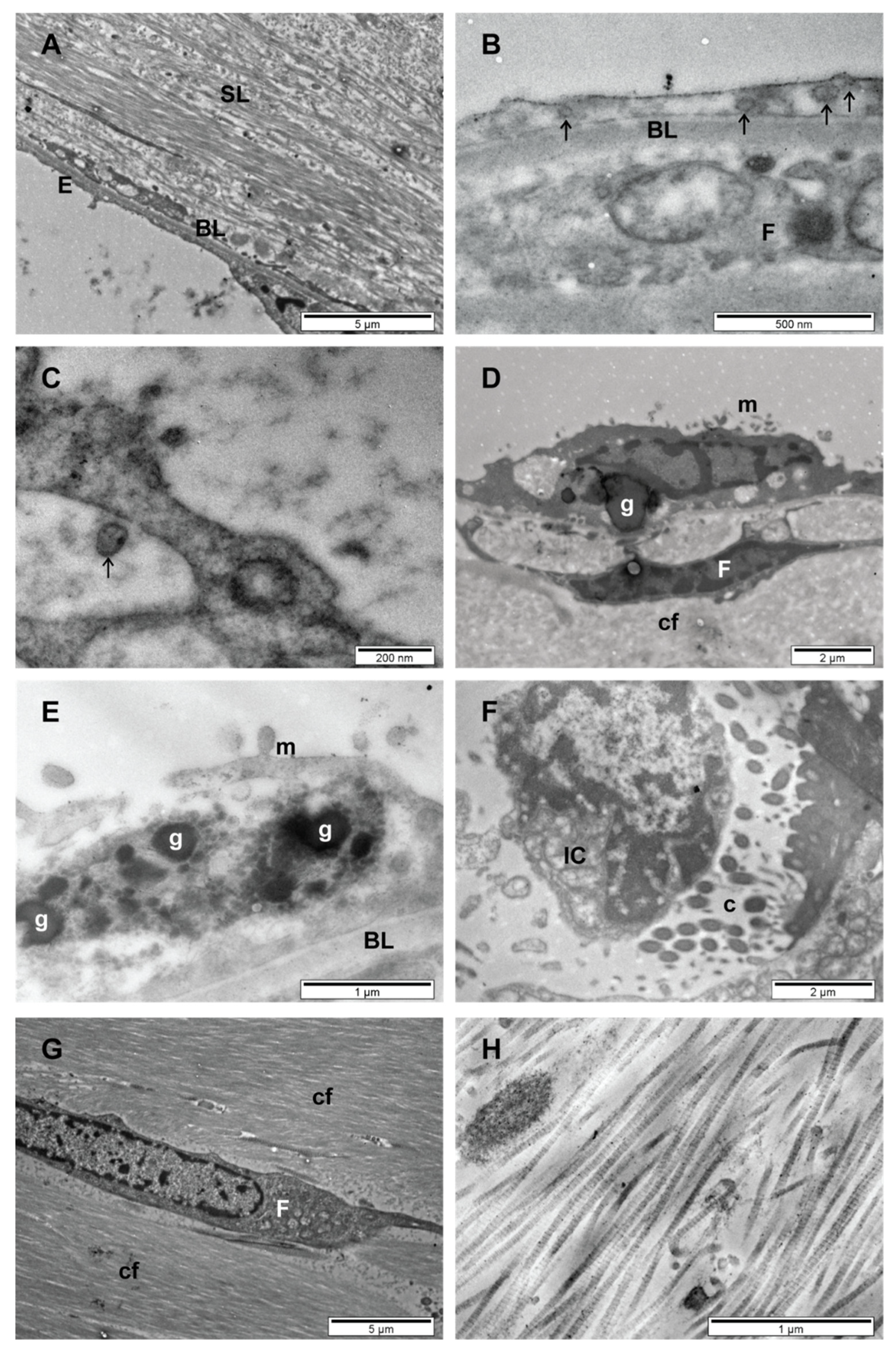
3.4. TEM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef]
- Massa, H.M.; Lim, D.J.; Kurono, Y.; Cripps, A.W. Middle Ear and Eustachian Tube Mucosal Immunology. Mucosal. Immunol. 2015, 2, 1923–1942. [Google Scholar] [CrossRef]
- Gallo, O.; Locatello, L.G.; Mazzoni, A.; Novelli, L.; Annunziato, F. The central role of the nasal microenvironment in the transmission, modulation, and clinical progression of SARS-CoV-2 infection. Mucosal. Immunol. 2021, 14, 305–316. [Google Scholar] [CrossRef]
- Couloigner, V.; Schmerber, S.; Nicollas, R.; Coste, A.; Barry, B.; Makeieff, M.; Boudard, P.; Bequignon, E.; Morel, N.; Lescanne, E. COVID-19 and ENT Surgery. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020, 137, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Cetinkaya, E.A. COVID-19 Pandemic and Otologic Surgery. J. Craniofac. Surg. 2020, 31, e651–e652. [Google Scholar] [CrossRef] [PubMed]
- Fidan, V. New type of corona virus induced acute otitis media in adult. Am. J. Otolaryngol. 2020, 41, 102487. [Google Scholar] [CrossRef]
- Frazier, K.M.; Hooper, J.E.; Mostafa, H.H.; Stewart, C.M. SARS-CoV-2 Virus Isolated from the Mastoid and Middle Ear: Implications for COVID-19 Precautions during Ear Surgery. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 964–966. [Google Scholar] [CrossRef]
- Raad, N.; Ghorbani, J.; Mikaniki, N.; Haseli, S.; Karimi-Galougahi, M. Otitis media in coronavirus disease 2019: A case series. J. Laryngol. Otol. 2021, 135, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, S.; Bello Alvarez, M.; Mungul, S.; Hari, K. Otologic dysfunction in patients with COVID-19: A systematic review. Laryngoscope Investig. Otolaryngol. 2020, 5, 1192–1196. [Google Scholar] [CrossRef]
- Givi, B.; Schiff, B.A.; Chinn, S.B.; Clayburgh, D.; Iyer, N.G.; Jalisi, S.; Moore, M.G.; Nathan, C.-A.; Orloff, L.A.; O’Neill, J.P.; et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID-19 Pandemic. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 579–584. [Google Scholar] [CrossRef] [PubMed]
- WHO. Infection Prevention and Control for the Safe Management of a Dead Body in the Context of COVID-19. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/331538/WHO-COVID-19-lPC_DBMgmt-2020.1-eng.pdf (accessed on 3 February 2021).
- Centers for Disease Control and Prevention. Collection and Submission of Postmortem Specimens from Deceased Persons with Known or Suspected COVID-19. 2020; (Interim Guidance). Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specimens.html (accessed on 26 March 2021).
- European Centre for Disease Prevention and Control. Considerations Related to the Safe Handling of Bodies of Deceased Persons with Suspected or Confirmed COVID-14. Available online: https://www.ecdc.europa.eu/en/publications-data/considerations-related-safe-handling-bodies-deceased-persons-suspected-or (accessed on 26 March 2021).
- Romanian Health Ministry. Order No. 436 of March 13, 2020 on Specific Protocol on the Management in Case of Death of Patients Infected with the New Coronavirus (SARS-CoV2); Romanian Health Ministry: Bucharest, Romania, 2020. [Google Scholar]
- Romanian National Institute for Public Health. Methodology for Surveillance of Acute Respiratory Syndrome with the New Coronavirus (COVID-19). Available online: https://www.cnscbt.ro/index.php/info-medical/2047-metodologia-de-supraveghere-a-covid-19-actualizare-23-10-2020-1/file (accessed on 20 July 2021).
- Quick, J.; Loman, N. hCoV-2019/nCoV-2019 Version 3 Amplicon Set. ARTIC Consortium. 2020. Available online: https://artic.network/resources/ncov/ncov-amplicon-v3.pdf (accessed on 31 January 2021).
- Hou, Y.J.; Okuda, K.; Edwards, C.E.; Martinez, D.R.; Asakura, T.; Dinnon, K.H.; Kato, T.; Lee, R.E.; Yount, B.L.; Mascenik, T.M.; et al. SARS-CoV-2 Reverse Genetics Reveals a Variable Infection Gradient in the Respiratory Tract. Cell 2020, 182, 429–446.e14. [Google Scholar] [CrossRef]
- Uranaka, T.; Kashio, A.; Ueha, R.; Sato, T.; Bing, H.; Ying, G.; Kinoshita, M.; Kondo, K.; Yamasoba, T. Expression of ACE2, TMPRSS2, and Furin in Mouse Ear Tissue, and the Implications for SARS-CoV-2 Infection. Laryngoscope 2021, 131, E2013–E2017. [Google Scholar] [CrossRef]
- Martines, F.; Dispenza, F.; Sireci, F.; Gallina, S.; Salvago, P. Eustachian Tube Function Assessment after Radiofrequency Turbinate Reduction in Atopic and Non-Atopic Patients. Int. J. Environ. Res. Public Health 2021, 18, 881. [Google Scholar] [CrossRef]
- Sawada, S.; Okutani, F.; Kobayashi, T. Comprehensive Detection of Respiratory Bacterial and Viral Pathogens in the Middle Ear Fluid and Nasopharynx of Pediatric Patients with Acute Otitis Media. Pediatr. Infect. Dis. J. 2019, 38, 1199–1203. [Google Scholar] [CrossRef]
- Pitkäranta, A.; Virolainen, A.; Jero, J.; Arruda, E.; Hayden, F.G. Detection of rhinovirus, respiratory syncytial virus, and coronavirus infections in acute otitis media by reverse transcriptase polymerase chain reaction. Pediatrics 1998, 102, 291–295. [Google Scholar] [CrossRef] [PubMed]
- E Gurgel, J.D.C.; Pereira, C.S.B.; GuerreiroFregnani, J.H.T.; Quintanilha Ribeiro, F.A. Method for removal of samples from the external ear canal and the tympanic membrane for histological and immunohistochemical studies. Braz. J. Otorhinolaryngol. 2012, 78, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Y.; Kang, J.-Y.; Chen, S.; He, Y.; Han, B.; Liu, M.-F.; Lu, L.; Li, L.; Yi, Z.; et al. Potential transmission chains of variant B.1.1.7 and co-mutations of SARS-CoV-2. Cell Discov. 2021, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mandel, E.M.; Doyle, W.J.; Winther, B.; Alper, C.M. The incidence, prevalence and burden of OM in unselected children aged 1-8 years followed by weekly otoscopy through the “common cold” season. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 491–499. [Google Scholar] [CrossRef][Green Version]
- Alper, C.M.; Winther, B.; Mandel, E.M.; Hendley, J.O.; Doyle, W.J. Rate of concurrent otitis media in upper respiratory tract infections with specific viruses. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 17–21. [Google Scholar] [CrossRef][Green Version]
- Heikkinen, T.; Chonmaitree, T. Importance of respiratory viruses in acute otitis media. Clin. Microbiol. Rev. 2003, 16, 230–241. [Google Scholar] [CrossRef]
- Suzuki, K.; Bakaletz, L.O. Synergistic effect of adenovirus type 1 and nontypeableHaemophilus influenzae in a chinchilla model of experimental otitis media. Infect. Immun. 1994, 62, 1710–1718. [Google Scholar] [CrossRef]
- Avadhanula, V.; Rodriguez, C.A.; Devincenzo, J.P.; Wang, Y.; Webby, R.J.; Ulett, G.C.; Adderson, E.E. Respiratory viruses augment the adhesion of bacterial pathogens to respiratory epithelium in a viral species- and cell type-dependent manner. J. Virol. 2006, 80, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Wadowsky, R.M.; Mietzner, S.M.; Skoner, D.P.; Doyle, W.J.; Fireman, P. Effect of experimental influenza A virus infection on isolation of Streptococcus pneumoniae and other aerobic bacteria from the oropharynges of allergic and nonallergic adult subjects. Infect. Immun. 1995, 63, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.H.; Fisher, L.M.; Kosunick, G.M.; DeMaria, T.F. Effect of adenovirus type 1 and influenza A virus on Streptococcus pneumoniae nasopharyngeal colonization and otitis media in the chinchilla. Ann. Otol. Rhinol. Laryngol. 2000, 109, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.H.; Griffith, S.R.; Park, K.H.; Lim, D.J.; DeMaria, T.F. Cytological and histological changes in the middle ear after inoculation of influenza A virus. Acta Otolaryngol. 1993, 113, 81–87. [Google Scholar] [CrossRef]
- Park, K.; Bakaletz, L.O.; Coticchia, J.M.; Lim, D.J. Effect of influenza A virus on ciliary activity and dye transport function in the chinchilla eustachian tube. Ann. Otol. Rhinol. Laryngol. 1993, 102, 551–558. [Google Scholar] [CrossRef]
- Liu, X.; Cong, N.; Cheng, X.; Ma, R.; Wang, J.; Huang, Y.-B.; Zhao, M.; Wang, X.-W.; Chi, F.-L.; Ren, D.-D. The Role of the Notch Signal Pathway in Mucosal Cell Metaplasia in Mouse Acute Otitis Media. Sci. Rep. 2017, 7, 4588. [Google Scholar] [CrossRef]
- Scarano, E.; Paludetti, G.; Frusoni, F.; Deli, R.; Maurizi, M. Morphological distribution of middle-ear epithelium in the Wistar rat: A functional hypothesis. ORL J. Otorhinolaryngol. Relat. Spec. 1997, 59, 166–169. [Google Scholar] [CrossRef]
- Ansari, A.; Tariq, M.A.; Sadiq, N.M. Histology, Ear. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK545170/ (accessed on 26 March 2021).
- Hentzer, E. Ultrastructure of the middle ear mucosa. Acta Otolaryngol. Suppl. 1984, 414, 19–27. [Google Scholar] [CrossRef]
- Ars, B.; Dirckx, J.; Ars-Piret, N.; Buytaert, J. Insights in the physiology of the human mastoid: Message to the surgeon. J. Int. Adv. Otol. 2012, 8, 296–310. [Google Scholar]
- Luers, J.C.; Hüttenbrink, K.B. Surgical anatomy and pathology of the middle ear. J. Anat. 2016, 228, 338–353. [Google Scholar] [CrossRef] [PubMed]
- Danishyar, A.; Ashurst, J.V. Acute Otitis Media. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470332/ (accessed on 26 March 2021).
- Tsuchiya, K.; Komori, M.; Zheng, Q.Y.; Ferrieri, P.; Lin, J. Interleukin-10 is an essential modulator of mucoid metaplasia in a mouse otitis media model. Ann. Otol. Rhinol. Laryngol. 2008, 117, 630–636. [Google Scholar] [CrossRef]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brünink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Bullock, H.A.; Goldsmith, C.S.; Miller, S.E. Best practices for correctly identifying coronavirus by transmission electron microscopy. Kidney Int. 2021, 99, 824–827. [Google Scholar] [CrossRef] [PubMed]
- Dittmayer, C.; Meinhardt, J.; Radbruch, H.; Radke, J.; Heppner, B.I.; Heppner, F.L.; Stenzel, W.; Holland, G.; Laue, M. Why misinterpretation of electron micrographs in SARS-CoV-2-infected tissue goes viral. Lancet 2020, 396, e64–e65. [Google Scholar] [CrossRef]
- Pérez, A.; Torregrosa, I.; D’Marco, L.; Juan, I.; Terradez, L.; Solís, M.Á.; Moncho, F.; Carda-Batalla, C.; Forner, M.J.; Gorriz, J.L. IgA-Dominant Infection-Associated Glomerulonephritis Following SARS-CoV-2 Infection. Viruses 2021, 13, 587. [Google Scholar] [CrossRef]
- Ye, W.; Xianyang, L. A Novel Coronavirus Pneumonia Case Report from an Ear, Nose, and Throat Clinic. Laryngoscope 2020, 130, 1106–1107. [Google Scholar] [CrossRef]
- Mohan, S.; Workman, A.; Barshak, M.; Welling, D.B.; Abdul-Aziz, D. Considerations in Management of Acute Otitis Media in the COVID-19 Era. Ann. Otol. Rhinol. Laryngol. 2021, 130, 520–527. [Google Scholar] [CrossRef]
- Ayache, S.; Schmerber, S. Covid-19 and Otologic/Neurotologic Practices: Suggestions to Improve the Safety of Surgery and Consultations. Otol. Neurotol. 2020, 41, 1175–1181. [Google Scholar] [CrossRef]
- Liaw, J.; Saadi, R.; Patel, V.A.; Isildak, H. Middle Ear Viral Load Considerations in the COVID-19 Era: A Systematic Review. Otol. Neurotol. 2021, 42, 217–226. [Google Scholar] [CrossRef]
- Hilal, A.; Walshe, P.; Gendy, S.; Knowles, S.; Burns, H. Mastoidectomy and trans-corneal viral transmission. Laryngoscope 2005, 115, 1873–1876. [Google Scholar] [CrossRef] [PubMed]
- Workman, A.D.; Welling, D.B.; Carter, B.S.; Curry, W.T.; Holbrook, E.H.; Gray, S.T.; Scangas, G.A.; Bleier, B.S. Endonasal instrumentation and aerosolization risk in the era of COVID-19: Simulation, literature review, and proposed mitigation strategies. Int. Forum. Allergy Rhinol. 2020, 10, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Ayache, S.; Kutz, W.; Isaacson, B.; Badr-El-Dine, M.; Nogueira, J.F.; Marchioni, D.; Presutti, L. COVID-19 and ear endoscopy in otologic practices. Eur. Arch. Otorhinolaryngol. 2021, 278, 2133–2135. [Google Scholar] [CrossRef]
- Xu, T.; Huang, R.; Zhu, L.; Wang, J.; Cheng, J.; Zhang, B.; Zhao, H.; Chen, K.; Shao, H.; Zhu, C.; et al. Epidemiological and clinical features of asymptomatic patients with SARS-CoV-2 infection. J. Med. Virol. 2020, 92, 1884–1889. [Google Scholar] [CrossRef] [PubMed]
- Saadi, R.A.; Bann, D.V.; Patel, V.A.; Goldenberg, D.; May, J.; Isildak, H. A Commentary on Safety Precautions for Otologic Surgery during the COVID-19 Pandemic. Otolaryngol. Head Neck Surg. 2020, 162, 797–799. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. of Samples, Sex, Age | Ct Values Nasal Mucosa (E/RdRp/N) | Ct Values Middle Ear (E/RdRp/N) | Genome Sequences | GISAID |
|---|---|---|---|---|
| 1, M, 56 | -/-/37 | -/-/- | - | - |
| 2, M, 75 | 34/37/34 | -/-/- | - | - |
| 3, M, 87 | 24/25/22 | -/-/37 | Lineage B.1.1.7 (20I/501Y.V1), Alpha | EPI_ISL_2727499 |
| 4, F, 68 | 26/23/26 | 32/25/31 | Lineage B.1.1.7 (20I/501Y.V1), Alpha | EPI_ISL_2727500 |
| 5, M, 80 | 20/17/20 | 24/23/24 | Lineage B.1.1.7 (20I/501Y.V1), Alpha | EPI_ISL_2727566 |
| 6, M, 58 | -/29/33 | 29/25/28 | Lineage B.1.1.7 (20I/501Y.V1), Alpha | EPI_ISL_2727501 |
| 7, F, 82 | -/-/35 | -/-/35 | - | - |
| 8, F, 78 | 21/19/23 | 27/22/26 | Lineage B.1.1.7 (20I/501Y.V1), Alpha | EPI_ISL_2652169 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeican, I.I.; Aluaș, M.; Lazăr, M.; Barbu-Tudoran, L.; Gheban, D.; Inișca, P.; Albu, C.; Tripon, S.; Albu, S.; Siserman, C.; et al. Evidence of SARS-CoV-2 Virus in the Middle Ear of Deceased COVID-19 Patients. Diagnostics 2021, 11, 1535. https://doi.org/10.3390/diagnostics11091535
Jeican II, Aluaș M, Lazăr M, Barbu-Tudoran L, Gheban D, Inișca P, Albu C, Tripon S, Albu S, Siserman C, et al. Evidence of SARS-CoV-2 Virus in the Middle Ear of Deceased COVID-19 Patients. Diagnostics. 2021; 11(9):1535. https://doi.org/10.3390/diagnostics11091535
Chicago/Turabian StyleJeican, Ionuț Isaia, Maria Aluaș, Mihaela Lazăr, Lucian Barbu-Tudoran, Dan Gheban, Patricia Inișca, Camelia Albu, Septimiu Tripon, Silviu Albu, Costel Siserman, and et al. 2021. "Evidence of SARS-CoV-2 Virus in the Middle Ear of Deceased COVID-19 Patients" Diagnostics 11, no. 9: 1535. https://doi.org/10.3390/diagnostics11091535
APA StyleJeican, I. I., Aluaș, M., Lazăr, M., Barbu-Tudoran, L., Gheban, D., Inișca, P., Albu, C., Tripon, S., Albu, S., Siserman, C., Vica, M. L., Muntean, M., Opincariu, I., & Junie, L. M. (2021). Evidence of SARS-CoV-2 Virus in the Middle Ear of Deceased COVID-19 Patients. Diagnostics, 11(9), 1535. https://doi.org/10.3390/diagnostics11091535