
Magnetic Resonance Detects Structural Heart Disease in Patients with Frequent Ventricular Ectopy and Normal Echocardiographic Findings

 , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Statistics
4. Results
4.1. CMR—Findings
4.2. PVC Morphology
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheriyath, P.; He, F.; Peters, I.; Li, X.; Alagona, P.; Wu, C.; Pu, M.; Cascio, W.E.; Liao, D. Relation of Atrial and/or Ventricular Premature Complexes on a Two-Minute Rhythm Strip to the Risk of Sudden Cardiac Death (the Atherosclerosis Risk in Communities [ARIC] Study). Am. J. Cardiol. 2011, 107, 151–155. [Google Scholar] [CrossRef]
- Simpson, R.J.; Cascio, W.E.; Schreiner, P.J.; Crow, R.S.; Rautaharju, P.M.; Heiss, G. Prevalence of premature ventricular contractions in a population of African American and white men and women: The Atherosclerosis Risk in Communities (ARIC) study. Am. Hear. J. 2002, 143, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, H.L.; Whitlock, J.A.; Sprague, M.K.; Kennedy, L.J.; Buckingham, T.A.; Goldberg, R.J. Long-Term Follow-up of Asymptomatic Healthy Subjects with Frequent and Complex Ventricular Ectopy. N. Engl. J. Med. 1985, 312, 193–197. [Google Scholar] [CrossRef]
- Fisher, F.D.; Tyroler, H.A. Relationship between Ventricular Premature Contractions on Routine Electrocardiography and Subsequent Sudden Death from Coronary Heart Disease. Circulation 1973, 47, 712–719. [Google Scholar] [CrossRef] [Green Version]
- Abdalla, I.S.; Prineas, R.J.; Neaton, J.D.; Jacobs, D.R.; Crow, R.S. Relation between ventricular premature complexes and sudden cardiac death in apparently healthy men. Am. J. Cardiol. 1987, 60, 1036–1042. [Google Scholar] [CrossRef]
- Yang, J.; Dudum, R.; Mandyam, M.C.; Marcus, G.M. Characteristics of Unselected High-Burden Premature Ventricular Contraction Patients. Pacing Clin. Electrophysiol. 2014, 37, 1671–1680. [Google Scholar] [CrossRef]
- Ataklte, F.; Erqou, S.; Laukkanen, J.; Kaptoge, S. Meta-Analysis of Ventricular Premature Complexes and Their Relation to Cardiac Mortality in General Populations. Am. J. Cardiol. 2013, 112, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.; Hemingway, H.; Harb, R.; Crake, T.; Lambiase, P. The prognostic significance of premature ventricular complexes in adults without clinically apparent heart disease: A meta-analysis and systematic review. Heart 2012, 98, 1290–1298. [Google Scholar] [CrossRef]
- Wijnmaalen, A.P.; Delgado, V.; Schalij, M.J.; Taxis, C.F.B.V.H.V.; Holman, E.R.; Bax, J.J.; Zeppenfeld, K. Beneficial effects of catheter ablation on left ventricular and right ventricular function in patients with frequent premature ventricular contractions and preserved ejection fraction. Heart 2010, 96, 1275–1280. [Google Scholar] [CrossRef] [PubMed]
- Latchamsetty, R.; Bogun, F. Premature Ventricular Complex-induced Cardiomyopathy. Rev. Española Cardiol. 2016, 69, 365–369. [Google Scholar] [CrossRef]
- Proclemer, A.; Basadonna, P.T.; Slavich, G.A.; Miani, D.; Fresco, C.; Fioretti, P.M. Cardiac magnetic resonance imaging findings in patients with right ventricular outflow tract premature contractions. Eur. Hear. J. 1997, 18, 2002–2010. [Google Scholar] [CrossRef] [Green Version]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. G. Ital. Cardiol. 2016, 17, 108–170. [Google Scholar] [CrossRef]
- Zipes, D.; Camm, A.J.; Borggrefe, M.; Buxton, A.E.; Chaitman, B.; Fromer, M.; Gregoratos, G.; Klein, G.; Moss, A.J.; Myerburg, R.J.; et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death--executive summary: A report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death) Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Eur. Hear. J. 2006, 27, 2099–2140. [Google Scholar] [CrossRef] [Green Version]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm 2018, 15, e190–e252. [Google Scholar] [PubMed] [Green Version]
- Aquaro, G.D.; Pingitore, A.; Strata, E.; Di Bella, G.; Molinaro, S.; Lombardi, M. Cardiac Magnetic Resonance Predicts Outcome in Patients with Premature Ventricular Complexes of Left Bundle Branch Block Morphology. J. Am. Coll. Cardiol. 2010, 56, 1235–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markowitz, S.M.; Weinsaft, J.W.; Waldman, L.; Petashnick, M.; Liu, C.F.; Cheung, J.; Thomas, G.; Ip, J.E.; Lerman, B.B. Reappraisal of Cardiac Magnetic Resonance Imaging in Idiopathic Outflow Tract Arrhythmias. J. Cardiovasc. Electrophysiol. 2014, 25, 1328–1335. [Google Scholar] [CrossRef] [Green Version]
- Nucifora, G.; Muser, D.; Masci, P.G.; Barison, A.; Rebellato, L.; Piccoli, G.; Daleffe, E.; Toniolo, M.; Zanuttini, D.; Facchin, D.; et al. Prevalence and Prognostic Value of Concealed Structural Abnormalities in Patients with Apparently Idiopathic Ventricular Arrhythmias of Left Versus Right Ventricular Origin A Magnetic Resonance Imaging Study. Circ. Arrhythmia Electrophysiol. 2014, 7, 456–462. [Google Scholar] [CrossRef] [Green Version]
- White, R.D.; Trohman, R.G.; Flamm, S.D.; VanDyke, C.W.; Optican, R.J.; Sterba, R.; A Obuchowski, N.; Carlson, M.D.; Tchou, P.J. Right ventricular arrhythmia in the absence of arrhythmogenic dysplasia: MR imaging of myocardial abnormalities. Radiology 1998, 207, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Zorzi, A.; Sarto, P.; Donini, M.; Rigato, I.; Bariani, R.; de Lazzari, M.; Pilichou, K.; Thiene, G.; Iliceto, S.; et al. Predictive value of exercise testing in athletes with ventricular ectopy evaluated by cardiac magnetic resonance. Hear. Rhythm. 2019, 16, 239–248. [Google Scholar] [CrossRef]
- Russo, A.D.; Pieroni, M.; Santangeli, P.; Bartoletti, S.; Casella, M.; Pelargonio, G.; Smaldone, C.; Bianco, M.; Di Biase, L.; Bellocci, F.; et al. Concealed cardiomyopathies in competitive athletes with ventricular arrhythmias and an apparently normal heart: Role of cardiac electroanatomical mapping and biopsy. Heart Rhythm 2011, 8, 1915–1922. [Google Scholar] [CrossRef]
- Oebel, S.; Dinov, B.; Arya, A.; Hilbert, S.; Sommer, P.; Bollmann, A.; Hindricks, G.; Paetsch, I.; Jahnke, C. ECG morphology of premature ventricular contractions predicts the presence of myocardial fibrotic substrate on cardiac magnetic resonance imaging in patients undergoing ablation. J. Cardiovasc. Electrophysiol. 2017, 28, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Sestito, A.; Pardeo, M.; A Sgueglia, G.; Natale, L.; Delogu, A.; Infusino, F.; De Rosa, G.; Bellocci, F.; Crea, F.; A Lanza, G. Cardiac magnetic resonance of healthy children and young adults with frequent premature ventricular complexes. J. Cardiovasc. Med. 2007, 8, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Yokokawa, M.; Siontis, K.C.; Kim, H.M.; Stojanovska, J.; Latchamsetty, R.; Crawford, T.; Jongnarangsin, K.; Ghanbari, H.; Cunnane, R.; Chugh, A.; et al. Value of cardiac magnetic resonance imaging and programmed ventricular stimulation in patients with frequent premature ventricular complexes undergoing radiofrequency ablation. Hear. Rhythm. 2017, 14, 1695–1701. [Google Scholar] [CrossRef] [PubMed]
- Cabanelas, N.; Ferreira, M.J.V.; Donato, P.; Gaspar, A.; Pinto, J.; Caseiro-Alves, F.; Providência, L.A. Added value of cardiac magnetic resonance in etiological diagnosis of ventricular arrhythmias. Rev. Port. Cardiol. 2013, 32, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Hudsmith, L.E.; Petersen, S.; Francis, J.M.; Robson, M.D.; Neubauer, S. Normal Human Left and Right Ventricular and Left Atrial Dimensions Using Steady State Free Precession Magnetic Resonance Imaging. J. Cardiovasc. Magn. Reson. 2005, 7, 775–782. [Google Scholar] [CrossRef]
- Tanawuttiwat, T.; Nazarian, S.; Calkins, H. The role of catheter ablation in the management of ventricular tachycardia. Eur. Hear. J. 2016, 37, 594–609. [Google Scholar] [CrossRef]
- Muser, D.; Santangeli, P.; Selvanayagam, J.B.; Nucifora, G. Role of Cardiac Magnetic Resonance Imaging in Patients with Idiopathic Ventricular Arrhythmias. Curr. Cardiol. Rev. 2018, 15, 12–23. [Google Scholar] [CrossRef]
- Mahida, S.; Sacher, F.; Dubois, R.; Sermesant, M.; Bogun, F.; Haïssaguerre, M.; Jaïs, P.; Cochet, H. Cardiac Imaging in Patients with Ventricular Tachycardia. Circulation 2017, 136, 2491–2507. [Google Scholar] [CrossRef]
- Sassone, B.; Muser, D.; Casella, M.; Luzi, M.; Virzì, S.; Balla, C.; Nucifora, G. Task Force on Imaging and Task Force on Ablation of Ventricular Tachycardia of the Italian Association of Arrhythmias and Cardiac Pacing (AIAC). Detection of concealed structural heart disease by imaging in patients with apparently idiopathic premature ventricular complexes: A review of current literature. Clin. Cardiol. 2019, 42, 1162–1169. [Google Scholar] [CrossRef] [Green Version]
- Globits, S.; Kreiner, G.; Frank, H.; Heinz, G.; Klaar, U.; Frey, B.; Gössinger, H. Significance of Morphological Abnormalities Detected by MRI in Patients Undergoing Successful Ablation of Right Ventricular Outflow Tract Tachycardia. Circulation 1997, 96, 2633–2640. [Google Scholar] [CrossRef]
- Grimm, W.; Wig, E.L.-H.; Hoffmann, J.; Menz, V.; Klose, K.J.; Maisch, B.; Hahn-Rinn, R. Magnetic Resonance Imaging and Signal-Averaged Electrocardiography in Patients with Repetitive Monomorphic Ventricular Tachycardia and Otherwise Normal Electrocardiogram. Pacing Clin. Electrophysiol. 1997, 20, 1826–1833. [Google Scholar] [CrossRef]
- Pellegrino, P.L.; Casavecchia, G.; Gravina, M.; Carpagnano, G.; Guastafierro, F.; Di Biase, L.; Romero, J.; Santoro, F.; Di Biase, M.; Macarini, L.; et al. Concealed structural heart disease discovered at cardiac magnetic resonance in patients with ventricular extrasystoles from ventricular outflow tract and apparently normal hearts. J. Interv. Card. Electrophysiol. 2021, 61, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Reithmann, C.; Kling, T.; Herkommer, B.; Fiek, M.; Ulbrich, M. Magnetic resonance imaging abnormalities in the basal interventricular septum of patients with left ventricular outflow tract arrhythmias. J. Cardiovasc. Electrophysiol. 2019, 30, 1042–1052. [Google Scholar] [CrossRef] [PubMed]
- Tandri, H.; Saranathan, M.; Rodriguez, E.R.; Martinez, C.; Bomma, C.; Nasir, K.; Rosen, B.; Lima, J.A.; Calkins, H.; Bluemke, D.A. Noninvasive detection of myocardial fibrosis in arrhythmogenic right ventricular cardiomyopathy using delayed-enhancement magnetic resonance imaging. J. Am. Coll. Cardiol. 2005, 45, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Tandri, H.; Bluemke, D.; Ferrari, V.; Bomma, C.; Nasir, K.; Rutberg, J.; Tichnell, C.; James, C.; Lima, J.A.; Calkins, H. Findings on magnetic resonance imaging of idiopathic right ventricular outflow tachycardia. Am. J. Cardiol. 2004, 94, 1441–1445. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidou, C.; Kotanidis, C.; Wijesurendra, R.; Leal-Pelado, J.; Kouskouras, K.; Vassilikos, V.; Karvounis, H.; Ntusi, N.; Antoniades, C.; Neubauer, S.; et al. Cardiac Magnetic Resonance to Detect the Underlying Substrate in Patients with Frequent Idiopathic Ventricular Arrhythmias. Diagnostics 2021, 11, 1109. [Google Scholar] [CrossRef] [PubMed]
- Andreini, D.; Russo, A.D.; Pontone, G.; Mushtaq, S.; Conte, E.; Perchinunno, M.; Guglielmo, M.; Santos, A.C.; Magatelli, M.; Baggiano, A.; et al. CMR for Identifying the Substrate of Ventricular Arrhythmia in Patients with Normal Echocardiography. JACC Cardiovasc. Imaging 2020, 13, 410–421. [Google Scholar] [CrossRef]
- Muser, D.; Santangeli, P.; Castro, S.A.; Casado Arroyo, R.; Maeda, S.; Benhayon, D.A.; Liuba, I.; Liang, J.J.; Sadek, M.M.; Chahal, A.; et al. Risk Stratification of Patients with Apparently Idiopathic Premature Ventricular Contractions A Multicenter International CMR Registry. JACC Clin. Electrophysiol. 2020, 6, 722–735. [Google Scholar] [CrossRef] [PubMed]
- Saurav, A.; Smer, A.; Abuzaid, A.; Bansal, O.; Abuissa, H. Premature Ventricular Contraction-Induced Cardiomyopathy. Clin. Cardiol. 2015, 38, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Laplante, L.; Benzaquen, B.S. A Review of the Potential Pathogenicity and Management of Frequent Premature Ventricular Contractions. Pacing Clin. Electrophysiol. 2016, 39, 723–730. [Google Scholar] [CrossRef]
- Ferrari, A.D.; Borges, A.P.; Albuquerque, L.C.; Sussenbach, C.P.; Rosa, P.R.; Piantá, R.M.; Wiehe, M.; Goldani, M.A. Cardiomyopathy induced by artificial cardiac pacing: Myth or reality sustained by evidence? Rev. Bras. Cir. Cardiovasc. 2014, 29, 402–413. [Google Scholar] [PubMed] [Green Version]
- Ge, Y.; Antiochos, P.; Qamar, I.; Seno, A.; Steigner, M.L.; Aghayev, A.; Blankstein, R.; Stevenson, W.; Jerosch-Herold, M.; Kwong, R.Y. Diagnostic impact and prognostic value of cardiac MRI in patients with ventricular arrhythmias. J. Am. Coll. Cardiol. 2020, 75, 3665. [Google Scholar] [CrossRef]
- Gulani, V.; Calamante, F.; Shellock, F.G.; Kanal, E.; Reeder, S.B. Gadolinium deposition in the brain: Summary of evidence and recommendations. Lancet Neurol. 2017, 16, 564–570. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N | Percent (%) | |
|---|---|---|
| Women | 23 | 45 |
| Hypertension | 16 | 31 |
| Paroxysmal Atrial Fibrillation | 6 | 12 |
| Diabetes Mellitus | 1 | 2 |
| Hyperlipidemia | 3 | 6 |
| <40 Years Old | 10 | 20 |
| 40–70 Years Old | 21 | 41 |
| >70 Years Old | 20 | 39 |
| Parameter | Value |
|---|---|
| LV EF, %, median (IQR) | 55 (53–58.5) |
| LVEDD, mL, mean (±SD) | 165.43 (±33.72) |
| LVESD, mL, mean (±SD) | 73.31 (±19.11) |
| LVSV, mL, median (IQR) | 84.5 (76–107.5) |
| RVEF, mean (±SD) | 56.72 (±5.65) |
| RVEDD, mL, mean (±SD) | 141.95 (±39.55) |
| RVESD, mL, mean (±SD) | 62.78 (±22.72) |
| RVSV, mL, median (IQR) | 76.5 (73.5–106) |
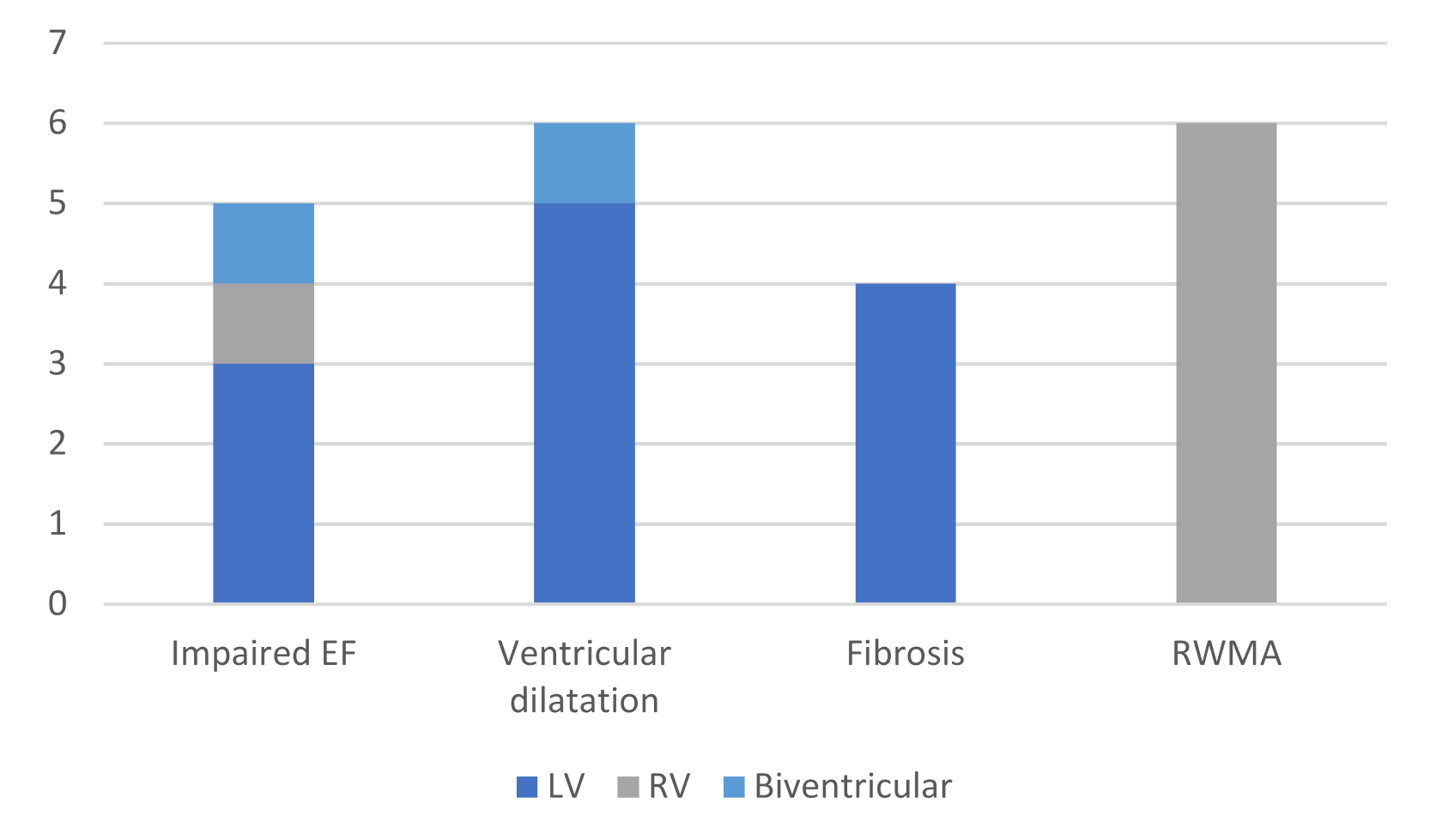
| CMR Finding | RVOT | RV, Intracavity | LV | Multifocal |
|---|---|---|---|---|
| Impaired Left Ventricular Function | 1 | 0 | 0 | 1 |
| Impaired Right Ventricular Function | 1 | 0 | 0 | 0 |
| Impaired Biventricular Function | 1 | 0 | 0 | 0 |
| Left Ventricular Dilatation | 1 | 1 | 1 | 0 |
| Biventricular Dilatation | 0 | 0 | 1 | 0 |
| Fibrosis | 0 | 0 | 2 | 0 |
| Wall Motion Abnormalities | 3 | 1 | 1 | 0 |
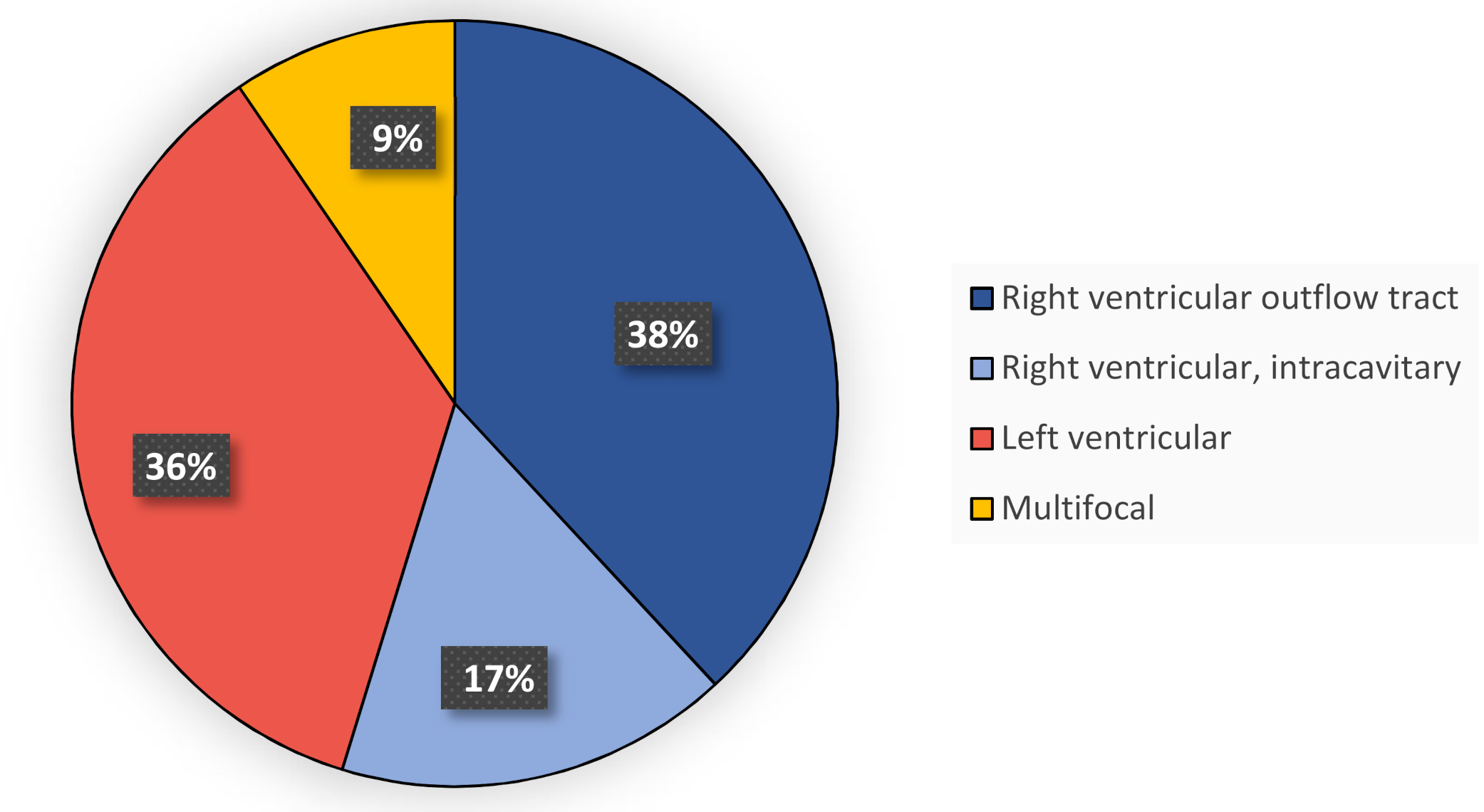
| Origin of PVCs | Patients with Pathology at CMR | Patients with Normal CMR |
|---|---|---|
| RVOT | 5 | 11 |
| RV, Intracavity | 2 | 5 |
| LV | 4 | 11 |
| Multifocal | 1 | 3 |
| CMR Finding | Total Number | RV–PVCs | LV–PVCs | Multifocal PVCs | Unknown PVC Morphology |
|---|---|---|---|---|---|
| Any Solitary RV Finding | 5 | 4 | 0 | 0 | 1 |
| Any Solitary LV Finding | 8 | 2 | 2 | 1 | 3 |
| Any Biventricular Finding | 3 | 1 | 2 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scorza, R.; Jansson, A.; Sörensson, P.; Rosenqvist, M.; Frykman, V. Magnetic Resonance Detects Structural Heart Disease in Patients with Frequent Ventricular Ectopy and Normal Echocardiographic Findings. Diagnostics 2021, 11, 1505. https://doi.org/10.3390/diagnostics11081505
Scorza R, Jansson A, Sörensson P, Rosenqvist M, Frykman V. Magnetic Resonance Detects Structural Heart Disease in Patients with Frequent Ventricular Ectopy and Normal Echocardiographic Findings. Diagnostics. 2021; 11(8):1505. https://doi.org/10.3390/diagnostics11081505
Chicago/Turabian StyleScorza, Raffaele, Anders Jansson, Peder Sörensson, Mårten Rosenqvist, and Viveka Frykman. 2021. "Magnetic Resonance Detects Structural Heart Disease in Patients with Frequent Ventricular Ectopy and Normal Echocardiographic Findings" Diagnostics 11, no. 8: 1505. https://doi.org/10.3390/diagnostics11081505
APA StyleScorza, R., Jansson, A., Sörensson, P., Rosenqvist, M., & Frykman, V. (2021). Magnetic Resonance Detects Structural Heart Disease in Patients with Frequent Ventricular Ectopy and Normal Echocardiographic Findings. Diagnostics, 11(8), 1505. https://doi.org/10.3390/diagnostics11081505