
A Feasibility Study to Increase Chronic Hepatitis C Virus RNA Testing and Linkage to Care among Clients Attending Homeless Services in Amsterdam, The Netherlands

Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Homeless Services, and Participants
2.2. Ethical Procedures
2.3. Procedures to Increase HCV Testing and Linkage to Care
- (1).
- Educating employees about HCV
- (2).
- Instating hepatitis ambassadors at homeless services
- (3).
- Rapid onsite HCV testing
- (4).
- Improving linkage to care for HCV-positive individuals
2.4. Recruitment and Data Collection Procedures
2.5. Sociodemographic Characteristics, HCV-Related Risk Factors, and Sexual Behavior
2.6. Statistical Analyses
2.7. Sensitivity Analyses
3. Results
3.1. Characteristics of the Study Population
3.2. Characteristics of the HCV RNA-Positive Individuals
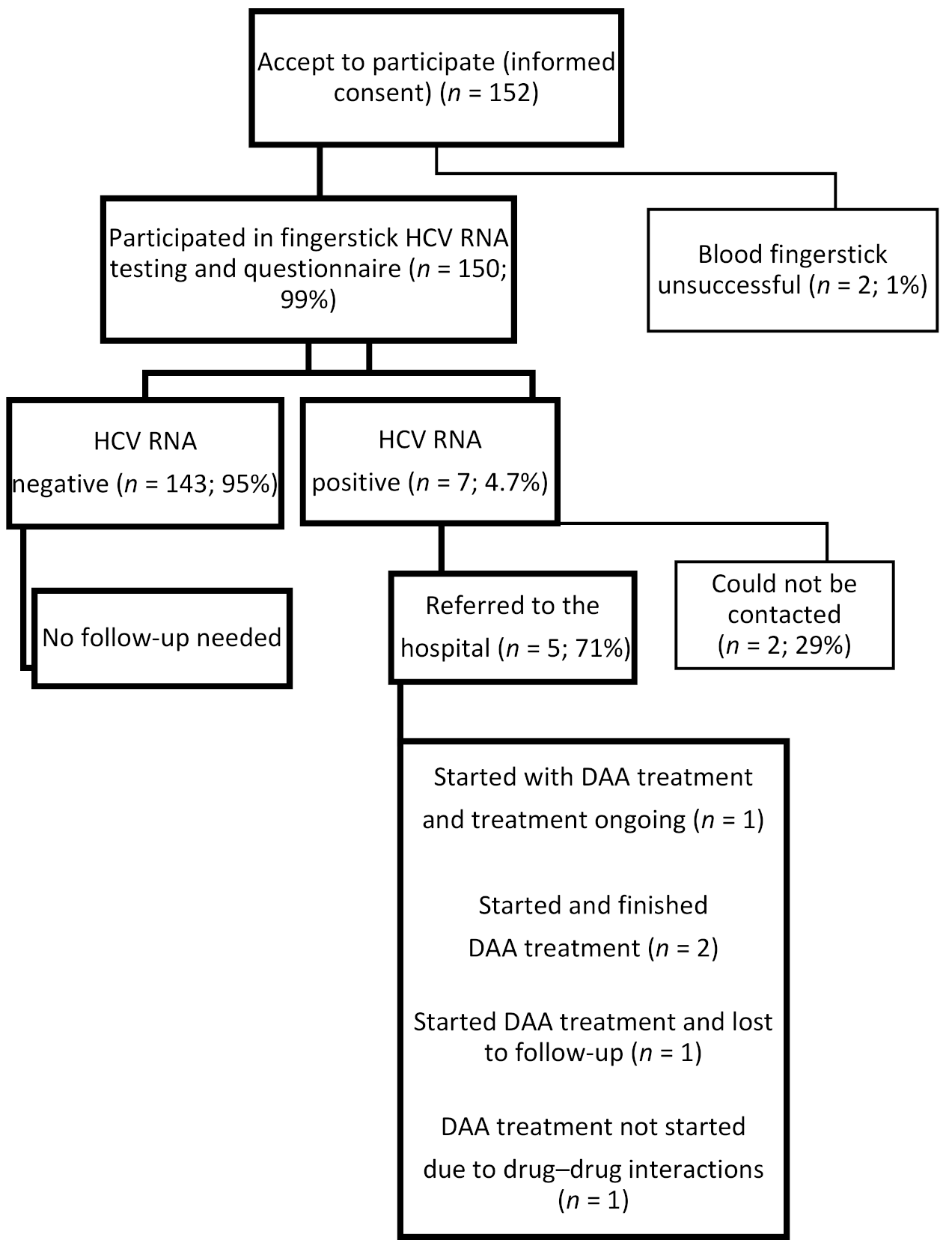
3.3. Linkage to Care
3.4. Risk Factors for HCV RNA Positivity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perz, J.F.; Armstrong, G.L.; Farrington, L.A.; Hutin, Y.J.; Bell, B.P. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J. Hepatol. 2006, 45, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Thein, H.H.; Yi, Q.; Dore, G.J.; Krahn, M.D. Estimation of stage-specific fibrosis progression rates in chronic hepatitis C virus infection: A meta-analysis and meta-regression. Hepatology 2008, 48, 418–431. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Geneva. 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/246177/WHO-HIV-2016.06-eng.pdf;jsessionid=F32ABD1E0EBB024BEBE9509F73FA8B88?sequence=1 (accessed on 29 June 2021).
- Thomas, D.L. Global Elimination of Chronic Hepatitis. N. Engl. J. Med. 2019, 380, 2041–2050. [Google Scholar] [CrossRef] [PubMed]
- Vermeiren, A.P.; Dukers-Muijrers, N.H.; van Loo, I.H.; Stals, F.; van Dam, D.W.; Ambergen, T.; Hoebe, C.J.P.A. Identification of hidden key hepatitis C populations: An evaluation of screening practices using mixed epidemiological methods. PLoS ONE 2012, 7, e51194. [Google Scholar] [CrossRef]
- Poel, A.v.d.; Lindt, S.v.d.; Laghaei, F.; Croes, E. Verbetering van de opsporing van hepatitis C in de verslavingszorg. Resultaten van doorbraakproject 2013–2014. Tijdschr. Gezondh. 2015, 93, 129–131. [Google Scholar] [CrossRef]
- Kracht, P.A.M.; de Gee, E.A.; van der Poel, A.; Verhagen, M.; Hoepelman, A.I.M.; Croes, E.A.; Arends, J.E. Introducing hepatitis C virus healthcare pathways in addiction care in the Netherlands with a Breakthrough project: A mixed method study. Harm. Reduct. J. 2019, 16, 45. [Google Scholar] [CrossRef]
- Koopsen, J.; van Steenbergen, J.E.; Richardus, J.H.; Prins, M.; Op de Coul, E.L.M.; Croes, E.A.; Heil, J.; Zuure, F.R.; Veldhuijzen, I.K. Chronic hepatitis B and C infections in the Netherlands: Estimated prevalence in risk groups and the general population. Epidemiol. Infect. 2019, 147, e147. [Google Scholar] [CrossRef]
- Health Council of The Netherlands. Screening Risk Groups for Hepatitis B and C. The Hague: Health Council of the Netherlands; Publication No. 2016/16. 2016. Available online: https://www.healthcouncil.nl/binaries/healthcouncil/documents/advisory-reports/2016/11/01/screening-risk-groups-for-hepatitis-b-and-c/summary-screening-risk-groups-for-hepatitis-b-and-c.pdf (accessed on 29 June 2021).
- van Santen, D.K.; van der Helm, J.J.; Lindenburg, K.; Schim van der Loeff, M.; Prins, M. HIV and hepatitis C treatment uptake among people who use drugs participating in the Amsterdam Cohort Studies, 1985–2015. Int. J. Drug Policy 2017, 47, 95–101. [Google Scholar] [CrossRef]
- Lindenburg, C.E.; Lambers, F.A.; Urbanus, A.T.; Schinkel, J.; Jansen, P.L.; Krol, A.; Casteelen, G.; van Santen, G.; van den Berg, C.H.S.B.; Coutinho, R.A.; et al. Hepatitis C testing and treatment among active drug users in Amsterdam: Results from the DUTCH-C project. Eur. J. Gastroenterol. Hepatol. 2011, 23, 23–31. [Google Scholar] [CrossRef]
- Logtenberg-van der Grient, H.W.R.; van Woerden, E.; Schatz, E. Hepatitis C: Van testen tot behandelen. Opsporen van hepatitis C-positieve cliënten van de Maatschappelijke Opvang in Amsterdam. Tijdschr. Voor Gezondh. 2019, 97, 116–121. [Google Scholar] [CrossRef][Green Version]
- Bajis, S.; Dore, G.J.; Hajarizadeh, B.; Cunningham, E.B.; Maher, L.; Grebely, J. Interventions to enhance testing, linkage to care and treatment uptake for hepatitis C virus infection among people who inject drugs: A systematic review. Int. J. Drug. Policy 2017, 47, 34–46. [Google Scholar] [CrossRef]
- Bottero, J.; Boyd, A.; Gozlan, J.; Carrat, F.; Nau, J.; Pauti, M.D.; Rougier, H.; Girard, P.-M.; Lacombe, K. Simultaneous Human Immunodeficiency Virus-Hepatitis B-Hepatitis C Point-of-Care Tests Improve Outcomes in Linkage-to-Care: Results of a Randomized Control Trial in Persons Without Healthcare Coverage. Open Forum. Infect Dis. 2015, 2, ofv162. [Google Scholar] [CrossRef]
- Grebely, J.; Lamoury, F.M.J.; Hajarizadeh, B.; Mowat, Y.; Marshall, A.D.; Bajis, S.; Marks, P.; Amin, J.; Smith, J.; Edwards, M.; et al. Evaluation of the Xpert HCV Viral Load point-of-care assay from venepuncture-collected and finger-stick capillary whole-blood samples: A cohort study. Lancet Gastroenterol. Hepatol. 2017, 2, 514–520. [Google Scholar] [CrossRef]
- Degenhardt, L.; Peacock, A.; Colledge, S.; Leung, J.; Grebely, J.; Vickerman, P.; Stone, J.; Cunningham, E.B.; Trickey, A.; Dumchev, K.; et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of, HIV.; HBV, and HCV in people who inject drugs: A multistage systematic review. Lancet Glob. Health. 2017, 5, e1192–e1207. [Google Scholar] [CrossRef]
- Benova, L.; Mohamoud, Y.A.; Calvert, C.; Abu-Raddad, L.J. Vertical transmission of hepatitis C virus: Systematic review and meta-analysis. Clin. Infect Dis. 2014, 59, 765–773. [Google Scholar] [CrossRef]
- Greenland, S.; Mansournia, M.A.; Altman, D.G. Sparse data bias: A problem hiding in plain sight. BMJ 2016, 352, i1981. [Google Scholar] [CrossRef]
- Greenland, S.; Mansournia, M.A. Penalization, bias reduction, and default priors in logistic and related categorical and survival regressions. Stat. Med. 2015, 34, 3133–3143. [Google Scholar] [CrossRef]
- Newsum, A.M.; Matser, A.; Schinkel, J.; van der Valk, M.; Brinkman, K.; van Eeden, A.; Lauw, F.N.; Rijnders, B.J.; van de Laar, T.J.W.; van de Kerkhof, M.; et al. Incidence of HCV reinfection among HIV-positive MSM and its association with sexual risk behavior: A longitudinal analysis. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- ECDC. European Center for Disease Prevention and Control. Technical Report. Hepatitis B and C Epidemiology in Selected Population Groups in the EU/EEA. 2018. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Hepatitis-B-C-epidemiology-in-selected-populations-in-the-EU.pdf (accessed on 29 June 2021).
- Avramovic, G.; Oprea, C.; Surey, J.; Story, A.; Macías, J.; Cullen, W.; Iglesias, M.; Mc Hugh, T.; Crowley, D.; Naughton, A.M.; et al. HepCare Europe-A service innovation project. HepCheck: Characteristics of the patient population with active infection as defined by HCV RNA. Int. J. Infect. Dis. 2020, 91, 246–251. [Google Scholar] [CrossRef]
- Roy, K.; Hay, G.; Andragetti, R.; Taylor, A.; Goldberg, D.; Wiessing, L. Monitoring hepatitis C virus infection among injecting drug users in the European Union: A review of the literature. Epidemiol. Infect. 2002, 129, 577–585. [Google Scholar] [CrossRef]
- Barror, S.; Avramovic, G.; Oprea, C.; Surey, J.; Story, A.; Macías, J.; Cullen, W.; Crowley, D.; Horan, A.; Naughton, A.M.; et al. HepCare Europe: A service innovation project. HepCheck: Enhancing HCV identification and linkage to care for vulnerable populations through intensified outreach screening: A prospective multisite feasibility study. J. Antimicrob. Chemother. 2019, 74 (Suppl. 5), v39–v46. [Google Scholar] [CrossRef]
- Alavi, M.; Poustchi, H.; Merat, S.; Kaveh-Ei, S.; Rahimi-Movaghar, A.; Shadloo, B.; Hajarizadeh, B.; Grebely, J.; Dore, G.J.; Malekzadeh, R. An intervention to improve HCV testing, linkage to care, and treatment among people who use drugs in Tehran, Iran: The ENHANCE study. Int. J. Drug Policy 2019, 72, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Bajis, S.; Grebely, J.; Cooper, L.; Smith, J.; Owen, G.; Chudleigh, A.; Hajarizadeh, B.; Martinello, M.; Adey, S.; Read, P.; et al. Hepatitis C virus testing, liver disease assessment and direct-acting antiviral treatment uptake and outcomes in a service for people who are homeless in Sydney, Australia: The LiveRLife homelessness study. J. Viral. Hepat. 2019, 26, 969–979. [Google Scholar]
- Fokuo, J.K.; Masson, C.L.; Anderson, A.; Powell, J.; Bush, D.; Ricco, M.; Zevin, B.; Ayala, C.; Khalili, M. Recommendations for Implementing Hepatitis C Virus Care in Homeless Shelters: The Stakeholder Perspective. Hepatol. Commun. 2020, 4, 646–656. [Google Scholar] [CrossRef] [PubMed]
- Lambert, J.S.; Murtagh, R.; Menezes, D.; O’Carroll, A.; Murphy, C.; Cullen, W.; McHugh, T.; Avramovic, G.; Tinago, W.; Hout, M.C.V. ‘HepCheck Dublin’: An intensified hepatitis C screening programme in a homeless population demonstrates the need for alternative models of care. BMC Infect. Dis. 2019, 19, 128. [Google Scholar] [CrossRef]
- Harney, B.L.; Whitton, B.; Lim, C.; Paige, E.; McDonald, B.; Nolan, S.; Pemberton, D.; Hellard, M.E.; Doyle, J.S. Quantitative evaluation of an integrated nurse model of care providing hepatitis C treatment to people attending homeless services in Melbourne, Australia. Int. J. Drug Policy 2019, 72, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Arum, C.; Fraser, H.; Artenie, A.A.; Bivegete, S.; Trickey, A.; Alary, M.; Astemborski, J.; Iversen, J.; Lim, A.G.; MacGregor, L.; et al. Homelessness, unstable housing, and risk of HIV and hepatitis C virus acquisition among people who inject drugs: A systematic review and meta-analysis. Lancet Public Health 2021, 6, e309–e323. [Google Scholar] [CrossRef]
- Harney, B.; McColl, R.; Pedrana, A.; Morrison, E.; Doyle, J.; Hellard, M.; Higgs, P. Letter to the Editor: Recommendations for Implementing Hepatitis C Virus Care in Homeless Shelters: The Stakeholder Perspective. Hepatol. Commun. 2021, 5, 146–147. [Google Scholar] [CrossRef]
- Global prevalence and genotype distribution of hepatitis C virus infection in 2015: A modelling study. Lancet Gastroenterol. Hepatol. 2017, 2, 161–176. [CrossRef]
- Wiessing, L.; Likatavicius, G.; Hedrich, D.; Guarita, B.; van de Laar, M.J.; Vicente, J. Trends in HIV and hepatitis C virus infections among injecting drug users in Europe, 2005 to 2010. Eurosurveillance 2011, 16, 20031. [Google Scholar] [CrossRef]
- Statistics The Netherlands (CBS). How Many Immigrants Come to The Netherlands? 2020. Available online: https://www.cbs.nl/nl-nl/dossier/dossier-asiel-migratie-en-integratie/hoeveel-immigranten-komen-naar-nederland-#:~:text=In%202020%20immigreerden%20219%20250,minder%20dan%20een%20jaar%20eerder (accessed on 29 June 2021).
- World Health Organization. Combating Hepatitis B and C to Reach Elimination by 2030. 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/206453/WHO_HIV_2016.04_eng.pdf;jsessionid=F56A6BBF13DD1D6BCB479DB9EB318948?sequence=1 (accessed on 29 June 2021).


{kind=link}
| N | Percentage or Median (IQR) | TotalN * | |
| Sociodemographic characteristics | |||
| Male sex | 132 | 87% | 151 |
| Age in years | 47 (38–56) | 152 | |
| Continent/country of birth | 152 | ||
| Western Europe, The Netherlands | 41 | 27% | |
| Western/Northern Europe (other) | 8 | 5.3% | |
| Eastern Europe (Former Soviet Union) | 26 | 17% | |
| Africa | 34 | 22% | |
| South America, Suriname | 22 | 15% | |
| North America, USA | 1 | 0.7% | |
| Caribbean/Antilles | 14 | 9.2% | |
| Central Asia (Middle East) | 6 | 3.9% | |
| N | Percentage or Median (IQR) | TotalN * | |
| Current treatment | |||
| Methadone treatment, yes | 25 | 17% | 149 |
| Homeless service/test location in Amsterdam | 152 | ||
| Long-term shelter | 68 | 45% | |
| Short-term shelter | 30 | 20% | |
| Mixed center (short- and long-term) | 17 | 11% | |
| Drop-in center | 37 | 24% | |
| HCV-related risk factors | |||
| Procedures in HCV endemic country (lifetime) | |||
| Medical procedure | 16 | 11% | 146 |
| Blood transfusion | 4 | 2.8% | 144 |
| Tattoo or piercing | 29 | 20% | 146 |
| Dental procedures | 23 | 16% | 144 |
| Procedures in the Netherlands (lifetime) | |||
| Tattoo/piercing in a nonregistered location | 26 | 18% | 142 |
| Injecting drugs (ever) | 22 | 15% | 146 |
| Injecting drugs (last 30 days) | 10 | 6.7% | 149 |
| Ever sharing of: | |||
| needles and/or syringes | 7 | 4.8% | 146 |
| straws and/or crack pipe | 70 | 48% | 146 |
| razors and/or toothbrushes | 35 | 25% | 140 |
| Sexual behavior | |||
| Condomless anal sex by men (ever) | 15 | 13% | 120 |
| Ever sharing sex toys | 11 | 8.1% | 136 |
| Medical history related to HCV | |||
| Had been previously tested for HCV (1985–2019) ** | 38 | 66% | 110 |
| Had previously tested positive for HCV | 7 | 22% | 32 |
| HCV RNA testing | |||
| Participated in HCV RNA testing | 152 | ||
| Yes | 150 | 99% | |
| No, fingerstick unsuccessful *** | 2 | 1.3% | |
| Result HCV RNA test | 150 | ||
| Negative | 143 | 95% | |
| Positive | 7 | 4.7% | |
| Unaware of HCV RNA positivity | 5 | 71% | 7 |
| HCV RNA Negative (N = 143), Median (IQR) or Number/N (%) | HCV RNA Positive (N = 7), Median (IQR) or Number/N (%) | Prior OR (95% CrI) | Posterior OR (95% CrI) | |
|---|---|---|---|---|
| Sociodemographic characteristics | ||||
| Age (per 10 year increase) a | 47 (39–56) | 33 (29–59) | 0.90 (0.23–3.60) | 0.67 (0.40–1.12) |
| Females (versus males) | 18/142 (12.7) | 1/7 (14.3) | 1.00 (0.25–4.00) | 1.02 (0.30–3.24) |
| Eastern European origin | 20/143 (14.0) | 5/7 (71.4) | 1.50 (0.38–6.00) | 3.59 (1.27–10.04) |
| HCV-related risk factors | ||||
| Injecting drug use (ever) | 18/138 (13.0) | 4/6 (66.7) | 2.00 (0.50–8.00) | 3.89 (1.37–11.09) |
| Injecting drug use (last 30 days) | 7/141 (5.0) | 3/6 (50.0) | 2.00 (0.50–8.00) | 3.94 (1.29–11.71) |
| Ever sharing needles or syringes | 5/138 (3.6) | 2/6 (33.3) | 2.00 (0.50–8.00) | 3.16 (0.96–9.39) |
| Ever sharing straws/crack pipe | 65/138 (47.1) | 4/6 (66.7) | 1.50 (0.38–6.00) | 1.69 (0.56–4.95) |
| Ever sharing razors/toothbrush | 35/134 (26.1) | 1/5 (20.0) | 1.50 (0.38–6.00) | 1.47 (0.38–3.78) |
| Procedures b in HCV endemic country | 46/138 (33.3) | 1/6 (16.7) | 1.50 (0.38–6.00) | 1.00 (0.32–2.81) |
| Tattoo/piercing in nonregistered location c | 25/134 (18.7) | 1/7 (14.3) | 1.50 (0.38–6.00) | 1.10 (0.35–3.09) |
| Sexual behavior | ||||
| Condomless anal sex | 16/130 (14.0) | 0/4 (0) | 1.50 (0.38–6.00) | 1.05 (0.29–3.47) |
| Sharing of sex toys | 11/114 (8.5) | 0/5 (0) | 1.50 (0.38–6.00) | 1.14 (0.31–3.80) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Generaal, E.; Logtenberg van der Grient, H.; Schatz, E.; van Santen, D.K.; Boyd, A.; Woods, S.K.; Baak, B.L.C.; Prins, M. A Feasibility Study to Increase Chronic Hepatitis C Virus RNA Testing and Linkage to Care among Clients Attending Homeless Services in Amsterdam, The Netherlands. Diagnostics 2021, 11, 1197. https://doi.org/10.3390/diagnostics11071197
Generaal E, Logtenberg van der Grient H, Schatz E, van Santen DK, Boyd A, Woods SK, Baak BLC, Prins M. A Feasibility Study to Increase Chronic Hepatitis C Virus RNA Testing and Linkage to Care among Clients Attending Homeless Services in Amsterdam, The Netherlands. Diagnostics. 2021; 11(7):1197. https://doi.org/10.3390/diagnostics11071197
Chicago/Turabian StyleGeneraal, Ellen, Hilje Logtenberg van der Grient, Eberhard Schatz, Daniela K. van Santen, Anders Boyd, Sara K. Woods, Bert L. C. Baak, and Maria Prins. 2021. "A Feasibility Study to Increase Chronic Hepatitis C Virus RNA Testing and Linkage to Care among Clients Attending Homeless Services in Amsterdam, The Netherlands" Diagnostics 11, no. 7: 1197. https://doi.org/10.3390/diagnostics11071197
APA StyleGeneraal, E., Logtenberg van der Grient, H., Schatz, E., van Santen, D. K., Boyd, A., Woods, S. K., Baak, B. L. C., & Prins, M. (2021). A Feasibility Study to Increase Chronic Hepatitis C Virus RNA Testing and Linkage to Care among Clients Attending Homeless Services in Amsterdam, The Netherlands. Diagnostics, 11(7), 1197. https://doi.org/10.3390/diagnostics11071197