
Arterial Digital Pulse Photoplethysmography in Patients with Suspected Thoracic Outlet Syndrome: A Study of the “Ca+Pra” Maneuver

 and
and
Abstract
1. Introduction
2. Materials and Methods
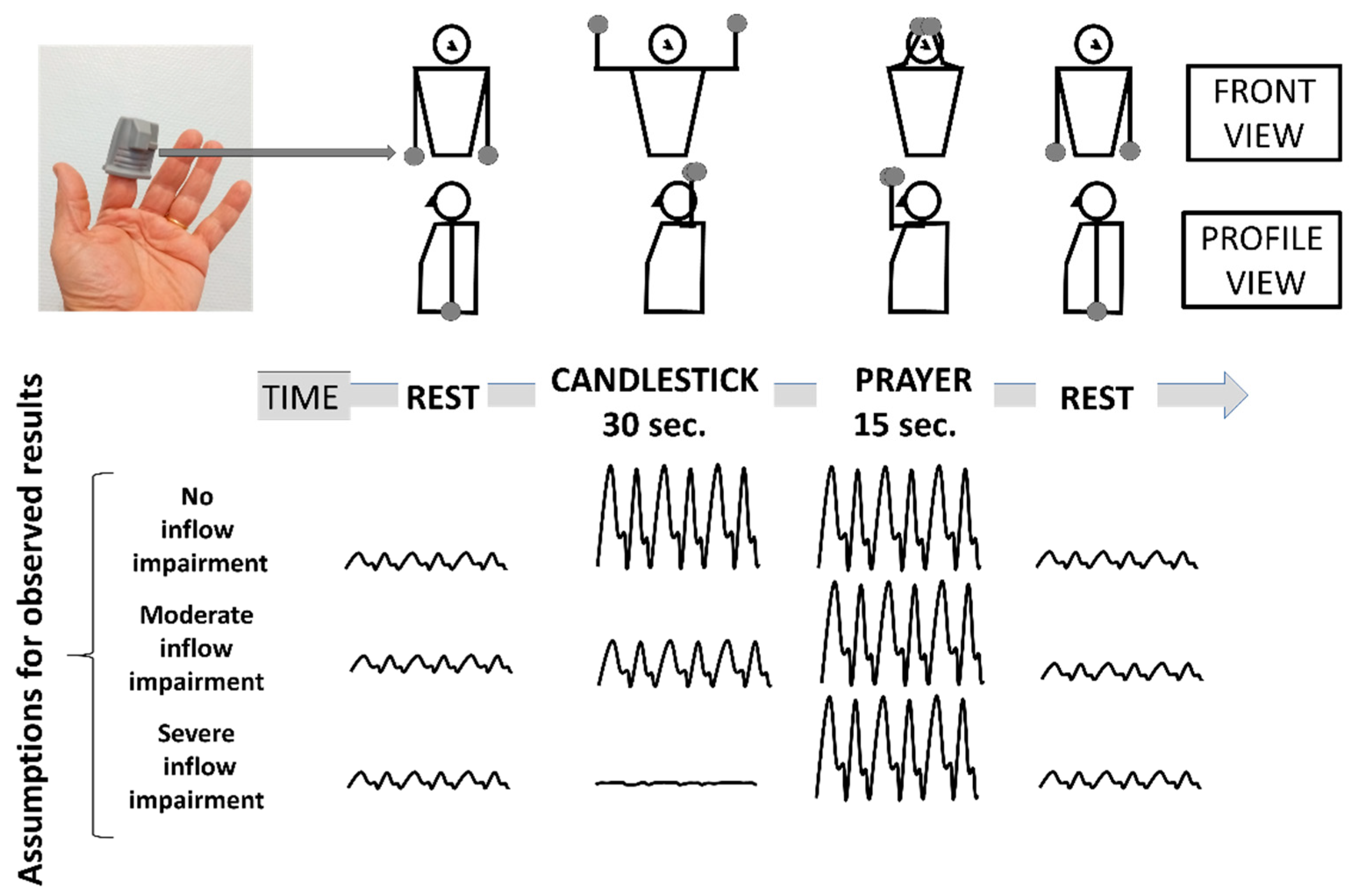
2.1. Experimental Design
2.2. Attitudinal Maneuvers
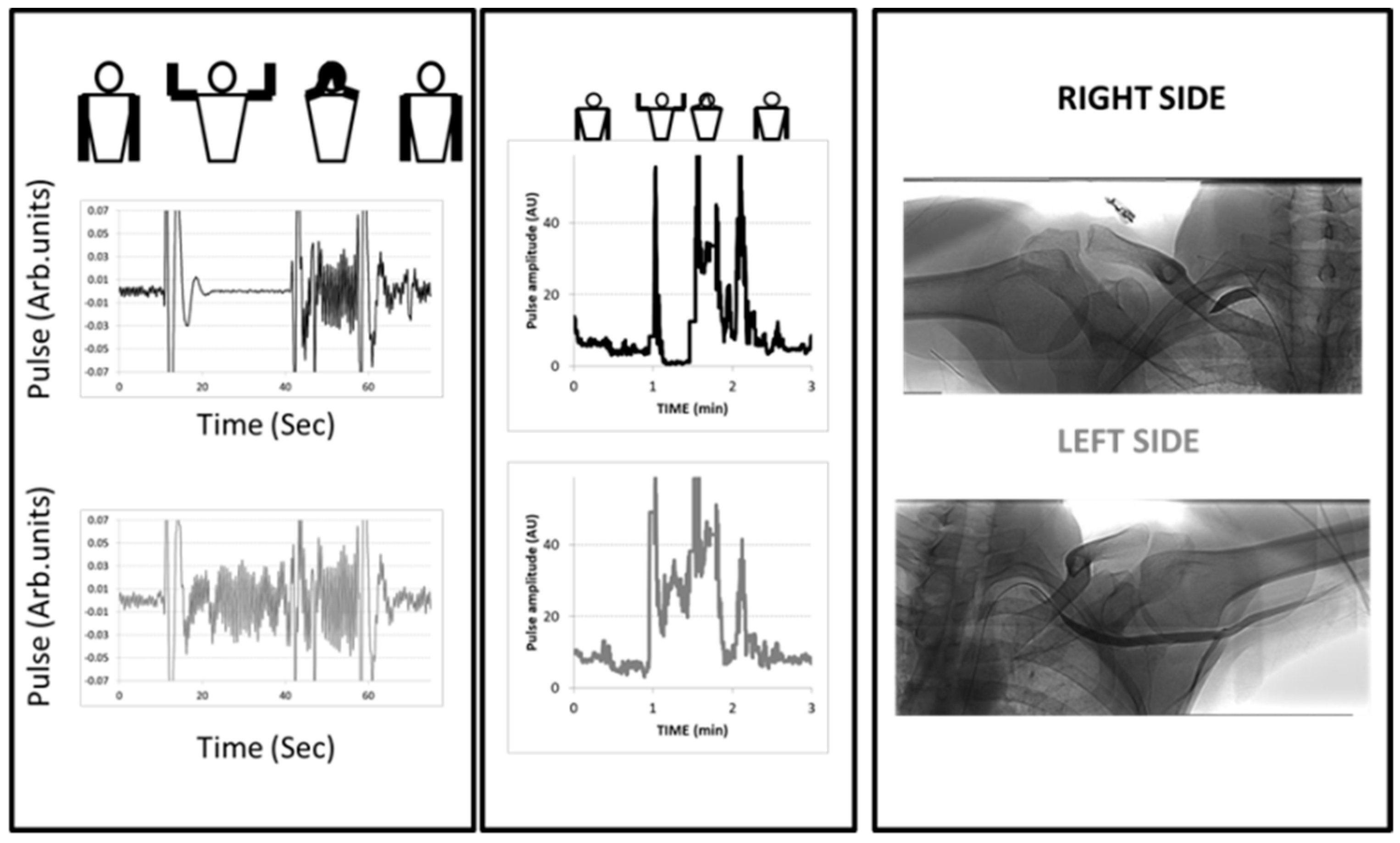
2.3. Photoplethysmography Recordings
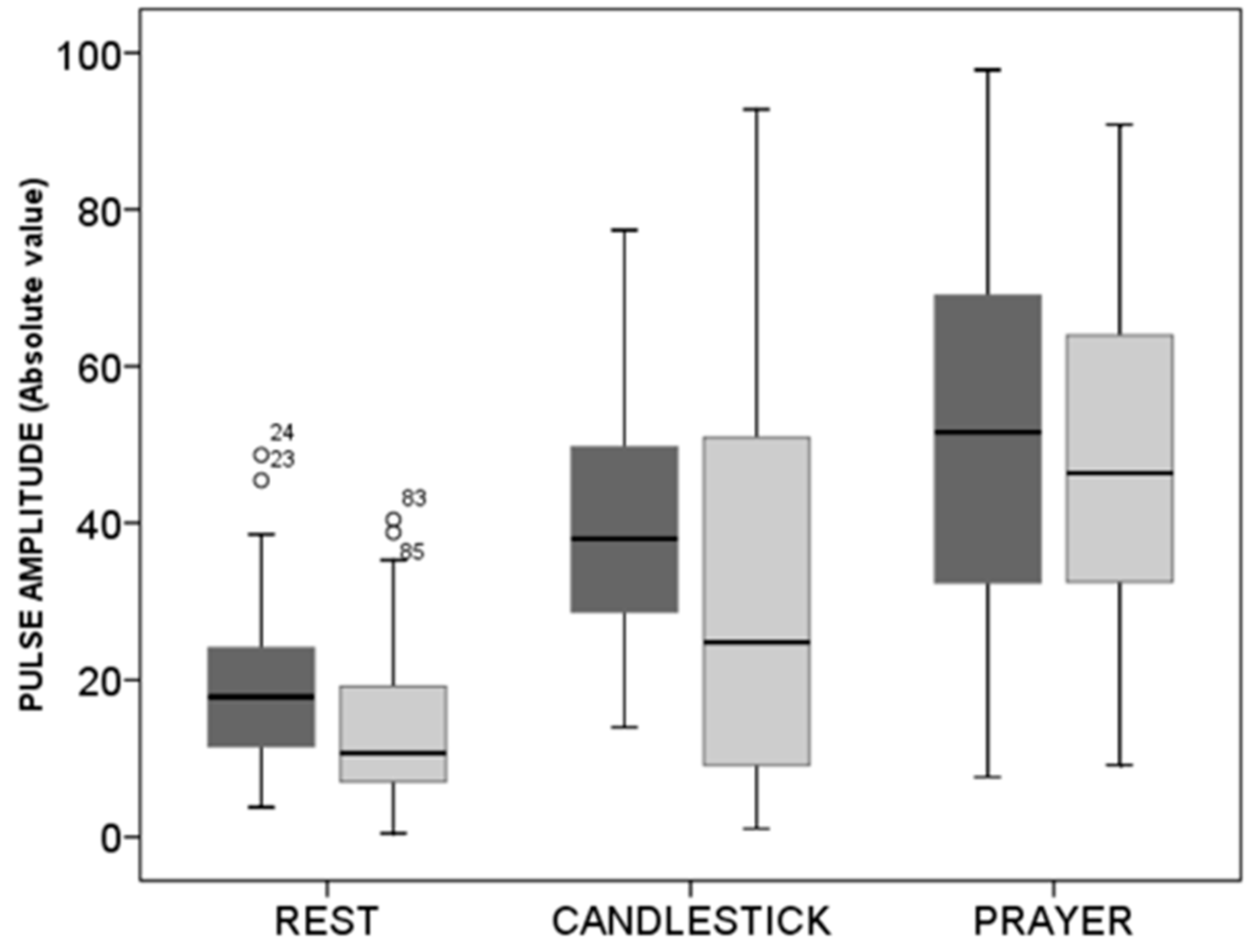
2.4. Statistical Analysis
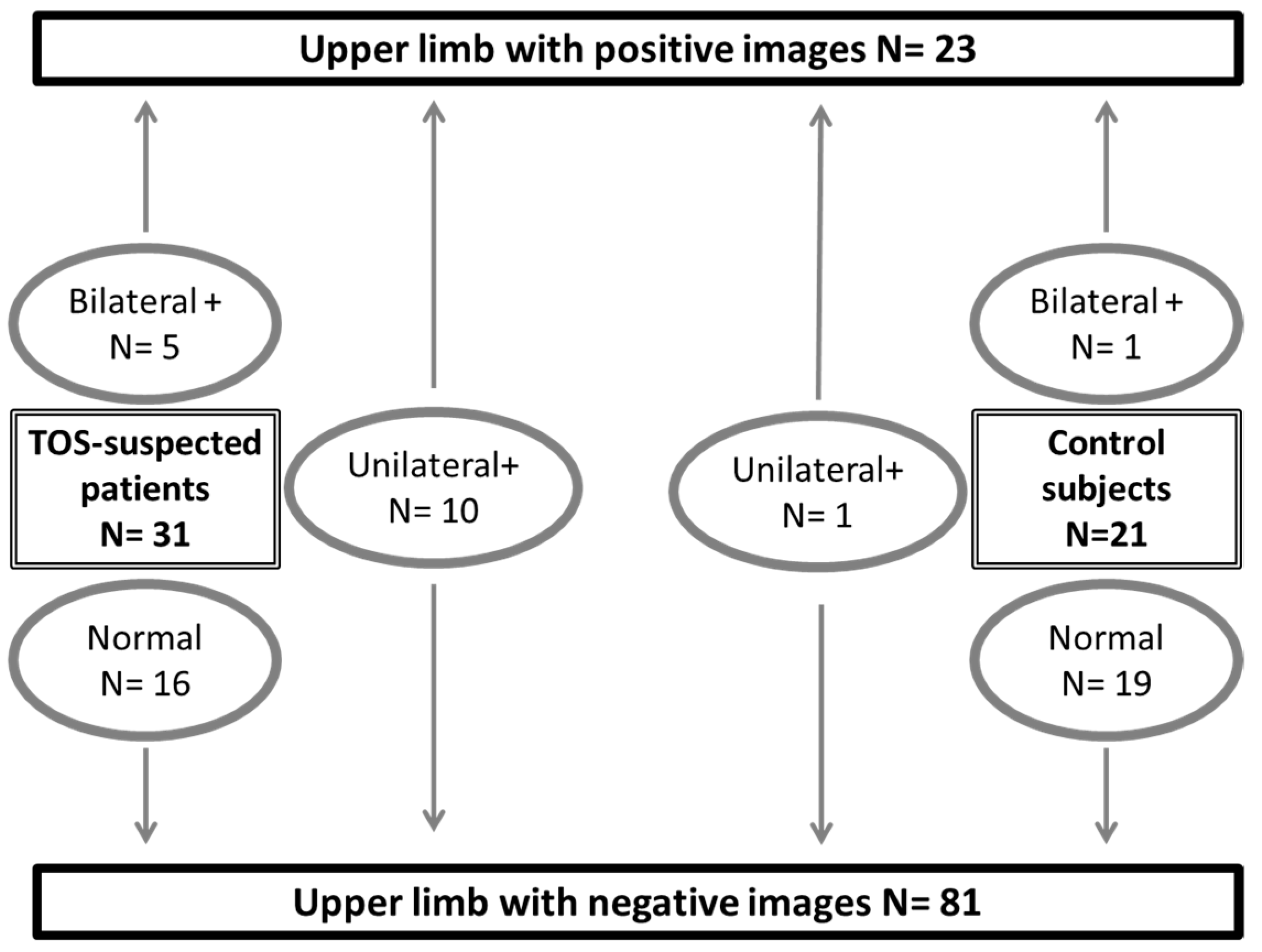
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Illig, K.A. Neurogenic thoracic outlet syndrome: Bringing order to chaos. J. Vasc. Surg. 2018, 68, 939–940. [Google Scholar] [CrossRef]
- Burt, B.M. Thoracic outlet syndrome for thoracic surgeons. J. Thorac. Cardiovasc. Surg. 2018, 156, 1318–1323.e1. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, J.; Kanwal, A. Thoracic Outlet Syndrome; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Ferrante, M.A.; Ferrante, N.D. The thoracic outlet syndromes: Part 1. Overview of the thoracic outlet syndromes and review of true neurogenic thoracic outlet syndrome. Muscle Nerve 2017, 55, 782–793. [Google Scholar] [CrossRef]
- Ferrante, M.A.; Ferrante, N.D. The thoracic outlet syndromes: Part 2. The arterial, venous, neurovascular, and disputed thoracic outlet syndromes. Muscle Nerve 2017, 56, 663–673. [Google Scholar] [CrossRef]
- Longley, D.G.; Yedlicka, J.W.; Molina, E.J.; Schwabacher, S.; Hunter, D.W.; Letourneau, J.G. Thoracic outlet syndrome: Evaluation of the subclavian vessels by color duplex sonography. AJR Am. J. Roentgenol. 1992, 158, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Povlsen, S.; Povlsen, B. Diagnosing Thoracic Outlet Syndrome: Current Approaches and Future Directions. Diagnostics 2018, 8, 21. [Google Scholar] [CrossRef]
- Sallstrom, J.; Thulesius, O. Non-invasive investigation of vascular compression in patients with thoracic outlet syndrome. Clin. Physiol. 1982, 2, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Geven, L.I.; Smit, A.J.; Ebels, T. Vascular thoracic outlet syndrome. Longer posterior rib stump causes poor outcome. Eur. J. Cardio-Thorac. Surg. 2006, 30, 232–236. [Google Scholar] [CrossRef]
- Chen, H.; Doornbos, N.; Williams, K.; Criado, E. Physiologic variations in venous and arterial hemodynamics in response to postural changes at the thoracic outlet in normal volunteers. Ann. Vasc. Surg. 2014, 28, 1583–1588. [Google Scholar] [CrossRef]
- Lai, D.T.; Walsh, J.; Harris, J.P.; May, J. Predicting outcomes in thoracic outlet syndrome. Med. J. Aust. 1995, 162, 345–347. [Google Scholar] [CrossRef]
- Colon, E.; Westdorp, R. Vascular compression in the thoracic outlet. Age dependent normative values in noninvasive testing. J. Cardiovasc. Surg. (Torino) 1988, 29, 166–171. [Google Scholar]
- Gergoudis, R.; Barnes, R.W. Thoracic outlet arterial compression: Prevalence in normal persons. Angiology 1980, 31, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Adam, G.; Wang, K.; Demaree, C.J.; Jiang, J.S.; Cheung, M.; Bechara, C.F.; Lin, P.H. A Prospective Evaluation of Duplex Ultrasound for Thoracic Outlet Syndrome in High-Performance Musicians Playing Bowed String Instruments. Diagnostics 2018, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Hickey, M.; Phillips, J.P.; Kyriacou, P.A. The effect of vascular changes on the photoplethysmographic signal at different hand elevations. Physiol. Meas. 2015, 36, 425–440. [Google Scholar] [CrossRef] [PubMed]
- Hickey, M.; Phillips, J.P.; Kyriacou, P.A. Investigation of peripheral photoplethysmographic morphology changes induced during a hand-elevation study. J. Clin. Monit. Comput. 2016, 30, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Goksuluk, D.; Korkmaz, S.; Zararsiz, G.; Karaagaoglu, A.E. EasyROC: An interactive web-tool for ROC curve analysis using R language environment. R J. 2016, 8, 213–230. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983, 148, 839–843. [Google Scholar] [CrossRef]
- Illig, K.A.; Donahue, D.; Duncan, A.; Freischlag, J.; Gelabert, H.; Johansen, K.; Jordan, S.; Sanders, R.; Thompson, R. Reporting standards of the Society for Vascular Surgery for thoracic outlet syndrome. J. Vasc. Surg. 2016, 64, e23–e35. [Google Scholar] [CrossRef]
- Likes, K.; Rochlin, D.H.; Call, D.; Freischlag, J.A. Coexistence of arterial compression in patients with neurogenic thoracic outlet syndrome. JAMA Surg. 2014, 149, 1240–1243. [Google Scholar] [CrossRef]
- Molina, J.E.; D’Cunha, J. The vascular component in neurogenic-arterial thoracic outlet syndrome. Int. J. Angiol. 2008, 17, 83–87. [Google Scholar] [CrossRef]
- Nord, K.M.; Kapoor, P.; Fisher, J.; Thomas, G.; Sundaram, A.; Scott, K.; Kothari, M.J. False positive rate of thoracic outlet syndrome diagnostic maneuvers. Electromyogr. Clin. Neurophysiol. 2008, 48, 67–74. [Google Scholar] [PubMed]
- Sobey, A.V.; Grewal, R.P.; Hutchison, K.J.; Urschel, J.D. Investigation of nonspecific neurogenic thoracic outlet syndrome. J. Cardiovasc. Surg. (Torino) 1993, 34, 343–345. [Google Scholar]
- Suzuki, J.; Maeda, J.; Takemiya, T. Analysis of microvascular responses in the finger to changes in arm position during cold water stimulation. Jpn. J. Physiol. 1994, 44, 181–191. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jagomagi, K.; Raamat, R.; Talts, J.; Ragun, U.; Lansimies, E.; Jurvelin, J. Recording of dynamic arterial compliance changes during hand elevation. Clin. Physiol. Funct. Imaging 2005, 25, 350–356. [Google Scholar] [CrossRef]
- Hixson, K.M.; Horris, H.B.; McLeod, T.C.V.; Bacon, C.E.W. The Diagnostic Accuracy of Clinical Diagnostic Tests for Thoracic Outlet Syndrome. J. Sport Rehabil. 2017, 26, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, F.; Zuazo, I.; Bonnefoy, O.; Abric, B.; Borocco, A.; Strainchamps, P.; Tauzin, C.; Faure, D.; Minniti, A.; Ledoyer, G.; et al. Diagnosis of thoracic outlet syndrome. Value of angiography in the sitting position. J. Radiol. 2008, 89, 47–52. [Google Scholar] [CrossRef]
- Henni, S.; Hersant, J.; Ammi, M.; Mortaki, F.E.; Picquet, J.; Feuilloy, M.; Abraham, P. Microvascular Response to the Roos Test Has Excellent Feasibility and Good Reliability in Patients with Suspected Thoracic Outlet Syndrome. Front. Physiol. 2019, 10, 136. [Google Scholar] [CrossRef]
- Abraham, P.; Hersant, J.; Ramondou, P.; Thouveny, F.; Feuilloy, M.; Picquet, J.; Henni, S. Comparison of transcutaneous oximetry with symptoms and arteriography in thoracic outlet syndrome. Clin. Hemorheol. Microcirc. 2020, 75, 107–119. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area under ROC Curve | Significance of the AUC | Asymptotic 95%CI Lower Limit | Asymptotic 95%CI Upper Limit | |
|---|---|---|---|---|
| Absolute change from rest (AU) | 0.715 ± 0.066 | 0.002 | 0.585 | 0.845 |
| Percentage change from rest (%) | 0.733 ± 0.071 | 0.001 | 0.616 | 0.851 |
| Pulse amplitude change (NA) | 0.765 ± 0.065 | 0.000 | 0.637 | 0.891 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hersant, J.; Ramondou, P.; Thouveny, F.; Daligault, M.; Feuilloy, M.; Saulnier, P.; Abraham, P.; Henni, S. Arterial Digital Pulse Photoplethysmography in Patients with Suspected Thoracic Outlet Syndrome: A Study of the “Ca+Pra” Maneuver. Diagnostics 2021, 11, 1128. https://doi.org/10.3390/diagnostics11061128
Hersant J, Ramondou P, Thouveny F, Daligault M, Feuilloy M, Saulnier P, Abraham P, Henni S. Arterial Digital Pulse Photoplethysmography in Patients with Suspected Thoracic Outlet Syndrome: A Study of the “Ca+Pra” Maneuver. Diagnostics. 2021; 11(6):1128. https://doi.org/10.3390/diagnostics11061128
Chicago/Turabian StyleHersant, Jeanne, Pierre Ramondou, Francine Thouveny, Mickael Daligault, Mathieu Feuilloy, Patrick Saulnier, Pierre Abraham, and Samir Henni. 2021. "Arterial Digital Pulse Photoplethysmography in Patients with Suspected Thoracic Outlet Syndrome: A Study of the “Ca+Pra” Maneuver" Diagnostics 11, no. 6: 1128. https://doi.org/10.3390/diagnostics11061128
APA StyleHersant, J., Ramondou, P., Thouveny, F., Daligault, M., Feuilloy, M., Saulnier, P., Abraham, P., & Henni, S. (2021). Arterial Digital Pulse Photoplethysmography in Patients with Suspected Thoracic Outlet Syndrome: A Study of the “Ca+Pra” Maneuver. Diagnostics, 11(6), 1128. https://doi.org/10.3390/diagnostics11061128