
3D Occlusal Tooth Wear Assessment in Presence of Limited Changes in Non-Occlusal Surfaces

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Tooth Wear Simulation
2.3. 3D Model Acquisition
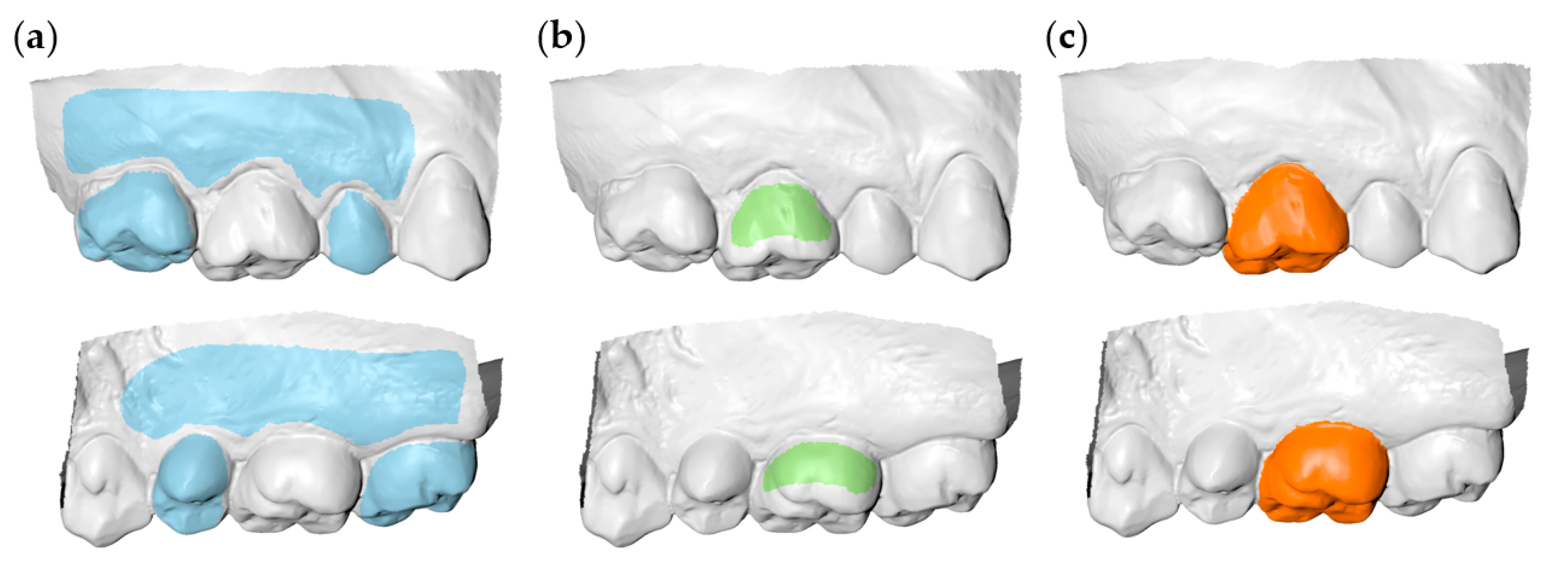
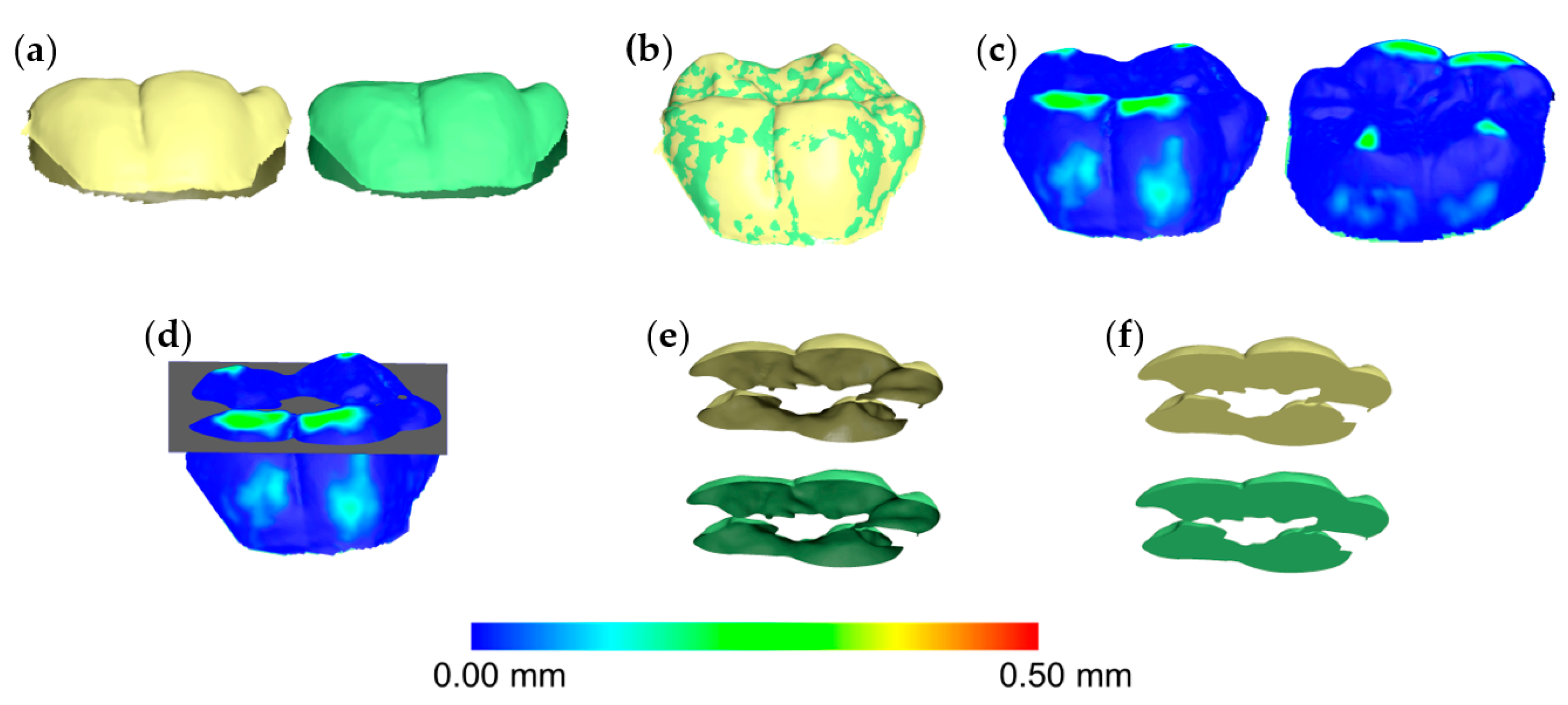
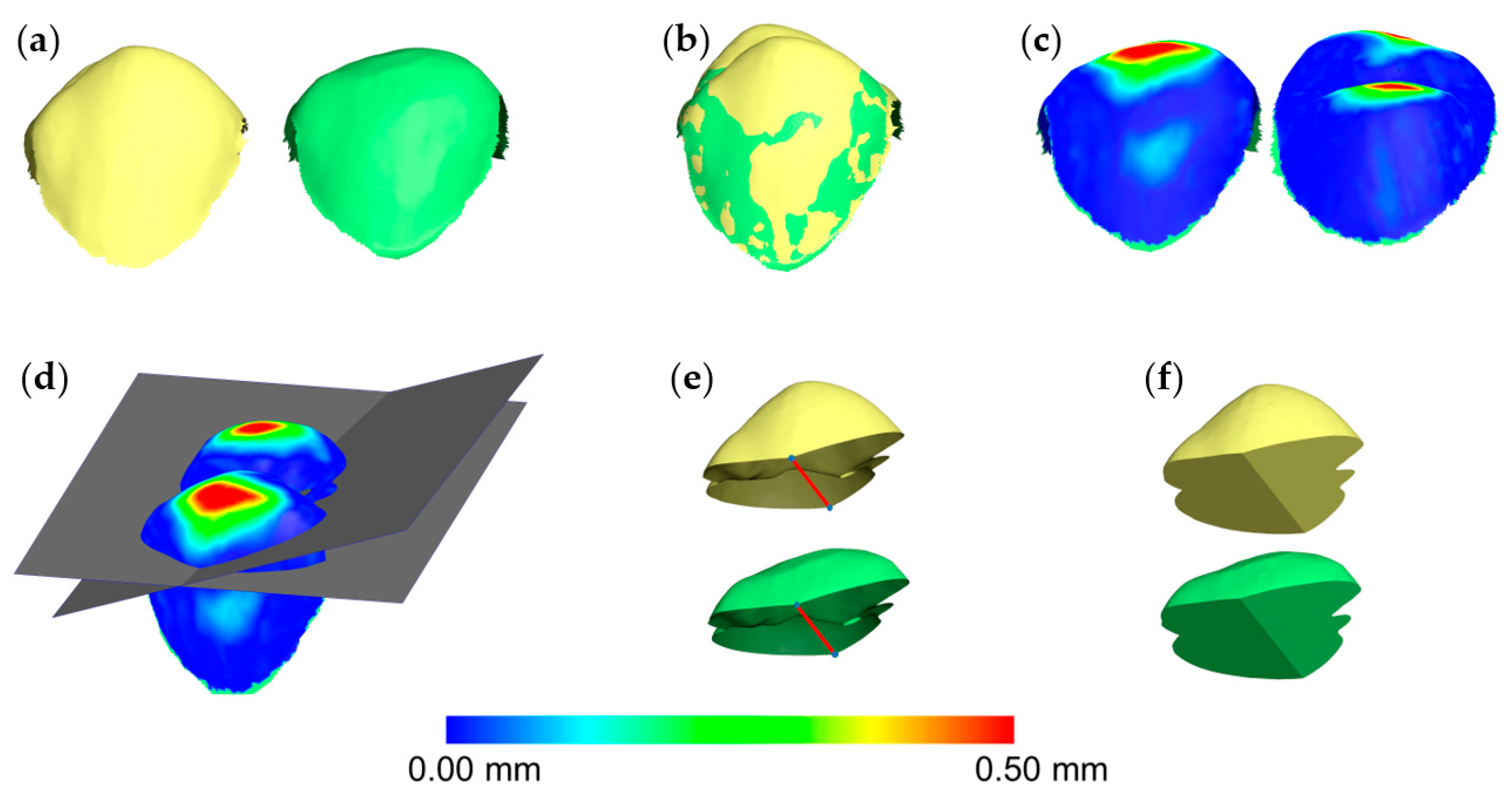
2.4. Tooth Wear Measurement
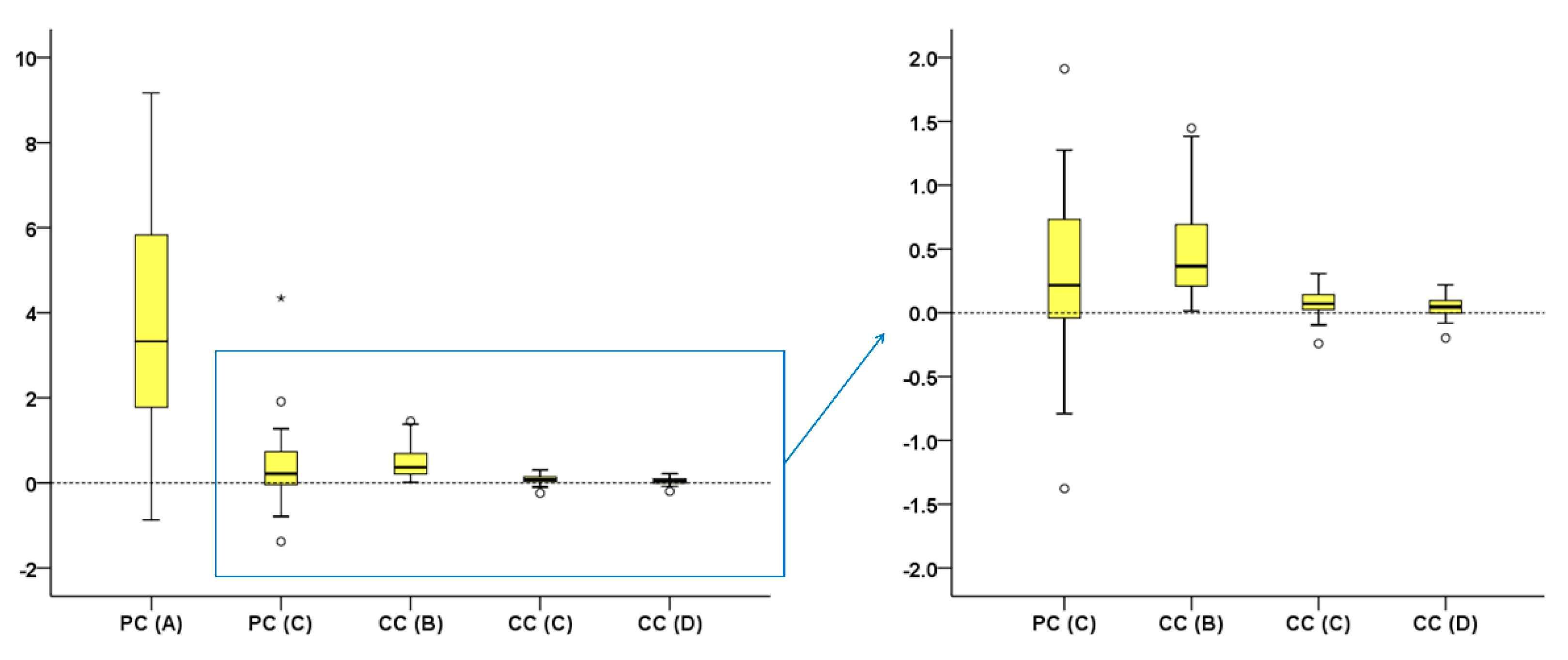
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lussi, A.; Carvalho, T.S. Erosive tooth wear: A multifactorial condition of growing concern and increasing knowledge. Monogr. Oral Sci. 2014, 25, 1–15. [Google Scholar]
- Loomans, B.; Opdam, N.; Attin, T.; Bartlett, D.; Edelhoff, D.; Frankenberger, R.; Benic, G.; Ramseyer, S.; Wetselaar, P.; Sterenborg, B.; et al. Severe tooth wear: European consensus statement on management guidelines. J. Adhes. Dent. 2017, 19, 111–119. [Google Scholar]
- Stober, T.; Bermejo, J.L.; Schwindling, F.S.; Schmitter, M. Clinical assessment of enamel wear caused by monolithic zirconia crowns. J. Oral Rehabil. 2016, 43, 621–629. [Google Scholar] [CrossRef]
- Lee, A.; He, L.H.; Lyons, K.; Swain, M.V. Tooth wear and wear investigations in dentistry. J. Oral Rehabil. 2012, 39, 217–225. [Google Scholar] [CrossRef]
- Wetselaar, P.; Faris, A.; Lobbezoo, F. A plea for the development of an universally accepted modular tooth wear evaluation system. BMC Oral Health 2016, 16, 115. [Google Scholar] [CrossRef] [PubMed]
- Al-Omiri, M.K.; Sghaireen, M.G.; Alzarea, B.K.; Lynch, E. Quantification of incisal tooth wear in upper anterior teeth: Conventional vs. new method using toolmakers microscope and a three-dimensional measuring technique. J. Dent. 2013, 41, 1214–1221. [Google Scholar] [CrossRef] [PubMed]
- Wulfman, C.; Koenig, V.; Mainjot, A.K. Wear measurement of dental tissues and materials in clinical studies: A systematic review. Dent. Mater. 2018, 34, 825–850. [Google Scholar] [CrossRef]
- Heintze, S.D. How to qualify and validate wear simulation devices and methods. Dent. Mater. 2006, 22, 712–734. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.M.; Bartlett, D.W. The dimensional stability of impression materials and its effect on in vitro tooth wear studies. Dent. Mater. 2011, 27, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Dritsas, K.; Ren, Y.; Halazonetis, D.; Katsaros, C. An accurate and efficient method for occlusal tooth wear assessment using 3D digital dental models. Sci. Rep. 2020, 10, 10103. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Dritsas, K.; Katsaros, C.; Halazonetis, D.; Ren, Y. 3D method for occlusal tooth wear assessment in presence of substantial changes on other tooth surfaces. J. Clin. Med. 2020, 9, 3937. [Google Scholar] [CrossRef] [PubMed]
- Stucki, S.; Gkantidis, N. Assessment of techniques used for superimposition of maxillary and mandibular 3D surface models to evaluate tooth movement: A systematic review. Eur. J. Orthod. 2020, 42, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Winkler, J.; Gkantidis, N. Trueness and precision of intraoral scanners in the maxillary dental arch: An in vivo analysis. Sci. Rep. 2020, 10, 1172. [Google Scholar] [CrossRef]
- Bartlett, D.W.; Lussi, A.; West, N.X.; Bouchard, P.; Sanz, M.; Bourgeois, D. Prevalence of tooth wear on buccal and lingual surfaces and possible risk factors in young European adults. J. Dent. 2013, 41, 1007–1013. [Google Scholar] [CrossRef]
- Gkantidis, N.; Christou, P.; Topouzelis, N. The orthodontic-periodontic interrelationship in integrated treatment challenges: A systematic review. J. Oral Rehabil. 2010, 37, 377–390. [Google Scholar] [CrossRef]
- Iliadi, A.; Kloukos, D.; Gkantidis, N.; Katsaros, C.; Pandis, N. Failure of fixed orthodontic retainers: A systematic review. J. Dent. 2015, 43, 876–896. [Google Scholar] [CrossRef]
- Henninger, E.; Vasilakos, G.; Halazonetis, D.; Gkantidis, N. The effect of regular dental cast artifacts on the 3D superimposition of serial digital maxillary dental models. Sci. Rep. 2019, 9, 10501. [Google Scholar] [CrossRef] [PubMed]
- Besl, P.J.; Mckay, N.D. A method for registration of 3-D shapes. IEEE Trans. Pattern Anal. Mach. Intell. 1992, 14, 239–256. [Google Scholar] [CrossRef]
- Marro, M.L.; Aranguiz, V.; Ramirez, V.; Lussi, A. Prevalence of erosive tooth wear in chilean adults, 2016: A cross-sectional study. J. Oral Rehabil. 2020, 47, 467–472. [Google Scholar] [CrossRef]
- Schierz, O.; Dommel, S.; Hirsch, C.; Reissmann, D.R. Occlusal tooth wear in the general population of germany: Effects of age, sex, and location of teeth. J. Prosthet. Dent. 2014, 112, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Awad, M.A.; El Kassas, D.; Al Harthi, L.; Abraham, S.B.; Al-Khalifa, K.S.; Khalaf, M.E.; Al Habashneh, R.; Bartlett, D. Prevalence, severity and explanatory factors of tooth wear in Arab populations. J. Dent. 2019, 80, 69–74. [Google Scholar] [CrossRef]
- Ahmed, K.E.; Whitters, J.; Ju, X.; Pierce, S.G.; MacLeod, C.N.; Murray, C.A. A proposed methodology to assess the accuracy of 3d scanners and casts and monitor tooth wear progression in patients. Int. J. Prosthodont. 2016, 29, 514–521. [Google Scholar] [CrossRef]
- Li, H.; Lyu, P.; Wang, Y.; Sun, Y. Influence of object translucency on the scanning accuracy of a powder-free intraoral scanner: A laboratory study. J. Prosthet. Dent. 2017, 117, 93–101. [Google Scholar] [CrossRef]
- Lim, J.H.; Mangal, U.; Nam, N.E.; Choi, S.H.; Shim, J.S.; Kim, J.E. A comparison of accuracy of different dental restorative materials between intraoral scanning and conventional impression-taking: An in vitro Study. Materials 2021, 14, 2060. [Google Scholar] [CrossRef]
- González de Villaumbrosia, P.; Martínez-Rus, F.; García-Orejas, A.; Salido, M.P.; Pradíes, G. In vitro comparison of the accuracy (trueness and precision) of six extraoral dental scanners with different scanning technologies. J. Prosthet. Dent. 2016, 116, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Vasilakos, G.; Schilling, R.; Halazonetis, D.; Gkantidis, N. Assessment of different techniques for 3D superimposition of serial digital maxillary dental casts on palatal structures. Sci. Rep. 2017, 7, 5838. [Google Scholar] [CrossRef]
- Friedli, L.; Kloukos, D.; Kanavakis, G.; Halazonetis, D.; Gkantidis, N. The effect of threshold level on bone segmentation of cranial base structures from CT and CBCT images. Sci. Rep. 2020, 10, 7361. [Google Scholar] [CrossRef] [PubMed]
- Häner, S.T.; Kanavakis, G.; Matthey, F.; Gkantidis, N. Voxel-based superimposition of serial craniofacial CBCTs: Reliability, reproducibility and segmentation effect on hard-tissue outcomes. Orthod. Craniofac. Res. 2020, 23, 92–101. [Google Scholar] [CrossRef]
- Ray, D.S.; Wiemann, A.H.; Patel, P.B.; Ding, X.; Kryscio, R.J.; Miller, C.S. Estimation of the rate of tooth wear in permanent incisors: A cross-sectional digital radiographic study. J. Oral Rehabil. 2015, 42, 460–466. [Google Scholar] [CrossRef]
- O’Toole, S.; Lau, J.S.; Rees, M.; Warburton, F.; Loomans, B.; Bartlett, D. Quantitative tooth wear analysis of index teeth compared to complete dentition. J. Dent. 2020, 97, 103342. [Google Scholar] [CrossRef]
- Park, J.; Choi, D.S.; Jang, I.; Yook, H.T.; Jost-Brinkmann, P.G.; Cha, B.K. A novel method for volumetric assessment of tooth wear using three-dimensional reverse-engineering technology: A preliminary report. Angle Orthod. 2014, 84, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.P.; Nam, S.E.; Lee, Y.M.; Park, Y.S.; Hayashi, K.; Lee, J.B. The development of quantitative methods using virtual models for the measurement of tooth wear. Clin. Anat. 2012, 25, 347–358. [Google Scholar] [CrossRef]
- Stober, T.; Heuschmid, N.; Zellweger, G.; Rousson, V.; Rues, S.; Heintze, S.D. Comparability of clinical wear measurements by optical 3D laser scanning in two different centers. Dent. Mater. 2014, 30, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.E.; Whitters, J.; Ju, X.; Pierce, S.G.; MacLeod, C.N.; Murray, C.A. Clinical monitoring of tooth wear progression in patients over a period of one year using CAD/CAM. Int. J. Prosthodont. 2017, 30, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Comparing methods of measurement: Why plotting difference against standard method is misleading. Lancet 1995, 346, 1085–1087. [Google Scholar] [CrossRef]
- O’Toole, S.; Osnes, C.; Bartlett, D.; Keeling, A. Investigation into the validity of WearCompare, a purpose-built software to quantify erosive tooth wear progression. Dent. Mater. 2019, 35, 1408–1414. [Google Scholar] [CrossRef]
- Marro, F.; Jacquet, W.; Martens, L.; Keeling, A.; Bartlett, D.; O’Toole, S. Quantifying increased rates of erosive tooth wear progression in the early permanent dentition. J. Dent. 2020, 93, 103282. [Google Scholar] [CrossRef] [PubMed]
- Perry, R.; Kugel, G.; Kunzelmann, K.H.; Flessa, H.P.; Estafan, D. Composite restoration wear analysis: Conventional methods vs. three-dimensional laser digitizer. J. Am. Dent. Assoc. 2000, 131, 1472–1477. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technique | Reference Area | Estimated Overlap |
|---|---|---|
| GS | Adjacent intact teeth and alveolar processes | 100% |
| PC(A) | Buccolingual surfaces | 100% |
| PC(C) | Buccolingual surfaces | User defined |
| CC(B) | Complete crown | 80% |
| CC(C) | Complete crown | User defined |
| CC(D) | Complete crown | 30% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkantidis, N.; Dritsas, K.; Katsaros, C.; Halazonetis, D.; Ren, Y. 3D Occlusal Tooth Wear Assessment in Presence of Limited Changes in Non-Occlusal Surfaces. Diagnostics 2021, 11, 1033. https://doi.org/10.3390/diagnostics11061033
Gkantidis N, Dritsas K, Katsaros C, Halazonetis D, Ren Y. 3D Occlusal Tooth Wear Assessment in Presence of Limited Changes in Non-Occlusal Surfaces. Diagnostics. 2021; 11(6):1033. https://doi.org/10.3390/diagnostics11061033
Chicago/Turabian StyleGkantidis, Nikolaos, Konstantinos Dritsas, Christos Katsaros, Demetrios Halazonetis, and Yijin Ren. 2021. "3D Occlusal Tooth Wear Assessment in Presence of Limited Changes in Non-Occlusal Surfaces" Diagnostics 11, no. 6: 1033. https://doi.org/10.3390/diagnostics11061033
APA StyleGkantidis, N., Dritsas, K., Katsaros, C., Halazonetis, D., & Ren, Y. (2021). 3D Occlusal Tooth Wear Assessment in Presence of Limited Changes in Non-Occlusal Surfaces. Diagnostics, 11(6), 1033. https://doi.org/10.3390/diagnostics11061033