
Machine-Learning-Based Rehabilitation Prognosis Prediction in Patients with Ischemic Stroke Using Brainstem Auditory Evoked Potential


Abstract
1. Introduction
2. Materials and Methods
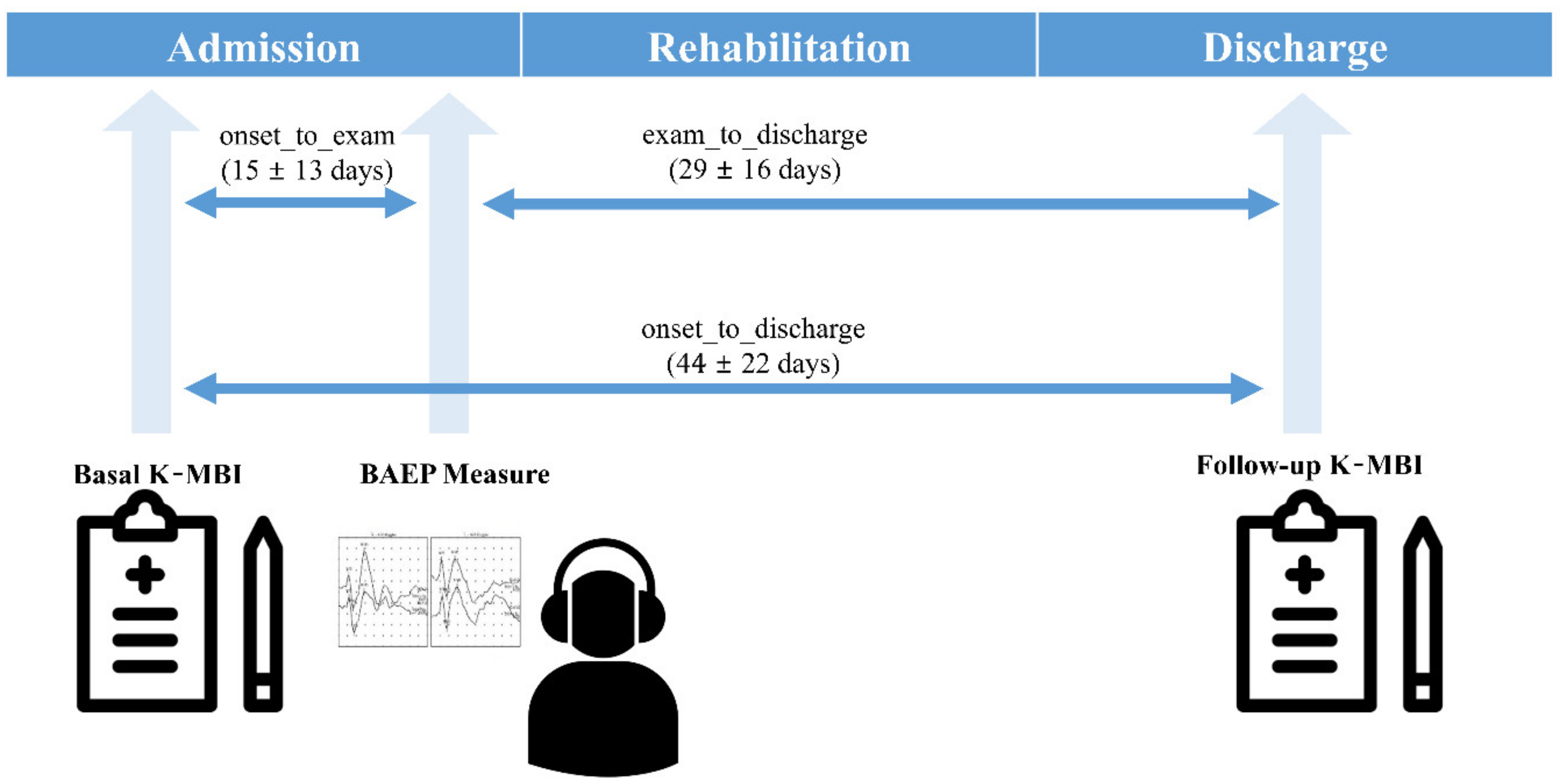
2.1. Subjects and Study Protocol
2.2. BAEP Measurement
2.3. K-MBI
2.4. Data Analysis
3. Results
3.1. Effects of Confounding Factors on BAEP IPLs
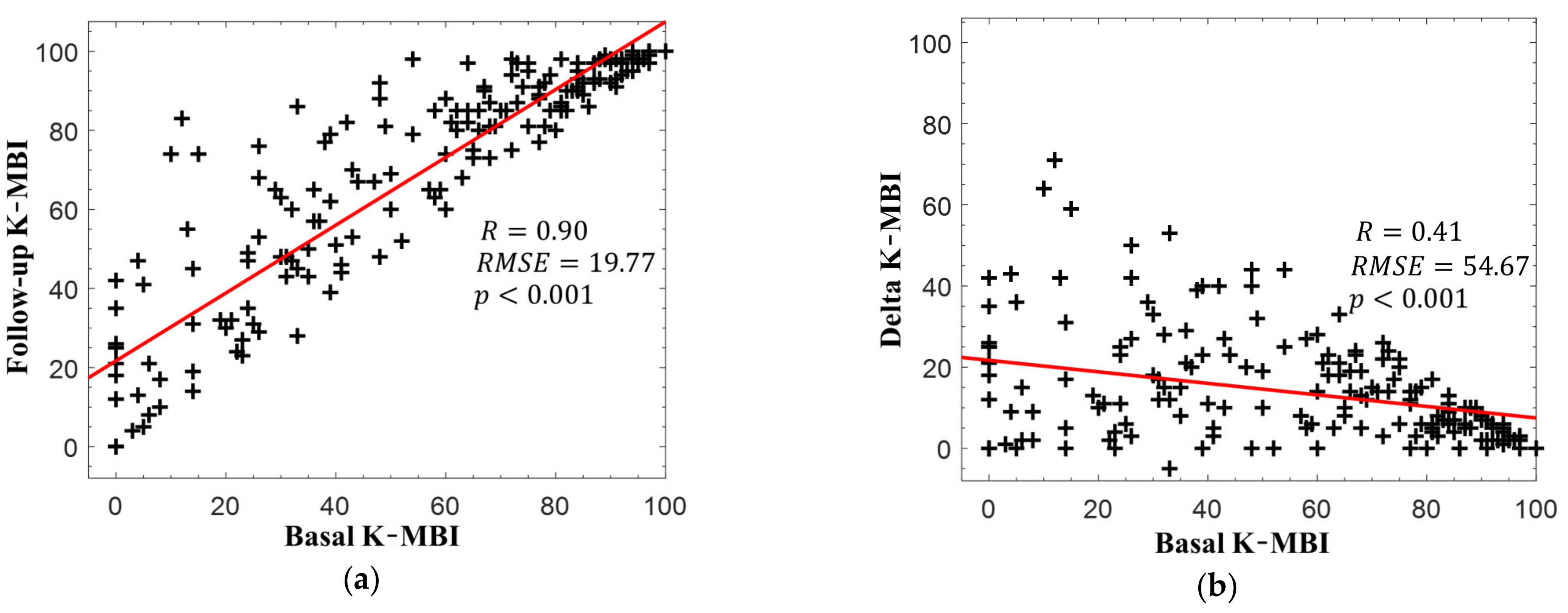
3.2. Changes in K-MBI Scores
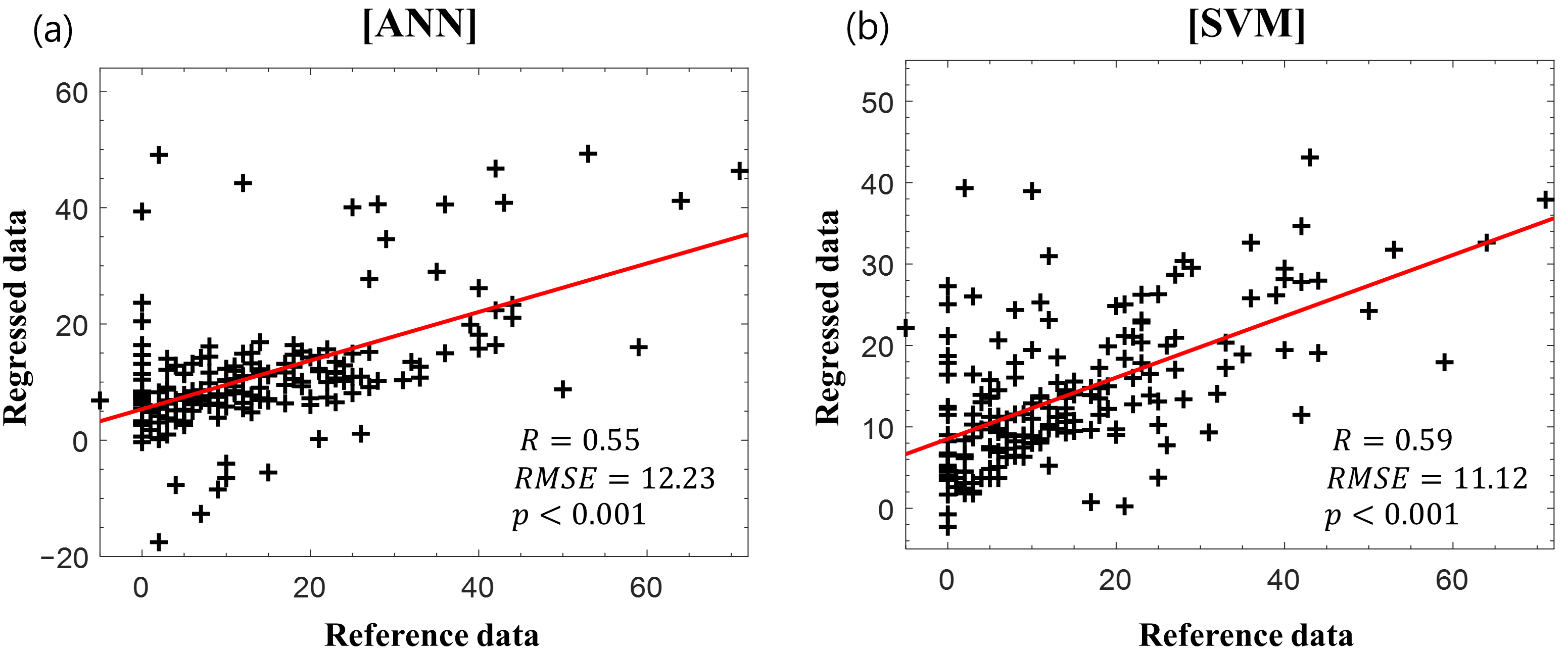
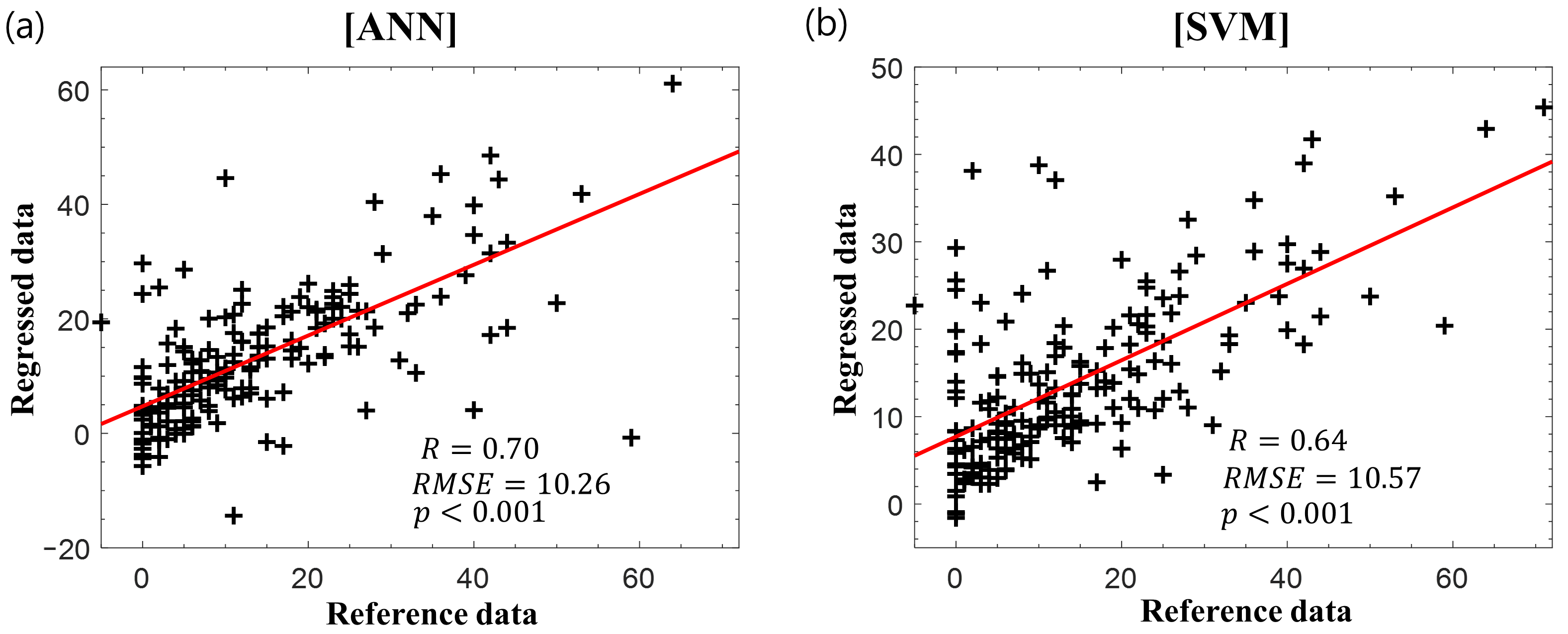
3.3. Regression and Feature Importance Analysis Subsection
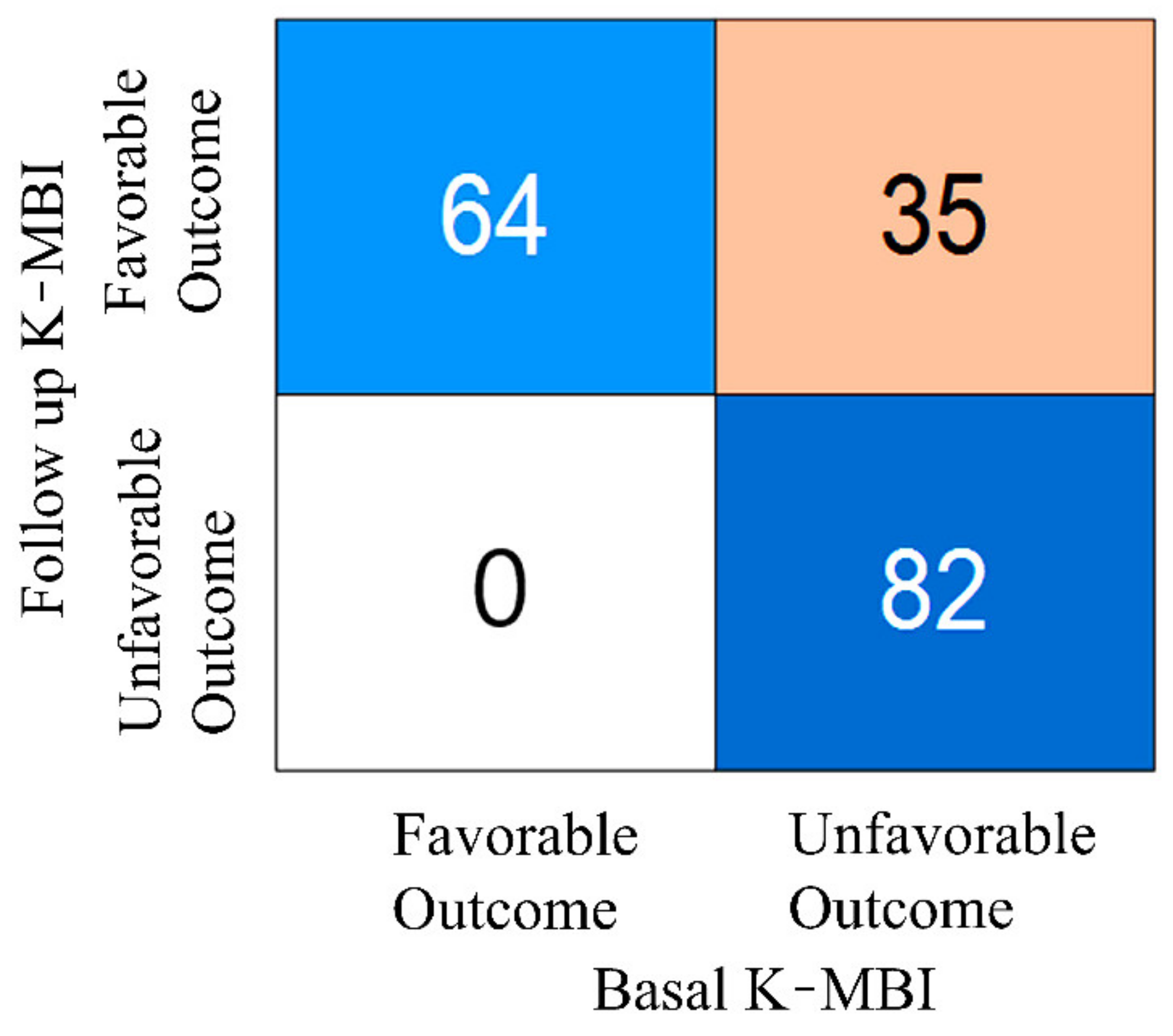
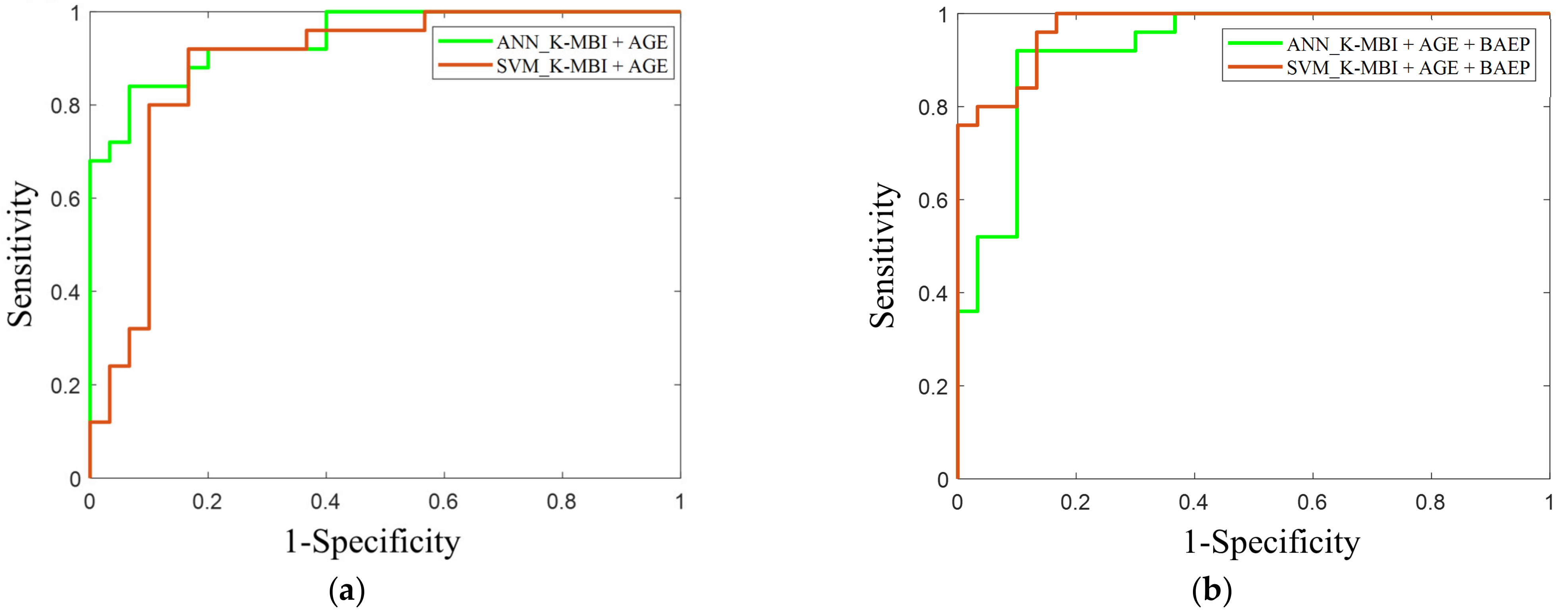
3.4. Prognosis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heinz, U.E.; Rollnik, J.D. Outcome and prognosis of hypoxic brain damage patients undergoing neurological early rehabilitation. BMC Res. Notes 2015, 8, 243. [Google Scholar] [CrossRef]
- Konig, I.R.; Ziegler, A.; Bluhmki, E.; Hacke, W.; Bath, P.M.; Sacco, R.L.; Diener, H.C.; Weimar, C.; Virtual International Stroke Trials Archive. Predicting long-term outcome after acute ischemic stroke: A simple index works in patients from controlled clinical trials. Stroke 2008, 39, 1821–1826. [Google Scholar] [CrossRef]
- Su, Y.Y.; Xiao, S.Y.; Haupt, W.F.; Zhang, Y.; Zhao, H.; Pang, Y.; Wang, L.; Ding, J.P.; Zhao, J.W. Parameters and grading of evoked potentials: Prediction of unfavorable outcome in patients with severe stroke. J. Clin. Neurophysiol. 2010, 27, 25–29. [Google Scholar] [CrossRef]
- Daroff, R.B.; Aminoff, M.J. Encyclopedia of the Neurological Sciences; Academic Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Holdefer, R.N.; MacDonald, D.B.; Skinner, S.A. Somatosensory and motor evoked potentials as biomarkers for post-operative neurological status. Clin. Neurophysiol. 2015, 126, 857–865. [Google Scholar] [CrossRef]
- Cantone, M.; Lanza, G.; Le Pira, A.; Barone, R.; Pennisi, G.; Bella, R.; Pennisi, M.; Fiumara, A. Adjunct Diagnostic Value of Transcranial Magnetic Stimulation in Mucopolysaccharidosis-Related Cervical Myelopathy: A Pilot Study. Brain Sci. 2019, 9, 200. [Google Scholar] [CrossRef]
- Calugaru, L.; Calugaru, G.T.; Calugaru, O.M. Somatosensory Evoked Potentials in Predicting Motor Deficit after Ischemic or Hemorrhagic Stroke. Curr. Health Sci. J. 2015, 41, 42–46. [Google Scholar] [CrossRef]
- Tzvetanov, P.; Rousseff, R.T. Median SSEP changes in hemiplegic stroke: Long-term predictive values regarding ADL recovery. NeuroRehabilitation 2003, 18, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Tzvetanov, P.; Rousseff, R.T.; Milanov, I. Lower limb SSEP changes in stroke-predictive values regarding functional recovery. Clin. Neurol. Neurosurg. 2003, 105, 121–127. [Google Scholar] [CrossRef]
- Steube, D.; Wietholter, S.; Correll, C. Prognostic value of lower limb motor evoked potentials for motor impairment and disability after 8 weeks of stroke rehabilitation—A prospective investigation of 100 patients. Electromyogr. Clin. Neurophysiol. 2001, 41, 463–469. [Google Scholar] [PubMed]
- Fisicaro, F.; Lanza, G.; Grasso, A.A.; Pennisi, G.; Bella, R.; Paulus, W.; Pennisi, M. Repetitive transcranial magnetic stimulation in stroke rehabilitation: Review of the current evidence and pitfalls. Adv. Neurol. Disord. 2019, 12, 1756286419878317. [Google Scholar] [CrossRef] [PubMed]
- Rollnik, J.D. May clinical neurophysiology help to predict the recovery of neurological early rehabilitation patients? BMC Neurol. 2015, 15, 239. [Google Scholar] [CrossRef]
- Kim, Y.-W.; Sohn, M.K.; Jung, I.-Y. Relationship between Brainstem Auditory Evoked Potentials and Clinical Function in Patients with Cerebral Infarction. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2020. [Google Scholar] [CrossRef]
- Hairston, W.D.; Letowski, T.R.; McDowell, K. Task-related suppression of the brainstem frequency following response. PLoS ONE 2013, 8, e55215. [Google Scholar] [CrossRef] [PubMed]
- Saiz-Alia, M.; Forte, A.E.; Reichenbach, T. Individual differences in the attentional modulation of the human auditory brainstem response to speech inform on speech-in-noise deficits. Sci. Rep. 2019, 9, 14131. [Google Scholar] [CrossRef] [PubMed]
- Scrutinio, D.; Ricciardi, C.; Donisi, L.; Losavio, E.; Battista, P.; Guida, P.; Cesarelli, M.; Pagano, G.; D’Addio, G. Machine learning to predict mortality after rehabilitation among patients with severe stroke. Sci. Rep. 2020, 10, 1–10. [Google Scholar]
- Kourou, K.; Exarchos, T.P.; Exarchos, K.P.; Karamouzis, M.V.; Fotiadis, D.I. Machine learning applications in cancer prognosis and prediction. Comput. Struct. Biotechnol. J. 2015, 13, 8–17. [Google Scholar] [CrossRef]
- Hong, I.; Woo, H.S.; Shim, S.; Li, C.Y.; Yoonjeong, L.; Velozo, C.A. Equating activities of daily living outcome measures: The Functional Independence Measure and the Korean version of Modified Barthel Index. Disabil. Rehabil. 2018, 40, 217–224. [Google Scholar] [CrossRef]
- Hong, I.; Lim, Y.; Han, H.; Hay, C.C.; Woo, H.S. Application of the Korean Version of the Modified Barthel Index: Development of a keyform for use in Clinical Practice. Hong Kong J. Occup. Ther. 2017, 29, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Baker, W.L.; Colby, J.A.; Tongbram, V.; Talati, R.; Silverman, I.E.; White, C.M.; Kluger, J.; Coleman, C.I. Neurothrombectomy devices for the treatment of acute ischemic stroke: State of the evidence. Ann. Intern. Med. 2011, 154, 243–252. [Google Scholar] [CrossRef]
- Konrad-Martin, D.; Dille, M.F.; McMillan, G.; Griest, S.; McDermott, D.; Fausti, S.A.; Austin, D.F. Age-related changes in the auditory brainstem response. J. Am. Acad. Audiol. 2012, 23, 18–35. [Google Scholar] [CrossRef]
- Hall, J.W. New Handbook of Auditory Evoked Responses; Pearson: London, UK, 2007. [Google Scholar]
- Neu, M.; Strauss, C.; Romstock, J.; Bischoff, B.; Fahlbusch, R. The prognostic value of intraoperative BAEP patterns in acoustic neurinoma surgery. Clin. Neurophysiol. 1999, 110, 1935–1941. [Google Scholar] [CrossRef]
- Schick, U.; Dohnert, J.; Meyer, J.J.; Vitzthum, H.E. Prognostic significance of SSEP, BAEP and serum S-100B monitoring after aneurysm surgery. Acta Neurol. Scand. 2003, 108, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Mackey-Hargadine, J.R.; Hall, J.W., 3rd. Sensory evoked responses in head injury. Cent. Nerv. Syst. Trauma 1985, 2, 187–206. [Google Scholar] [CrossRef] [PubMed]
- Wachter, D.; Christophis, P.; Stein, M.; Oertel, M. Use of multimodal electrophysiological monitoring to predict outcome after subarachnoid hemorrhage? A prospective series. J. Neurosurg. Sci. 2011, 55, 179–187. [Google Scholar] [PubMed]
- Jung, H.Y.; Park, B.K.; Shin, H.S.; Kang, Y.K.; Pyun, S.B.; Paik, N.J.; Kim, S.H.; Kim, T.H.; Han, T.R. Development of the Korean Version of Modified Barthel Index (K-MBI): Multi-center Study for Subjects with Stroke. J. Korean Acad. Rehabil. Med. 2007, 31, 283–297. [Google Scholar]
- Pasini, A. Artificial neural networks for small dataset analysis. J. Thorac. Dis 2015, 7, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Jiang, X. Overcome support vector machine diagnosis overfitting. Cancer Inf. 2014, 13, 145–158. [Google Scholar] [CrossRef]
- Bishop, C.M. Pattern Recognition and Machine Learning; Springer: Cham, Switzerland, 2006. [Google Scholar]
- Dobrowolski, A.; Suchocki, M.; Tomczykiewicz, K.; Majda-Zdancewicz, E. Classification of auditory brainstem response using wavelet decomposition and SVM network. Biocybern. Biomed. Eng. 2016, 36, 427–436. [Google Scholar] [CrossRef]
- Arulampalam, G.; Bouzerdoum, A. A generalized feedforward neural network architecture for classification and regression. Neural. Netw. 2003, 16, 561–568. [Google Scholar] [CrossRef]
- Nazzal, M.; Sa’Adah, M.; Al-Ansaris, D.; Al-Awadi, O.; Inshasi, J.; Eyadah, A.; Al-Kadiri, M.; Trebinjac, S.; Khader, S. Stroke rehabilitation: Application and analysis of the modified Barthel index in an Arab community. Disabil. Rehabil. 2001, 23, 36–42. [Google Scholar] [CrossRef]
- Burges, C.J. A tutorial on support vector machines for pattern recognition. Data Min. Knowl. Discov. 1998, 2, 121–167. [Google Scholar] [CrossRef]
- Haupt, W.F.; Pawlik, G.; Thiel, A. Initial and serial evoked potentials in cerebrovascular critical care patients. J. Clin. Neurophysiol. 2006, 23, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Beier, A.D.; Dirks, P.B. Pediatric brainstem hemorrhages after traumatic brain injury. J. Neurosurg. Pediatr. 2014, 14, 421–424. [Google Scholar] [CrossRef]
- Gilbert, C.D.; Sigman, M. Brain states: Top-down influences in sensory processing. Neuron 2007, 54, 677–696. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, T.; Weisz, N. Auditory cortical generators of the Frequency Following Response are modulated by intermodal attention. Neuroimage 2019, 203, 116185. [Google Scholar] [CrossRef]
- Heo, J.; Yoon, J.G.; Park, H.; Kim, Y.D.; Nam, H.S.; Heo, J.H. Machine Learning-Based Model for Prediction of Outcomes in Acute Stroke. Stroke 2019, 50, 1263–1265. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, B.R.; Han, E.Y. Association between evoked potentials and balance recovery in subacute hemiparetic stroke patients. Ann. Rehabil. Med. 2015, 39, 451. [Google Scholar] [CrossRef] [PubMed]
- Feys, H.; Van Hees, J.; Bruyninckx, F.; Mercelis, R.; De Weerdt, W. Value of somatosensory and motor evoked potentials in predicting arm recovery after a stroke. J. Neurol. Neurosurg. Psychiatry 2000, 68, 323–331. [Google Scholar] [CrossRef]
- Mazzini, L.; Pisano, F.; Zaccala, M.; Miscio, G.; Gareri, F.; Galante, M. Somatosensory and motor evoked potentials at different stages of recovery from severe traumatic brain injury. Arch. Phys. Med. Rehabil. 1999, 80, 33–39. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | |
|---|---|---|
| Participants, n | 181 | |
| Demographics | ||
| Sex, % males | 56.35 | |
| Age, years, mean ± SD (min/max) | 68.15 ± 11.68 (36/89) | |
| Stroke onset, n | ||
| First ever | 142 | |
| Recurrent | 39 | |
| Lesion side of cerebral infarction, n | ||
| Right | 83 | |
| Left | 98 | |
| Lesion location, n | ||
| Supratentorial | ||
| Cortex | 75 | |
| BG/IC | 41 | |
| Thalamus | 4 | |
| Corona radiata | 23 | |
| Infratentorial | ||
| Brainstem | 33 | |
| Cerebellum | 11 | |
| Both | 2 | |
| Duration, days | ||
| From onset to study, mean ± SD | 15.82 ± 13.16 | |
| From onset to discharge, mean ± SD | 44.04 ± 22.24 | |
| Clinical evaluation level, mean ± SD | At admission | At discharge |
| K-MBI | 53.08 ± 31.71 | 67.24 ± 30.19 |
| NIHSS | 5± 4.69 | 3.87± 4.28 |
| Partial Correlations | Stroke Onset | Lesion Location | Onset to Study | Onset to Discharge |
|---|---|---|---|---|
| Wave I | ||||
| r | −0.02 | 0.04 | 0.09 | 0.07 |
| p | 0.82 | 0.61 | 0.22 | 0.36 |
| Waves I–III | ||||
| r | −0.13 | 0.06 | −0.07 | -0.03 |
| p | 0.08 | 0.39 | 0.38 | 0.66 |
| Waves III–V | ||||
| r | 0.02 | 0.16 | 0.05 | 0.01 |
| p | 0.82 | 0.03 | 0.51 | 0.97 |
| Input Features | Wave I | Waves I–III | Waves III–V | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BAEP Latency (msec) | L.S (mean ± SD) | N.S (mean ± SD) | p-Value | L.S (mean ± SD) | N.S (mean ± SD) | p-Value | L.S (mean ± SD) | N.S (mean ± SD) | p-Value | |
| Total subjects | 1.83 ± 0.21 | 1.85 ± 0.22 | 0.37 | 2.24 ± 0.22 | 2.25 ± 0.25 | 0.73 | 3.83 ± 0.32 | 3.82 ± 0.29 | 0.47 | |
| Lesion location | Supratentorial | 1.83 ± 0.20 | 1.86 ± 0.23 | 0.25 | 2.24 ± 0.24 | 2.26 ± 0.26 | 0.25 | 3.81 ± 0.30 | 3.82 ± 0.30 | 0.83 |
| Infratentorial | 1.84 ± 0.23 | 1.83 ± 0.18 | 0.85 | 2.21 ± 0.16 | 2.19 ± 0.20 | 0.33 | 3.89 ± 0.39 | 3.83 ± 0.26 | 0.41 | |
| Feature Importance | KNN | Stepwise Regression | ||
|---|---|---|---|---|
| Feature Weight (Arbitrary Value) | Coefficients | t-Value | Sig. | |
| K-MBI (basal) | 6.48 | −6.45 | −6.32 | 2.16 × 10 −9 ** |
| Age | 2.28 | −4.17 | −4.06 | 7.35 × 10 −5 ** |
| Wave I | 2.54 | 0.21 | 0.18 | 0.86 |
| Waves I–III | 0.01 | 0.78 | 0.55 | 0.58 |
| Waves III–V | 2.64 | −2.96 | −2.27 | 0.02 * |
| Input Variables | Adjusted r-Square |
|---|---|
| K-MBI (basal) | 0.20 |
| K-MBI (basal) + Age | 0.32 |
| K-MBI (basal) + Age + Waves III–V | 0.48 |
| K-MBI (basal) + Age + Waves I–III + Waves III–V | 0.44 |
| K-MBI (basal) + Age + Wave I + Waves I–III + Waves III–V | 0.40 |
| Input Features | Model | Accuracy | Sensitivity | Specificity | AUC |
|---|---|---|---|---|---|
| K-MBI (basal) + Age | ANN | 85% (0.76 to 0.94) | 84% (0.74 to 0.94) | 86% (0.77 to 0.95) | 0.90 (0.82 to 0.97) |
| SVM | 87% (0.78 to 0.96) | 84% (0.74 to 0.94) | 90% (0.82 to 0.97) | 0.87 (0.78 to 0.96) | |
| K-MBI (basal) + Age + IPLs (I, I–III, and III–V) | ANN | 91% (0.83 to 0.99) | 92% (0.84 to 0.99) | 90% (0.82 to 0.97) | 0.90 (0.82 to 0.97) |
| SVM | 84% (0.74 to 0.94) | 88% (0.79 to 0.96) | 86% (0.77 to 0.95) | 0.93 (0.86 to 0.99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sohn, J.; Jung, I.-Y.; Ku, Y.; Kim, Y. Machine-Learning-Based Rehabilitation Prognosis Prediction in Patients with Ischemic Stroke Using Brainstem Auditory Evoked Potential. Diagnostics 2021, 11, 673. https://doi.org/10.3390/diagnostics11040673
Sohn J, Jung I-Y, Ku Y, Kim Y. Machine-Learning-Based Rehabilitation Prognosis Prediction in Patients with Ischemic Stroke Using Brainstem Auditory Evoked Potential. Diagnostics. 2021; 11(4):673. https://doi.org/10.3390/diagnostics11040673
Chicago/Turabian StyleSohn, Jangjay, Il-Young Jung, Yunseo Ku, and Yeongwook Kim. 2021. "Machine-Learning-Based Rehabilitation Prognosis Prediction in Patients with Ischemic Stroke Using Brainstem Auditory Evoked Potential" Diagnostics 11, no. 4: 673. https://doi.org/10.3390/diagnostics11040673
APA StyleSohn, J., Jung, I.-Y., Ku, Y., & Kim, Y. (2021). Machine-Learning-Based Rehabilitation Prognosis Prediction in Patients with Ischemic Stroke Using Brainstem Auditory Evoked Potential. Diagnostics, 11(4), 673. https://doi.org/10.3390/diagnostics11040673