
Endoscopic Ultrasound-Guided Sampling for Personalized Pancreatic Cancer Treatment

 , and
, and
Abstract

1. Introduction
2. Personalized Cancer Treatment Using Genomic Profiling
2.1. The Current Status of Cancer Precision Medicine
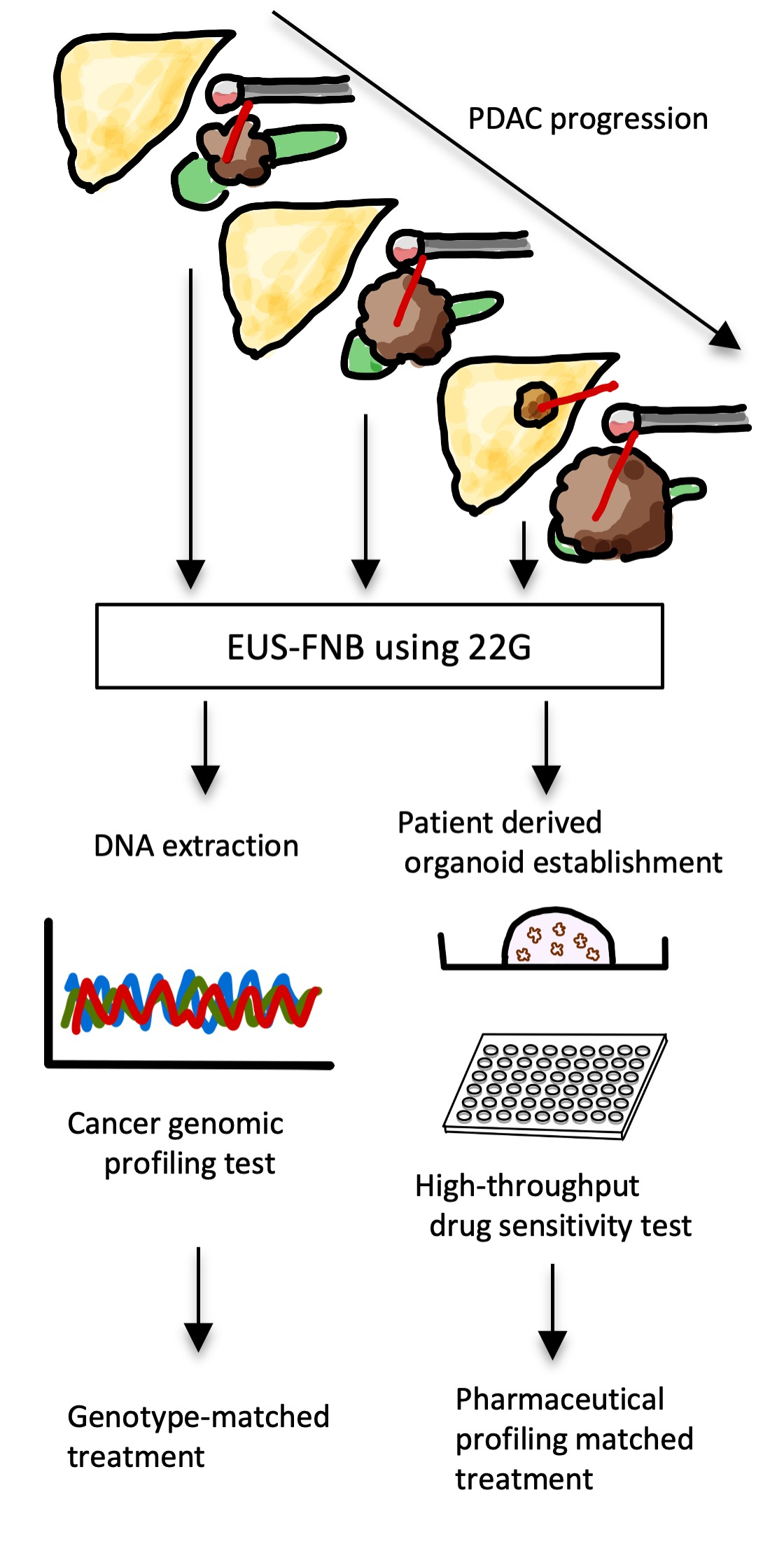
2.2. Using EUS-Guided Sampling to Improve Personalized Treatment for PDAC
2.3. Cancer Genomic Medicine for PDAC: A Future Perspective
3. Personalized Cancer Treatment Using Pharmacological Profiling
3.1. Effectiveness and Role of Chemosensitivity Tests for PDAC Treatment
3.2. Patient-Derived Tumor Organoids for PDAC: A Future Perspective
3.3. EUS-Guided Sampling for Personalized Medicine Using PDOs
3.4. Human PDOs Establishment from EUS-Guided Sampling
3.5. High Throughput Drug Screening Test Using PDOs
3.6. Drug Screening Test for PDAC Using Organoids
4. Additional Diagnostic Methods for PDACs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Vincent, A.; Herman, J.; Schulick, R.; Hruban, R.H.; Goggins, M. Pancreatic cancer. Lancet 2011, 378, 607–620. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Pishvaian, M.J.; Blais, E.M.; Brody, J.R.; Lyons, E.; DeArbeloa, P.; Hendifar, A.; Mikhail, S.; Chung, V.; Sahai, V.; Sohal, D.P.S.; et al. Overall survival in patients with pancreatic cancer receiving matched therapies following molecular profiling: A retrospective analysis of the Know Your Tumor registry trial. Lancet Oncol. 2020, 21, 508–518. [Google Scholar] [CrossRef]
- Li, D.F.; Wang, J.Y.; Yang, M.F.; Xiong, F.; Zhang, D.G.; Xu, Z.L.; Luo, M.H.; Jing, Z.D.; Wang, K.X.; Wang, L.S.; et al. Factors associated with diagnostic accuracy, technical success and adverse events of endoscopic ultrasound-guided fine-needle biopsy: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2020, 35, 1264–1276. [Google Scholar] [CrossRef] [PubMed]
- Kandel, P.; Nassar, A.; Gomez, V.; Raimondo, M.; Woodward, T.A.; Crook, J.E.; Fares, N.S.; Wallace, M.B. Comparison of endoscopic ultrasound-guided fine-needle biopsy versus fine-needle aspiration for genomic profiling and DNA yield in pancreatic cancer: A randomized crossover trial. Endoscopy 2020. online ahead of print. [Google Scholar] [CrossRef]
- Berry, W.; Lundy, J.; Croagh, D.; Jenkins, B.J. Reviewing the utility of EUS FNA to advance precision medicine in pancreatic cancer. Cancers 2018, 10, 35. [Google Scholar] [CrossRef]
- Tiriac, H.; Bucobo, J.C.; Tzimas, D.; Grewel, S.; Lacomb, J.F.; Rowehl, L.M.; Nagula, S.; Wu, M.; Kim, J.; Sasson, A.; et al. Successful creation of pancreatic cancer organoids by means of EUS-guided fine-needle biopsy sampling for personalized cancer treatment. Gastrointest. Endosc. 2018, 87, 1474–1480. [Google Scholar] [CrossRef] [PubMed]
- Cloyd, J.M.; Heh, V.; Pawlik, T.M.; Ejaz, A.; Dillhoff, M.; Tsung, A.; Williams, T.; Abushahin, L.; Bridges, J.F.P.; Santry, H. Neoadjuvant therapy for resectable and borderline resectable pancreatic cancer: A meta-analysis of randomized controlled trials. J. Clin. Med. 2020, 9, 1129. [Google Scholar] [CrossRef] [PubMed]
- Larson, B.K.; Tuli, R.; Jamil, L.H.; Lo, S.K.; Deng, N.; Hendifar, A.E. Utility of endoscopic ultrasound-guided biopsy for next-generation sequencing of pancreatic exocrine malignancies. Pancreas 2018, 47, 990–995. [Google Scholar] [CrossRef]
- Bournet, B.; Pointreau, A.; Souque, A.; Oumouhou, N.; Muscari, F.; Lepage, B.; Senesse, P.; Barthet, M.; Lesavre, N.; Hammel, P.; et al. Gene expression signature of advanced pancreatic ductal adenocarcinoma using low density array on endoscopic ultrasound-guided fine needle aspiration samples. Pancreatology 2012, 12, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Kapałczyńska, M.; Kolenda, T.; Przybyła, W.; Zajączkowska, M.; Teresiak, A.; Filas, V.; Ibbs, M.; Bliźniak, R.; Łuczewski, Ł.; Lamperska, K. 2D and 3D cell cultures—A comparison of different. Arch. Med. Sci. 2016, 14, 910–919. [Google Scholar]
- Hyman, D.M.; Taylor, B.S.; Baselga, J. Implementing genome-driven oncology. Cell 2017, 168, 584–599. [Google Scholar] [CrossRef] [PubMed]
- Schütte, M.; Risch, T.; Abdavi-Azar, N.; Boehnke, K.; Schumacher, D.; Keil, M.; Yildiriman, R.; Jandrasits, C.; Borodina, T.; Amstislavskiy, V.; et al. Molecular dissection of colorectal cancer in pre-clinical models identifies biomarkers predicting sensitivity to EGFR inhibitors. Nat. Commun. 2017, 8, 14262. [Google Scholar] [CrossRef]
- Phan, N.; Hong, J.J.; Tofig, B.; Mapua, M.; Elashoff, D.; Moatamed, N.A.; Huang, J.; Memarzadeh, S.; Damoiseaux, R.; Soragni, A. A simple high-throughput approach identifies actionable drug sensitivities in patient-derived tumor organoids. Commun. Biol. 2019, 2, 1–11. [Google Scholar] [CrossRef]
- Vlachogiannis, G.; Hedayat, S.; Vatsiou, A.; Jamin, Y.; Fernández-Mateos, J.; Khan, K.; Lampis, A.; Eason, K.; Huntingford, I.; Burke, R.; et al. Patient-derived organoids model treatment response of metastatic gastrointestinal cancers. Science 2018, 359, 920–926. [Google Scholar] [CrossRef]
- Biankin, A.V.; Piantadosi, S.; Hollingsworth, S.J. Patient-centric trials for therapeutic development in precision oncology. Nature 2015, 526, 361–370. [Google Scholar] [CrossRef]
- Renfro, L.A.; Sargent, D.J. Statistical controversies in clinical research: Basket trials, umbrella trials, and other master protocols: A review and examples. Ann. Oncol. 2017, 28, 34–43. [Google Scholar] [CrossRef]
- Redig, A.J.; Jänne, P.A. Basket trials and the evolution of clinical trial design in an era of genomic medicine. J. Clin. Oncol. 2015, 33, 975–977. [Google Scholar] [CrossRef] [PubMed]
- Cunanan, K.M.; Gonen, M.; Shen, R.; Hyman, D.M.; Riely, G.J.; Begg, C.B.; Iasonos, A. Basket trials in oncology: A trade-off between complexity and efficiency. J. Clin. Oncol. 2017, 35, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Kopetz, S.; Grothey, A.; Yaeger, R.; Van Cutsem, E.; Desai, J.; Yoshino, T.; Wasan, H.; Ciardiello, F.; Loupakis, F.; Hong, Y.S.; et al. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. N. Engl. J. Med. 2019, 381, 1632–1643. [Google Scholar] [CrossRef]
- Redman, M.W.; Papadimitrakopoulou, V.; Minichiello, K.; Gandara, D.R.; Hirsch, F.R.; Mack, P.C.; Schwartz, L.H.; Vokes, E.E.; Ramalingam, S.S.; Leighl, N.B.; et al. Lung-MAP (SWOG S1400): Design, implementation, and lessons learned from a biomarker-driven master protocol (BDMP) for previously-treated squamous lung cancer (sqNSCLC). J. Clin. Oncol. 2020, 38, 9576. [Google Scholar] [CrossRef]
- van Cutsem, E.; Huijberts, S.; Grothey, A.; Yaeger, R.; Cuyle, P.; Elez, E. Therapy for patients with BRAF V600E—Mutant metastatic colorectal cancer: Safety lead-in results from the phase III BEACON colorectal cancer study. J. Clin. Oncol. 2019, 37, 22–24. [Google Scholar] [CrossRef]
- Kohno, T. Implementation of “clinical sequencing” in cancer genome medicine in Japan. Cancer Sci. 2018, 109, 507–512. [Google Scholar] [CrossRef]
- Kris, M.G.; Johnson, B.E.; Berry, L.D.; Kwiatkowski, D.J.; Iafrate, A.J.; Wistuba, I.I.; Varella-Garcia, M.; Franklin, W.A.; Aronson, S.L.; Su, P.F.; et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA J. Am. Med. Assoc. 2014, 311, 1998–2006. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef]
- Shaw, A.T.; Kim, D.-W.; Nakagawa, K.; Seto, T.; Crinó, L.; Ahn, M.-J.; De Pas, T.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N. Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef]
- Shaw, A.T.; Ou, S.-H.I.; Bang, Y.-J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-Rearranged Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; DuBois, S.G.; Lassen, U.N.; Demetri, G.D.; Nathenson, M.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef] [PubMed]
- Itoi, T.; Sofuni, A.; Itokawa, F.; Irisawa, A.; Khor, C.J.L.; Rerknimitr, R. Current status of diagnostic endoscopic ultrasonography in the evaluation of pancreatic mass lesions. Dig. Endosc. 2011, 23, 17–21. [Google Scholar] [CrossRef]
- Vilmann, P.; Hancke, S.; Henriksen, F.W.; Jacobsen, G.K. Endosonographically-guided fine needle aspiration biopsy of malignant lesions in the upper gastrointestinal tract. Endoscopy 1993, 25, 523–527. [Google Scholar] [CrossRef]
- Möller, K.; Papanikolaou, I.S.; Toermer, T.; Delicha, E.M.; Sarbia, M.; Schenck, U.; Koch, M.; Al-Abadi, H.; Meining, A.; Schmidt, H.; et al. EUS-guided FNA of solid pancreatic masses: High yield of 2 passes with combined histologic-cytologic analysis. Gastrointest. Endosc. 2009, 70, 60–69. [Google Scholar] [CrossRef]
- Iwashita, T.; Yasuda, I.; Mukai, T.; Doi, S.; Nakashima, M.; Uemura, S.; Mabuchi, M.; Shimizu, M.; Hatano, Y.; Hara, A.; et al. Macroscopic on-site quality evaluation of biopsy specimens to improve the diagnostic accuracy during EUS-guided FNA using a 19-gauge needle for solid lesions: A single-center prospective pilot study (MOSE study). Gastrointest. Endosc. 2015, 81, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Eloubeidi, M.A.; Jhala, D.; Chhieng, D.C.; Chen, V.K.; Eltoum, I.; Vickers, S.; Wilcox, C.M.; Jhala, N. Yield of endoscopic ultrasound-guided fine-needle aspiration biopsy in patients with suspected pancreatic carcinoma: Emphasis on atypical, suspicious, and false-negative aspirates. Cancer 2003, 99, 285–292. [Google Scholar] [CrossRef]
- Norton, I.D.; Petersen, B.T.; Bosco, J.; Nelson, D.B.; Meier, P.B.; Baron, T.H.; Lange, S.M.; Gostout, C.J.; Loeb, D.S.; Levy, M.J.; et al. A randomized trial of endoscopic biliary sphincterotomy using pure-cut versus combined cut and coagulation waveforms. Clin. Gastroenterol. Hepatol. 2005, 3, 1029–1033. [Google Scholar] [CrossRef]
- Bang, J.Y.; Hawes, R.; Varadarajulu, S. A meta-analysis comparing ProCore and standard fine-needle aspiration needles for endoscopic ultrasound-guided tissue acquisition. Endoscopy 2016, 48, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Ishigaki, K.; Nakai, Y.; Oyama, H.; Kanai, S.; Suzuki, T.; Nakamura, T.; Sato, T.; Hakuta, R.; Saito, K.; Saito, T.; et al. Endoscopic ultrasound-guided tissue acquisition by 22-gauge franseen and standard needles for solid pancreatic lesions. Gut Liver 2020, 14, 817–825. [Google Scholar] [CrossRef]
- Oppong, K.W.; Bekkali, N.L.H.; Leeds, J.S.; Johnson, S.J.; Nayar, M.K.; Darné, A.; Egan, M.; Bassett, P.; Haugk, B. Fork-tip needle biopsy versus fine-needle aspiration in endoscopic ultrasound-guided sampling of solid pancreatic masses: A randomized crossover study. Endoscopy 2020, 52, 454–461. [Google Scholar] [CrossRef]
- Hayashi, H.; Tanishima, S.; Fujii, K.; Mori, R.; Okamura, Y.; Yanagita, E.; Matsuoka, R.; Amano, T.; Kinoshita, I.; Komatsu, Y.; et al. Genomic testing for pancreatic cancer in clinical practice as real-world evidence. Pancreatology 2018, 18, 647–654. [Google Scholar] [CrossRef]
- Fujita, H.; Ohuchida, K.; Mizumoto, K.; Itaba, S.; Ito, T.; Nakata, K.; Yu, J.; Kayashima, T.; Souzaki, R.; Tajiri, T.; et al. Gene expression levels as predictive markers of outcome in pancreatic cancer after gemcitabine-based adjuvant chemotherapy. Neoplasia 2010, 12, 807–817. [Google Scholar] [CrossRef]
- Ashida, R.; Nakata, B.; Shigekawa, M.; Mizuno, N.; Sawaki, A.; Hirakawa, K.; Arakawa, T.; Yamao, K. Gemcitabine sensitivity-related mRNA expression in endoscopic ultrasound-guided fine-needle aspiration biopsy of unresectable pancreatic cancer. J. Exp. Clin. Cancer Res. 2009, 28, 1–7. [Google Scholar] [CrossRef]
- Bang, J.Y.; Magee, S.H.; Ramesh, J.; Trevino, J.M.; Varadarajulu, S. Randomized trial comparing fanning with standard technique for endoscopic ultrasound-guided fine-needle aspiration of solid pancreatic mass lesions. Endoscopy 2013, 45, 445–450. [Google Scholar] [CrossRef]
- Bang, J.Y.; Hebert-Magee, S.; Navaneethan, U.; Hasan, M.K.; Hawes, R.; Varadarajulu, S. EUS-guided fine needle biopsy of pancreatic masses can yield true histology: Results of a randomised trial. Gut 2017, 67, 2081–2084. [Google Scholar] [CrossRef]
- Archibugi, L.; Ruta, V.; Panzeri, V.; Redegalli, M.; Testoni, S.G.G.; Petrone, M.C.; Rossi, G.; Falconi, M.; Reni, M.; Doglioni, C.; et al. RNA extraction from endoscopic ultrasound-acquired tissue of pancreatic cancer is feasible and allows investigation of molecular features. Cells 2020, 9, 2561. [Google Scholar] [CrossRef] [PubMed]
- Elhanafi, S.; Mahmud, N.; Vergara, N.; Kochman, M.L.; Das, K.K.; Ginsberg, G.G.; Rajala, M.; Chandrasekhara, V. Comparison of endoscopic ultrasound tissue acquisition methods for genomic analysis of pancreatic cancer. J. Gastroenterol. Hepatol. 2019, 34, 907–913. [Google Scholar] [CrossRef]
- Semaan, A.; Bernard, V.; Lee, J.J.; Wong, J.W.; Huang, J.; Swartzlander, D.B.; Stephens, B.M.; Monberg, M.E.; Weston, B.; Bhutani, M.S.; et al. Defining the comprehensive genomic landscapes of pancreatic ductal adenocarcinoma using real world endoscopic aspiration samples. Clin. Cancer Res. 2020, 27, 1082–1093. [Google Scholar] [CrossRef]
- Jones, S.; Zhang, X.; Parsons, D.W.; Lin, J.C.H.; Leary, R.J.; Angenendt, P.; Mankoo, P.; Carter, H.; Kamiyama, H.; Jimeno, A.; et al. Core signaling pathways in human pancreatic cancers revealed by global genomic analyses. Science 2008, 321, 1801–1806. [Google Scholar] [CrossRef]
- Waddell, N.; Pajic, M.; Patch, A.M.; Chang, D.K.; Kassahn, K.S.; Bailey, P.; Johns, A.L.; Miller, D.; Nones, K.; Quek, K.; et al. Whole genomes redefine the mutational landscape of pancreatic cancer. Nature 2015, 518, 495–501. [Google Scholar] [CrossRef]
- Hayashi, H.; Kohno, T.; Ueno, H.; Hiraoka, N.; Kondo, S.; Saito, M.; Shimada, Y.; Ichikawa, H.; Kato, M.; Shibata, T.; et al. Utility of assessing the number of mutated KRAS, CDKN2A, TP53, and SMAD4 genes using a targeted deep sequencing assay as a prognostic biomarker for pancreatic cancer. Pancreas 2017, 46, 335–340. [Google Scholar] [CrossRef]
- Lowery, M.A.; Jordan, E.J.; Basturk, O.; Ptashkin, R.N.; Zehir, A.; Berger, M.F.; Leach, T.; Herbst, B.; Askan, G.; Maynard, H.; et al. Real-time genomic profiling of pancreatic ductal adenocarcinoma: Potential actionability and correlation with clinical phenotype. Clin. Cancer Res. 2017, 23, 6094–6100. [Google Scholar] [CrossRef]
- Golan, T.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance olaparib for germline BRCA-mutated metastatic pancreatic cancer. N. Engl. J. Med. 2019, 381, 317–327. [Google Scholar] [CrossRef]
- Nicolle, R.; Blum, Y.; Marisa, L.; Loncle, C.; Gayet, O.; Moutardier, V.; Turrini, O.; Giovannini, M.; Bian, B.; Bigonnet, M.; et al. Pancreatic adenocarcinoma therapeutic targets revealed by tumor-stroma cross-talk analyses in patient-derived xenografts. Cell Rep. 2017, 21, 2458–2470. [Google Scholar] [CrossRef] [PubMed]
- Bailey, P.; Chang, D.K.; Nones, K.; Johns, A.L.; Patch, A.M.; Gingras, M.C.; Miller, D.K.; Christ, A.N.; Bruxner, T.J.C.; Quinn, M.C.; et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature 2016, 531, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Witkiewicz, A.K.; Balaji, U.; Eslinger, C.; McMillan, E.; Conway, W.; Posner, B.; Mills, G.B.; O’Reilly, E.M.; Knudsen, E.S. Integrated patient-derived models delineate individualized therapeutic vulnerabilities of pancreatic cancer. Cell Rep. 2016, 16, 2017–2031. [Google Scholar] [CrossRef]
- Driehuis, E.; Van Hoeck, A.; Moore, K.; Kolders, S.; Francies, H.E.; Gulersonmez, M.C.; Stigter, E.C.A.; Burgering, B.; Geurts, V.; Gracanin, A.; et al. Pancreatic cancer organoids recapitulate disease and allow personalized drug screening. Proc. Natl. Acad. Sci. USA 2019, 116, 26580–26590. [Google Scholar] [CrossRef] [PubMed]
- Wolff, R.A.; Wang-Gillam, A.; Alvarez, H.; Tiriac, H.; Engle, D.; Hou, S.; Groff, A.F.; Lucas, A.S.; Bernard, V.; Allenson, K.; et al. Dynamic changes during the treatment of pancreatic cancer. Oncotarget 2018, 9, 14764–14790. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Holtzinger, A.; Jagan, I.; Begora, M.; Lohse, I.; Ngai, N.; Nostro, C.; Wang, R.; Muthuswamy, L.B.; Crawford, H.C.; et al. Ductal pancreatic cancer modeling and drug screening using human pluripotent stem cell- and patient-derived tumor organoids. Nat. Med. 2015, 21, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Ricci-Vitiani, L.; Lombardi, D.G.; Pilozzi, E.; Biffoni, M.; Todaro, M.; Peschle, C.; De Maria, R. Identification and expansion of human colon-cancer-initiating cells. Nature 2007, 445, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, N.; Sasaki, N.; Aoki, R.; Miyamoto, K.; Suda, W.; Teratani, T.; Suzuki, T.; Koda, Y.; Chu, P.S.; Taniki, N.; et al. Gut pathobionts underlie intestinal barrier dysfunction and liver T helper 17 cell immune response in primary sclerosing cholangitis. Nat. Microbiol. 2019, 4, 492–503. [Google Scholar] [CrossRef] [PubMed]
- Seino, T.; Kawasaki, S.; Shimokawa, M.; Tamagawa, H.; Toshimitsu, K.; Fujii, M.; Ohta, Y.; Matano, M.; Nanki, K.; Kawasaki, K.; et al. Human pancreatic tumor organoids reveal loss of stem cell niche factor dependence during disease progression. Cell Stem Cell 2018, 22, 454–467.e6. [Google Scholar] [CrossRef] [PubMed]
- Tiriac, H.; Belleau, P.; Engle, D.D.; Plenker, D.; Deschênes, A.; Somerville, T.D.D.; Froeling, F.E.M.; Burkhart, R.A.; Denroche, R.E.; Jang, G.H.; et al. Organoid profiling identifies common responders to chemotherapy in pancreatic cancer. Cancer Discov. 2018, 8, 1112–1129. [Google Scholar] [CrossRef] [PubMed]
- Tuveson, D.; Clevers, H. Cancer modeling meets human organoid technology. Science 2019, 364, 952–955. [Google Scholar] [CrossRef] [PubMed]
- Nanki, K.; Fujii, M.; Shimokawa, M.; Matano, M.; Nishikori, S.; Date, S.; Takano, A.; Toshimitsu, K.; Ohta, Y.; Takahashi, S.; et al. Somatic inflammatory gene mutations in human ulcerative colitis epithelium. Nature 2020, 577, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Nanki, K.; Toshimitsu, K.; Takano, A.; Fujii, M.; Shimokawa, M.; Ohta, Y.; Matano, M.; Seino, T.; Nishikori, S.; Ishikawa, K.; et al. Divergent routes toward wnt and R-spondin niche independency during human gastric carcinogenesis. Cell 2018, 174, 856–869.e17. [Google Scholar] [CrossRef] [PubMed]
- Sbeit, W.; Kadah, A.; Mari, A.; Mahamid, M.; Khoury, T. A Comprehensive narrative review on the evolving role of endoscopic ultrasound in focal solid liver lesions diagnosis and management. Diagnostics 2020, 10, 688. [Google Scholar] [CrossRef]
- Yao, Y.; Xu, X.; Yang, L.; Zhu, J.; Wan, J.; Shen, L.; Xia, F.; Fu, G.; Deng, Y.; Pan, M.; et al. Patient-derived organoids predict chemoradiation responses of locally advanced rectal cancer. Cell Stem Cell 2020, 26, 17–26.e6. [Google Scholar] [CrossRef]
- Li, D.; Xie, K.; Wolff, R.; Abbruzzese, J.L. Pancreatic cancer. Lancet 2004, 363, 1049–1057. [Google Scholar] [CrossRef]
- Bang, J.Y.; Hebert-Magee, S.; Hasan, M.K.; Navaneethan, U.; Hawes, R.; Varadarajulu, S. Endoscopic ultrasonography-guided biopsy using a Franseen needle design: Initial assessment. Dig. Endosc. 2017, 29, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Boj, S.F.; Hwang, C.-I.; Baker, L.A.; Chio, I.I.C.; Engle, D.D.; Corbo, V.; Jager, M.; Ponz-Sarvise, M.; Tiriac, H.; Spector, M.S.; et al. Organoid models of human and mouse ductal pancreatic cancer. Cell 2015, 160, 324–338. [Google Scholar] [CrossRef] [PubMed]
- Bian, B.; Juiz, N.A.; Gayet, O.; Bigonnet, M.; Brandone, N.; Roques, J.; Cros, J.; Wang, N.; Dusetti, N.; Iovanna, J. Pancreatic cancer organoids for determining sensitivity to bromodomain and extra-terminal inhibitors (BETI). Front. Oncol. 2019, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Vilgelm, A.E.; Bergdorf, K.; Wolf, M.; Bharti, V.; Shattuck-Brandt, R.; Blevins, A.; Jones, C.; Phifer, C.; Lee, M.; Lowe, C.; et al. Fine-needle aspiration-based patient-derived cancer organoids. iScience 2020, 23, 101408. [Google Scholar] [CrossRef]
- Juiz, N.; Elkaoutari, A.; Bigonnet, M.; Gayet, O.; Roques, J.; Nicolle, R.; Iovanna, J.; Dusetti, N. Basal-like and classical cells coexist in pancreatic cancer revealed by single-cell analysis on biopsy-derived pancreatic cancer organoids from the classical subtype. FASEB J. 2020, 34, 12214–12228. [Google Scholar] [CrossRef] [PubMed]
- Lacomb, J.F.; Plenker, D.; Tiriac, H.; Bucobo, J.C.; D’souza, L.S.; Khokhar, A.S.; Patel, H.; Channer, B.; Joseph, D.; Wu, M.; et al. Single-pass vs 2-pass endoscopic ultrasound-guided fine-needle biopsy sample collection for creation of pancreatic adenocarcinoma organoids. Clin. Gastroenterol. Hepatol. 2020. online ahead of print. [Google Scholar] [CrossRef]
- Hennig, A.; Wolf, L.; Jahnke, B.; Polster, H.; Seidlitz, T.; Werner, K.; Aust, D.E.; Hampe, J.; Distler, M.; Weitz, J.; et al. CFTR expression analysis for subtyping of human pancreatic cancer organoids. Stem Cells Int. 2019, 2019, 1024614. [Google Scholar] [CrossRef] [PubMed]
- Bode, K.J.; Mueller, S.; Schweinlin, M.; Metzger, M.; Brunner, T. A fast and simple fluorometric method to detect cell death in 3D intestinal organoids. Biotechniques 2019, 67, 23–28. [Google Scholar] [CrossRef]
- Frappart, P.O.; Hofmann, T.G. Pancreatic ductal adenocarcinoma (Pdac) organoids: The shining light at the end of the tunnel for drug response prediction and personalized medicine. Cancers 2020, 12, 2750. [Google Scholar] [CrossRef] [PubMed]
- Brand, R.E.; Adai, A.T.; Centeno, B.A.; Lee, L.S.; Rateb, G.; Vignesh, S.; Menard, C.; Wiechowska-Kozłowska, A.; Bołdys, H.; Hartleb, M.; et al. A microRNA-based test improves endoscopic ultrasound-guided cytologic diagnosis of pancreatic cancer. Clin. Gastroenterol. Hepatol. 2014, 12, 1717–1723. [Google Scholar] [CrossRef]
- Ungureanu, B.S.; Pirici, D.; Dima, S.O.; Popescu, I.; Hundorfean, G.; Surlin, V.; Saftoiu, A. Morphometric assessment of confocal laser endomicroscopy for pancreatic ductal adenocarcinoma, an ex-vivo pilot study. Diagnostics 2020, 10, 923. [Google Scholar] [CrossRef]
- Underwood, P.W.; Gerber, M.H.; Nguyen, K.; Delitto, D.; Han, S.; Thomas, R.M.; Forsmark, C.E.; Trevino, J.G.; Gooding, W.E.; Hughes, S.J. Protein signatures and tissue diagnosis of pancreatic cancer. J. Am. Coll. Surg. 2020, 230, 26–36.e1. [Google Scholar] [CrossRef]
- Ashizawa, K.; Yoshimura, K.; Johno, H.; Inoue, T.; Katoh, R.; Funayama, S.; Sakamoto, K.; Takeda, S.; Masuyama, K.; Matsuoka, T.; et al. Construction of mass spectra database and diagnosis algorithm for head and neck squamous cell carcinoma. Oral Oncol. 2017, 75, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, K.; Mandal, M.K.; Hara, M.; Fujii, H.; Chen, L.C.; Tanabe, K.; Hiraoka, K.; Takeda, S. Real-time diagnosis of chemically induced hepatocellular carcinoma using a novel mass spectrometry-based technique. Anal. Biochem. 2013, 441, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Mandal, M.K.; Yoshimura, K.; Chen, L.C.; Yu, Z.; Nakazawa, T.; Katoh, R.; Fujii, H.; Takeda, S.; Nonami, H.; Hiraoka, K. Application of probe electrospray ionization mass spectrometry (PESI-MS) to clinical diagnosis: Solvent effect on lipid analysis. J. Am. Soc. Mass Spectrom. 2012, 23, 2043–2047. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.Y.; Correa, E.; Yoshimura, K.; Chang, M.C.; Dennison, A.; Takeda, S.; Chang, Y.T. Using probe electrospray ionization mass spectrometry and machine learning for detecting pancreatic cancer with high performance. Am. J. Transl. Res. 2020, 12, 171–179. [Google Scholar]

{kind=link}
| Authors and Year | Method of Sampling and Type of Needle | Number of Patients | Successfully Sequenced Samples, n (%) |
|---|---|---|---|
| Larson et al. [10], 2018 | EUS-FNB EUS-FNA Percutaneous | 54 7 8 | 38 (70.4%) 3 (42.9%) 8 (100%) |
| Hayashi et al. [40], 2018 | EUS-FNA (FFPE) 22-G | 9 | 7 (78%) Re-biopsy 2 (22%) |
| Elhanafi et al. [46], 2020 | EUS-FNB 22-G EUS-FNA 22-G | 22 145 | 20 (90.9%) 97 (66.9%) |
| Semaan et al. [47], 2020 | EUS-FNA (cytology) | ND | 23 (ND) |
| Kandel et al. [6], 2020 | EUS-FNB (fresh frozen) EUS-FNA (fresh frozen) 19-G for body and tail/22-G for head | 50 50 | 39 (78%) 7 (14%) |
| Authors, Year | Method of Sampling/Type of Needle | Number of Patients | Number of Organoids Created n (%) |
|---|---|---|---|
| Boj et al. [70], 2015 | FNA/ND | ND | 2 (primary and metastasis) |
| Tiriac et al. [62], 2018 | FNB/22-G | 60 | 43 (71%) |
| Seino et al. [61], 2019 | FNB/22-G | ND | 27 (ND) |
| Bian et al. [71], 2019 | FNB/ND | ND | 24 (85%) |
| Henning et al. [75] 2019 | FNA/ND | 6 | 5 (83%) |
| Vilgelm et al. [72], 2020 | FNA/25-G | 5 | 5 (ex vivo tumor, 100%) |
| Juiz et al. [73], 2020 | ND | ND | 20 (ND) |
| Lacomb et al. [74], 2020 | FNB/22-G 1 pass FNB/22-G 2 pass | 25 42 | 22 (88%) 34 (81%) |
| Authors, Year | ECM-Matrix | Medium |
|---|---|---|
| Tiriac et al., 2018 [8] | Matrigel 100% Dome-type | Advanced DMEM/F12, HEPES (10 mM), Glutamax (1X), A83-01 (500 nM), hEGF (50 ng/mL), mNoggin (100 ng/mL), hFGF10 (100 ng/mL), hGastrin I (10 nM), N-acetylcysteine (1.25 mM), Nicotinamide (10 mM), PGE2 (1 μM), B27 supplement (1X), R-spondin-1 (10%), Afamin/Wnt3A (50%). |
| Seino et al., 2018 [61] | GFR-Matrigel 100% Dome-type | Advanced DMEM/F12, HEPES (10 mM), Glutamax (2 mM), B27 (1X), Gastrin I (10 nM), N-acetylcysteine (1 mM), mEGF (50 ng/mL), mNoggin (100 ng/mL), R-spondin-1 (10%), Afamin-Wnt-3A (25%), A83-01 (500 nM), SB202190 (10 μM). |
| Bian et al., 2019 [71]/Juiz et al., 2020 [73] | GFR-Matrigel 100% Dome-type | Advanced DMEM/F12, HEPES (10 mM), Glutamax (1X), hFGF10 (100 ng/mL); hEGF (50 ng/mL), hNoggin (100 ng/mL), Wnt3a (30%), R-spondin-1 (10%), hGastrin I (10 nM), Nicotinamide (10 mM), N-acetylcysteine (1.25 mM), B27 (1X); A83-01 (500 nM); Y27632 (10.5 µM). |
| Hennig et al., 2019 [75] | GFR-Matrigel Dome-type | DMEM/F12, Wnt3a (50%), HEPES (1X), Pen/Strep (1X), and 1x Glutamax (1X), Noggin (10%), R-spondin-1 (10%), B27 (1X), Nicotinamide (10 mM), gastrin (1 nM), N-acetyl-L-cysteine (1 mM), Primocin (1 mg/mL), mEGF (50 ng/mL), hFGF10 (100 ng/mL), A-83-01 (0.5 μM), N2 (1X). |
| Authors, Year | Plate | Number of Seeded Cells | Timing of Assay | Assay Method | Target Agents | No of PDOs |
|---|---|---|---|---|---|---|
| Tiriac et al., 2018 [8] | 96 well | 500 cells/well | 5 days after administration. | CellTiter-Glo® (luminescence ATP) | 5 | 66 |
| Driehuis et al., 2019 [56] | 384 well | ND | 3 days after administration. | CellTiter-Glo® (luminescence ATP) | 76 | 24 |
| Frappart et al., 2020 [77] | 96 well | 2000 cells/well | 4 days after administration. | CytoTox-GloTM (luminescence non-ATP) | 22 | 21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwasaki, E.; Fukuhara, S.; Horibe, M.; Kawasaki, S.; Seino, T.; Takimoto, Y.; Tamagawa, H.; Machida, Y.; Kayashima, A.; Noda, M.; et al. Endoscopic Ultrasound-Guided Sampling for Personalized Pancreatic Cancer Treatment. Diagnostics 2021, 11, 469. https://doi.org/10.3390/diagnostics11030469
Iwasaki E, Fukuhara S, Horibe M, Kawasaki S, Seino T, Takimoto Y, Tamagawa H, Machida Y, Kayashima A, Noda M, et al. Endoscopic Ultrasound-Guided Sampling for Personalized Pancreatic Cancer Treatment. Diagnostics. 2021; 11(3):469. https://doi.org/10.3390/diagnostics11030469
Chicago/Turabian StyleIwasaki, Eisuke, Seiichiro Fukuhara, Masayasu Horibe, Shintaro Kawasaki, Takashi Seino, Yoichi Takimoto, Hiroki Tamagawa, Yujiro Machida, Atsuto Kayashima, Marin Noda, and et al. 2021. "Endoscopic Ultrasound-Guided Sampling for Personalized Pancreatic Cancer Treatment" Diagnostics 11, no. 3: 469. https://doi.org/10.3390/diagnostics11030469
APA StyleIwasaki, E., Fukuhara, S., Horibe, M., Kawasaki, S., Seino, T., Takimoto, Y., Tamagawa, H., Machida, Y., Kayashima, A., Noda, M., Hayashi, H., & Kanai, T. (2021). Endoscopic Ultrasound-Guided Sampling for Personalized Pancreatic Cancer Treatment. Diagnostics, 11(3), 469. https://doi.org/10.3390/diagnostics11030469