
New Predictive Biomarkers for Ovarian Cancer


 ,
, 
Abstract
1. Introduction
Search Strategy of Review
2. An Overview of Ovarian Cancer Biomarkers and Cell Signalling Pathways
2.1. Ovarian Cancer Cell Signalling Pathways and Their Clinical Utility
2.1.1. BRCA1 and BRCA2 Pathway
2.1.2. MAPK/ERK Pathway
2.1.3. EGFR/AKT Signalling Pathway
2.1.4. Integrin Inhibitor Pathway
2.1.5. GRP78 Expression Pathway
2.1.6. P38 Alpha Pathway
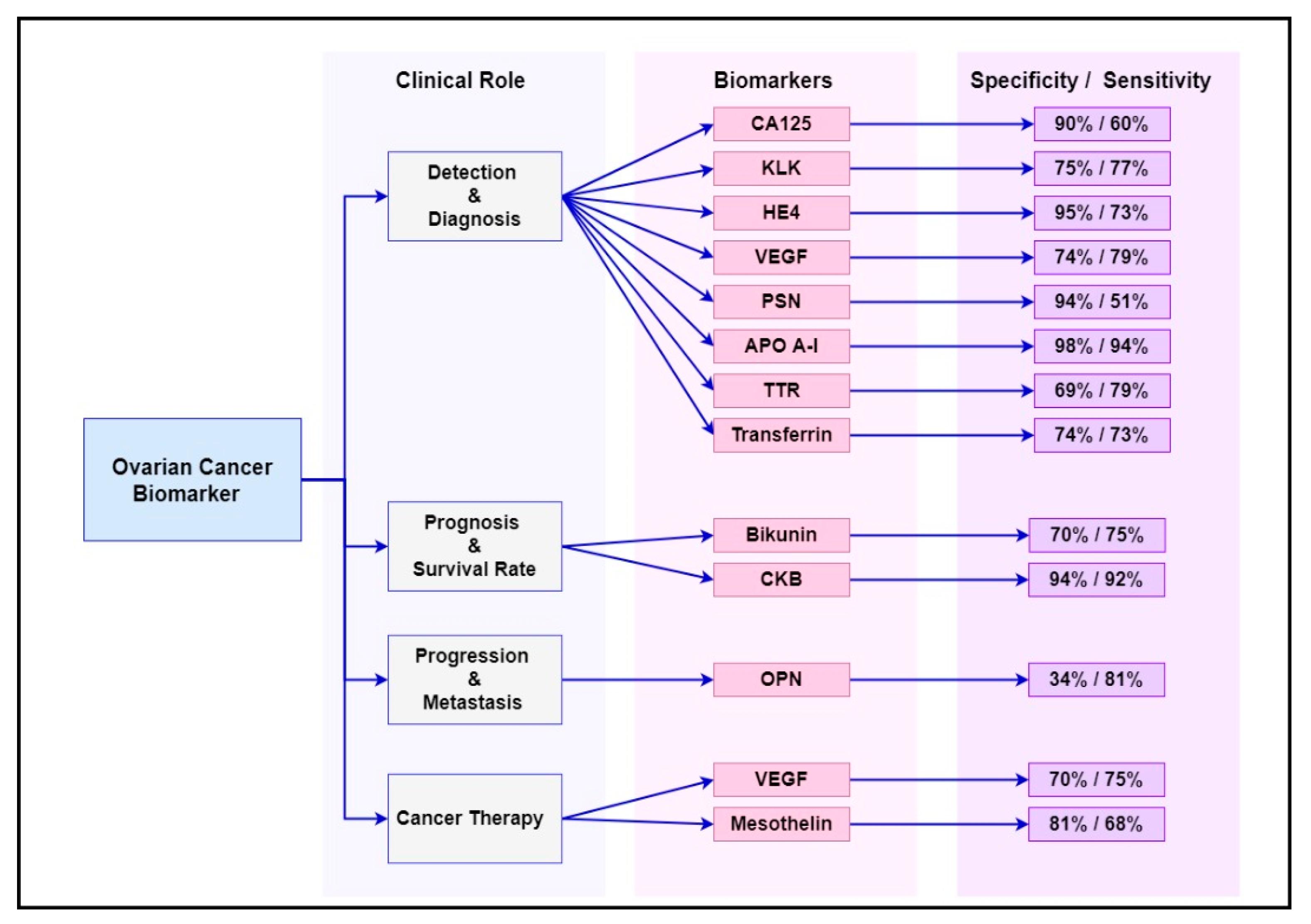
2.2. Current Biomarkers Associated with Diagnosis, Progression and Treatment Response of Ovarian Cancer
2.2.1. Carbohydrate Antigen 125 (CA125)
2.2.2. Osteopontin (OPN)
2.2.3. Kallikreins (KLKs)
2.2.4. Bikunin
2.2.5. Human Epididymis Protein 4 (HE4)
2.2.6. Vascular Endothelial Growth Factor (VEGF)
2.2.7. Human Prostasin (PSN)
2.2.8. Creatine Kinase B (CKB)
2.2.9. Mesothelin
2.2.10. Apolipoprotein A-I (apoA-I)
2.2.11. Transthyretin (TTR)
2.2.12. Transferrin
2.3. Highlighting the Most Common Biomarker Combinations for the Management of Ovarian Cancer
3. Emerging Predictive Ovarian Cancer Biomarkers
3.1. An Overview of the Molecular Approaches to the Discovery of New Ovarian Cancer Biomarkers
3.1.1. Whole Genome Analysis
3.1.2. Transcription Profiling
3.1.3. MicroRNA Profiling
3.1.4. Proteomic Profiling
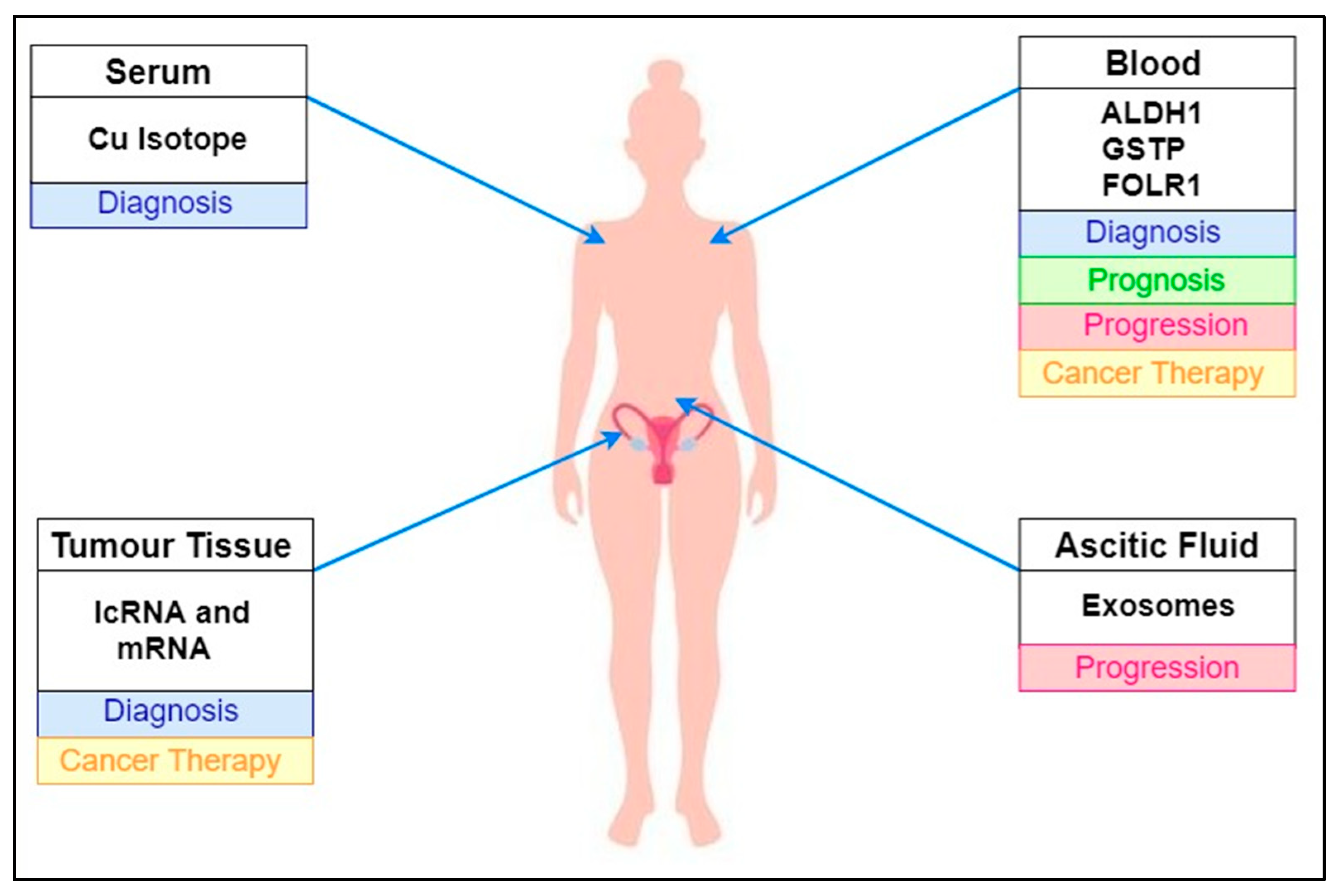
3.2. Emerging Biomarkers Associated with Ovarian Cancer Diagnosis and Prognosis
3.2.1. Cu Isotope
3.2.2. Exosomes
3.2.3. lncRNA and mRNA Biomarkers
3.2.4. Aldehyde Dehydrogenase 1 (ALDH1)
3.2.5. Folate Receptor Alpha (FOLR1)
3.2.6. Glutathione S-Transferase Polymorphisms
4. Summary and Discussion
5. Future Directions
6. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jayson, G.C.; Kohn, E.C.; Kitchener, H.C.; Ledermann, J.A. Ovarian cancer. Lancet 2014, 384, 1376–1388. [Google Scholar] [CrossRef]
- Ries, L.A.G.; Kosary, C.L.; Hankey, B.F.; Miller, B.A.; Edwards, B.K. SEER Cancer Statistics Review, 1973–1995; National Cancer Institute: Bethesda, MD, USA, 1998. [Google Scholar]
- Prat, J. Pathology of borderline and invasive cancers. Best Pr. Res. Clin. Obstet. Gynaecol. 2017, 41, 15–30. [Google Scholar] [CrossRef]
- Carcangiu, M.L.; Kurman, R.J.; Carcangiu, M.L.; Herrington, C.S. WHO Classification of Tumours of Female Reproductive Organs, International Agency for Research on Cancer; Wiley Online Library: Hoboken, NJ, USA, 2014. [Google Scholar]
- Grisham, R.N. Low-Grade Serous Carcinoma of the Ovary. Oncology 2016, 30, 650–652. [Google Scholar] [PubMed]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef]
- Klotz, D.M.; Wimberger, P. Cells of origin of ovarian cancer: Ovarian surface epithelium or fallopian tube? Arch. Gynecol. Obstet. 2017, 296, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Kurman, R.J.; Shih, I.-M. The Origin and Pathogenesis of Epithelial Ovarian Cancer: A Proposed Unifying Theory. Am. J. Surg. Pathol. 2010, 34, 433–443. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Raja, F.A.; Fotopoulou, C.; Gonzalez-Martin, A.; Colombo, N.; Sessa, C. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi24–vi32. [Google Scholar] [CrossRef] [PubMed]
- A Doherty, J.; Peres, L.C.; Wang, C.; Way, G.P.; Greene, C.S.; Schildkraut, J.M. Challenges and Opportunities in Studying the Epidemiology of Ovarian Cancer Subtypes. Curr. Epidemiol. Rep. 2017, 4, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Smolle, E.; Taucher, V.; Pichler, M.; Petru, E.; Lax, S.; Haybaeck, J. Targeting Signaling Pathways in Epithelial Ovarian Cancer. Int. J. Mol. Sci. 2013, 14, 9536–9555. [Google Scholar] [CrossRef] [PubMed]
- Norquist, B.M.; Garcia, R.L.; Allison, K.H. The molecular pathogenesis of hereditary ovarian carcinoma: Alterations in the tubal epithelium of women with BRCA1 and BRCA2 mutations. Cancer 2010, 116, 5261–5271. [Google Scholar] [CrossRef]
- Press, J.Z.; Wurz, K.; Norquist, B.M.; Lee, M.K.; Pennil, C.; Garcia, R.; Welcsh, P.; Goff, B.A.; Swisher, E.M. Identification of a Preneoplastic Gene Expression Profile in Tubal Epithelium of BRCA1 Mutation Carriers. Neoplasia 2010, 12, 993–1002. [Google Scholar] [CrossRef]
- Press, J.Z.; De Luca, A.; Boyd, N.; Young, S.; Troussard, A.; Ridge, Y.; Kaurah, P.; Kalloger, S.; A Blood, K.; Smith, M.; et al. Ovarian carcinomas with genetic and epigenetic BRCA1 loss have distinct molecular abnormalities. BMC Cancer 2008, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Tinelli, A.; Malvasi, A.; Leo, G.; Vergara, D.; Pisanò, M.; Ciccarese, M.; Chiuri, V.E.; Lorusso, V. Hereditary ovarian cancers: From BRCA mutations to clinical management. A modern appraisal. Cancer Metastasis Rev. 2010, 29, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Scully, R.; Livingston, D.M. In search of the tumour-suppressor functions of BRCA1 and BRCA2. Nat. Cell Biol. 2000, 408, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Tan, A.R. PARP Inhibitors. Curr. Breast Cancer Rep. 2011, 3, 44–54. [Google Scholar] [CrossRef]
- Mangerich, A.; Bürkle, A. How to kill tumor cells with inhibitors of poly(ADP-ribosyl)ation. Int. J. Cancer 2010, 128, 251–265. [Google Scholar] [CrossRef] [PubMed]
- I Szabo, C.; King, M.C. Inherited breast and ovarian cancer. Hum. Mol. Genet. 1995, 4, 1811–1817. [Google Scholar] [CrossRef]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- Nakayama, K.; Nakayama, N.; Kurman, R.J.; Cope, L.M.; Pohl, G.; Samuels, Y.; Velculescu, V.E.; Wang, T.-L.; Shih, I.-M. Sequence mutations and amplification of PIK3CA and AKT2 genes in purified ovarian serous neoplasms. Cancer Biol. Ther. 2006, 5, 779–785. [Google Scholar] [CrossRef]
- Singer, G.; Oldt, R.; Cohen, Y.; Wang, B.G.; Sidransky, D.; Kurman, R.J.; Shih, I.-M. Mutations in BRAF and KRAS Characterize the Development of Low-Grade Ovarian Serous Carcinoma. J. Natl. Cancer Inst. 2003, 95, 484–486. [Google Scholar] [CrossRef]
- Peyssonnaux, C.; Eychène, A. The Raf/MEK/ERK pathway: New concepts of activation. Biol. Cell 2001, 93, 53–62. [Google Scholar] [CrossRef]
- Allen, L.F.; Sebolt-Leopold, J.; Meyer, M.B. CI-1040 (PD184352), a targeted signal transduction inhibitor of MEK (MAPKK). In Seminars in Oncology; Elsevier: Amsterdam, The Netherlands, 2003. [Google Scholar]
- Choi, K.-C.; Kang, S.K.; Tai, C.-J. Follicle-stimulating hormone activates mitogen-activated protein kinase in preneoplastic and neoplastic ovarian surface epithelial cells. J. Clin. Endocrinol. Metab. 2002, 87, 2245–2253. [Google Scholar] [CrossRef]
- Gershenson, D. A Randomized Phase II/III Study to Assess the Efficacy of Trametinib in Patientswith Recurrent or Progressive Low-Grade Serous Ovarian or Peritoneal Cancer. In Gynecologic Oncology; 525 B ST, STE 1900; Academic Press Inc.: Cambridge, MA, USA; Elsevier Science: San Diego, CA, USA, 2020; p. 92101. [Google Scholar]
- Farley, J.H.; Brady, W.E.; Vathipadiekal, V.; Lankes, H.A.; Coleman, R.L.; Morgan, M.A.; Mannel, R.S.; Yamada, S.D.; Mutch, D.G.; Rodgers, W.H.; et al. Selumetinib in women with recurrent low-grade serous carcinoma of the ovary or peritoneum: An open-label, single-arm, phase 2 study. Lancet Oncol. 2013, 14, 134–140. [Google Scholar] [CrossRef]
- Zeineldin, R.; Muller, C.Y.; Stack, M.S.; Hudson, L.G. Targeting the EGF Receptor for Ovarian Cancer Therapy. J. Oncol. 2009, 2010, 1–11. [Google Scholar] [CrossRef]
- Fontanini, G.; Vignati, S.; Bigini, D.; Mussi, A.; Lucchi, H.; Angeletti, C.; Pingitore, R.; Pepe, S.; Basolo, F.; Bevilacqua, G. Epidermal growth factor receptor (EGFr) expression in non-small cell lung carcinomas correlates with metastatic involvement of hilar and mediastinal lymph nodes in the squamous subtype. Eur. J. Cancer 1995, 31, 178–183. [Google Scholar] [CrossRef]
- Jorissen, R.N. Epidermal growth factor receptor: Mechanisms of activation and signalling. Exp. Cell Res. 2003, 284, 31–53. [Google Scholar] [CrossRef]
- Casanova, M.L.; Larcher, F.; Casanova, B.; Murillas, R.; Fernández-Aceñero, M.J.; Villanueva, C.; Martínez-Palacio, J.; Ullrich, A.; Conti, C.J.; Jorcano, J.L. A critical role for ras-mediated, epidermal growth factor receptor-dependent angiogenesis in mouse skin carcinogenesis. Cancer Res. 2002, 62, 3402–3407. [Google Scholar] [PubMed]
- A Altomare, D.; Wang, H.Q.; Skele, K.L.; De Rienzo, A.; Klein-Szanto, A.J.; Godwin, A.K.; Testa, J.R. AKT and mTOR phosphorylation is frequently detected in ovarian cancer and can be targeted to disrupt ovarian tumor cell growth. Oncogene 2004, 23, 5853–5857. [Google Scholar] [CrossRef] [PubMed]
- Harandi, A.; Zaidi, A.S.; Stocker, A.M.; Laber, D.A. Clinical Efficacy and Toxicity of Anti-EGFR Therapy in Common Cancers. J. Oncol. 2009, 2009, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Sawada, K.; Kimura, T. Potential of Integrin Inhibitors for Treating Ovarian Cancer: A Literature Review. Cancers 2017, 9, 83. [Google Scholar] [CrossRef]
- Sawada, K.; Ohyagi-Hara, C.; Kimura, T.; Morishige, K.-I. Integrin Inhibitors as a Therapeutic Agent for Ovarian Cancer. J. Oncol. 2011, 2012, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Delie, F.; Petignat, P.; Cohen, M. GRP78 Protein Expression in Ovarian Cancer Patients and Perspectives for a Drug-Targeting Approach. J. Oncol. 2012, 2012, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Matrone, A.; Grossi, V.; Chiacchiera, F.; Fina, E.; Cappellari, M.; Caringella, A.M.; Di Naro, E.; Loverro, G.; Simone, C. p38α Is Required for Ovarian Cancer Cell Metabolism and Survival. Int. J. Gynecol. Cancer 2010, 20, 203–211. [Google Scholar] [CrossRef]
- Grossi, V.; Simone, C. Special Agents Hunting down Women Silent Killer: The Emerging Role of the p38αKinase. J. Oncol. 2012, 2012, 1–7. [Google Scholar] [CrossRef]
- Bast, R.C., Jr.; Siegal, F.P. Elevation of serum CA 125 prior to diagnosis of an epithelial ovarian carcinoma. Gynecol. Oncol. 1985, 22, 115–120. [Google Scholar] [CrossRef]
- Paramasivam, S.; Tripcony, L.; Crandon, A.; Quinn, M.; Hammond, I.; Marsden, D.; Proietto, A.; Davy, M.; Carter, J.; Nicklin, J.; et al. Prognostic Importance of Preoperative CA125 in International Federation of Gynecology and Obstetrics Stage I Epithelial Ovarian Cancer: An Australian Multicenter Study. J. Clin. Oncol. 2005, 23, 5938–5942. [Google Scholar] [CrossRef] [PubMed]
- Coticchia, C.M.; Yang, J.; Moses, M.A. Ovarian cancer biomarkers: Current options and future promise. J. Natl. Compr. Cancer Netw. 2008, 6, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.H.; Sakaguchi, H.; Fujimoto, J.; Tamaya, T. Osteopontin in metastatic lesions as a prognostic marker in ovarian cancers. J. Biomed. Sci. 2007, 14, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Ye, B.; Skates, S.; Mok, S.C.; Horick, N.K.; Rosenberg, H.F.; Vitonis, A.; Edwards, D.; Sluss, P.; Han, W.K.; Berkowitz, R.S.; et al. Proteomic-Based Discovery and Characterization of Glycosylated Eosinophil-Derived Neurotoxin and COOH-Terminal Osteopontin Fragments for Ovarian Cancer in Urine. Clin. Cancer Res. 2006, 12, 432–441. [Google Scholar] [CrossRef]
- Brakora, K.; Lee, H.; Yusuf, R.; Sullivan, L.; Harris, A.L.; Colella, T.; Seiden, M.V. Utility of osteopontin as a biomarker in recurrent epithelial ovarian cancer. Gynecol. Oncol. 2004, 93, 361–365. [Google Scholar] [CrossRef] [PubMed]
- A Borgoño, C.; Grass, L.; Soosaipillai, A.; Yousef, G.M.; Petraki, C.; Howarth, D.H.C.; Fracchioli, S.; Katsaros, D.; Diamandis, E.P. Human kallikrein 14: A new potential biomarker for ovarian and breast cancer. Cancer Res. 2003, 63, 9032–9041. [Google Scholar] [PubMed]
- Yousef, G.M.; ScorilasP, A.; Katsaros, D.; Fracchioli, S.; Iskander, L.; Borgono, C.; De La Longrais, I.A.R.; Puopolo, M.; Massobrio, M.; Diamandis, E.P. Prognostic Value of the Human Kallikrein Gene 15 Expression in Ovarian Cancer. J. Clin. Oncol. 2003, 21, 3119–3126. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Kobayashi, H.; Suzuki, M.; Kanayama, N.; Suzuki, M.; Terao, T. Upregulation of bikunin in tumor-infiltrating macrophages as a factor of favorable prognosis in ovarian cancer. Gynecol. Oncol. 2004, 94, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Kobayashi, H.; Suzuki, M.; Kanayama, N.; Suzuki, M.; Yamakawa, T.; Morishita, H.; Terao, T. Reduced bikunin gene expression as a factor of poor prognosis in ovarian carcinoma. Cancer 2003, 98, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, H.; Kobayashi, H.; Yagyu, T.; Wakahara, K.; Kondo, T.; Kurita, N.; Sekino, H.; Inagaki, K.; Suzuki, M.; Kanayama, N.; et al. Plasma Bikunin As a Favorable Prognostic Factor in Ovarian Cancer. J. Clin. Oncol. 2005, 23, 1463–1472. [Google Scholar] [CrossRef] [PubMed]
- Drapkin, R.; Von Horsten, H.H.; Lin, Y.; Mok, S.C.; Crum, C.P.; Welch, W.R.; Hecht, J.L. Human Epididymis Protein 4 (HE4) Is a Secreted Glycoprotein that Is Overexpressed by Serous and Endometrioid Ovarian Carcinomas. Cancer Res. 2005, 65, 2162–2169. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.G.; Miller, M.C.; DiSilvestro, P.; Landrum, L.M.; Gajewski, W.; Ball, J.J.; Skates, S.J. Evaluation of the Diagnostic Accuracy of the Risk of Ovarian Malignancy Algorithm in Women With a Pelvic Mass. Obstet. Gynecol. 2011, 118, 280–288. [Google Scholar] [CrossRef]
- Hellström, I.; Raycraft, J.; Hayden-Ledbetter, M.; A Ledbetter, J.; Schummer, M.; McIntosh, M.; Drescher, C.; Urban, N.; Hellström, K.E. The HE4 (WFDC2) protein is a biomarker for ovarian carcinoma. Cancer Res. 2003, 63, 3695–3700. [Google Scholar]
- Yamamoto, S.; Konishi, I.; Mandai, M.; Kuroda, H.; Komatsu, T.; Nanbu, K.; Sakahara, H.; Mori, T. Expression of vascular endothelial growth factor (VEGF) in epithelial ovarian neoplasms: Correlation with clinicopathology and patient survival, and analysis of serum VEGF levels. Br. J. Cancer 1997, 76, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Hefler, L.A.; Zeillinger, R.; Grimm, C.; Sood, A.K.; Cheng, W.-F.; Gadducci, A.; Tempfer, C.B.B.; Reinthaller, A. Preoperative serum vascular endothelial growth factor as a prognostic parameter in ovarian cancer. Gynecol. Oncol. 2006, 103, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Sriram, K.B.; Relan, V.; E Clarke, B.; E Duhig, E.; A Yang, I.; Bowman, R.V.; Lee, Y.C.G.; Fong, K.M. Diagnostic molecular biomarkers for malignant pleural effusions. Futur. Oncol. 2011, 7, 737–752. [Google Scholar] [CrossRef] [PubMed]
- Mok, S.C.; Chao, J.; Skates, S.; Wong, K.-K.; Yiu, G.K.; Muto, M.G.; Berkowitz, R.S.; Cramer, D.W. Prostasin, a Potential Serum Marker for Ovarian Cancer: Identification Through Microarray Technology. J. Natl. Cancer Inst. 2001, 93, 1458–1464. [Google Scholar] [CrossRef]
- Costa, F.P.; Rodrigues-Junior, V.; Zelmanowicz, A.; Svedman, C.; Devenz, G.; Alves, S.; Da Silva, A.S.M.; Garicochea, B. Prostasin, a potential tumor marker in ovarian cancer: A pilot study. Clinics 2009, 64, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-H.; Chen, X.-J.; Ou, W.-B.; Zhang, Q.; Lv, Z.-R.; Zhan, Y.; Ma, L.; Huang, T.; Yan, Y.-B.; Zhou, H.-M. Knockdown of creatine kinase B inhibits ovarian cancer progression by decreasing glycolysis. Int. J. Biochem. Cell Biol. 2013, 45, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Ghafoor, A.; Thomas, A.; Hassan, R. Targeting mesothelin in ovarian cancer. Oncotarget 2018, 9, 36050–36051. [Google Scholar] [CrossRef] [PubMed]
- Kreitman, R.J.; Hassan, R.; Fitzgerald, D.J.; Pastan, I. Phase I Trial of Continuous Infusion Anti-Mesothelin Recombinant Immunotoxin SS1P. Clin. Cancer Res. 2009, 15, 5274–5279. [Google Scholar] [CrossRef] [PubMed]
- Macuks, R.; Baidekalna, I.; Gritcina, J.; Avdejeva, A.; Donina, S. Apolipoprotein A1 and Transferrin as Biomarkers in Ovarian Cancer Diagnostics. Acta Chir. Latv. 2010, 10, 16. [Google Scholar] [CrossRef]
- Zamanian-Daryoush, M.; DiDonato, J.A. Apolipoprotein A-I and Cancer. Front. Pharmacol. 2015, 6. [Google Scholar] [CrossRef]
- Zhang, Z.; Bast, R.C.; Yu, Y.; Li, J.; Sokoll, L.J.; Rai, A.J.; Rosenzweig, J.M.; Cameron, B.; Wang, Y.Y.; Meng, X.-Y.; et al. Three Biomarkers Identified from Serum Proteomic Analysis for the Detection of Early Stage Ovarian Cancer. Cancer Res. 2004, 64, 5882–5890. [Google Scholar] [CrossRef]
- Liu, L.; Liu, J.; Dai, S.; Wang, X.; Wu, S.; Wang, J.; Huang, L.; Xiao, X.; He, D. Reduced transthyretin expression in sera of lung cancer. Cancer Sci. 2007, 98, 1617–1624. [Google Scholar] [CrossRef]
- Rastogi, M.; Gupta, S.; Sachan, M. Biomarkers towards Ovarian Cancer Diagnostics: Present and Future Prospects. Braz. Arch. Biol. Technol. 2016, 59, 59. [Google Scholar] [CrossRef]
- Yin, B.W.; Lloyd, K.O. Molecular cloning of the CA125 ovarian cancer antigen identification as a new mucin, MUC16. J. Biol. Chem. 2001, 276, 27371–27375. [Google Scholar] [CrossRef] [PubMed]
- Kampan, N.C.; Madondo, M.T.; Reynolds, J.; Hallo, J.; McNally, O.M.; Jobling, T.W.; Stephens, A.N.; Quinn, M.A.; Plebanski, M. Pre-operative sera interleukin-6 in the diagnosis of high-grade serous ovarian cancer. Sci. Rep. 2020, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-L.; Chiang, Y.-C.; Huang, C.-Y.; Lin, H.-W.; Chen, C.-A.; Hsieh, C.-Y.; Cheng, W.-F. Serous ovarian carcinoma patients with high alpha-folate receptor had reducing survival and cytotoxic chemo-response. Mol. Oncol. 2011, 6, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.; Cheng, R.S.; Mok, S.C. Identification of Differentially Expressed Genes from Ovarian Cancer Cells by MICROMAX™ cDNA Microarray System. Biotechniques 2001, 30, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Skates, S.J.; Uede, T.; Wong, K.; Schorge, J.O.; Feltmate, C.M.; Berkowitz, R.S.; Cramer, D.W.; Mok, S.C. Osteopontin as a potential diagnostic biomarker for ovarian cancer. JAMA 2002, 287, 1671–1679. [Google Scholar] [CrossRef] [PubMed]
- Diamandis, E.P.; Yousef, G.M. Human Tissue Kallikreins: A Family of New Cancer Biomarkers. Clin. Chem. 2002, 48, 1198–1205. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Magdolen, V.; Seidl, C.; Dorn, J.; Drecoll, E.; Kotzsch, M.; Yang, F.; Schmitt, M.; Schilling, O.; Rockstroh, A.; et al. Kallikrein-related peptidases 4, 5, 6 and 7 regulate tumour-associated factors in serous ovarian cancer. Br. J. Cancer 2018, 119, 1–9. [Google Scholar] [CrossRef]
- Luo, L.Y.; Katsaros, D.; Scorilas, A.; Fracchioli, S.; Piccinno, R.; Longrais, I.A.R.D.L.; Howarth, D.J.; Diamandis, E.P. Prognostic value of human kallikrein 10 expression in epithelial ovarian carcinoma. Clin. Cancer Res. 2001, 7, 2372–2379. [Google Scholar]
- Schummer, M.; Ng, W.V.; E Bumgarner, R.; Nelson, P.S.; Schummer, B.; Bednarski, D.W.; Hassell, L.; Baldwin, R.L.; Karlan, B.Y.; Hood, L. Comparative hybridization of an array of 21 500 ovarian cDNAs for the discovery of genes overexpressed in ovarian carcinomas. Gene 1999, 238, 375–385. [Google Scholar] [CrossRef]
- Lu, R.; Sun, X.; Xiao, R.; Zhou, L.; Gao, X.; Guo, L. Human epididymis protein 4 (HE4) plays a key role in ovarian cancer cell adhesion and motility. Biochem. Biophys. Res. Commun. 2012, 419, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Huhtinen, K.; Suvitie, P.; Hiissa, J.; Junnila, J.; Huvila, J.; Kujari, H.; Setala, M.; Härkki, P.; Jalkanen, J.; Fraser, J.K.; et al. Serum HE4 concentration differentiates malignant ovarian tumours from ovarian endometriotic cysts. Br. J. Cancer 2009, 100, 1315–1319. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.S.; Ferrara, N. Developmental and Pathological Angiogenesis. Annu. Rev. Cell Dev. Biol. 2011, 27, 563–584. [Google Scholar] [CrossRef] [PubMed]
- A Nagy, J.; Masse, E.M.; Herzberg, K.T.; Meyers, M.S.; Yeo, K.T.; Yeo, T.K.; Sioussat, T.M.; Dvorak, H.F. Pathogenesis of ascites tumor growth: Vascular permeability factor, vascular hyperpermeability, and ascites fluid accumulation. Cancer Res. 1995, 55, 360–368. [Google Scholar] [PubMed]
- Hartenbach, E.M.; A Olson, T.; Goswitz, J.J.; Mohanraj, D.; Twiggs, L.B.; Carson, L.F.; Ramakrishnan, S. Vascular endothelial growth factor (VEGF) expression and survival in human epithelial ovarian carcinomas. Cancer Lett. 1997, 121, 169–175. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Lheureux, S.; Moore, K.N. PARP Inhibitors for Ovarian Cancer: Current Indications, Future Combinations, and Novel Assets in Development to Target DNA Damage Repair. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, e116–e131. [Google Scholar] [CrossRef] [PubMed]
- Cramer, D.W.; Bast, R.C.; Berg, C.D.; Diamandis, E.P.; Godwin, A.K.; Hartge, P.; Lokshin, A.E.; Lu, K.H.; McIntosh, M.W.; Mor, G.; et al. Ovarian Cancer Biomarker Performance in Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial Specimens. Cancer Prev. Res. 2011, 4, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Chao, L.; Chao, J. Prostasin is a novel human serine proteinase from seminal fluid. Purification, tissue distribution, and localization in prostate gland. J. Biol. Chem. 1994, 269, 18843–18848. [Google Scholar] [CrossRef]
- Tamir, A.; Gangadharan, A.; Balwani, S.; Tanaka, T.; Patel, U.; Hassan, A.; Benke, S.; Agas, A.; D’Agostino, J.; Shin, D.; et al. The serine protease prostasin (PRSS8) is a potential biomarker for early detection of ovarian cancer. J. Ovarian Res. 2016, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Huddleston, H.G.; Wong, K.; Welch, W.R.; Berkowitz, R.S.; Mok, S.C. Clinical applications of microarray technology: Creatine kinase B is an up-regulated gene in epithelial ovarian cancer and shows promise as a serum marker. Gynecol. Oncol. 2005, 96, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Pastan, I. Molecular cloning of mesothelin, a differentiation antigen present on mesothelium, mesotheliomas, and ovarian cancers. Proc. Natl. Acad. Sci. USA 1996, 93, 136–140. [Google Scholar] [CrossRef]
- Hassan, R.; Thomas, A.; Alewine, C.; Le, D.T.; Jaffee, E.M.; Pastan, I. Mesothelin Immunotherapy for Cancer: Ready for Prime Time? J. Clin. Oncol. 2016, 34, 4171–4179. [Google Scholar] [CrossRef] [PubMed]
- Quanz, M.; Hagemann, U.B.; Zitzmann-Kolbe, S.; Stelte-Ludwig, B.; Golfier, S.; Elbi, C.; Mumberg, D.; Ziegelbauer, K.; Schatz, C.A. Anetumab ravtansine inhibits tumor growth and shows additive effect in combination with targeted agents and chemotherapy in mesothelin-expressing human ovarian cancer models. Oncotarget 2018, 9, 34103–34121. [Google Scholar] [CrossRef] [PubMed]
- Gadomska, H.; Grzechocińska, B.; Janecki, J.; Nowicka, G.; Powolny, M.; Marianowski, L. Serum lipids concentration in women with benign and malignant ovarian tumours. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 120, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Pal, M.K.; Rashid, M.; Bisht, M. Multiplexed magnetic nanoparticle-antibody conjugates (MNPs-ABS) based prognostic detection of ovarian cancer biomarkers, CA125, β-2M and ApoA1 using fluorescence spectroscopy with comparison of surface plasmon resonance (SPR) analysis. Biosens. Bioelectron. 2015, 73, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Kozak, K.R.; Su, F.; Whitelegge, J.P.; Faull, K.; Reddy, S.; Farias-Eisner, R. Characterization of serum biomarkers for detection of early stage ovarian cancer. Proteom. 2005, 5, 4589–4596. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-W.; Bee, S.M. Development of multiplexed bead-based immunoassays for the detection of early stage ovarian cancer using a combination of serum biomarkers. PLoS ONE 2012, 7, e44960. [Google Scholar] [CrossRef] [PubMed]
- Fassl, S.; Leisser, C.; Maier, S. Transferrin ensures survival of ovarian carcinoma cells when apoptosis is induced by TNF α, FasL, TRAIL, or Myc. Oncogene 2003, 22, 8343–8355. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Oliva, K.T.; Barker, G.; Hoffmann, P.; Reeve, S.; Smith, I.A.; Quinn, M.A.; Rice, G.E. Proteomic tracking of serum protein isoforms as screening biomarkers of ovarian cancer. Proteomics 2005, 5, 4625–4636. [Google Scholar] [CrossRef] [PubMed]
- Clarke, C.H.; Yip, C.; Badgwell, D.; Fung, E.T.; Coombes, K.R.; Zhang, Z.; Lu, K.H.; Bast, R.C. Proteomic biomarkers apolipoprotein A1, truncated transthyretin and connective tissue activating protein III enhance the sensitivity of CA125 for detecting early stage epithelial ovarian cancer. Gynecol. Oncol. 2011, 122, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Chen, S.; Li, L.; Liu, X.; Liu, X.; Dai, S.; Zhang, P.; Lu, H.; Lin, Z.; Yu, Y.; et al. Evaluation of HE4 and TTR for diagnosis of ovarian cancer: Comparison with CA125. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Su, F.; Lang, J.; Kumar, A.; Ng, C.; Hsieh, B.; Suchard, M.A.; Reddy, S.T.; Farias-Eisner, R. Validation of Candidate Serum Ovarian Cancer Biomarkers for Early Detection. Biomark. Insights 2007, 2, 369–375. [Google Scholar] [CrossRef]
- Suzuki, S.; Moore, D.H.; Ginzinger, D.G.; E Godfrey, T.; Barclay, J.; Powell, B.; Pinkel, D.; Zaloudek, C.; Lu, K.; Mills, G.; et al. An approach to analysis of large-scale correlations between genome changes and clinical endpoints in ovarian cancer. Cancer Res. 2000, 60, 5382–5385. [Google Scholar]
- Kiechle, M.; Jacobson, A. Comparative genomic hybridization detects genetic imbalances in primary ovarian carcinomas as correlated with grade of differentiation. Cancer 2001, 91, 534–540. [Google Scholar] [CrossRef]
- Schwartz, D.R.; Kardia, S.L.R.; A Shedden, K.; Kuick, R.; Michailidis, G.; Taylor, J.M.G.; Misek, D.E.; Wu, R.; Zhai, Y.; Darrah, D.M.; et al. Gene expression in ovarian cancer reflects both morphology and biological behavior, distinguishing clear cell from other poor-prognosis ovarian carcinomas. Cancer Res. 2002, 62, 4722–4729. [Google Scholar] [PubMed]
- Spentzos, D.; Levine, D.A.; Ramoni, M.F.; Joseph, M.; Gu, X.; Boyd, J.; Libermann, T.A.; Cannistra, S.A. Gene Expression Signature With Independent Prognostic Significance in Epithelial Ovarian Cancer. J. Clin. Oncol. 2004, 22, 4700–4710. [Google Scholar] [CrossRef] [PubMed]
- Garzon, R.; Fabbri, M.; Cimmino, A.; Calin, G.A.; Croce, C.M. MicroRNA expression and function in cancer. Trends Mol. Med. 2006, 12, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Petricoin, E.F.; Ardekani, A.M.; Hitt, B.A.; Levine, P.J.; Fusaro, V.A.; Steinberg, S.M.; Mills, G.B.; Simone, C.; Fishman, D.A.; Kohn, E.C.; et al. Use of Proteomic Patterns in Serum to Identify Ovarian Cancer. Obstet. Gynecol. Surv. 2002, 57, 352–353. [Google Scholar] [CrossRef]
- Gortzak-Uzan, L.; Ignatchenko, A.; Evangelou, A.I.; Agochiya, M.; Brown, K.A.; St.Onge, P.; Kireeva, I.; Schmitt-Ulms, G.; Brown, T.J.; Murphy, J.; et al. A Proteome Resource of Ovarian Cancer Ascites: Integrated Proteomic and Bioinformatic Analyses To Identify Putative Biomarkers. J. Proteome Res. 2008, 7, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Zowczak, M.; Iskra, M.; Torlinski, L.; Cofta, S. Analysis of Serum Copper and Zinc Concentrations in Cancer Patients. Biol. Trace Element Res. 2001, 82, 1–8. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, Z.; Li, A.; Zhang, Y. Association between serum zinc levels and lung cancer: A meta-analysis of observational studies. World J. Surg. Oncol. 2019, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Baxter, E.; Caddick, M.; Dragovic, B. Garnet: A Rock-Forming Mineral Petrochronometer. Rev. Miner. Geochem. 2017, 83, 469–533. [Google Scholar] [CrossRef]
- Jalalian, S.H.; Ramezani, M.; Abnous, K.; Taghdisi, S.M. Exosomes, new biomarkers in early cancer detection. Anal. Biochem. 2019, 571, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Zhan, X. Identification of clinical trait–related lncRNA and mRNA biomarkers with weighted gene co-expression network analysis as useful tool for personalized medicine in ovarian cancer. EPMA J. 2019, 10, 273–290. [Google Scholar] [CrossRef]
- Steffensen, K.D.; Alvero, A.B.; Yang, Y.; Waldstrøm, M.; Hui, P.; Holmberg, J.C.; Silasi, D.-A.; Jakobsen, A.; Rutherford, T.; Mor, G. Prevalence of Epithelial Ovarian Cancer Stem Cells Correlates with Recurrence in Early-Stage Ovarian Cancer. J. Oncol. 2011, 2011, 1–12. [Google Scholar] [CrossRef]
- Townsend, D.M.; Tew, K.D.; Tapiero, H. The importance of glutathione in human disease. Biomed. Pharmacother. 2003, 57, 145–155. [Google Scholar] [CrossRef]
- Olivares, M.; Uauy, R. Limits of metabolic tolerance to copper and biological basis for present recommendations and regulations. Am. J. Clin. Nutr. 1996, 63, 846S–852S. [Google Scholar] [CrossRef]
- Toubhans, B.; Gourlan, A.; Telouk, P.; Lutchman-Singh, K.; Francis, L.; Conlan, R.; Margarit, L.; Gonzalez, D.; Charlet, L. Cu isotope ratios are meaningful in ovarian cancer diagnosis. J. Trace Elements Med. Biol. 2020, 62, 126611. [Google Scholar] [CrossRef]
- Zhang, X.; Yuan, X.; Shi, H.; Wu, L.; Qian, H.; Xu, W. Exosomes in cancer: Small particle, big player. J. Hematol. Oncol. 2015, 8, 1–13. [Google Scholar] [CrossRef]
- Greening, D.W.; Gopal, S.K.; Xu, R.; Simpson, R.J.; Chen, W. Exosomes and their roles in immune regulation and cancer. Semin. Cell Dev. Biol. 2015, 40, 72–81. [Google Scholar] [CrossRef]
- Mathivanan, S.; Ji, H.; Simpson, R.J. Exosomes: Extracellular organelles important in intercellular communication. J. Proteom. 2010, 73, 1907–1920. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.-K.; Zhang, H.; Liu, P.; Tsao, S.-W.; Lung, M.L.; Mak, N.-K.; Wong, R.N.-S.; Yue, P.Y.-K.; Tsao, G.S.-W. Proteomic analysis of exosomes from nasopharyngeal carcinoma cell identifies intercellular transfer of angiogenic proteins. Int. J. Cancer 2015, 137, 1830–1841. [Google Scholar] [CrossRef] [PubMed]
- del Conde, I.; Shrimpton, C.N. Tissue-factor–bearing microvesicles arise from lipid rafts and fuse with activated platelets to initiate coagulation. Blood 2005, 106, 1604–1611. [Google Scholar] [CrossRef]
- Théry, C. Exosomes: Secreted vesicles and intercellular communications. F1000 Biol. Rep. 2011, 3, 15. [Google Scholar] [CrossRef] [PubMed]
- Azmi, A.S.; Bao, B.; Sarkar, F.H. Exosomes in cancer development, metastasis, and drug resistance: A comprehensive review. Cancer Metastasis Rev. 2013, 32, 623–642. [Google Scholar] [CrossRef] [PubMed]
- Paggetti, J.; Haderk, F.; Seiffert, M.; Janji, B.; Distler, U.; Ammerlaan, W.; Kim, Y.J.; Adam, J.; Lichter, P.; Solary, E.; et al. Exosomes released by chronic lymphocytic leukemia cells induce the transition of stromal cells into cancer-associated fibroblasts. Blood 2015, 126, 1106–1117. [Google Scholar] [CrossRef]
- Went, P.T.; Lugli, A.; Meier, S.; Bundi, M.; Mirlacher, M.; Sauter, G.; Dirnhofer, S. Frequent EpCam protein expression in human carcinomas. Hum. Pathol. 2004, 35, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Golubnitschaja, O.; Baban, B.; Boniolo, G.; Wang, W.; Bubnov, R.; Kapalla, M.; Krapfenbauer, K.; Mozaffari, M.S.; Costigliola, V. Medicine in the early twenty-first century: Paradigm and anticipation-EPMA position paper 2016. EPMA J. 2016, 7, 1–13. [Google Scholar] [CrossRef]
- Janssens, J.P.; Schuster, K.; Voss, A. Preventive, predictive, and personalized medicine for effective and affordable cancer care. EPMA J. 2018, 9, 113–123. [Google Scholar] [CrossRef]
- Wang, H.; Fu, Z.; Dai, C.; Cao, J.; Liu, X.; Xu, J.; Lv, M.; Gu, Y.; Zhang, Y.G.J.; Hua, X.; et al. LncRNAs expression profiling in normal ovary, benign ovarian cyst and malignant epithelial ovarian cancer. Sci. Rep. 2016, 6, 38983. [Google Scholar] [CrossRef]
- Anaya, J. OncoLnc: Linking TCGA survival data to mRNAs, miRNAs, and lncRNAs. PeerJ Comput. Sci. 2016, 2, e67. [Google Scholar] [CrossRef]
- Chang, M.-C.; Chen, C.-A. Mesothelin enhances invasion of ovarian cancer by inducing MMP-7 through MAPK/ERK and JNK pathways. Biochem. J. 2012, 442, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Li, X.; Holm, R.; Trope, C.G.; Nesland, J.M.; Suo, Z. The expression of aldehyde dehydrogenase 1 (ALDH1) in ovarian carcinomas and its clinicopathological associations: A retrospective study. BMC Cancer 2015, 15, 502. [Google Scholar] [CrossRef] [PubMed]
- Dainty, L.A.; Risinger, J.I.; Morrison, C.; Chandramouli, G.; Bidus, M.A.; Zahn, C.; Rose, G.S.; Fowler, J.; Berchuck, A.; Maxwell, G.L. Overexpression of folate binding protein and mesothelin are associated with uterine serous carcinoma. Gynecol. Oncol. 2007, 105, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Kelemen, L.E. The role of folate receptor α in cancer development, progression and treatment: Cause, consequence or innocent bystander? Int. J. Cancer 2006, 119, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Rahilly, M.; Carder, P.J.; Al Nafussi, A.; Harrison, D.J. Distribution of glutathione S-transferase isoenzymes in human ovary. Reproduction 1991, 93, 303–311. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Coughlin, S.S.; Hall, I.J. Glutathione S-transferase polymorphisms and risk of ovarian cancer: A HuGE review. Genet. Med. 2002, 4, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Beeghly, A.; Katsaros, D.; Chen, H.; Fracchioli, S.; Zhang, Y.; Massobrio, M.; Risch, H.; Jones, B.; Yu, H. Glutathione S-transferase polymorphisms and ovarian cancer treatment and survival. Gynecol. Oncol. 2006, 100, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Xu, J.; Deng, S.; Zhou, F.; Li, J. Core signaling pathways in ovarian cancer stem cell revealed by integrative analysis of multi-marker genomics data. PLoS ONE 2018, 13, e0196351. [Google Scholar] [CrossRef]
- Häusler, S.F.M.; Keller, A.; A Chandran, P.; Ziegler, K.; Zipp, K.; Heuer, S.; Krockenberger, M.; Engel, J.B.; Hönig, A.; Scheffler, M.; et al. Whole blood-derived miRNA profiles as potential new tools for ovarian cancer screening. Br. J. Cancer 2010, 103, 693–700. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Biomarker | Source | Clinical Role | Clinical Utility | Reference | ||
|---|---|---|---|---|---|---|
| Diagnosis | Prognosis | Cancer Therapy | ||||
| Carbohydrate Antigen 125 (CA125) | Serum | ✓ | ✓ | Screen for ovarian cancer; evaluate the chemotherapy response and monitor disease recurrence using ELISA. | [12,13,14,15] | |
| Osteopontin (OPN) | Plasma | ✓ | ✓ | Diagnosis of ovarian cancer and prognostic indicator of metastasis using PCR and ELISA. | [16,17] | |
| Kallikreins (KLKs) | Serum | ✓ | Diagnosis of ovarian cancer using ELISA. | [17,18,19,20,21] | ||
| Bikunin | Serum | ✓ | Predict the stage of the disease and the survival rate preoperatively using ELISA or immunoblot assay. | [22,23,24,25] | ||
| Human Epididymis Protein 4 (HE4) | Serum | ✓ | High-sensitivity diagnostic tool for detecting stage I ovarian cancer using ELISA. | [26,27,28] | ||
| Vascular Endothelial Growth Factor (VEGF) | Serum | ✓ | ✓ | ✓ | Indicator of a shorter survival time in patients with ovarian cancers using ELISA. | [29,30,31,32] |
| Prostasin (PSN) | Serum | ✓ | Identify patients with ovarian cancer through RT-PCR. | [33,34] | ||
| Creatine Kinase B (CKB) | Serum | ✓ | Predict survival rate and prognosis of ovarian cancer using microarray technology. | [35] | ||
| Mesothelin | Serum | ✓ | Detected using ELISA method and used clinically as an antimesothelin immunotoxin therapy to attack cancer cells in combination with standard chemotherapy. | [36,37,38] | ||
| Apolipoprotein A-I (apoA-I) | Plasma | ✓ | Detected clinically using ELISA method to confirm diagnosis with ovarian cancer. | [39,40,41,42] | ||
| Transthyretin (TTR) | Serum | ✓ | Diagnosis of early stage ovarian cancer patients using matrix-assisted laser desorption-ionisation (MALDI). | [43] | ||
| Transferrin | Serum | ✓ | Used in combination with CA125 as an improved and sensitive ovarian cancer detection method estimated by measurements of the serum total iron-binding capacity (TIBC). | [44,45] | ||
| Emerging Biomarkers | Source | Potential Clinical Role | Reference |
|---|---|---|---|
| Cu isotope | Serum | Early diagnostic tool | [46] |
| Exosomes | Ascites | Cancer progression | [47] |
| lncRNA and mRNA | Tumour tissue | Early diagnostic tool and cancer therapy | [48] |
| Aldehyde Dehydrogenase 1 (ALDH1) | Blood/Cytosol | Early diagnostic and cancer progression | [49] |
| Folate Receptor Alpha (FOLR1) | Blood/Gene | Progression and cancer therapy | [50] |
| Glutathione S-Transferase Polymorphisms (GSTP) | Blood/DNA | Anticancer drug response | [51] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atallah, G.A.; Abd. Aziz, N.H.; Teik, C.K.; Shafiee, M.N.; Kampan, N.C. New Predictive Biomarkers for Ovarian Cancer. Diagnostics 2021, 11, 465. https://doi.org/10.3390/diagnostics11030465
Atallah GA, Abd. Aziz NH, Teik CK, Shafiee MN, Kampan NC. New Predictive Biomarkers for Ovarian Cancer. Diagnostics. 2021; 11(3):465. https://doi.org/10.3390/diagnostics11030465
Chicago/Turabian StyleAtallah, Ghofraan Abdulsalam, Nor Haslinda Abd. Aziz, Chew Kah Teik, Mohamad Nasir Shafiee, and Nirmala Chandralega Kampan. 2021. "New Predictive Biomarkers for Ovarian Cancer" Diagnostics 11, no. 3: 465. https://doi.org/10.3390/diagnostics11030465
APA StyleAtallah, G. A., Abd. Aziz, N. H., Teik, C. K., Shafiee, M. N., & Kampan, N. C. (2021). New Predictive Biomarkers for Ovarian Cancer. Diagnostics, 11(3), 465. https://doi.org/10.3390/diagnostics11030465