
Unfavorable Changes of Platelet Reactivity on Clopidogrel Therapy Assessed by Impedance Aggregometry Affect a Larger Volume of Acute Ischemic Lesions in Stroke

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Platelet Reactivity Testing
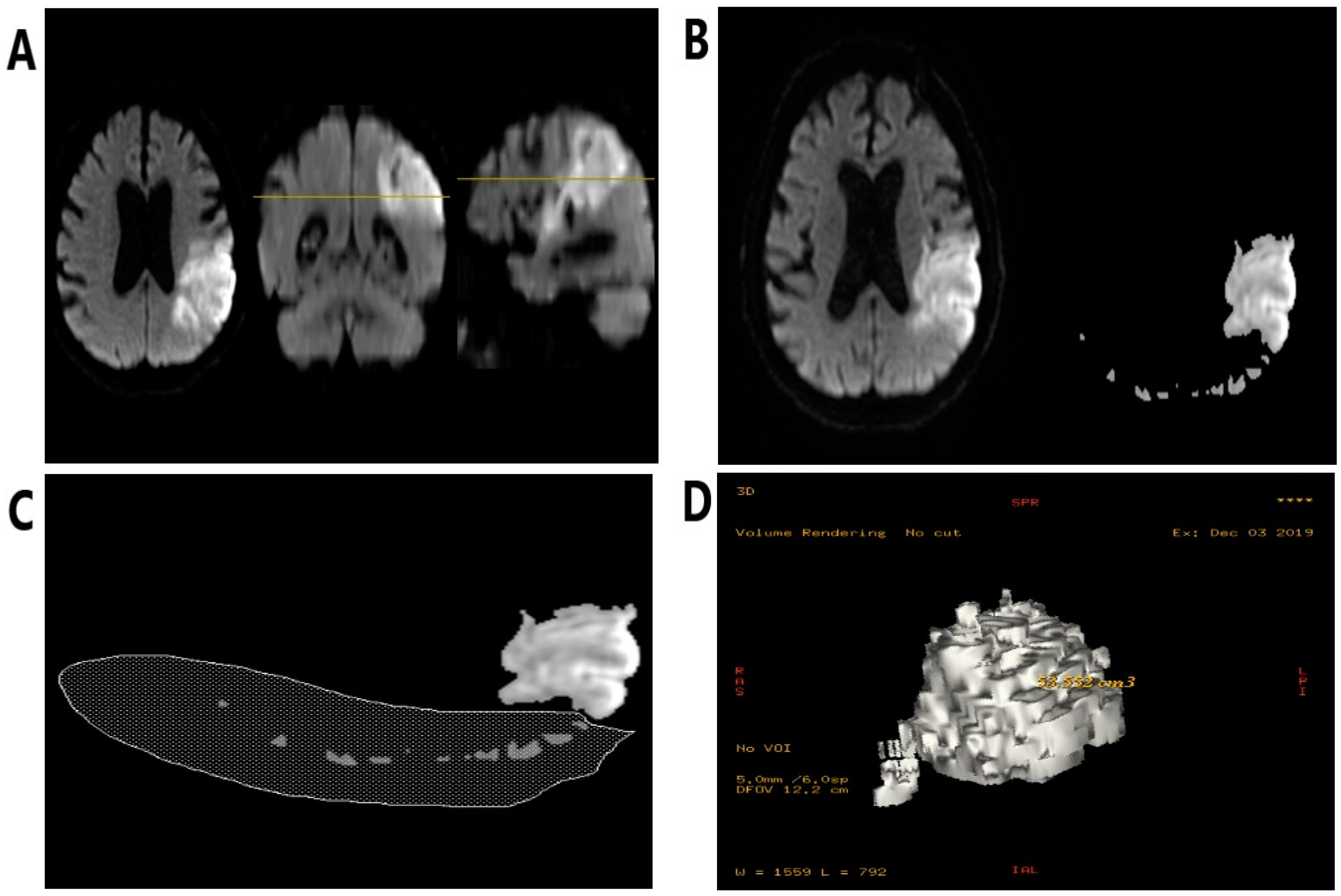
2.3. The Volumetric Evaluation
2.4. Ethical Statement
2.5. Statistical Evaluation Methods
2.6. Definitions of Clopidogrel Resistance
3. Results
3.1. Overall Results
3.2. Platelet Reactivity and Chronic Ischemic Lesions
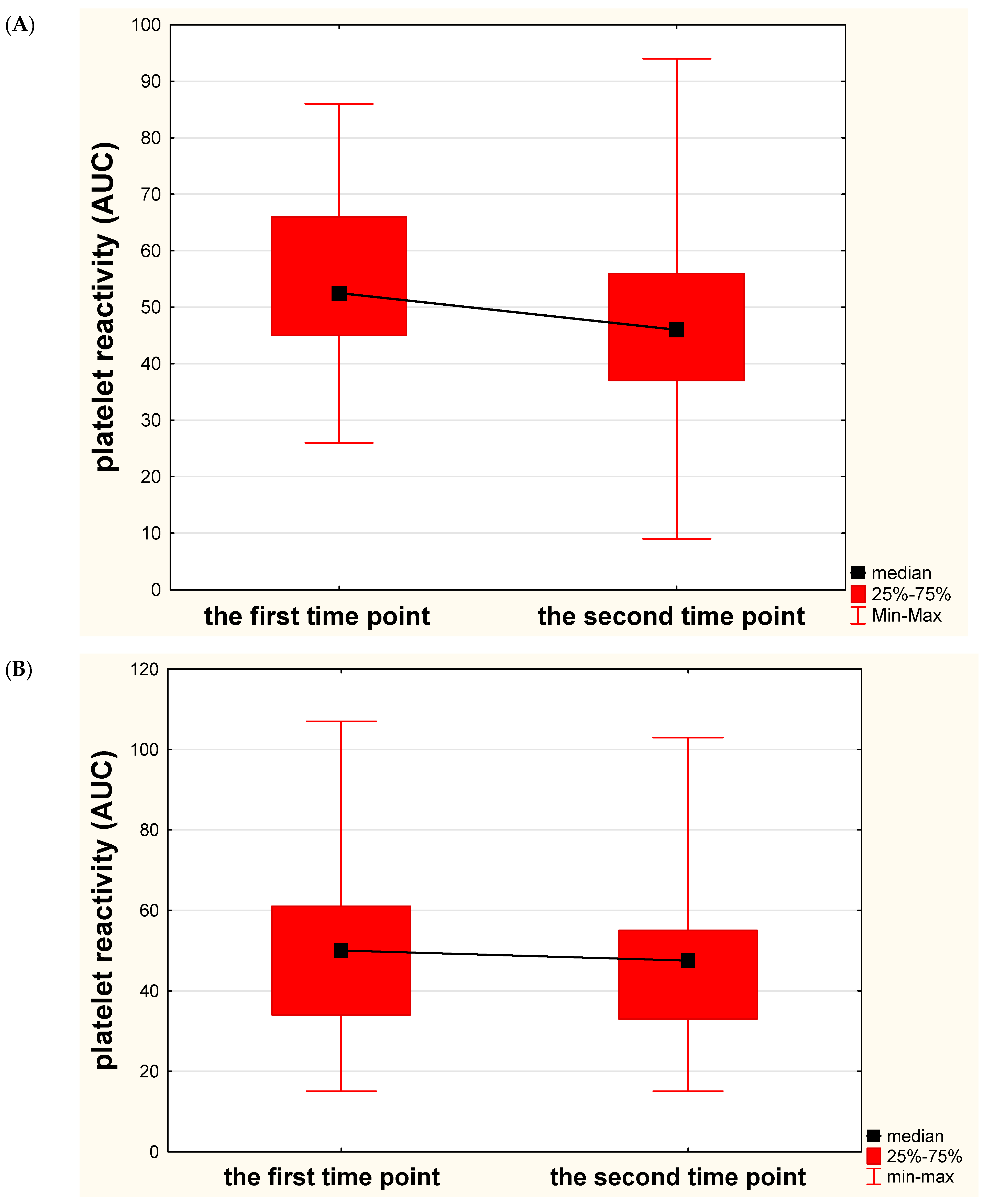
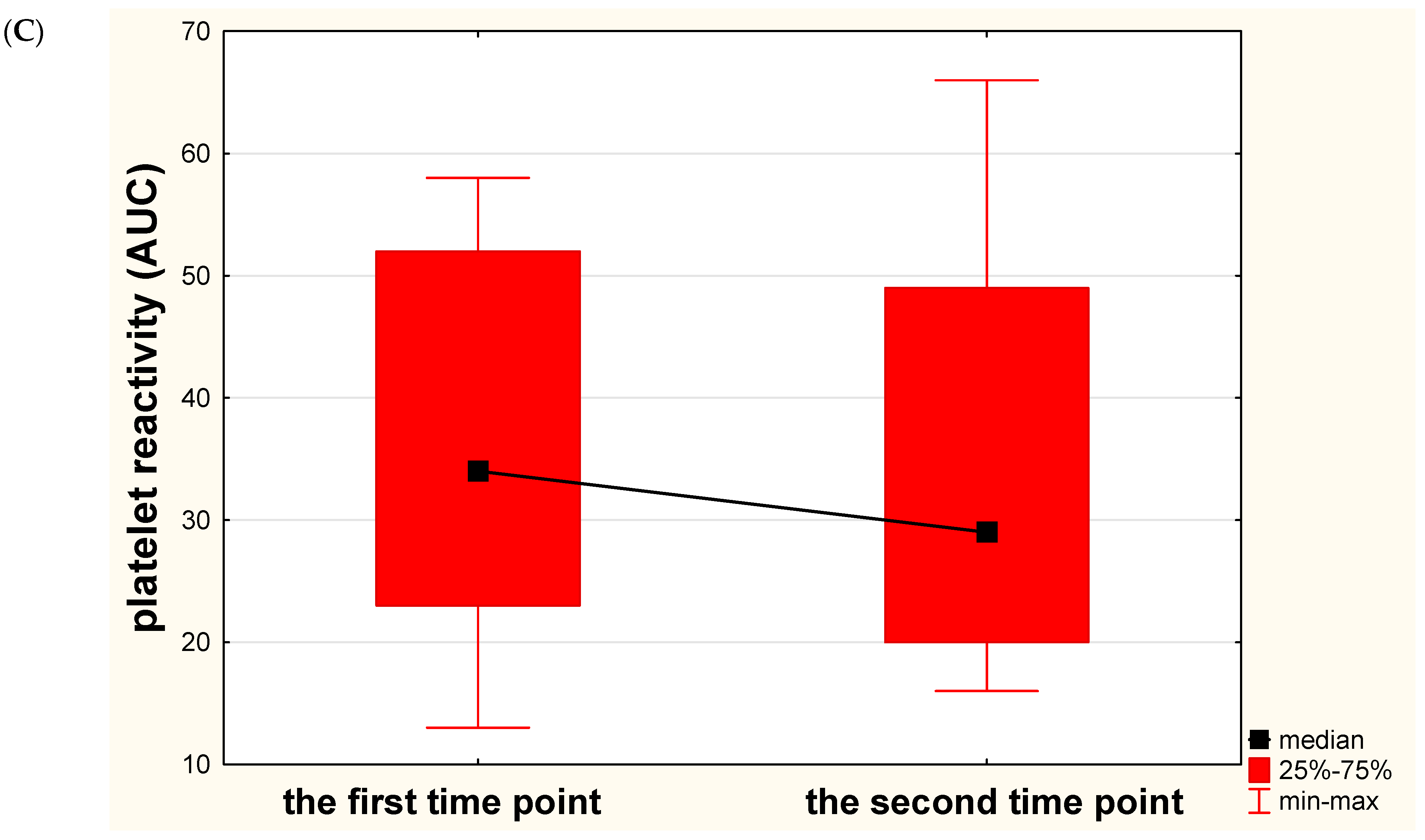
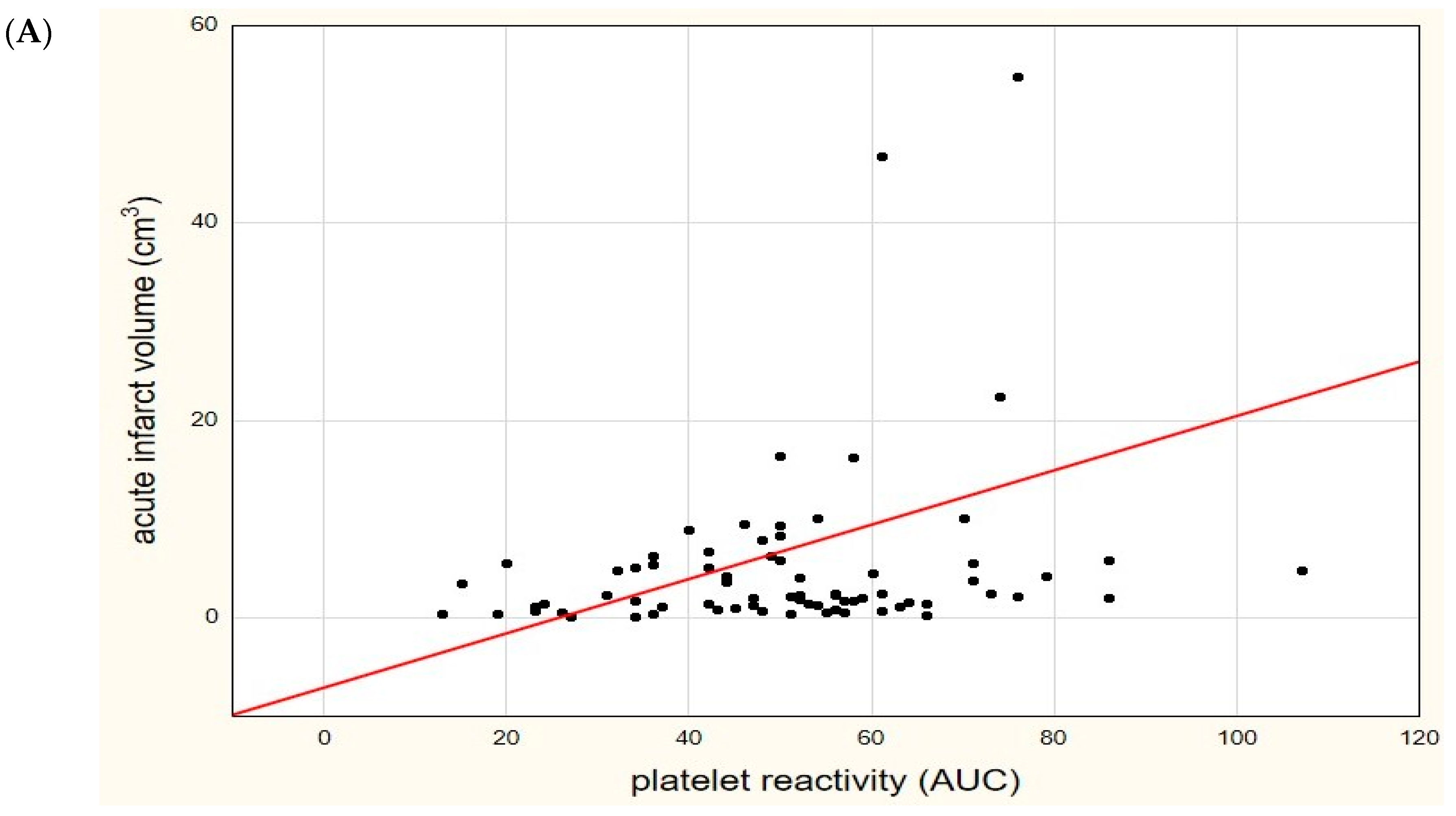
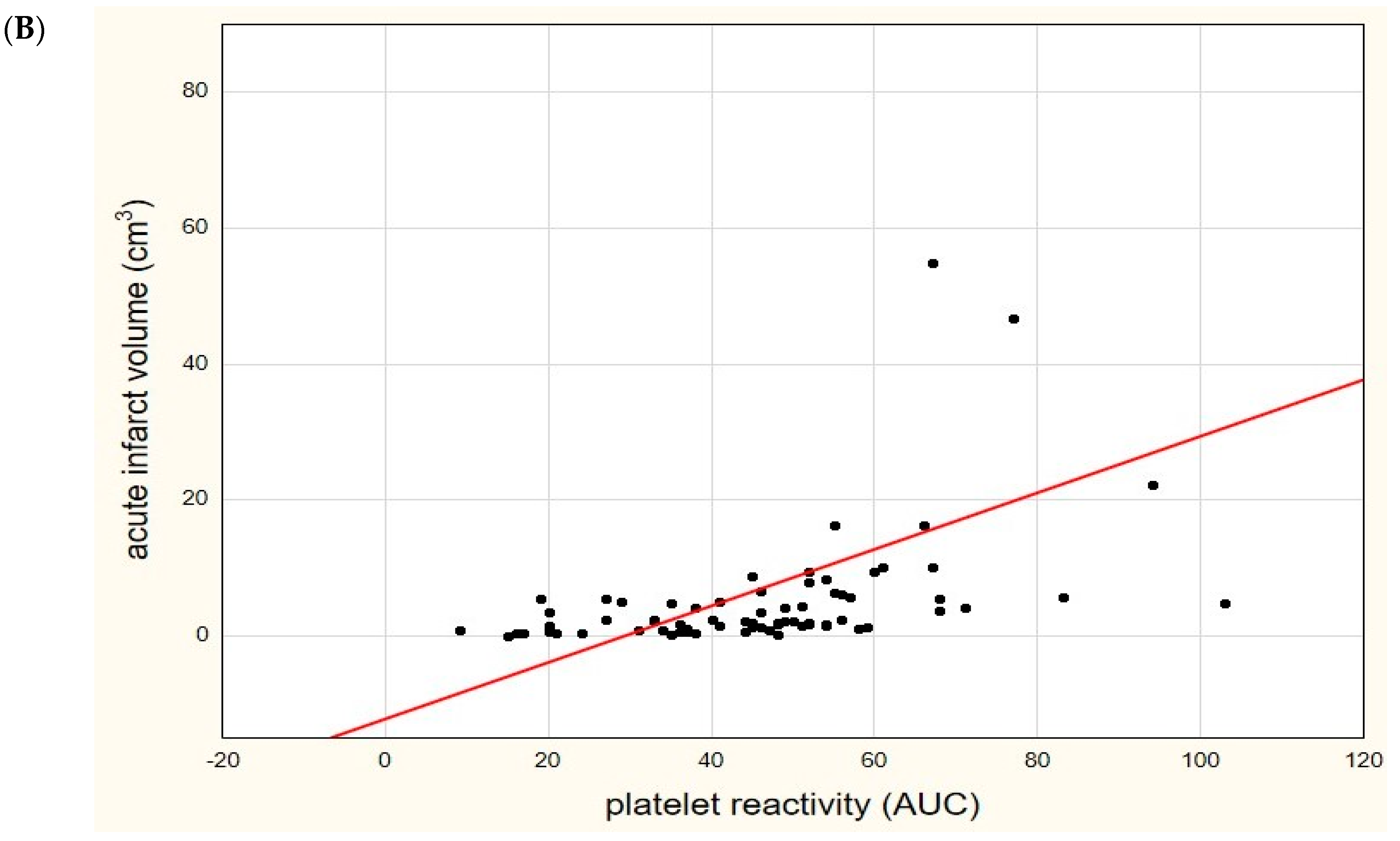
3.3. Platelet Reactivity and Acute Ischemic Lesions
3.4. Logistic Regression Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e99. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, Y.; Zhao, X.; Liu, L.; Wang, D.; Wang, C.; Wang, C.; Li, H.; Meng, X.; Cui, L.; et al. Clopidogrel with Aspirin in Acute Minor Stroke or Transient Ischemic Attack. N. Engl. J. Med. 2013, 369, 11–19. [Google Scholar] [CrossRef]
- Wang, Y.; Pan, Y.; Zhao, X.; Li, H.; Wang, D.; Johnston, S.C.; Liu, L.; Meng, X.; Wang, A.; Wang, C.; et al. CHANCE Investigators. Clopidogrel With Aspirin in Acute Minor Stroke or Transient Ischemic Attack (CHANCE) trial: One-year outcomes. Circulation 2015, 132, 40–46. [Google Scholar] [PubMed]
- Johnston, S.C.; Easton, J.D.; Farrant, M.; Barsan, W.; Conwit, R.A.; Elm, J.J.; Kim, A.S.; Lindblad, A.S.; Palesch, Y.Y. Point Ivestigators. Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA. J. Engl. J. Med. 2018, 379, 215–225. [Google Scholar] [CrossRef]
- Gent, M.; Beaumont, D.; Blanchard, J.; Bousser, M.G.; Coffman, J.; Easton, J.D.; Hampton, J.R.; Harker, L.A.; Janzon, L.; Kusmierek, J.J.; et al. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 1996, 348, 1329–1339. [Google Scholar]
- Wiśniewski, A.; Filipska, K. The Phenomenon of Clopidogrel High On-Treatment Platelet Reactivity in Ischemic Stroke Subjects: A Comprehensive Review. Int. J. Mol. Sci. 2020, 21, 6408. [Google Scholar] [CrossRef]
- Qiu, L.-N.; Wang, L.; Li, X.; Han, R.-F.; Xia, X.-S.; Liu, J. Predictive Value of High Residual Platelet Reactivity by Flow Cy-tometry for Outcomes of Ischemic Stroke Patients on Clopidogrel Therapy. J. Stroke Cerebrovasc. Dis. 2015, 24, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Yi, X.; Lin, J.; Wang, Y.; Zhou, J.; Zhou, Q.; Wang, C. Response to clopidogrel is associated with early neurological deterioration after acute ischemic stroke. Oncotarget 2018, 9, 19900–19910. [Google Scholar] [CrossRef][Green Version]
- Lee, J.; Gwon, J.; Kim, M. Abstract WMP39: Clopidogrel Resistance Predicts Early Neurological Worsening In Patients With Acute Large Artery Atherosclerotic Stroke. Stroke 2018, 49, 39. [Google Scholar] [CrossRef]
- Yi, X.; Lin, J.; Zhou, Q.; Wu, L.; Cheng, W.; Wang, C. Clopidogrel Resistance Increases Rate of Recurrent Stroke and Other Vascular Events in Chinese Population. J. Stroke Cerebrovasc. Dis. 2016, 25, 1222–1228. [Google Scholar] [CrossRef]
- Jeon, S.M. Clopidogrel Resistance in Acute Ischemic Stroke. J. Korean Neurol. Assoc. 2006, 24, 318–322. [Google Scholar]
- Wiśniewski, A.; Sikora, J.; Sławińska, A.; Filipska, K.; Karczmarska-Wódzka, A.; Serafin, Z.; Kozera, G. High On-Treatment Platelet Reactivity Affects the Extent of Ischemic Lesions in Stroke Patients Due to Large-Vessel Disease. J. Clin. Med. 2020, 9, 251. [Google Scholar] [CrossRef]
- Hvas, A.-M.; Grove, E.L. Platelet Function Tests: Preanalytical Variables, Clinical Utility, Advantages, and Disadvantages. Methods Mol. Biol. 2017, 1646, 305–320. [Google Scholar] [CrossRef]
- Kim, J.-T.; Heo, S.-H.; Choi, K.-H.; Nam, T.-S.; Choi, S.-M.; Lee, S.-H.; Park, M.-S.; Kim, B.C.; Kim, M.-K.; Saver, J.L.; et al. Clinical Implications of Changes in Individual Platelet Reactivity to Aspirin Over Time in Acute Ischemic Stroke. Stroke 2015, 46, 2534–2540. [Google Scholar] [CrossRef] [PubMed]
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef]
- Bonello, L.; Tantry, U.S.; Marcucci, R.; Blindt, R.; Angiolillo, D.J.; Becker, R.; Bhatt, D.L.; Cattaneo, M.; Collet, J.P.; Cuisset, T.; et al. Consensus and Future Directions on the Definition of High On-Treatment Platelet Reactivity to Adenosine Diphosphate. J. Am. Coll. Cardiol. 2010, 56, 919–933. [Google Scholar] [CrossRef]
- Sibbing, D.; Braun, S.; Morath, T.; Mehilli, J.; Vogt, W.; Schömig, A.; Kastrati, A.; Von Beckerath, N. Platelet Reactivity After Clopidogrel Treatment Assessed With Point-of-Care Analysis and Early Drug-Eluting Stent Thrombosis. J. Am. Coll. Cardiol. 2009, 53, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Jawansky, S.; Vogt, W.; Mehilli, J.; Schömig, A.; Kastrati, A.; Von Beckerath, N.; Sibbing, D. Assessment of ADP-induced platelet aggregation with light transmission aggregometry and multiple electrode platelet aggregometry before and after clopidogrel treatment. Thromb. Haemost. 2008, 99, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.S.; Roberts, N. Measurement of brain volume using MRI: Software, techniques, choices and prerequisites. J. Anthr. Sci. Riv. di Antropol. 2009, 87, 127–151. [Google Scholar]
- Wahlund, L.O.; Barkhof, F.; Fazekas, F.; Bronge, L.; Augustin, M.; Sjögren, M.; Wallin, A.; Ader, H.; Leys, D.; Pantoni, L.; et al. A New Rating Scale for Age-Related White Matter Changes Applicable to MRI and CT. Stroke 2001, 32, 1318–1322. [Google Scholar] [CrossRef]
- Oh, M.S.; Yu, K.-H.; Lee, J.-H.; Jung, S.; Kim, C.; Jang, M.U. Aspirin resistance is associated with increased stroke severity and infarct volume. Neurol. 2016, 86, 1808–1817. [Google Scholar] [CrossRef]
- Cheng, X.; Xie, N.-C.; Xu, H.-L.; Chen, C.; Lian, Y.-J. Biochemical aspirin resistance is associated with increased stroke severity and infarct volumes in ischemic stroke patients. Oncotarget 2017, 8, 77086–77095. [Google Scholar] [CrossRef] [PubMed]
- Agayeva, N.; Topcuoglu, M.A.; Arsava, E.M. The Interplay between Stroke Severity, Antiplatelet Use, and Aspirin Resistance in Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2016, 25, 397–403. [Google Scholar] [CrossRef] [PubMed]
- El-Mitwalli, A.; Azzam, H.; Abu-Hegazy, M.; Gomaa, M.; Wasel, Y. Clinical and biochemical aspirin resistance in patients with recurrent cerebral ischemia. Clin. Neurol. Neurosurg. 2013, 115, 944–947. [Google Scholar] [CrossRef] [PubMed]
- Lundstroem, A.; Wallen, H.; von Arbin, M.; Joerneskog, G.; Gigante, B.; Dembrower, H.K.; Laurencikas, E.; Laska, A.C. Clopidogrel Resistance after Minor Ischemic Stroke or Transient Ischemic Attack is Associated with Radiological Cerebral Small-Vessel Disease. J. Stroke Cerebrovasc. Dis. 2015, 24, 2348–2357. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Values |
|---|---|
| Age | 67.5 (18–91) |
| Sex: | |
| Male | 36 (48.6%) |
| Female | 38 (51.4%) |
| Hypertension | 53 (71.6%) |
| Diabetes | 19 (25.7%) |
| Hyperlipidemia | 24 (32.4%) |
| Smoking | 22 (29.7%) |
| Obesity | 22 (29.7%) |
| Alcohol abuse | 6 (8.1%) |
| CRP (mg/L) | 2.37 (0.21–148.96) |
| HbA1c (%) | 5.8 (4.9–13.01) |
| D-Dimer (mg/mL) | 451 (165–5926) |
| Fibrinogen (mg/dL) | 335 (212–658) |
| Platelet count (thousands/µL) | 256 (112–545) |
| NIHSS on admission | 3 (1–16) |
| mRS on admission | 2 (0–5) |
| The volume of ischemic focus DWI (cm3) | 2.3 (0.09–136.9) |
| The volume of ischemic focus FLAIR (cm3) | 2.5 (0.13–143.3) |
| Resistance to clopidogrel | 47 (63.5%) |
| Etiology of stroke: | |
| Large vessel disease | 18 (24.3%) |
| Small vessel disease | 56 (75.4%) |
| Definition1 | Definition 2 | Definition 3 | |
|---|---|---|---|
| OR (95%CI) p | OR (95%CI) p | OR (95%CI) p | |
| Infarct volume (vs insignificant) Mild | 1.20 (0.44, 3.26) 0.724 | 6.5 (0.88, 47.9) 0.066 | 6.89 (0.78, 60.88) 0.083 |
| Moderate | 2.74 (0.27, 27.4) 0.391 | 3.19 (1.04, 9.84) 0.043 * | 46.5 (3.2, 676.21) 0.005 * |
| Large | 6.23 (0.30, 125.5) 0.234 | 13.0 (1.14, 147.8) 0.039 * | 93.0 (4.56, 1895.27) 0.003 * |
| Model 1 (Definition 2) | Model 2 (Definition 3) | |||
|---|---|---|---|---|
| Adjusted OR (95% CI) | p | Adjusted OR (95% CI) | p | |
| Age | 1.06 (0.99, 1.13) | 0.076 | 1.07 (0.99, 1.14) | 0.05 |
| Clopidogrel resistance | 7.16 (1.69, 30.31) | 0.008 * | 26.49 (1.88, 372.44) | 0.015 * |
| Sex (male) | 0.45 (0.12, 1.7) | 0.241 | 0.57 (0.16, 2.09) | 0.398 |
| Diabetes | 1.01 (0.23, 4.51) | 0.985 | 1.94 (0.41, 9.09) | 0.402 |
| Large vessel disease | 23.99 (2.39, 241.4) | 0.007 * | 28.46 (2.74, 295.47) | 0.005 * |
| Smoking | 0.23 (0.05, 0.99) | 0.054 | 0.25 (0.06, 1.05) | 0.059 |
| Hyperlipidemia | 1.41 (0.36, 5.51) | 0.623 | 0.99 (0.24, 4.03) | 0.988 |
| Hypertension | 0.97 (0.12, 4.84) | 0.966 | 1.35 (0.27, 6.8) | 0.715 |
| Obesity | 0.36 (0.07, 1.69) | 0.193 | 0.31 (0.06, 1.52) | 0.149 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiśniewski, A.; Sikora, J.; Karczmarska-Wódzka, A.; Sobczak, P.; Lemanowicz, A.; Zawada, E.; Masiliūnas, R.; Jatužis, D. Unfavorable Changes of Platelet Reactivity on Clopidogrel Therapy Assessed by Impedance Aggregometry Affect a Larger Volume of Acute Ischemic Lesions in Stroke. Diagnostics 2021, 11, 405. https://doi.org/10.3390/diagnostics11030405
Wiśniewski A, Sikora J, Karczmarska-Wódzka A, Sobczak P, Lemanowicz A, Zawada E, Masiliūnas R, Jatužis D. Unfavorable Changes of Platelet Reactivity on Clopidogrel Therapy Assessed by Impedance Aggregometry Affect a Larger Volume of Acute Ischemic Lesions in Stroke. Diagnostics. 2021; 11(3):405. https://doi.org/10.3390/diagnostics11030405
Chicago/Turabian StyleWiśniewski, Adam, Joanna Sikora, Aleksandra Karczmarska-Wódzka, Przemysław Sobczak, Adam Lemanowicz, Elżbieta Zawada, Rytis Masiliūnas, and Dalius Jatužis. 2021. "Unfavorable Changes of Platelet Reactivity on Clopidogrel Therapy Assessed by Impedance Aggregometry Affect a Larger Volume of Acute Ischemic Lesions in Stroke" Diagnostics 11, no. 3: 405. https://doi.org/10.3390/diagnostics11030405
APA StyleWiśniewski, A., Sikora, J., Karczmarska-Wódzka, A., Sobczak, P., Lemanowicz, A., Zawada, E., Masiliūnas, R., & Jatužis, D. (2021). Unfavorable Changes of Platelet Reactivity on Clopidogrel Therapy Assessed by Impedance Aggregometry Affect a Larger Volume of Acute Ischemic Lesions in Stroke. Diagnostics, 11(3), 405. https://doi.org/10.3390/diagnostics11030405