
Interreader Reliability of Liver Imaging Reporting and Data System Treatment Response: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
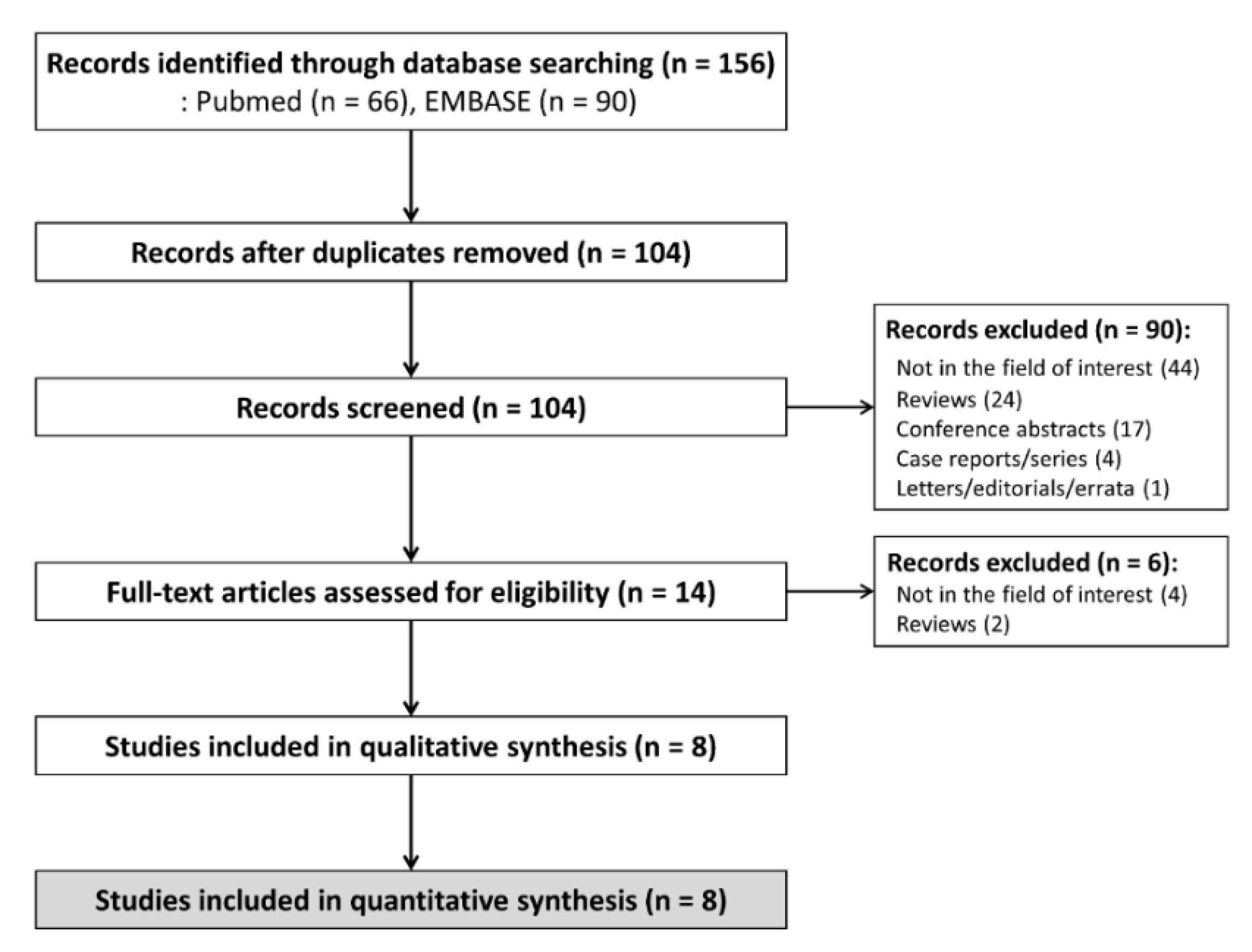
3.1. Literature Search
3.2. Study Characteristics
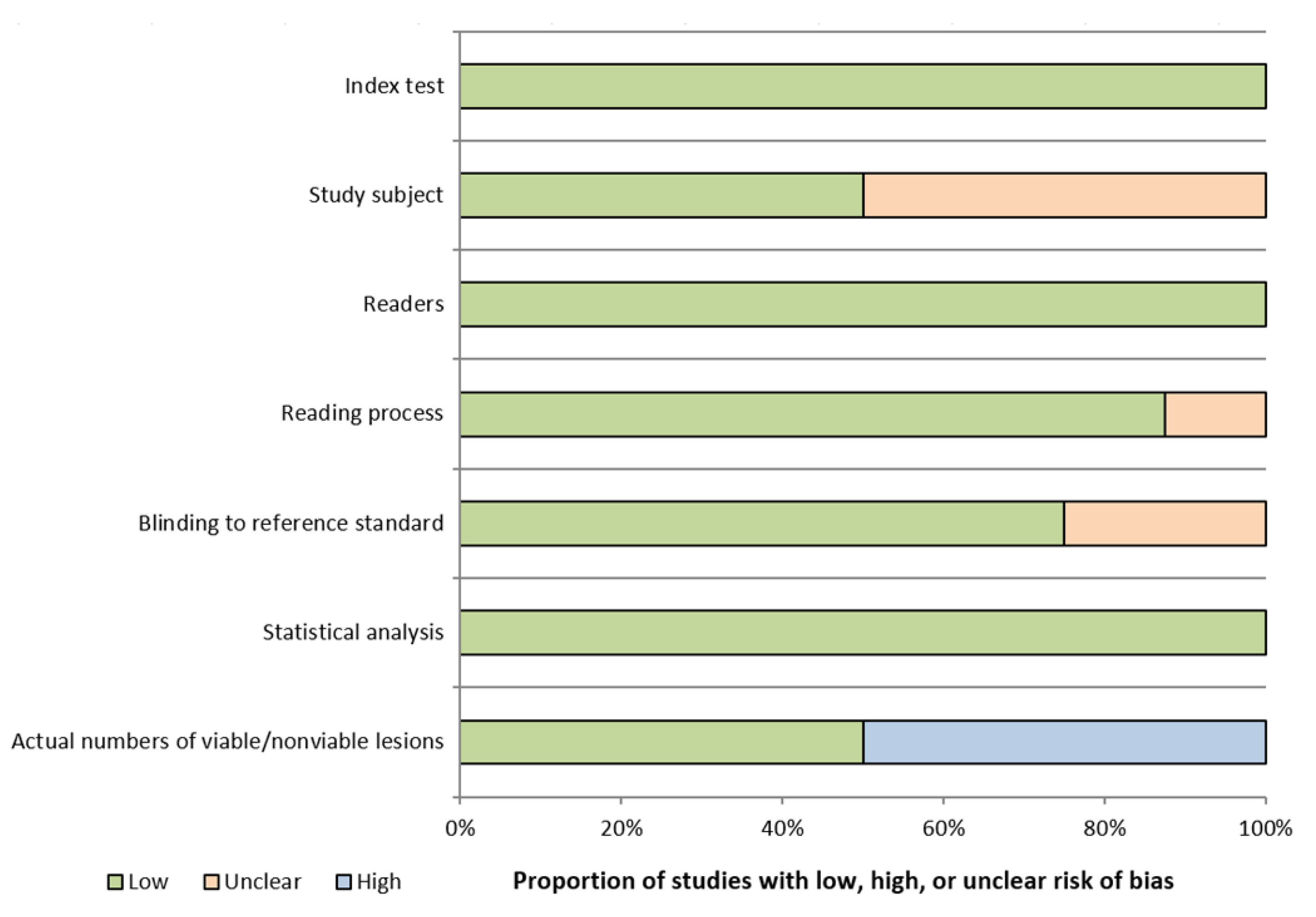
3.3. Quality Assessments
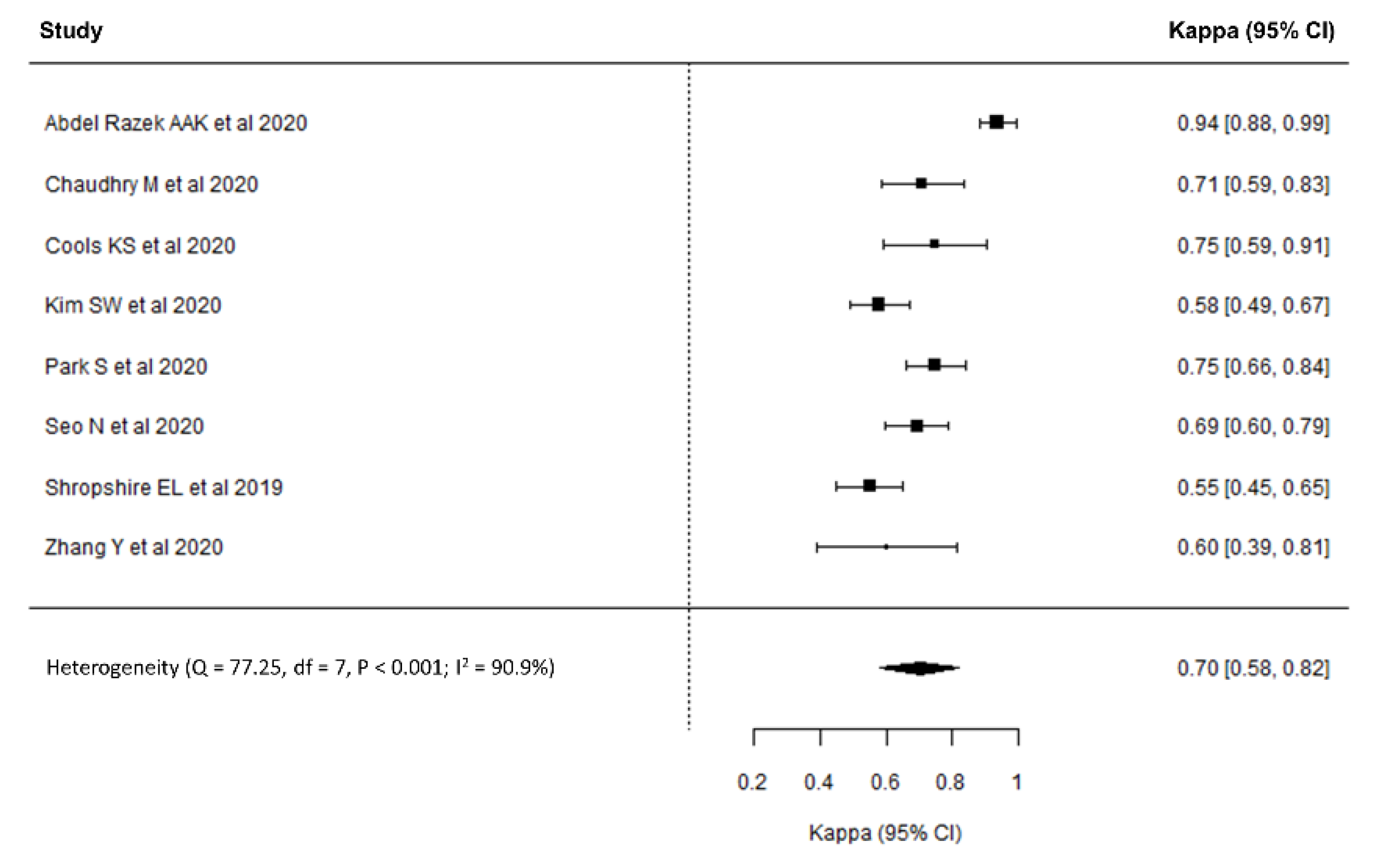
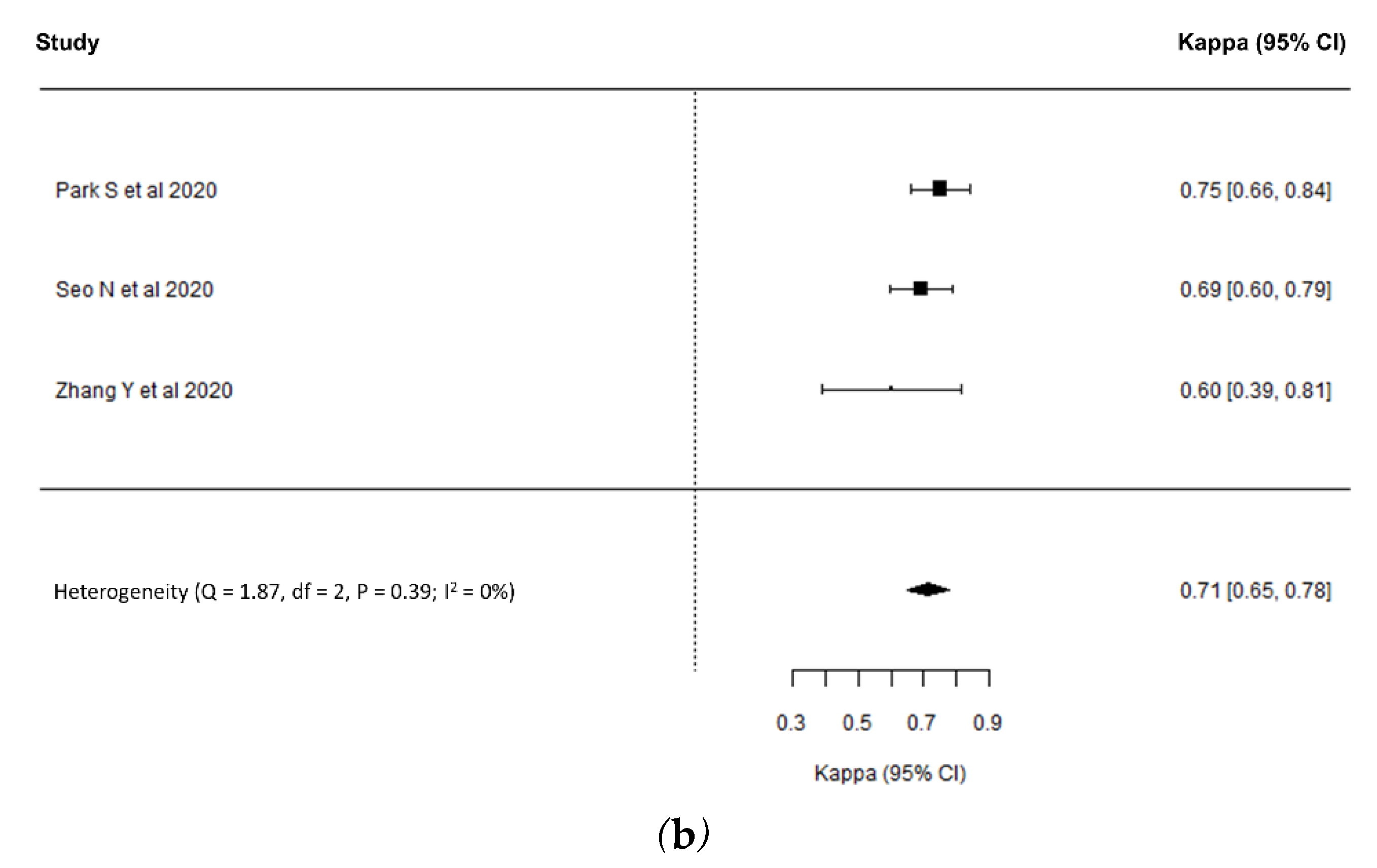
3.4. Interreader Reliability for LR-TR Category Assignment
3.5. Meta-Regression Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Search Query for MEDLINE |
|---|---|
| #1 | (((liver neoplasms[MeSH Terms]) OR (Liver[MeSH Terms]))) AND (radiology information systems[MeSH Terms]) |
| #2 | (LI-RADS[Text Word]) OR (“liver imaging reporting”[Text Word]) |
| #3 | (treatment[Text Word]) OR (response[Text Word]) |
| #4 | #1 OR #2 |
| #5 | #3 AND #4 |
| #6 | LR-TR[Text Word] |
| #7 | #5 OR #6 |
| #8 | (((magnetic resonance imaging[MeSH Terms]) OR (“magnetic resonanc*”[Text Word])) OR (MRI[Text Word])) OR (MR[Text Word]) |
| #9 | ((x ray tomography, computed[MeSH Terms]) OR (“computed tomograph*”[Text Word])) OR (CT[Text Word]) |
| #10 | #8 OR #9 |
| #11 | #7 AND #10 |
| #12 | #11 AND English[Lang] |
| No. | Search Query for EMBASE |
| #1 | ‘liver imaging reporting and data system’/exp OR ‘liver imaging reporting and data system’ |
| #2 | ‘li-rads’:ab,ti,kw OR ‘liver imaging reporting’:ab,ti,kw |
| #3 | ‘treatment’/exp OR treatment OR ‘response’/exp OR response |
| #4 | #1 OR #2 |
| #5 | #3 AND #4 |
| #6 | ‘lr-tr’ |
| #7 | #5 OR #6 |
| #8 | ‘magnetic resonanc*’:ab,ti,kw OR mri:ab,ti,kw OR mr:ab,ti,kw |
| #9 | ‘computed tomograph*’:ab,ti,kw OR ct:ab,ti,kw |
| #10 | #8 OR #9 |
| #11 | #7 AND #10 |
| #12 | #11 AND [english]/lim |
| Domain | Questionnaires |
|---|---|
| Index test | Was information of CT and MRI examination explicitly described? |
| Were methods of CT and MRI examination applicable? | |
| Study subject | Was a consecutive or random sample of patients enrolled? |
| Was a case-control design avoided? | |
| Did the study avoid inappropriate exclusion? | |
| Readers | Was information (e.g., number and experiences of readers) explicitly described? |
| Were readers representative for general reading practice? | |
| Reading Process | Were readers blinded to clinical information of patients which potentially affected their judgements? |
| Was reading process conducted independently? | |
| Blinding to reference standard | Were readers blinded to reference standard which potentially affected their judgements? |
| Statistical analysis | Was information regarding statistical analysis explicitly described? |
| Was statistical analysis applicable? | |
| Actual numbers of viable/nonviable lesions | Was information regarding the actual number of viable/nonviable lesions diagnosed by reference standard described? |


References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Ghouri, Y.A.; Mian, I.; Rowe, J.H. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J. Carcinog. 2017, 16, 1. [Google Scholar] [CrossRef]
- Cescon, M.; Cucchetti, A.; Ravaioli, M.; Pinna, A.D. Hepatocellular carcinoma locoregional therapies for patients in the waiting list. Impact on transplantability and recurrence rate. J. Hepatol. 2013, 58, 609–618. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.W.; Raman, S.S.; Asvadi, N.H.; Siripongsakun, S.; Hicks, R.M.; Chen, J.; Worakitsitisatorn, A.; McWilliams, J.; Tong, M.J.; Finn, R.S.; et al. Radiofrequency ablation of hepatocellular carcinoma as bridge therapy to liver transplantation: A 10-year intention-to-treat analysis. Hepatology 2017, 65, 1979–1990. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.S.; Yu, N.C.; Raman, S.S.; Lassman, C.; Tong, M.J.; Britten, C.; Durazo, F.; Saab, S.; Han, S.; Finn, R.; et al. Percutaneous radiofrequency ablation of hepatocellular carcinoma as a bridge to liver transplantation. Hepatology 2005, 41, 1130–1137. [Google Scholar] [CrossRef]
- Ho, M.H.; Yu, C.Y.; Chung, K.P.; Chen, T.W.; Chu, H.C.; Lin, C.K.; Hsieh, C.B. Locoregional therapy-induced tumor necrosis as a predictor of recurrence after liver transplant in patients with hepatocellular carcinoma. Ann. Surg. Oncol. 2011, 18, 3632–3639. [Google Scholar] [CrossRef] [PubMed]
- Allard, M.A.; Sebagh, M.; Ruiz, A.; Guettier, C.; Paule, B.; Vibert, E.; Cunha, A.S.; Cherqui, D.; Samuel, D.; Bismuth, H.; et al. Does pathological response after transarterial chemoembolization for hepatocellular carcinoma in cirrhotic patients with cirrhosis predict outcome after liver resection or transplantation? J. Hepatol. 2015, 63, 83–92. [Google Scholar] [CrossRef]
- American College of Radiology. Liver Imaging Reporting and Data System (LI-RADS). Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS/CT-MRI-LI-RADS-v2017 (accessed on 11 November 2020).
- Abdel Razek, A.A.K.; El-Serougy, L.G.; Saleh, G.A.; Shabana, W.; Abd El-Wahab, R. Reproducibility of LI-RADS treatment response algorithm for hepatocellular carcinoma after locoregional therapy. Diagn. Inter. Imaging 2020, 101, 547–553. [Google Scholar] [CrossRef]
- Chaudhry, M.; McGinty, K.A.; Mervak, B.; Lerebours, R.; Li, C.; Shropshire, E.; Ronald, J.; Commander, L.; Hertel, J.; Luo, S.; et al. The LI-RADS Version 2018 MRI treatment response algorithm: Evaluation of ablated hepatocellular carcinoma. Radiology 2020, 294, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Cools, K.S.; Moon, A.M.; Burke, L.M.B.; McGinty, K.A.; Strassle, P.D.; Gerber, D.A. Validation of the Liver Imaging Reporting and Data System Treatment Response Criteria After Thermal Ablation for Hepatocellular Carcinoma. Liver Transplant. 2020, 26, 203–214. [Google Scholar] [CrossRef]
- Kim, S.W.; Joo, I.; Kim, H.C.; Ahn, S.J.; Kang, H.J.; Jeon, S.K.; Lee, J.M. LI-RADS treatment response categorization on gadoxetic acid-enhanced MRI: Diagnostic performance compared to mRECIST and added value of ancillary features. Eur. Radiol. 2020, 30, 2861–2870. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Joo, I.; Lee, D.H.; Bae, J.S.; Yoo, J.; Kim, S.W.; Lee, J.M. Diagnostic Performance of LI-RADS Treatment Response Algorithm for Hepatocellular Carcinoma: Adding Ancillary Features to MRI Compared with Enhancement Patterns at CT and MRI. Radiology 2020, 296, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Seo, N.; Kim, M.S.; Park, M.S.; Choi, J.Y.; Do, R.K.G.; Han, K.; Kim, M.J. Evaluation of treatment response in hepatocellular carcinoma in the explanted liver with Liver Imaging Reporting and Data System version 2017. Eur. Radiol. 2020, 30, 261–271. [Google Scholar] [CrossRef]
- Shropshire, E.L.; Chaudhry, M.; Miller, C.M.; Allen, B.C.; Bozdogan, E.; Cardona, D.M.; King, L.Y.; Janas, G.L.; Do, R.K.; Kim, C.Y.; et al. LI-RADS treatment response algorithm: Performance and diagnostic accuracy. Radiology 2019, 292, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, J.; Li, H.; Zheng, T.; Jiang, H.; Li, M.; Song, B. Performance of LI-RADS version 2018 CT treatment response algorithm in tumor response evaluation and survival prediction of patients with single hepatocellular carcinoma after radiofrequency ablation. Ann. Transl. Med. 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Kottner, J.; Audigé, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed. J. Clin. Epidemiol. 2011, 64, 96–106. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Donati, O.F.; Do, R.K.; Hötker, A.M.; Katz, S.S.; Zheng, J.; Moskowitz, C.S.; Beattie, C.; Brown, K.T. Interreader and inter–test agreement in assessing treatment response following transarterial embolization for hepatocellular carcinoma. Eur. Radiol. 2015, 25, 2779–2788. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Lee, E.J.; Cha, S.S.; Han, S.S.; Choi, S.J.; Juhn, J.R.; Kim, M.H.; Lee, Y.J.; Park, S.J. Comparison of gadoxetic acid-enhanced MR imaging versus four-phase multi-detector row computed tomography in assessing tumor regression after radiofrequency ablation in subjects with hepatocellular carcinomas. J. Vasc. Interv. Radiol. 2010, 21, 348–356. [Google Scholar] [CrossRef]
- Kloeckner, R.; Otto, G.; Biesterfeld, S.; Oberholzer, K.; Dueber, C.; Pitton, M.B. MDCT versus MRI assessment of tumor response after transarterial chemoembolization for the treatment of hepatocellular carcinoma. Cardiovasc. Interv. Radiol. 2010, 33, 532–540. [Google Scholar] [CrossRef]
- Shim, J.H.; Han, S.; Shin, Y.M.; Yu, E.; Park, W.; Kim, K.M.; Lim, Y.S.; Lee, H.C. Optimal measurement modality and method for evaluation of responses to transarterial chemoembolization of hepatocellular carcinoma based on enhancement criteria. J. Vasc. Interv. Radiol. 2013, 24, 316–325. [Google Scholar] [CrossRef]
- Watanabe, H.; Kanematsu, M.; Goshima, S.; Yoshida, M.; Kawada, H.; Kondo, H.; Moriyama, N. Is gadoxetate disodium-enhanced MRI useful for detecting local recurrence of hepatocellular carcinoma after radiofrequency ablation therapy? AJR Am. J. Roentgenol. 2012, 198, 589–595. [Google Scholar] [CrossRef]
- Kim, H.C.; Kim, A.Y.; Han, J.K.; Chung, J.W.; Lee, J.Y.; Park, J.H.; Choi, B.I. Hepatic arterial and portal venous phase helical CT in patients treated with transcatheter arterial chemoembolization for hepatocellular carcinoma: Added value of unenhanced images. Radiology 2002, 225, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Rhim, H.; Lim, H.K.; Park, C.K.; Lee, W.J.; Do, Y.S.; Cho, J.W. Completeness of treatment in hepatocellular carcinomas treated with image-guided tumor therapies: Evaluation of positive predictive value of contrast-enhanced CT with histopathologic correlation in the explanted liver specimen. J. Comput. Assist. Tomogr. 2006, 30, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Hunt, S.J.; Yu, W.; Weintraub, J.; Prince, M.R.; Kothary, N. Radiologic monitoring of hepatocellular carcinoma tumor viability after transhepatic arterial chemoembolization: Estimating the accuracy of contrast-enhanced cross-sectional imaging with histopathologic correlation. J. Vasc. Interv. Radiol. 2009, 20, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Chernyak, V.; Fowler, K.J.; Heiken, J.P.; Sirlin, C.B. Use of gadoxetate disodium in patients with chronic liver disease and its implications for liver imaging reporting and data system (LI-RADS). J. Magn. Reson Imaging 2019, 49, 1236–1252. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.S.; Jeong, Y.Y.; Kang, H.K.; Kim, J.K.; Park, J.G. Imaging features of hepatocellular carcinoma after transcatheter arterial chemoembolization and radiofrequency ablation. AJR Am. J. Roentgenol. 2006, 187, W341–W349. [Google Scholar] [CrossRef] [PubMed]
- Mastrocostas, K.; Jang, H.J.; Fischer, S.; Dawson, L.A.; Munoz-Schuffenegger, P.; Sapisochin, G.; Kim, T.K. Imaging post-stereotactic body radiation therapy responses for hepatocellular carcinoma: Typical imaging patterns and pitfalls. Abdom. Radiol. N. Y. 2019, 44, 1795–1807. [Google Scholar] [CrossRef] [PubMed]




| Study | Country | Duration | Study Design | No. of Patients | M:F | Age (Years; Mean ± SD) | Underlying Liver Disease (Number) | No. of HCCs | Treatment | Modality (Contrast Agent [If MRI]) | No. of Readers | Reader Experience |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abdel Razek AAK et al. [10] | Egypt | 2017.11–2019.01 | Prospective | 93 | 79:14 | 55 ± 2.6 | Not available | 112 | LA (MWA or RFA; 97) TAT (cTACE; 25) | MRI (gadopentetic acid) | 2 | 25 and 10 years in liver imaging |
| Chaudhry M et al. [11] | USA | 2011.01–2015.12 | Retrospective | 36 | 32:4 | 62 ± 5 | HCV + alcohol (20) HCV (10) NASH (3) Alcohol (2) HBV (1) | 53 | LA (MWA or RFA; 53) | MRI (gadobenic acid) | 3 | 8, 7, and 2 years of post-fellowship experience in abdominal MRI |
| Cools KS et al. [12] | USA | 2006.01–2017.12 | Retrospective | 45 | 38:7 | 60 ± 6 | HCV (24) HCV + alcohol (13) Alcohol (2) NASH (2) Autoimmune (1) | 59 | LA (MWA or RFA; 59) | MRI (gadoxetic acid or gadobenic acid) | 2 | 9 years in liver MRI |
| Kim SW et al. [13] | Korea | 2015.01–2016.12 | Retrospective | 183 | 133:50 | 59.9 ± 10.8 | HBV (111) Alcohol (34) HCV (25) Others (13) | 183 | TAT (cTACE or DEB-TACE; 137) LA (RFA; 42) LA + TAT (4) | MRI (gadoxetic acid) | 2 | 7 and 5 years in liver MRI |
| Park S et al. [14] | Korea | 2014.01–2017.12 | Retrospective | 138 | 119:19 | 58 ± 9 | HBV (111) HCV (13) Alcohol (6) Others (8) | 138 | TAT (cTACE, DEB-TACE, or TARE; 98) LA (RFA or PEIT; 18) TAT + LA (22) | CT and MRI (gadoxetic acid) | 2 | 7 and 5 years in liver imaging |
| Seo N et al. [15] | Korea | 2007.01–2014.12 | Retrospective | 114 (CT, 113; MRI, 53) | 96:18 | 54 ± 6.9 | HBV (100) HCV (8) Alcohol (2) Others (4) | 206 (CT, 203; MRI, 84) | TAT (cTACE or DEB-TACE; 168) LA (RFA; 34) TAT + LA (4) | CT and/or MRI (gadoxetic acid or gadoteric acid) | 2 | 17 and 16 years in liver MRI |
| Shropshire EL et al. [16] | USA | 2006–2016 | Retrospective | 45 (CT, 24; MRI, 21) | 32:13 | 57.1 ± 8.2 | HCV (22) HCV + alcohol (8) NASH (6) Alcohol (2) AIH (2) NASH + Alcohol (1) HBV (1) Glycogen storage disease (1) Others (2) | 63 | TAT (cTACE; 63) | CT or MRI (gadoxetic acid or gadobenic acid) | 3 | 17 and 11 years in abdominal MRI |
| Zhang Y et al. [17] | China | 2010.01–2016.12 | Retrospective | 40 | 35:5 | 60.3 ± 10.4 | HBV (32) HCV (2) Others (6) | 40 | LA (RFA; 40) | CT | 2 | 8 and 7 years in liver imaging |
| Covariate | Subgroup | Number of Studies | Estimates | 95% CI | p-Value |
|---|---|---|---|---|---|
| Study design | Prospective | 1 | 0.94 | 0.88–0.99 | <0.001 |
| Retrospective | 7 | 0.66 | 0.60–0.73 | ||
| Underlying liver disease | HBV dominant | 4 | 0.67 | 0.58–0.75 | 0.49 |
| Others | 4 | 0.74 | 0.54–0.94 | ||
| Type of treatment | Local ablation | 3 | 0.70 | 0.62–0.79 | 0.02 |
| Transarterial treatment | 1 | 0.55 | 0.45–0.65 | ||
| % of LR-TR nonviable | ≥50% | 5 | 0.72 | 0.55–0.90 | 0.63 |
| <50% | 3 | 0.67 | 0.55–0.78 | ||
| Reader number | 2 (Cohen’s kappa) | 6 | 0.73 | 0.59–0.86 | 0.46 |
| 3 (Fleiss kappa) | 2 | 0.63 | 0.47–0.78 | ||
| Reader experience | Junior + Senior | 3 | 0.63 | 0.50–0.75 | 0.22 |
| All senior | 5 | 0.75 | 0.61–0.89 | ||
| Statistical methods | Unweighted kappa | 5 | 0.66 | 0.58–0.74 | 0.39 |
| Weighed Kappa | 3 | 0.76 | 0.54–0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.W.; Choi, S.H.; Lee, J.S.; Kim, S.Y.; Lee, S.J.; Byun, J.H. Interreader Reliability of Liver Imaging Reporting and Data System Treatment Response: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 237. https://doi.org/10.3390/diagnostics11020237
Kim DW, Choi SH, Lee JS, Kim SY, Lee SJ, Byun JH. Interreader Reliability of Liver Imaging Reporting and Data System Treatment Response: A Systematic Review and Meta-Analysis. Diagnostics. 2021; 11(2):237. https://doi.org/10.3390/diagnostics11020237
Chicago/Turabian StyleKim, Dong Wook, Sang Hyun Choi, Ji Sung Lee, So Yeon Kim, So Jung Lee, and Jae Ho Byun. 2021. "Interreader Reliability of Liver Imaging Reporting and Data System Treatment Response: A Systematic Review and Meta-Analysis" Diagnostics 11, no. 2: 237. https://doi.org/10.3390/diagnostics11020237
APA StyleKim, D. W., Choi, S. H., Lee, J. S., Kim, S. Y., Lee, S. J., & Byun, J. H. (2021). Interreader Reliability of Liver Imaging Reporting and Data System Treatment Response: A Systematic Review and Meta-Analysis. Diagnostics, 11(2), 237. https://doi.org/10.3390/diagnostics11020237