
Applicability of Anatomic and Physiologic Scoring Systems for the Prediction of Outcome in Polytraumatized Patients with Blunt Aortic Injuries

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
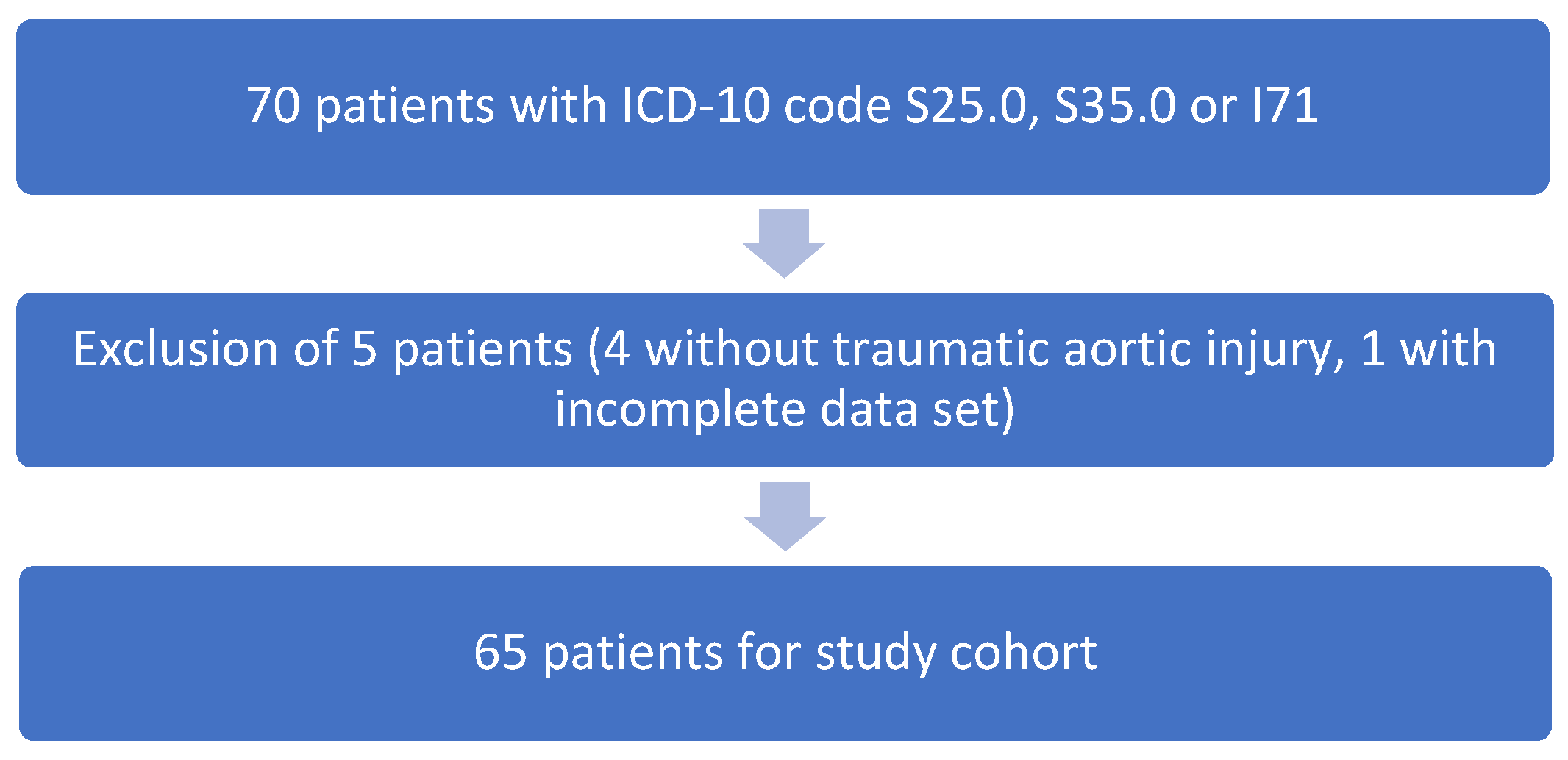
2.2. Inclusion/Exclusion Criteria
2.3. Ethical Approval
2.4. Scoring Systems
- Abbreviated Injury Scale (AIS);
- Injury Severity Score (ISS);
- New Injury Severity Score (NISS).
- Revised Trauma Score coded (RTSc);
- Acute Physiology and Chronic Health Evaluation II (APACHE II);
- Combined scores;
- Trauma and Injury Severity Score (TRISS).
2.5. Score Calculation
- Blunt trauma coefficient, −0.4499;
- RTSc coefficient, 0.8085;
- ISS coefficient, −0.0835;
- Age coefficient (if age > 54 years): −1.743.
2.6. Clinical Course/Clinical Parameters
2.7. Diagnosis and Management of Blunt Thoracic Aortic Injuries (BTAI)
2.8. Statistics
3. Results
3.1. Demographic Data
3.2. Mechanism of Injury
3.3. Aortic Injuries, Treatment of Blunt Aortic Injuries and Consequences of Stenting
3.4. Causes of Death
3.5. Logistic Regression
3.6. Correlation Analysis of Scores
3.7. Receiver Operating Characteristics Curves
- NISS, 0.812, (95%-CI, 0.689–0.935; asymptotic significance, 0.000*);
- ISS, 0.791 (95%-CI, 0.643–0.940; asymptotic significance, 0.001*);
- ISS without aortic injuries, 0.671 (95%-CI, 0.516–0.826; asymptotic significance 0.041*);
- APACHE II, 0.884 (95%-CI, 0.786–0.981; asymptotic significance 0.000*);
- RTSc, 0.679 (95%-CI, 0.486–0.872; asymptotic significance 0.140);
- TRISS, 0.761 (95%-CI, 0.577–0.945; asymptotic significance 0.030*);
- Shock index, 0.702 (95%-CI, 0.522–0.881; asymptotic significance 0.050).* significant
4. Discussion
4.1. Mortality
4.2. Abbreviated Injury Scale-Based Anatomic Scoring Systems
4.3. Physiologic Scoring Systems
4.4. Combined Scoring Systems
4.5. Limitations and Strength
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rhee, P.; Joseph, B.; Pandit, V.; Aziz, H.; Vercruysse, G.; Kulvatunyou, N.; Friese, R.S. Increasing trauma deaths in the United States. Ann. Surg. 2014, 260, 13–21. [Google Scholar] [CrossRef]
- David, J.S.; Bouzat, P.; Raux, M. Evolution and organisation of trauma systems. Anaesth. Crit. Care Pain Med. 2019, 38, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Galvagno, S.M., Jr.; Massey, M.; Bouzat, P.; Vesselinov, R.; Levy, M.J.; Millin, M.G.; Stein, D.M.; Scalea, T.M.; Hirshon, J.M. Correlation Between the Revised Trauma Score and Injury Severity Score: Implications for Prehospital Trauma Triage. Prehosp. Emerg. Care 2019, 23, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Franzen, D.; Genoni, M. Analysis of risk factors for death after blunt traumatic rupture of the thoracic aorta. Emerg. Med. J. 2015, 32, 124–129. [Google Scholar] [CrossRef]
- Teixeira, P.G.R.; Inaba, K.; Barmparas, G.; Georgiou, C.; Toms, C.; Noguchi, T.T.; Rogers, C.; Sathyavagiswaran, L.; Demetriades, D. Blunt thoracic aortic injuries: An autopsy study. J. Trauma 2011, 70, 197–202. [Google Scholar]
- Lee, W.A.; Matsumura, J.S.; Mitchell, R.S.; Farber, M.; Greenberg, R.K.; Azizzadeh, A.; Murad, M.H.; Fairman, R.M. Endovascular repair of traumatic thoracic aortic injury: Clinical practice guidelines of the Society for Vascular Surgery. J. Vasc. Surg. 2011, 53, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schimrigk, J.; Baulig, C.; Buschmann, C.; Ehlers, J.; Kleber, C.; Knippschild, S.; Leidel, B.A.; Malisch, T.; Steinhause, E.; Dahmen, J. Indications, procedure and outcome of prehospital emergency resuscitative thoracotomy-a systematic literature search. Unfallchirurg 2020, 123, 711–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAnena, O.J.; Moore, F.A.; Moore, E.E.; Mattox, K.L.; Marx, J.A.; Pepe, P. Invalidation of the APACHE II scoring system for patients with acute trauma. J. Trauma 1992, 33, 504–506; discussion 506–507. [Google Scholar] [CrossRef]
- Dossett, L.A.; Redhage, L.A.; Sawyer, R.G.; May, A.K. Revisiting the validity of APACHE II in the trauma ICU: Improved risk stratification in critically injured adults. Injury 2009, 40, 993–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauaia, A.; Moore, F.A.; Moore, E.E.; Moser, K.S.; Brennan, R.; Read, R.A.; Pons, P.T. Epidemiology of trauma deaths: A reassessment. J. Trauma 1995, 38, 185–193. [Google Scholar] [CrossRef]
- Baker, S.P.; O’Neill, B.; Haddon, W.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Greenspan, L.; McLellan, B.A.; Greig, H. Abbreviated Injury Scale and Injury Severity Score: A scoring chart. J. Trauma 1985, 25, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Osler, T.; Baker, S.P.; Long, W. A modification of the injury severity score that both improves accuracy and simplifies scoring. J. Trauma 1997, 43, 922–925; discussion 925–926. [Google Scholar] [CrossRef] [PubMed]
- Champion, H.R.; Sacco, W.J.; Copes, W.S.; Gann, D.S.; Gennarelli, T.A.; Flanagan, M.E. A revision of the Trauma Score. J. Trauma 1989, 29, 623–629. [Google Scholar] [CrossRef]
- Boyd, C.R.; Tolson, M.A.; Copes, W.S. Evaluating trauma care: The TRISS method. Trauma Score and the Injury Severity Score. J. Trauma 1987, 27, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Dyer, D.S.; Moore, E.E.; Mestek, M.F.; Bernstein, S.M.; Iklé, D.N.; Durham, J.D.; Heinig, M.J.; Russ, P.D.; Symonds, D.L.; Eule, J., Jr. Can chest CT be used to exclude aortic injury? Radiology 1999, 213, 195–202. [Google Scholar] [CrossRef]
- Fabian, T.C.; Richardson, J.D.; Croce, M.A.; Smith, J.S.; Rodman, G.; Kearney, P.A.; Flynn, W.; Ney, A.L.; Cone, J.B.; Luchette, F.A.; et al. Prospective study of blunt aortic injury: Multicenter Trial of the American Association for the Surgery of Trauma. J. Trauma 1997, 42, 374–380. [Google Scholar] [CrossRef]
- Parmley, L.F.; Mattingly, T.W.; Manion, W.C.; Jahnkejr, M.E.J. Nonpenetrating traumatic injury of the aorta. Circulation 1958, 17, 1086–1101. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.A.; van Wessem, K.J.P.; McDougall, D.; Lee, K.A.; Lyons, T.; Balogh, Z.J. Epidemiology of traumatic deaths: Comprehensive population-based assessment. World Surg. 2010, 34, 158–163. [Google Scholar] [CrossRef]
- Gennarelli, T.A.; Wodzin, E. Abbreviated Injury Scale 2005. In Association for the Advancement of Automotive Medicine; AIS: Barrington, IL, USA, 2005. [Google Scholar]
- Aharonson-Daniel, L.; Giveon, A.; Stein, M.; Peleg, K. Different AIS triplets: Different mortality predictions in identical ISS and NISS. J. Trauma 2006, 61, 711–717. [Google Scholar] [CrossRef]
- Rutledge, R. The Injury Severity Score is unable to differentiate between poor care and severe injury. J. Trauma 1996, 40, 944–950. [Google Scholar] [CrossRef]
- Parimi, N.; Fontaine, M.J.; Yang, S.; Hu, P.F.; Li, H.-C.; MacKenzie, C.F.; Kozar, R.A.; Miller, C.; Scalea, T.M.; Stein, D. Blood Transfusion Indicators Following Trauma in the Non-Massively Bleeding Patient. Ann. Clin. Lab. Sci. 2018, 48, 279–285. [Google Scholar]
- Harwood, P.J.; Giannoudis, P.V.; Probst, C.; Van Griensven, M.; Krettek, C.; Pape, H.C.; Polytrauma Study Group of the German Trauma Society. Which AIS based scoring system is the best predictor of outcome in orthopaedic blunt trauma patients? J. Trauma 2006, 60, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Esmer, E.; Derst, P.; Lefering, R.; Schulz, M.; Siekmann, H.; Delank, K.S. Prehospital assessment of injury type and severity in severely injured patients by emergency physicians: An analysis of the TraumaRegister DGU®. Unfallchirurg 2017, 120, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Pfeifer, R.; Tarkin, I.S.; Rocos, B.; Pape, H.C. Patterns of mortality and causes of death in polytrauma patients—Has anything changed? Injury 2009, 40, 907–911. [Google Scholar] [CrossRef] [PubMed]
- Malgras, B.; Prunet, B.; Lesaffre, X.; Boddaert, G.; Travers, S.; Cungi, P.-J.; Hornez, E.; Barbier, O.; Lefort, H.; Beaume, S.; et al. Damage control: Concept and implementation. J. Visc. Surg. 2017, 154 (Suppl. S1), S19–S29. [Google Scholar] [CrossRef]
- Wu, S.-C.; Chou, S.-E.; Liu, H.-T.; Hsieh, T.-M.; Su, W.-T.; Chien, P.-C.; Hsieh, C.-H. Performance of Prognostic Scoring Systems in Trauma Patients in the Intensive Care Unit of a Trauma Center. Int. J. Env. Res. Public Health 2020, 17, 7226. [Google Scholar] [CrossRef]
- Jiang, L.; Zheng, Z.; Zhang, M. The incidence of geriatric trauma is increasing and comparison of different scoring tools for the prediction of in-hospital mortality in geriatric trauma patients. World J. Emerg. Surg. 2020, 15, 59. [Google Scholar] [CrossRef]
- Agarwal, A.; Agrawal, A.; Maheshwari, R. Evaluation of Probability of Survival using APACHE II & TRISS Method in Orthopaedic Polytrauma Patients in a Tertiary Care Centre. J. Clin. Diagn. Res. 2015, 9, RC01–RC04. [Google Scholar]
- Gabbe, B.J.; Cameron, P.A.; Wolfe, R. TRISS: Does it get better than this? Acad. Emerg. Med. 2004, 11, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Kühne, C.A.; Ruchholtz, S.; Voggenreiter, G.; Eggebrecht, H.; Paffrath, T.; Waydhas, C.; Nast-Kolb, D. Traumatic aortic injuries in severely injured patients. Unfallchirurg 2005, 10, 279–287. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Parameter | Study Population | |
|---|---|---|
| Male | Female | |
| Number (n) | 56 | 9 |
| Age (years); mean ± SD | 41.4 (±17.5) | 43.3 (±20.5) |
| Sex; n (%) | 56 (86.2%) | 9 (13.8%) |
| ISS; median (IQR) | 34 (18.25) | 45 (17) |
| NISS; median (IQR) | 41 (17.75) | 50 (16) |
| RTS; median (IQR) | 6.904 (1.874) | 3.867 (0.733) |
| TRISS; median (IQR) | 82.75 (60.27) | 7.64 (11.67) |
| APACHE II; mean median (IQR) | 22 (11.5) | 22 (9) |
| ICU time (days); median (IQR) | 13 (19) | 24 (24) |
| Hospitalization time (days); median (IQR) | 19.5 (19.75) | 24 (24) |
| Ventilation (hours); median (IQR) | 230 (442) | 397 (555) |
| Mortality; n (%) | 12 (21.4%) | 4 (44.4%) |
| Types of Aortic Injuries | Frequency n (%) | Open Surgery n (%) | Endovascular Surgery n (%) | Conservative Therapy n (%) | Mortality n (%) |
|---|---|---|---|---|---|
| Aortic wall hematoma | 4 (6.2) | 0 (0) | 0 (0) | 4 (100) | 0 (0) |
| Aortic wall rupture | 38 (58.5) | 6 (15.8) | 27 (71.1) | 5 (13.2) | 11 (29.0) |
| Aortic dissection | 3 (4.6) | 0 (0) | 2 (66.7) | 1 (33.3) | 0 (0) |
| Comb. rupture and dissection | 16 (24.6) | 3 (18.8) | 12 (75.0) | 1 (6.3) | 4 (25.0) |
| Intimaflap | 2 (3.1) | 0 (0) | 0 (0) | 2 (100) | 0 (0) |
| Abdominal aortic injury | 1 (1.5) | 1 (100) | 0 (0) | 0 (0) | 0 (0) |
| Thoracic plaque rupture | 1 (1.5) | 0 (0) | 0 (0) | 1 (100) | 1 (100) * |
| Overall | 65 (100) | 10 (15.39) | 41 (63.08) | 14 (21.54) | 16 (24.62) |
| Number | Sex | Death after (days) | Cause of Death | ISS |
|---|---|---|---|---|
| 1 | female | 1 | hemorrhagic shock due to retroperitoneal bleeding | 45 |
| 2 | male | 1 | secondary free aortic rupture | 75 a,b |
| 3 | female | 1 | secondary free aortic rupture | 75 a,b |
| 4 | male | 1 | traumatic brain injury | 75 |
| 5 | male | 1 | secondary free aortic rupture | 75 a,b |
| 6 | male | 1 | secondary free aortic rupture | 75 a,b |
| 7 | male | 1 | traumatic brain injury | 45 |
| 8 | male | 1 | hemorrhage after left pulmonary hilus rupture | 75 a |
| 9 | male | 2 | myocardial infarction caused by coronary artery disease | 26 |
| 10 | male | 2 | Traumatic brain injury | 45 |
| 11 | male | 2 | hypotension (therapy limitation due to advance healthcare directive) | 21 |
| 12 | male | 3 | respiratory failure | 50 |
| 13 | male | 3 | multiple organ dysfunction syndrome | 34 |
| 14 | female | 8 | traumatic brain injury | 57 |
| 15 | male | 37 | multiple organ dysfunction syndrome | 50 |
| 16 | female | 61 | multiple organ dysfunction syndrome | 36 |
| Score | AUC | Sensitivity | Specificity | Odds Ratio | 95% Confidence Interval (ORS) |
|---|---|---|---|---|---|
| NISS | 0.812 | 0.375 | 0.980 | 1.117 | 0.050–0.171 * |
| ISS | 0.791 | 0.438 | 0.959 | 1.096 | 0.041–0.142 * |
| ISS w/o aorta | 0.671 | 0.125 | 1.000 | 1.059 | 0.007–0.107 * |
| TRISS | 0.761 | 0.250 | 0.957 | 0.977 | −0.047–0.001 |
| APACHE II | 0.880 | 0.545 | 0.938 | 1.089 | 0.034–0.136 * |
| RTSc | 0.679 | 0.000 | 1.000 | 0,802 | –0.623–0.221 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omar, A.; Winkelmann, M.; Liodakis, E.; Clausen, J.-D.; Graulich, T.; Omar, M.; Krettek, C.; Macke, C. Applicability of Anatomic and Physiologic Scoring Systems for the Prediction of Outcome in Polytraumatized Patients with Blunt Aortic Injuries. Diagnostics 2021, 11, 2156. https://doi.org/10.3390/diagnostics11112156
Omar A, Winkelmann M, Liodakis E, Clausen J-D, Graulich T, Omar M, Krettek C, Macke C. Applicability of Anatomic and Physiologic Scoring Systems for the Prediction of Outcome in Polytraumatized Patients with Blunt Aortic Injuries. Diagnostics. 2021; 11(11):2156. https://doi.org/10.3390/diagnostics11112156
Chicago/Turabian StyleOmar, Alexander, Marcel Winkelmann, Emmanouil Liodakis, Jan-Dierk Clausen, Tilman Graulich, Mohamed Omar, Christian Krettek, and Christian Macke. 2021. "Applicability of Anatomic and Physiologic Scoring Systems for the Prediction of Outcome in Polytraumatized Patients with Blunt Aortic Injuries" Diagnostics 11, no. 11: 2156. https://doi.org/10.3390/diagnostics11112156
APA StyleOmar, A., Winkelmann, M., Liodakis, E., Clausen, J.-D., Graulich, T., Omar, M., Krettek, C., & Macke, C. (2021). Applicability of Anatomic and Physiologic Scoring Systems for the Prediction of Outcome in Polytraumatized Patients with Blunt Aortic Injuries. Diagnostics, 11(11), 2156. https://doi.org/10.3390/diagnostics11112156