
Postmenopausal Chinese-Singaporean Women Have a Higher Ratio of Visceral to Subcutaneous Adipose Tissue Volume than Caucasian Women of the Same Age and BMI

 , ,
, ,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
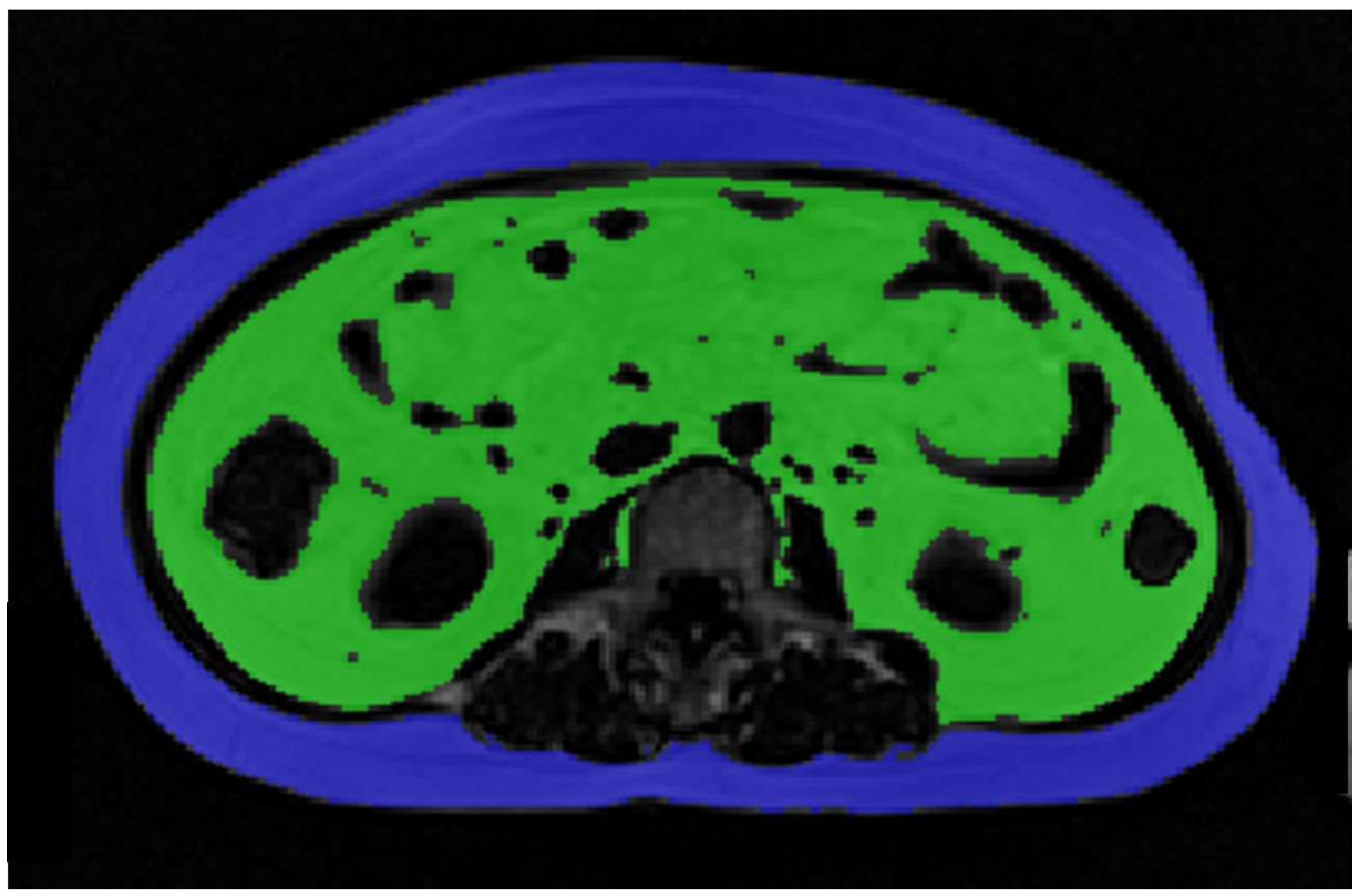
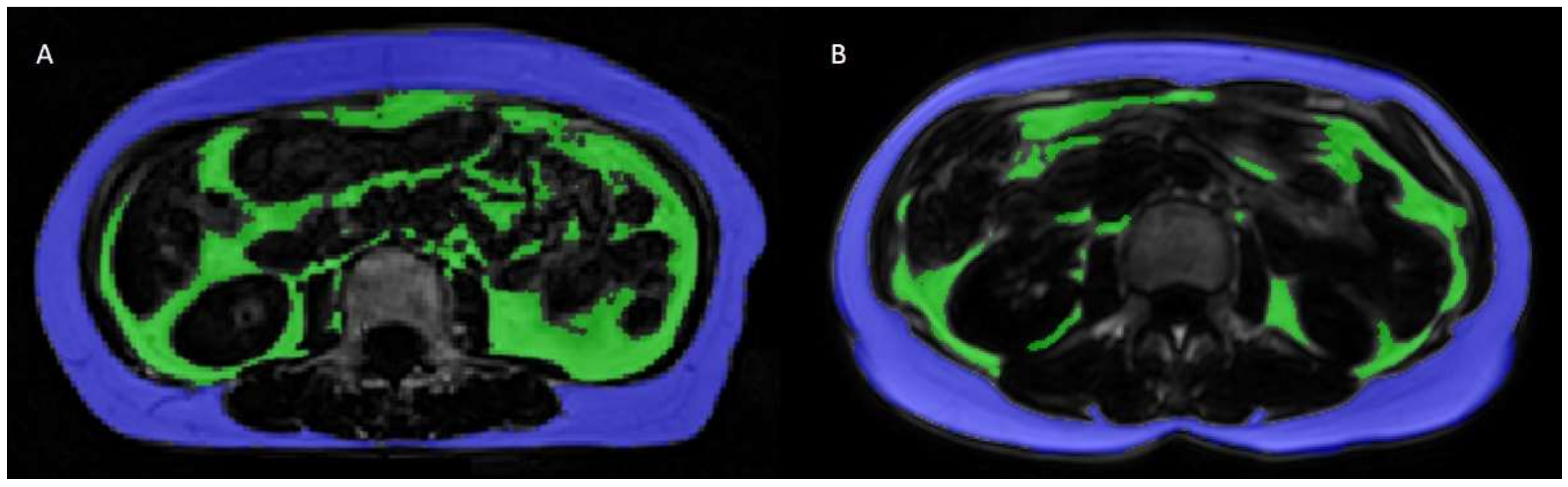
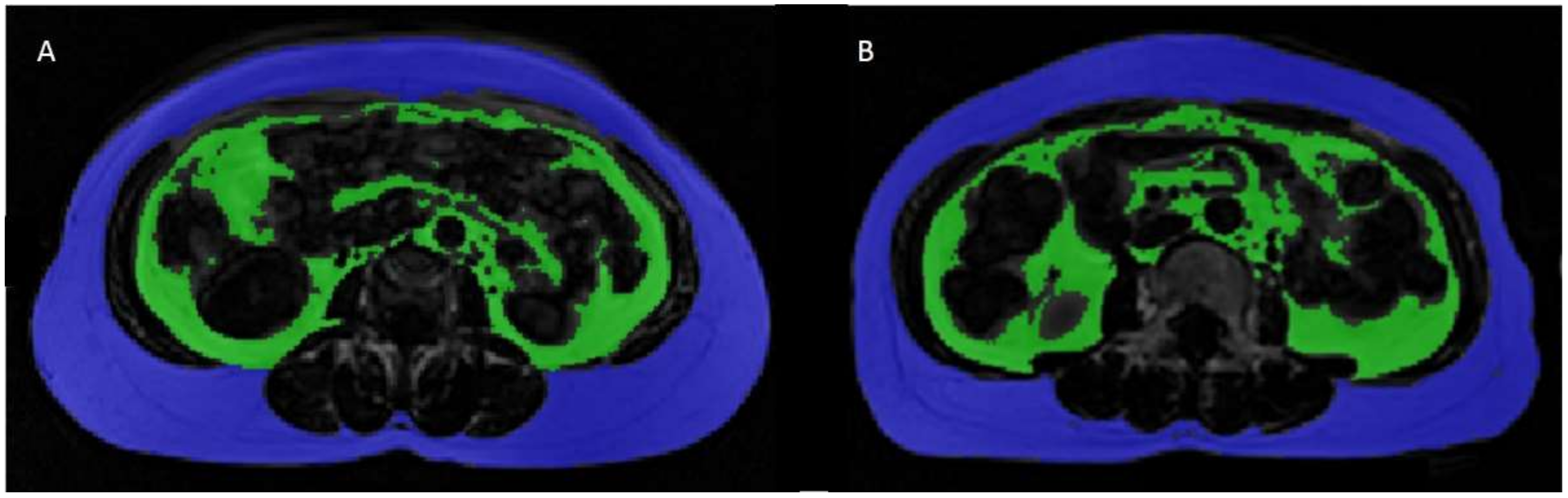
2.2. Adipose Tissue Volume Measurements
2.3. Calculation of SAT/VAT Volumes
2.4. Statistical Analysis
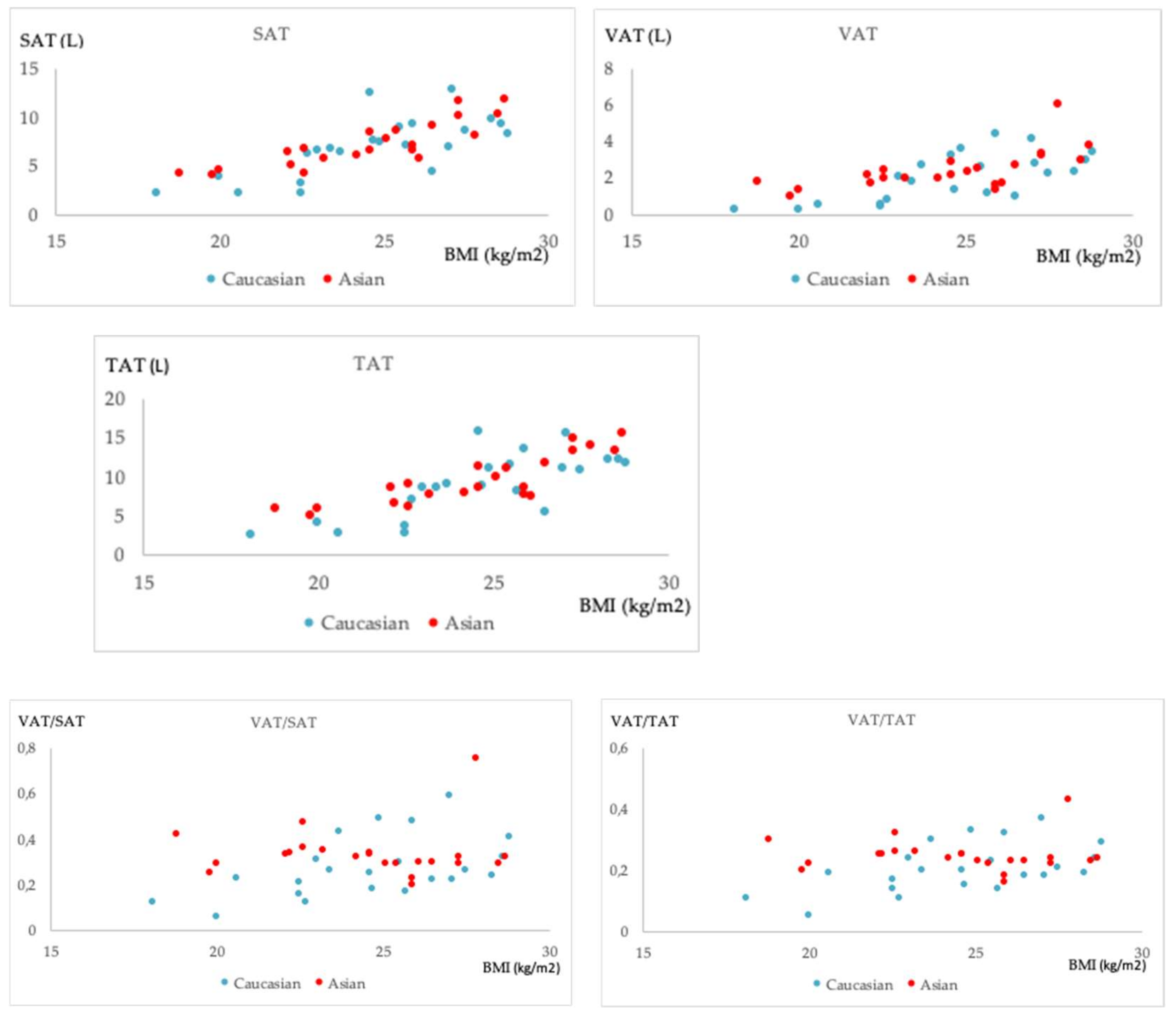
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wajchenberg, B.L. Subcutaneous and Visceral Adipose Tissue: Their Relation to the Metabolic Syndrome. Endocrine 2000, 21, 697–738. [Google Scholar] [CrossRef]
- Sites, C.K.; Calles-Escandón, J.; Brochu, M.; Butterfield, M.; Ashikaga, T.; Poehlman, E.T. Relation of regional fat distribution to insulin sensitivity in postmenopausal women. Fertil. Steril. 2000, 73, 61–65. [Google Scholar] [CrossRef]
- Fox, C.S.; Massaro, J.M.; Hoffmann, U.; Pou, K.M.; Maurovich-Horvat, P.; Liu, C.-Y.; Vasan, R.S.; Murabito, J.; Meigs, J.B.; Cupples, L.A.; et al. Abdominal Visceral and Subcutaneous Adipose Tissue Compartments. Circulation 2007, 116, 39–48. [Google Scholar] [CrossRef]
- Abraham, T.M.; Pedley, A.; Massaro, J.M.; Hoffmann, U.; Fox, C.S. Association Between Visceral and Subcutaneous Adipose Depots and Incident Cardiovascular Disease Risk Factors. Circulation 2015, 132, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Gast, K.B.; Heijer, M.D.; Smit, J.W.; Widya, R.L.; Lamb, H.J.; de Roos, A.; Jukema, J.W.; Rosendaal, F.R.; de Mutsert, R. Individual contributions of visceral fat and total body fat to subclinical atherosclerosis: The NEO study. Atherosclerosis 2015, 241, 547–554. [Google Scholar] [CrossRef]
- Donohoe, C.L.; Doyle, S.L.; Reynolds, J.V. Visceral adiposity, insulin resistance and cancer risk. Diabetol. Metab. Syndr. 2011, 3, 12. [Google Scholar] [CrossRef]
- Fujioka, S.; Matsuzawa, Y.; Tokunaga, K.; Tarui, S. Contribution of intra-abdominal fat accumulation to the impairment of glucose and lipid metabolism in human obesity. Metabolism 1987, 36, 54–59. [Google Scholar] [CrossRef]
- Demerath, E.W.; Sun, S.S.; Rogers, N.; Lee, M.; Reed, D.; Choh, A.C.; Couch, W.; Czerwinski, S.A.; Chumlea, W.C.; Siervogel, R.M.; et al. Anatomical Patterning of Visceral Adipose Tissue: Race, Sex, and Age Variation**. Obesity 2007, 15, 2984–2993. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, M.; Oka, R.; Sakurai, M.; Nakamura, K.; Moriuchi, T.; Miyamoto, S.; Takeda, Y.; Yagi, K.; Yamagishi, M. Age-related Changes in Abdominal Fat Distribution in Japanese Adults in the General Population. Intern. Med. 2011, 50, 679–685. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Janssen, I.; Powell, L.H.; Kazlauskaite, R.; Dugan, S.A. Testosterone and Visceral Fat in Midlife Women: The Study of Women’s Health Across the Nation (SWAN) Fat Patterning Study. Obesity 2010, 18, 604–610. [Google Scholar] [CrossRef]
- Whitaker, K.M.; Choh, A.C.; Lee, M.; Towne, B.; A Czerwinski, S.; Demerath, E.W. Sex differences in the rate of abdominal adipose accrual during adulthood: The Fels Longitudinal Study. Int. J. Obes. 2016, 40, 1278–1285. [Google Scholar] [CrossRef]
- Lovejoy, J.C.; de la Bretonne, J.A.; Klemperer, M.; Tulley, R. Abdominal fat distribution and metabolic risk factors: Effects of race. Metabolism 1996, 45, 1119–1124. [Google Scholar] [CrossRef]
- Sniderman, A.D.; Bhopal, R.; Prabhakaran, D.; Sarrafzadegan, N.; Tchernof, A. Why might South Asians be so susceptible to central obesity and its atherogenic consequences? The adipose tissue overflow hypothesis. Int. J. Epidemiol. 2007, 36, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.F.; Chiapa, A.L.; Rodriquez, M.; Phelps, D.R.; Cardarelli, K.M.; Vishwanatha, J.; Bae, S.; Cardarelli, R. Visceral Fat, Waist Circumference, and BMI: Impact of Race/ethnicity. Obesity 2008, 16, 600–607. [Google Scholar] [CrossRef]
- A Crawford, M.; Mendoza-Vasconez, A.S.; A Larsen, B. Type II Diabetes Disparities in Diverse Women: The Potential Roles of Body Composition, Diet and Physical Activity. Women’s Health 2015, 11, 913–927. [Google Scholar] [CrossRef] [PubMed]
- Deurenberg, P.; Deurenberg-Yap, M. Differences in body-composition assumptions across ethnic groups: Practical consequences. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Rønn, P.F.; Andersen, G.S.; Lauritzen, T.; Christensen, D.L.; Aadahl, M.; Carstensen, B.; E Jørgensen, M. Ethnic differences in anthropometric measures and abdominal fat distribution: A cross-sectional pooled study in Inuit, Africans and Europeans. J. Epidemiol. Community Health 2017, 71, 536–543. [Google Scholar] [CrossRef]
- Nazare, J.-A.; Smith, J.D.; Borel, A.-L.; Haffner, S.M.; Balkau, B.; Ross, R.; Massien, C.; Alméras, N.; Després, J.-P. Ethnic influences on the relations between abdominal subcutaneous and visceral adiposity, liver fat, and cardiometabolic risk profile: The International Study of Prediction of Intra-Abdominal Adiposity and Its Relationship With Cardiometabolic Risk/Intra-Abdominal Adiposity. Am. J. Clin. Nutr. 2012, 96, 714–726. [Google Scholar] [CrossRef] [PubMed]
- Deurenberg, P.; Deurenberg-Yap, M.; Guricci, S. Asians are different from Caucasians and from each other in their body mass index/body fat per cent relationship. Obes. Rev. 2002, 3, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Yoon, K.-H.; Lee, J.-H.; Kim, J.-W.; Cho, J.H.; Choi, Y.H.; Ko, S.-H.; Zimmet, P.; Son, H.-Y. Epidemic obesity and type 2 diabetes in Asia. Lancet 2006, 368, 1681–1688. [Google Scholar] [CrossRef]
- Khor, G.L. Cardiovascular epidemiology in the Asia-Pacific region. Asia Pac. J. Clin. Nutr. 2008, 10, 76–80. [Google Scholar] [CrossRef]
- Rosano, G.M.C.; Vitale, C.; Marazzi, G.; Volterrani, M. Menopause and cardiovascular disease: The evidence. Climacteric 2007, 10, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Pardhe, B.D.; Ghimire, S.; Shakya, J.; Pathak, S.; Shakya, S.; Bhetwal, A.; Khanal, P.R.; Parajuli, N.P. Elevated Cardiovascular Risks among Postmenopausal Women: A Community Based Case Control Study from Nepal. Biochem. Res. Int. 2017, 2017, 1–5. [Google Scholar] [CrossRef]
- Szmuilowicz, E.; Stuenkel, C.A.; Seely, E.W. Influence of menopause on diabetes and diabetes risk. Nat. Rev. Endocrinol. 2009, 5, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Lovejoy, J.C.; Champagne, C.M.; de Jonge, L.; Xie, H.; Smith, S.R. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int. J. Obes. 2008, 32, 949–958. [Google Scholar] [CrossRef]
- Ho, S.C.; Wu, S.; Chan, S.G.; Sham, A. Menopausal transition and changes of body composition: A prospective study in Chinese perimenopausal women. Int. J. Obes. 2010, 34, 1265–1274. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-W.; Allison, D.; Heymsfield, S.B.; Gallagher, D. Larger Amounts of Visceral Adipose Tissue in Asian Americans. Obes. Res. 2001, 9, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, T.; Sekikawa, A.; Murata, K.; Maegawa, H.; Takamiya, T.; Okamura, T.; El-Saed, A.; Miyamatsu, N.; Edmundowicz, D.; Kita, Y.; et al. Japanese men have larger areas of visceral adipose tissue than Caucasian men in the same levels of waist circumference in a population-based study. Int. J. Obes. 2006, 30, 1163–1165. [Google Scholar] [CrossRef]
- A Lear, S.; Humphries, K.H.; Kohli, S.; Chockalingam, A.; Frohlich, J.J.; Birmingham, C. Visceral adipose tissue accumulation differs according to ethnic background: Results of the Multicultural Community Health Assessment Trial (M-CHAT). Am. J. Clin. Nutr. 2007, 86, 353–359. [Google Scholar] [CrossRef]
- Lim, U.; Ernst, T.; Buchthal, S.D.; Latch, M.; Albright, C.L.; Wilkens, L.R.; Kolonel, L.N.; Murphy, S.P.; Chang, L.; Novotny, R.; et al. Asian women have greater abdominal and visceral adiposity than Caucasian women with similar body mass index. Nutr. Diabetes 2011, 1, e6. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Razak, F.; Anand, S.S.; Shannon, H.; Vuksan, V.; Davis, B.; Jacobs, R.; Teo, K.K.; McQueen, M.; Yusuf, S. Defining Obesity Cut Points in a Multiethnic Population. Circulation 2007, 115, 2111–2118. [Google Scholar] [CrossRef] [PubMed]
- Okorodudu, D.; Jumean, M.F.; Montori, V.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Rao, G.; Powell-Wiley, T.M.; Ancheta, I.; Hairston, K.; Kirley, K.; Lear, S.A.; North, K.E.; Palaniappan, L.; Rosal, M.C. Identification of Obesity and Cardiovascular Risk in Ethnically and Racially Diverse Populations. Circulation 2015, 132, 457–472. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Albu, J.B.; Murphy, L.; Frager, D.H.; A Johnson, J.; Pi-Sunyer, F.X. Visceral Fat and Race-Dependent Health Risks in Obese Nondiabetic Premenopausal Women. Diabetes 1997, 46, 456–462. [Google Scholar] [CrossRef]
- Park, Y.-W.; Heymsfield, S.; Gallagher, D. Are dual-energy X-ray absorptiometry regional estimates associated with visceral adipose tissue mass? Int. J. Obes. 2002, 26, 978–983. [Google Scholar] [CrossRef] [PubMed]
- Irlbeck, T.; Massaro, J.; Bamberg, F.; O’Donnell, C.J.; Hoffmann, U.; Fox, C.S. Association between single-slice measurements of visceral and abdominal subcutaneous adipose tissue with volumetric measurements: The Framingham Heart Study. Int. J. Obes. 2010, 34, 781–787. [Google Scholar] [CrossRef]
- Shen, W.; Chen, J.; Gantz, M.; Velasquez, G.; Punyanitya, M.; Heymsfield, S.B. A Single mri Slice Does Not Accurately Predict Visceral and Subcutaneous Adipose Tissue Changes During Weight Loss. Obesity 2012, 20, 2458–2463. [Google Scholar] [CrossRef]
- Shen, J.; Baum, T.; Cordes, C.; Ott, B.; Skurk, T.; Kooijman, H.; Rummeny, E.J.; Hauner, H.; Menze, B.H.; Karampinos, D.C. Automatic segmentation of abdominal organs and adipose tissue compartments in water-fat MRI: Application to weight-loss in obesity. Eur. J. Radiol. 2016, 85, 1613–1621. [Google Scholar] [CrossRef]
- Cordes, C.; Msc, M.D.; Ott, B.; Shen, J.; Ruschke, S.; Settles, M.; Eichhorn, C.; Bauer, J.S.; Kooijman, H.; Rummeny, E.J.; et al. MR-detected changes in liver fat, abdominal fat, and vertebral bone marrow fat after a four-week calorie restriction in obese women. J. Magn. Reson. Imaging 2015, 42, 1272–1280. [Google Scholar] [CrossRef] [PubMed]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3 D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. NeuroImage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.; Chan, J.; Cockram, C.; Woo, J. Prediction of hypertension, diabetes, dyslipidaemia or albuminuria using simple anthropometric indexes in Hong Kong Chinese. Int. J. Obes. 1999, 23, 1136–1142. [Google Scholar] [CrossRef]
- Palaniappan, L.P.; Wong, E.C.; Shin, J.J.; Fortmann, S.P.; Lauderdale, D.S. Asian Americans have greater prevalence of metabolic syndrome despite lower body mass index. Int. J. Obes. 2010, 35, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, W.Y.; Bergstrom, R.W.; Boyko, E.; Chen, K.-W.; E Kahn, S.; Leonetti, D.L.; McNeely, M.J.; Newell, L.L.; Shofer, J.B.; Wahl, P.W. Type 2 diabetes and the metabolic syndrome in Japanese Americans. Diabetes Res. Clin. Pr. 2000, 50, S73–S76. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Caucasian Group | Asian Group | |
|---|---|---|
| TR | 4 msec | 6.55 msec |
| TE1/TE2 | TE1 = 1.32 msec/ TE2 = 2.6 msec | TE1 = 1.35 msec/ TE2 = 2.58 msec |
| Flip angle | 10° | 9° |
| Field of view (FOV) | 500 × 446 mm3 | 450 × 450 mm3 |
| Acquisition voxel | 1.5 × 2.0 × 5.0 mm3 | 1.4 × 1.4 × 2.0 mm3 |
| Scan time | 10 sec | 116 sec |
| Caucasian Group (n = 22) | Asian Group (n = 22) | p | |
|---|---|---|---|
| Normally distributed | Mean (SD, range) | Mean (SD, range) | |
| BMI (kg/m2) | 24.62 (0.61, 18.1–28.8) | 24.51 (0.6, 18.8–28.7) | NS |
| Height (m) | 1.66 (0.01, 1.56–1.80) | 1.56 (0.01, 1.45–1.67) | <0.01 |
| Analyzed region length (m) | 0.35 (0.01, 0.3–0.4) | 0.36 (0.005, 0.32–0.40) | NS |
| Analyzed region length/Height | 0.21 (0.003, 0.18–0.24) | 0.23 (0.003, 0.21–0.25) | <0.01 |
| SAT (L) | 6.85 (0.65, 2.08–12.72) | 7.13 (0.5, 3.96–11.76) | NS |
| TAT (L) | 8.85 (0.87, 2.33–15.65) | 9.49 (0.67, 4.94–15.51) | NS |
| Age (years) | 57.15 (54–68) | 58 (55–67) | NS |
| VAT (L) | 2.11 (0.21–4.39) | 2.13 (0.98–5.98) | NS |
| VAT/SAT ratio | 0.25 (0.06–0.59) | 0.32 (0.20–0.75) | 0.02 |
| VAT/TAT ratio | 0.2 (0.05–0.37) | 0.24 (0.16–0.43) | 0.02 |
| Caucasian Group | Asian Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Age | BMI | Age | BMI | |||||
| rho | p | r | p | rho | p | r/rho | p | |
| VAT (l) | −0.12 | NS | 0.69 | <0.01 | −0.14 | NS | 0.67 | <0.01 |
| SAT (l) | −0.20 | NS | 0.72 | <0.01 | 0.03 | NS | 0.85 r | <0.01 |
| TAT (l) | −0.18 | NS | 0.75 | <0.01 | −0.02 | NS | 0.85 r | <0.01 |
| VAT/SAT | −0.29 | NS | 0.49 | 0.02 | −0.21 | NS | −0.25 | NS |
| VAT/TAT | −0.03 | NS | 0.53 | 0.01 | −0.23 | NS | −0.23 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalimeri, M.; Totman, J.J.; Baum, T.; Diefenbach, M.N.; Hauner, H.; Makowski, M.R.; Subburaj, K.; Cameron-Smith, D.; Henry, C.J.; Karampinos, D.C.; et al. Postmenopausal Chinese-Singaporean Women Have a Higher Ratio of Visceral to Subcutaneous Adipose Tissue Volume than Caucasian Women of the Same Age and BMI. Diagnostics 2021, 11, 2127. https://doi.org/10.3390/diagnostics11112127
Kalimeri M, Totman JJ, Baum T, Diefenbach MN, Hauner H, Makowski MR, Subburaj K, Cameron-Smith D, Henry CJ, Karampinos DC, et al. Postmenopausal Chinese-Singaporean Women Have a Higher Ratio of Visceral to Subcutaneous Adipose Tissue Volume than Caucasian Women of the Same Age and BMI. Diagnostics. 2021; 11(11):2127. https://doi.org/10.3390/diagnostics11112127
Chicago/Turabian StyleKalimeri, Maria, John J. Totman, Thomas Baum, Maximilian N. Diefenbach, Hans Hauner, Marcus R. Makowski, Karupppasamy Subburaj, David Cameron-Smith, Christiani Jeyakumar Henry, Dimitrios C. Karampinos, and et al. 2021. "Postmenopausal Chinese-Singaporean Women Have a Higher Ratio of Visceral to Subcutaneous Adipose Tissue Volume than Caucasian Women of the Same Age and BMI" Diagnostics 11, no. 11: 2127. https://doi.org/10.3390/diagnostics11112127
APA StyleKalimeri, M., Totman, J. J., Baum, T., Diefenbach, M. N., Hauner, H., Makowski, M. R., Subburaj, K., Cameron-Smith, D., Henry, C. J., Karampinos, D. C., & Junker, D. (2021). Postmenopausal Chinese-Singaporean Women Have a Higher Ratio of Visceral to Subcutaneous Adipose Tissue Volume than Caucasian Women of the Same Age and BMI. Diagnostics, 11(11), 2127. https://doi.org/10.3390/diagnostics11112127