
Comparative Analysis of BIOCHIP Mosaic-Based Indirect Immunofluorescence with Enzyme-Linked Immunosorbent Assay for Diagnosing Myasthenia Gravis




 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Biochemical Analysis
2.2.1. BIOCHIP Mosaic Indirect Immunofluorescence Assay
2.2.2. ELISA Methods
2.3. Statistical Analysis
3. Results
- -
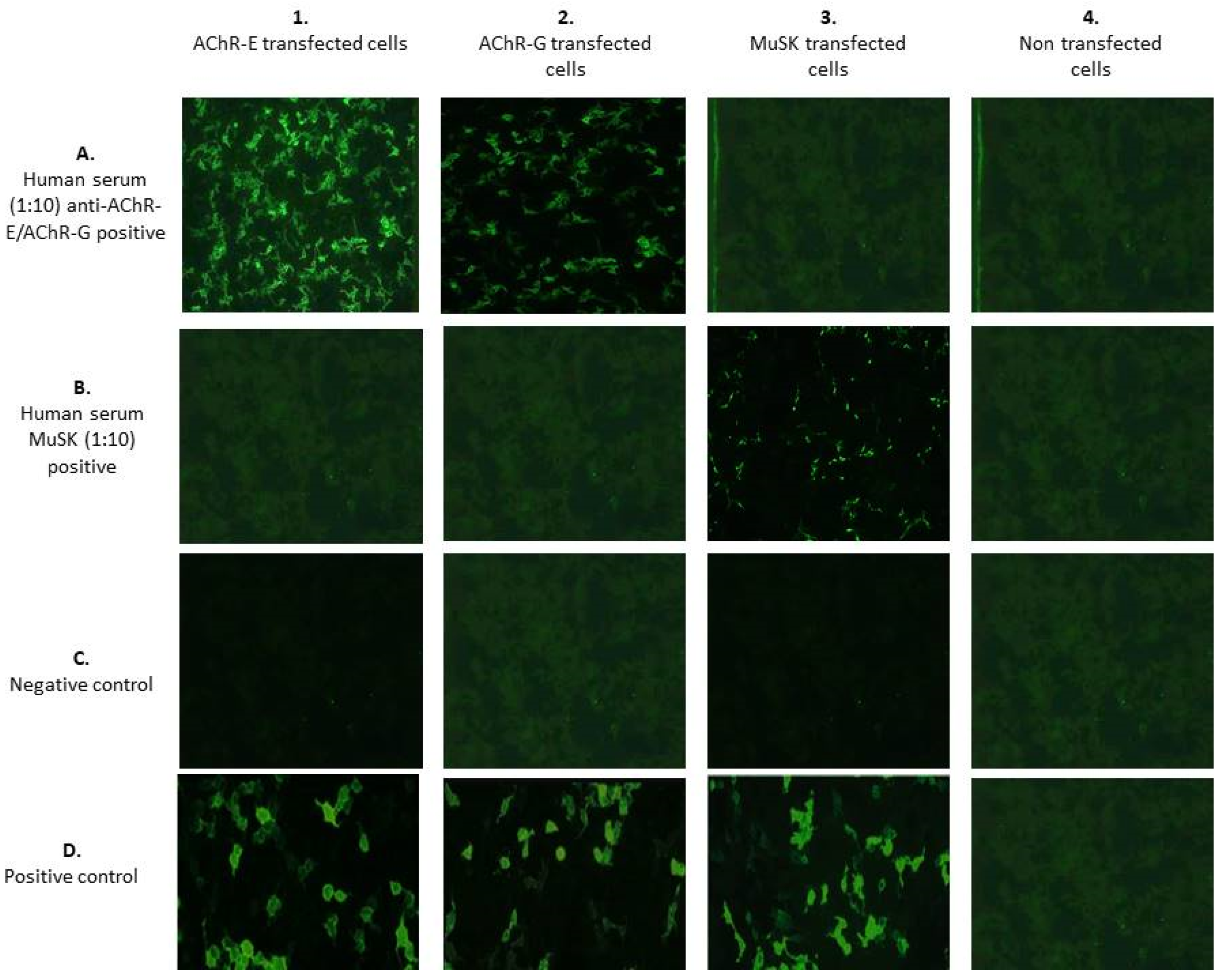
- Antibodies against AChR-E showed a flat or fine-to-coarse granular fluorescence of the cells, and also a smooth to very fine granular fluorescence of the cells in the absence of the staining of the membrane of the non-transfected cells. The area of the cell nucleus was only slightly stained (Figure 1(1A)).
- -
- Antibodies against AChR-G showed a spotted, and also a smooth-to-very fine granular fluorescence of the cells in the absence of the staining of the membrane of the non-transfected cells. The area of the cell nucleus was only slightly stained (Figure 1(2A)).
- -
- Antibodies against MuSK produced a smooth-to-very fine granular fluorescence of the cells in the absence of the staining of the membrane of the non-transfected cells. The area of the cell nucleus was only slightly stained (Figure 1(3B)). To evaluate the BIOCHIP mosaic intra-laboratory reproducibility, positive and negative control samples were tested 10 times in separate runs by 2 blinded operators. The overall agreement within the intra-laboratory runs was close to 100%.
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berrih-Aknin, S.; Le Panse, R. Myasthenia gravis: A comprehensive review of immune dysregulation and etiological mechanisms. J. Autoimmun. 2014, 52, 90–100. [Google Scholar] [CrossRef]
- Gilhus, N.E.; Verschuuren, J.J. Myasthenia gravis: Subgroup classification and therapeutic strategies. Lancet Neurol. 2015, 14, 1023–1036. [Google Scholar] [CrossRef]
- Gilhus, N.E.; Tzartos, S.; Evoli, A.; Palace, J.; Burns, T.M.; Verschuuren, J. Myasthenia gravis. Nat. Rev. Dis. Primers 2019, 5, 30. [Google Scholar] [CrossRef]
- Gilhus, N.E. Myasthenia Gravis. N. Engl. J. Med. 2016, 375, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Gastaldi, M.; Scaranzin, S.; Businaro, P.; Mobilia, E.; Benedetti, L.; Pesce, G.; Franciotta, D. Improving laboratory diagnostics in myasthenia gravis. Expert Rev. Mol. Diagn. 2021, 21, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Verschuuren, J.J.; Huijbers, M.G.; Plomp, J.J.; Niks, E.H.; Molenaar, P.C.; Martinez-Martinez, P.; Gomez, A.M.; De Baets, M.H.; Losen, M. Pathophysiology of myasthenia gravis with antibodies to the acetylcholine receptor, muscle-specific kinase and low-density lipoprotein receptor-related protein 4. Autoimmun. Rev. 2013, 12, 918–923. [Google Scholar] [CrossRef]
- Pevzner, A.; Schoser, B.; Peters, K.; Cosma, N.C.; Karakatsani, A.; Schalke, B.; Melms, A.; Kröger, S. Anti-LRP4 autoantibodies in AChR- and MuSK-antibody-negative myasthenia gravis. J. Neurol. 2012, 259, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.S.; Richman, D.P. Muscle-Specific Kinase Myasthenia Gravis. Front. Immunol. 2020, 11, 707. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, J. An assay for antibodies to human acetylcholine receptor in serum from patients with myasthenia gravis. Clin. Immunol. Immunopathol. 1977, 7, 36–43. [Google Scholar] [CrossRef]
- Matthews, I.; Chen, S.; Hewer, R.; McGrath, V.; Furmaniak, J.; Rees Smith, B. Muscle-specific receptor tyrosine kinase autoantibodies--A new immunoprecipitation assay. Clin. Chim. Acta 2004, 348, 95–99. [Google Scholar] [CrossRef]
- Hewer, R.; Matthews, I.; Chen, S.; McGrath, V.; Evans, M.; Roberts, E.; Nute, S.; Sanders, J.; Furmaniak, J.; Smith, B.R. A sensitive non-isotopic assay for acetylcholine receptor autoantibodies. Clin. Chim. Acta 2006, 364, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Leite, M.I.; Jacob, S.; Viegas, S.; Cossins, J.; Clover, L.; Morgan, B.P.; Beeson, D.; Willcox, N.; Vincent, A. IgG1 antibodies to acetylcholine receptors in ‘seronegative’ myasthenia gravis. Brain 2008, 131, 1940–1952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zisimopoulou, P.; Lagoumintzis, G.; Kostelidou, K.; Bitzopoulou, K.; Kordas, G.; Trakas, N.; Poulas, K.; Tzartos, S.J. Towards antigen-specific apheresis of pathogenic autoantibodies as a further step in the treatment of myasthenia gravis by plasmapheresis. J. Neuroimmunol. 2008, 201–202, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswami, P.; Sanders, D.B.; Wolfe, G.; Benatar, M.; Cea, G.; Evoli, A.; Gilhus, N.E.; Illa, I.; Kuntz, N.L.; Massey, J.; et al. International Consensus Guidance for Management of Myasthenia Gravis: 2020 Update. Neurology 2021, 96, 114–122. [Google Scholar] [CrossRef]
- Leite, M.I.; Waters, P.; Vincent, A. Diagnostic use of autoantibodies in myasthenia gravis. Autoimmunity 2010, 43, 371–379. [Google Scholar] [CrossRef]
- Frykman, H.; Kumar, P.; Oger, J. Immunopathology of Autoimmune Myasthenia Gravis: Implications for Improved Testing Algorithms and Treatment Strategies. Front. Neurol. 2020, 11, 596621. [Google Scholar] [CrossRef]
- Lazaridis, K.; Tzartos, S.J. Myasthenia Gravis: Autoantibody Specificities and Their Role in MG Management. Front. Neurol. 2020, 11, 596981. [Google Scholar] [CrossRef]
- Lindstrom, J. Acetylcholine receptors and myasthenia. Muscle Nerve 2000, 23, 453–477. [Google Scholar] [CrossRef]
- Vincent, A.; Newsom-Davis, J. Acetylcholine receptor antibody as a diagnostic test for myasthenia gravis: Results in 153 validated cases and 2967 diagnostic assays. J. Neurol. Neurosurg. Psychiatry 1985, 48, 1246–1452. [Google Scholar] [CrossRef] [Green Version]
- Tomschik, M.; Hilger, E.; Rath, J.; Mayer, E.M.; Fahrner, M.; Cetin, H.; Löscher, W.N.; Zimprich, F. Subgroup stratification and outcome in recently diagnosed generalized myasthenia gravis. Neurology 2020, 95, e1426–e1436. [Google Scholar] [CrossRef]
- Kohler, S.; Losen, M.; Alexander, T.; Hiepe, F.; Meisel, A. Myasthenia gravis: Subgroup classifications. Lancet Neurol. 2016, 15, 356–357. [Google Scholar] [CrossRef] [Green Version]
- Mantegazza, R.; Antozzi, C. When myasthenia gravis is deemed refractory: Clinical signposts and treatment strategies. Ther Adv Neurol Disord. 2018, 11, 1756285617749134. [Google Scholar] [CrossRef] [Green Version]
- Mantegazza, R.; Antozzi, C. From Traditional to Targeted Immunotherapy in Myasthenia Gravis: Prospects for Research. Front. Neurol. 2020, 11, 981. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C. Progress in the therapy of myasthenia gravis: Getting closer to effective targeted immunotherapies. Curr. Opin. Neurol. 2020, 33, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Litchman, T.; Roy, B.; Kumar, A.; Sharma, A.; Njike, V.; Nowak, R.J. Differential response to rituximab in anti-AChR and anti-MuSK positive myasthenia gravis patients: A single-center retrospective study. J. Neurol. Sci. 2020, 411, 116690. [Google Scholar] [CrossRef] [PubMed]
- Lazaridis, K.; Tzartos, S.J. Autoantibody Specificities in Myasthenia Gravis; Implications for Improved Diagnostics and Therapeutics. Front. Immunol. 2020, 11, 212. [Google Scholar] [CrossRef]
- Niks, E.H.; van Leeuwen, Y.; Leite, M.I.; Dekker, F.W.; Wintzen, A.R.; Wirtz, P.W.; Vincent, A.; van Tol, M.J.; Jol-van der Zijde, C.M.; Verschuuren, J.J. Clinical fluctuations in MuSK myasthenia gravis are related to antigen-specific IgG4 instead of IgG1. J. Neuroimmunol. 2008, 195, 151–156. [Google Scholar] [CrossRef]
- Huijbers, M.G.; Plomp, J.J.; van der Maarel, S.M.; Verschuuren, J.J. IgG4-mediated autoimmune diseases: A niche of antibody-mediated disorders. Ann. NY Acad. Sci. 2018, 1413, 92–103. [Google Scholar] [CrossRef]
- Rivner, M.H.; Pasnoor, M.; Dimachkie, M.M.; Barohn, R.J.; Mei, L. Muscle-Specific Tyrosine Kinase and Myasthenia Gravis Owing to Other Antibodies. Neurol. Clin. 2018, 36, 293–310. [Google Scholar] [CrossRef]
- Engel, A.G.; Arahata, K. The membrane attack complex of complement at the endplate in myasthenia gravis. Ann. NY Acad. Sci. 1987, 505, 326–332. [Google Scholar] [CrossRef]
- Rødgaard, A.; Nielsen, F.C.; Djurup, R.; Somnier, F.; Gammeltoft, S. Acetylcholine receptor antibody in myasthenia gravis: Predominance of IgG subclasses 1 and 3. Clin. Exp. Immunol. 1987, 67, 82–88. [Google Scholar]
- Bokoliya, S.; Patil, S.; Nagappa, M.; Taly, A. A Simple, Rapid and Non-Radiolabeled Immune Assay to Detect Anti-AChR Antibodies in Myasthenia Gravis. Lab. Med. 2019, 50, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Trakas, N.; Tzartos, S.J. Immunostick ELISA for rapid and easy diagnosis of myasthenia gravis. J. Immunol. Methods 2018, 460, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Zisimopoulou, P.; Brenner, T.; Trakas, N.; Tzartos, S.J. Serological diagnostics in myasthenia gravis based on novel assays and recently identified antigens. Autoimmun. Rev. 2013, 12, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.G.; Wang, Z.H.; Ma, X.W.; Zhang, D.Q.; Yang, C.S.; Shi, F.D.; Yang, L. Clinical significance of detection of antibodies to fetal and adult acetylcholine receptors in myasthenia gravis. Neurosci. Bull. 2012, 28, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Riemersma, S.; Vincent, A.; Beeson, D.; Newland, C.; Hawke, S.; Vernet-der Garabedian, B.; Eymard, B.; Newsom-Davis, J. Association of arthrogryposis multiplex congenita with maternal antibodies inhibiting fetal acetylcholine receptor function. J. Clin. Investig. 1966, 98, 2358–2363. [Google Scholar] [CrossRef]
- Saxena, A.; Stevens, J.; Cetin, H.; Koneczny, I.; Webster, R.; Lazaridis, K.; Tzartos, S.; Vrolix, K.; Nogales-Gadea, G.; Machiels, B.; et al. Characterization of an anti-fetal AChR monoclonal antibody isolated from a myasthenia gravis patient. Sci. Rep. 2017, 7, 14426. [Google Scholar] [CrossRef] [Green Version]
- Adaszewska, A.; Kalinska-Bienias, A.; Jagielski, P.; Wozniak, K.; Kowalewski, C. The use of BIOCHIP technique in diagnosis of different types of pemphigus: Vulgaris and foliaceus. J. Immunol. Methods 2019, 468, 35–39. [Google Scholar] [CrossRef]
- Tampoia, M.; Zucano, A.; Villalta, D.; Antico, A.; Bizzaro, N. Anti-skin specific autoantibodies detected by a new immunofluorescence multiplex biochip method in patients with autoimmune bullous diseases. Dermatology 2012, 225, 37–44. [Google Scholar] [CrossRef]
- Arunprasath, P.; Rai, R.; Venkataswamy, C. Comparative Analysis of BIOCHIP Mosaic-based Indirect Immunofluorescence with Direct Immunofluorescence in Diagnosis of Autoimmune Bullous Diseases: A Cross-Sectional Study. Indian Dermatol. Online J. 2021, 12, 105–109. [Google Scholar]
- van Beek, N.; Rentzsch, K.; Probst, C.; Komorowski, L.; Kasperkiewicz, M.; Fechner, K.; Bloecker, I.M.; Zillikens, D.; Stöcker, W.; Schmidt, E. Serological diagnosis of autoimmune bullous skin diseases: Prospective comparison of the BIOCHIP mosaic-based indirect immunofluorescence technique with the conventional multi-step single test strategy. Orphanet J. Rare Dis. 2019, 7, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xuan, R.R.; Yang, A.; Murrell, D.F. New biochip immunofluorescence test for the serological diagnosis of pemphigus vulgaris and foliaceus: A review of the literature. Int. J. Womens Dermatol. 2018, 4, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Xuan, R.; Melbourne, W.; Tran, K.; Murrell, D.F. Validation of the BIOCHIP test for the diagnosis of bullous pemphigoid, pemphigus vulgaris and pemphigus foliaceus. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Granieri, L.; Marnetto, F.; Valentino, P.; Frau, J.; Patanella, A.K.; Nytrova, P.; Sola, P.; Capobianco, M.; Jarius, S.; Bertolotto, A. Evaluation of a multiparametric immunofluorescence assay for standardization of neuromyelitis optica serology. PLoS ONE 2012, 7, e38896. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| ELISA Anti-AChR | ||||
|---|---|---|---|---|
| BIOCHIP IIF | Positive | Negative | Total | BIOCHIP IIF |
| Positive | 26 | 1 | 27 | Positive |
| Negative | 17 | 26 | 43 | Negative |
| Total | 43 | 27 | 70 | Total |
| ELISA anti-MuSK | ||||
|---|---|---|---|---|
| BIOCHIP IIF | Positive | Negative | Total | Kappa |
| Positive | 1 | 1 | 2 | |
| Negative | 10 | 58 | 68 | 0.11 |
| Total | 11 | 59 | 70 | |
| Name | Assay Type | Sensitivity | Detection Range | Company | Regulatory Status |
|---|---|---|---|---|---|
| Human AChR-Ab | Quantitative Sandwich | 0.04 pmol/mL | 0.06–4 pmol/mL | MyBioSource | RUO |
| Anti-AChR Ab | Competitive | 0.23 nmol/L | 0.2–20 IU/mL | Eagle Bioscience | RUO |
| Human Anti-AChR Ab | Indirect | 0.938 ng/mL | 1.563–100 ng/mL | Biomatik | RUO |
| Medizym® Anti-AChR Ab | Competitive | 0.23 U/mL | 0.2–20 U/mL | Medipan | IVD |
| Anti-AChR Ab | Competitive | 0.25 nmol/L | 0.2–20 nmol/L | RSR Limited | IVD |
| Anti-AChR Ab | Indirect | 0.11 nmol/L | 0–8 nmol/L | Euroimmun | IVD |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gambino, C.M.; Agnello, L.; Lo Sasso, B.; Scazzone, C.; Giglio, R.V.; Candore, G.; Ciaccio, A.M.; Di Stefano, V.; Brighina, F.; Vidali, M.; et al. Comparative Analysis of BIOCHIP Mosaic-Based Indirect Immunofluorescence with Enzyme-Linked Immunosorbent Assay for Diagnosing Myasthenia Gravis. Diagnostics 2021, 11, 2098. https://doi.org/10.3390/diagnostics11112098
Gambino CM, Agnello L, Lo Sasso B, Scazzone C, Giglio RV, Candore G, Ciaccio AM, Di Stefano V, Brighina F, Vidali M, et al. Comparative Analysis of BIOCHIP Mosaic-Based Indirect Immunofluorescence with Enzyme-Linked Immunosorbent Assay for Diagnosing Myasthenia Gravis. Diagnostics. 2021; 11(11):2098. https://doi.org/10.3390/diagnostics11112098
Chicago/Turabian StyleGambino, Caterina Maria, Luisa Agnello, Bruna Lo Sasso, Concetta Scazzone, Rosaria Vincenza Giglio, Giuseppina Candore, Anna Maria Ciaccio, Vincenzo Di Stefano, Filippo Brighina, Matteo Vidali, and et al. 2021. "Comparative Analysis of BIOCHIP Mosaic-Based Indirect Immunofluorescence with Enzyme-Linked Immunosorbent Assay for Diagnosing Myasthenia Gravis" Diagnostics 11, no. 11: 2098. https://doi.org/10.3390/diagnostics11112098
APA StyleGambino, C. M., Agnello, L., Lo Sasso, B., Scazzone, C., Giglio, R. V., Candore, G., Ciaccio, A. M., Di Stefano, V., Brighina, F., Vidali, M., & Ciaccio, M. (2021). Comparative Analysis of BIOCHIP Mosaic-Based Indirect Immunofluorescence with Enzyme-Linked Immunosorbent Assay for Diagnosing Myasthenia Gravis. Diagnostics, 11(11), 2098. https://doi.org/10.3390/diagnostics11112098