
Profile of Urinary Cytokines in Kawasaki Disease: Non-Invasive Markers

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Enrollment
2.2. Measurement of Urinary Cytokines
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data of Included Patients
3.2. Cytokines Expression in Urine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kawasaki, T.; Kosaki, F.; Okawa, S.; Shigematsu, I.; Yanagawa, H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics 1974, 54, 271–276. [Google Scholar]
- Liang, C.D.; Kuo, H.C.; Yang, K.D.; Wang, C.L.; Ko, S.F. Coronary artery fistula associated with Kawasaki disease. Am. Heart J. 2009, 157, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.C.; Glodé, M.P. Kawasaki syndrome. Lancet 2004, 364, 533–544. [Google Scholar] [CrossRef]
- Newburger, J.W.; Takahashi, M.; Beiser, A.S.; Burns, J.C.; Bastian, J.; Chung, K.J.; Colan, S.D.; Duffy, C.E.; Fulton, D.R.; Glode, M.P.; et al. A single intravenous infusion of gamma globulin as compared with four infusions in the treatment of acute Kawasaki syndrome. N. Engl. J. Med. 1991, 324, 1633–1639. [Google Scholar] [CrossRef]
- Rowley, A.H. Kawasaki disease: Novel insights into etiology and genetic susceptibility. Annu. Rev. Med. 2011, 62, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Park, S.Y.; Choi, K.H.; Park, Y.H.; Lee, Y.H. Clinical characteristics of Kawasaki disease with sterile pyuria. Korean J. Pediatr. 2013, 56, 13–18. [Google Scholar] [CrossRef]
- Subcommittee on Urinary Tract Infection; Steering Committee on Quality Improvement and Management; Roberts, K.B. Urinary tract infection: Clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef]
- Maury, C.P.; Salo, E.; Pelkonen, P. Circulating interleukin-1 beta in patients with Kawasaki disease. N. Engl. J. Med. 1988, 319, 1670–1671. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.M.H.; Tseng, W.N.; Ko, C.H.; Pan, H.M.; Hsieh, K.S.; Kuo, H.C. Th17- and Treg-related cytokine and mRNA expression are associated with acute and resolving Kawasaki disease. Allergy 2015, 70, 310–318. [Google Scholar] [CrossRef]
- Ko, T.M.; Kuo, H.C.; Chang, J.S.; Chen, S.P.; Liu, Y.M.; Chen, H.W.; Tsai, F.J.; Lee, Y.C.; Chen, C.H.; Wu, J.Y.; et al. CXCL10/IP-10 is a biomarker and mediator for Kawasaki disease. Circ. Res. 2015, 116, 876–883. [Google Scholar] [CrossRef]
- Jibiki, T.; Terai, M.; Kohno, Y. High concentrations of interleukin-8 and monocyte chemoattractant protein-1 in urine of patients with acute Kawasaki disease. Eur. J. Pediatr. 2004, 163, 749–750. [Google Scholar] [CrossRef]
- Wu, J.M.; Chiou, Y.Y.; Hung, W.P.; Chiu, N.T.; Chen, M.J.; Wang, J.N. Urinary cytokines and renal Doppler study in Kawasaki disease. J. Pediatr. 2010, 156, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Ohta, K.; Seno, A.; Shintani, N.; Kato, E.; Yachie, A.; Seki, H.; Miyawaki, T.; Taniguchi, N. Increased levels of urinary interleukin-6 in Kawasaki disease. Eur. J. Pediatr. 1993, 152, 647–649. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.L.; Huang, H.C.; Ou-Yang, M.C.; Chen, F.S.; Chung, M.Y.; Chen, C.C. A novel method to detect bacterial infection in premature infants: Using a combination of inflammatory markers in blood and saliva. J. Microbiol. Immunol. Infect. 2020, 53, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.; Varro, R.; Sepulveda, H.; Ember, J.A.; Apgar, J.; Wilson, J.; Lowe, L.; Chen, R.; Shivraj, L.; Agadir, A.; et al. Cytometric bead array: A multiplexed assay platform with applications in various areas of biology. Clin. Immunol. 2004, 110, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Lin, I.C.; Kuo, H.-C.; Lin, Y.-J.; Wang, F.-S.; Wang, L.; Huang, S.-C.; Chien, S.-J.; Huang, C.-F.; Wang, C.-L.; Yu, H.-R.; et al. Augmented TLR2 Expression on Monocytes in both Human Kawasaki Disease and a Mouse Model of Coronary Arteritis. PLoS ONE 2012, 7, e38635. [Google Scholar] [CrossRef] [PubMed]
- Sohn, M.H.; Noh, S.Y.; Chang, W.; Shin, K.M.; Kim, D.S. Circulating interleukin 17 is increased in the acute stage of Kawasaki disease. Scand. J. Rheumatol. 2003, 32, 364–366. [Google Scholar] [CrossRef]
- Terai, M.; Jibiki, T.; Harada, A.; Terashima, Y.; Yasukawa, K.; Tateno, S.; Hamada, H.; Oana, S.; Niimi, H.; Matsushima, K. Dramatic decrease of circulating levels of monocyte chemoattractant protein-1 in Kawasaki disease after gamma globulin treatment. J. Leukoc. Biol. 1999, 65, 566–572. [Google Scholar] [CrossRef]
- Kuo, H.C.; Wang, C.L.; Liang, C.D.; Yu, H.R.; Huang, C.F.; Wang, L.; Hwang, K.P.; Yang, K.D. Association of lower eosinophil-related T helper 2 (Th2) cytokines with coronary artery lesions in Kawasaki disease. Pediatr. Allergy Immunol. 2009, 20, 266–272. [Google Scholar] [CrossRef]
- Luster, A.D.; Ravetch, J.V. Biochemical characterization of a gamma interferon-inducible cytokine (IP-10). J. Exp. Med. 1987, 166, 1084–1097. [Google Scholar] [CrossRef]
- Vazirinejad, R.; Ahmadi, Z.; Kazemi Arababadi, M.; Hassanshahi, G.; Kennedy, D. The biological functions, structure and sources of CXCL10 and its outstanding part in the pathophysiology of multiple sclerosis. Neuroimmunomodulation 2014, 21, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Schulte, D.J.; Yilmaz, A.; Shimada, K.; Fishbein, M.C.; Lowe, E.L.; Chen, S.; Wong, M.; Doherty, T.M.; Lehman, T.; Crother, T.R.; et al. Involvement of innate and adaptive immunity in a murine model of coronary arteritis mimicking Kawasaki disease. J. Immunol. 2009, 183, 5311–5318. [Google Scholar] [CrossRef]
- Hirao, J.; Hibi, S.; Andoh, T.; Ichimura, T. High levels of circulating interleukin-4 and interleukin-10 in Kawasaki disease. Int. Arch. Allergy Immunol. 1997, 112, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Mori, M.; Kobayashi, Y.; Miyamae, T.; Imagawa, T.; Okuyama, T.; Kurozumi, H.; Yokota, S. Intravenous gamma-globulin therapy improves hypercytokinemia in the acute phase of Kawasaki disease. Mod. Rheumatol. 2004, 14, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Lin, C.C.; Hwang, B.; Chiang, B.N. The changes of interleukin-2, tumour necrotic factor and gamma-interferon production among patients with Kawasaki disease. Eur. J. Pediatr. 1991, 150, 179–182. [Google Scholar] [CrossRef]
- Hsu, Y.W.; Lu, H.F.; Chou, W.H.; Kuo, H.C.; Chang, W.C. Functional Correlations between CXCL10/IP10 Gene Polymorphisms and Risk of Kawasaki Disease. Pediatr. Allergy Immunol. 2020, 32, 363–370. [Google Scholar] [CrossRef]
- Poole, S.; Bird, T.A.; Selkirk, S.; Gaines-Das, R.E.; Choudry, Y.; Stephenson, S.L.; Kenny, A.J.; Saklatvaa, J. Fate of injected interleukin 1 in rats: Sequestration and degradation in the kidney. Cytokine 1990, 2, 416–422. [Google Scholar] [CrossRef]
- Bocci, V.; Paulesu, L.; Pessina, G.P. The renal catabolic pathways of cytokines. Contrib. Nephrol. 1993, 101, 55–60. [Google Scholar] [CrossRef]
- McBride, W.T.; McBride, S.J. The balance of pro- and anti-inflammatory cytokines in cardiac surgery. Curr. Opin. Anesthesiol. 1998, 11, 15–22. [Google Scholar] [CrossRef]
- Fukazawa, R.; Ogawa, S. Long-term prognosis of patients with Kawasaki disease: At risk for future atherosclerosis? J. Nippon Med. Sch. 2009, 76, 124–133. [Google Scholar] [CrossRef][Green Version]
- Denby, K.J.; Clark, D.E.; Markham, L.W. Management of Kawasaki disease in adults. Heart 2017, 103, 1760–1769. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.H.; Chen, H.C.; Yeh, S.J.; Lin, M.T.; Huang, S.C.; Huang, S.K. Prevalence and the long-term coronary risks of patients with Kawasaki disease in a general population <40 years: A national database study. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Adjagba, P.M.; Desjardins, L.; Fournier, A.; Spigelblatt, L.; Montigny, M.; Dahdah, N. N-terminal pro-brain natriuretic peptide in acute Kawasaki disease correlates with coronary artery involvement. Cardiol. Young 2015, 25, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.H.; Chen, K.D.; Lo, M.H.; Cai, X.Y.; Chang, L.S.; Kuo, Y.H.; Huang, W.D.; Kuo, H.C. Decreased DNA methyltransferases expression is associated with coronary artery lesion formation in Kawasaki disease. Int. J. Med. Sci. 2019, 16, 576–582. [Google Scholar] [CrossRef]
- Hui-Yuen, J.S.; Duong, T.T.; Yeung, R.S. TNF-alpha is necessary for induction of coronary artery inflammation and aneurysm formation in an animal model of Kawasaki disease. J. Immunol. 2006, 176, 6294–6301. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, W.; Gong, F.; Fu, S.; Zhang, Q.; Hu, J.; Qi, Y.; Xie, C.; Zhang, Y. Evaluation of intravenous immunoglobulin resistance and coronary artery lesions in relation to Th1/Th2 cytokine profiles in patients with Kawasaki disease. Arthritis Rheum. 2013, 65, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Thornhill, M.H.; Haskard, D.O. IL-4 regulates endothelial cell activation by IL-1, tumor necrosis factor, or IFN-gamma. J. Immunol. 1990, 145, 865–872. [Google Scholar]
- Brown, M.A.; Hural, J. Functions of IL-4 and Control of Its Expression. Crit. Rev. Immunol. 2017, 37, 181–212. [Google Scholar] [CrossRef]
- Schleimer, R.P.; Sterbinsky, S.A.; Kaiser, J.; Bickel, C.A.; Klunk, D.A.; Tomioka, K.; Newman, W.; Luscinskas, F.W.; Gimbrone, M.A., Jr.; McIntyre, B.W. IL-4 induces adherence of human eosinophils and basophils but not neutrophils to endothelium. Association with expression of VCAM-1. J. Immunol. 1992, 148, 1086–1092. [Google Scholar]
- Suzuki, H.; Uemura, S.; Tone, S.; Iizuka, T.; Koike, M.; Hirayama, K.; Maeda, J. Effects of immunoglobulin and gamma-interferon on the production of tumour necrosis factor-alpha and interleukin-1 beta by peripheral blood monocytes in the acute phase of Kawasaki disease. Eur. J. Pediatr. 1996, 155, 291–296. [Google Scholar] [CrossRef]
- Leung, D.Y.; Cotran, R.S.; Kurt-Jones, E.; Burns, J.C.; Newburger, J.W.; Pober, J.S. Endothelial cell activation and high interleukin-1 secretion in the pathogenesis of acute Kawasaki disease. Lancet 1989, 2, 1298–1302. [Google Scholar] [CrossRef]
- Okitsu-Negishi, S.; Furusawa, S.; Kawa, Y.; Hashira, S.; Ito, S.; Hiruma, F.; Mizoguchi, M.; Yoshino, K.; Abe, T. Suppressive effect of intravenous immunoglobulins on the activity of interleukin-1. Immunol. Res. 1994, 13, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Arend, W.P.; Leung, D.Y. IgG induction of IL-1 receptor antagonist production by human monocytes. Immunol. Rev. 1994, 139, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Popper, S.J.; Shimizu, C.; Shike, H.; Kanegaye, J.T.; Newburger, J.W.; Sundel, R.P.; Brown, P.O.; Burns, J.C.; Relman, D.A. Gene-expression patterns reveal underlying biological processes in Kawasaki disease. Genome Biol. 2007, 8, R261. [Google Scholar] [CrossRef]
- Hacham, M.; Argov, S.; White, R.M.; Segal, S.; Apte, R.N. Different patterns of interleukin-1alpha and interleukin-1beta expression in organs of normal young and old mice. Eur. Cytokine Netw. 2002, 13, 55–65. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FC (n = 42) | KD (n = 37) | UTI (n = 28) | p * Value | ||||
|---|---|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Median (IQR) | |||||
| All (n = 37) | CAL (n = 10) | No CAL (n = 27) | p Value | ||||
| Age (months) | 40.59 (13.50, 60.25) | 23.25 (8.50, 26.50) | 9.00 (6.50, 23.75) | 19.00 (11.00, 27.00) | 0.105 | 3.67 (1.68, 3.90) | <0.001 |
| Gender (F/M), n | 21/21 | 11/26 | 0/10 | 11/16 | 0.018 | 8/20 | 0.095 |
| Body weight (kg) | 15.87 (10.63, 7.73) | 12.07 (8.65, 11.45) | 10.20 (7.43, 10.38) | 10.20 (8.68, 11.58) | 0.158 | 6.02 (5.07, 6.90) | <0.001 |
| WBC (1000/μL) | 10.69 (6.40, 14.40) | 12.43 (9.40, 14.70) | 15.05 (9.88, 19.20) | 12.85 (10.55, 14.48) | 0.775 | 14.55 (12.95, 17.70) | 0.003 |
| Hemoglobin (g/dL) | 12.26 (11.60, 12.90) | 11.24 (10.50, 11.95) | 10.35 (9.88, 10.75) | 11.70 (10.88, 12.03) | 0.062 | 11.80 (10.10, 13.78) | 0.001 |
| Hematocrit (%) | 36.36 (34.4, 38.50) | 34.00 (31.80, 36.00) | 31.80 (31.30, 32.65) | 34.20 (32.65, 36.65) | 0.169 | 34.31 (29.98, 36.08) | 0.001 |
| Platelet (1000/μL) | 228.7 (180.0, 279.0) | 410.8 (299.0, 485.0) | 463.0 (356.0, 597.5) | 353.0 (285.8, 495.0) | 0.371 | 380.7 (323.0, 450.5) | <0.001 |
| BUN (mg/dL) | 8.56 (5.50, 11.00) | 7.22 (4.00, 9.00) | 5.50 (4.25, 9.00) | 7.00 (4.00, 9.00) | 0.621 | 7.65 (6.00, 8.25) | 0.261 |
| Cr (mg/dL) | 0.39 (0.34, 0.49) | 0.32 (0.22, 0.37) | 0.24 (0.21, 0.32) | 0.30 (0.26, 0.41) | 0.106 | 0.29 (0.22, 0.31) | 0.007 |
| CRP (mg/L) | 32.58 (4.48, 46.43) | 65.78 (22.45, 100.95) | 87.10 (61.03, 128.65) | 49.50 (16.95, 80.38) | 0.044 | 30.53 (6.70, 48.95) | 0.001 |
| U-WBC (/uL) | 2.95 (0.00, 3.00) | 40.15 (0.00, 31.50) | 10.50 (0.75, 42.75) | 4.50 (0.00, 27.75) | 0.223 | 98.77 (10.50, 171.0) | <0.001 |
| U-RBC (/uL) | 2.79 (0.00, 3.00) | 5.23 (0.00, 6.00) | 3.00 (0.75, 6.00) | 1.50 (0.00, 6.75) | 0.460 | 41.68 (6.75, 53.25) | <0.001 |
| U-Cr (mg/dL) | 54.34 (29.40, 70.05) | 24.96 (9.09, 29.60) | 13.09 (3.11, 26.54) | 21.67 (11.23, 36.89) | 0.158 | 13.29 (6.22, 15.13) | <0.001 |
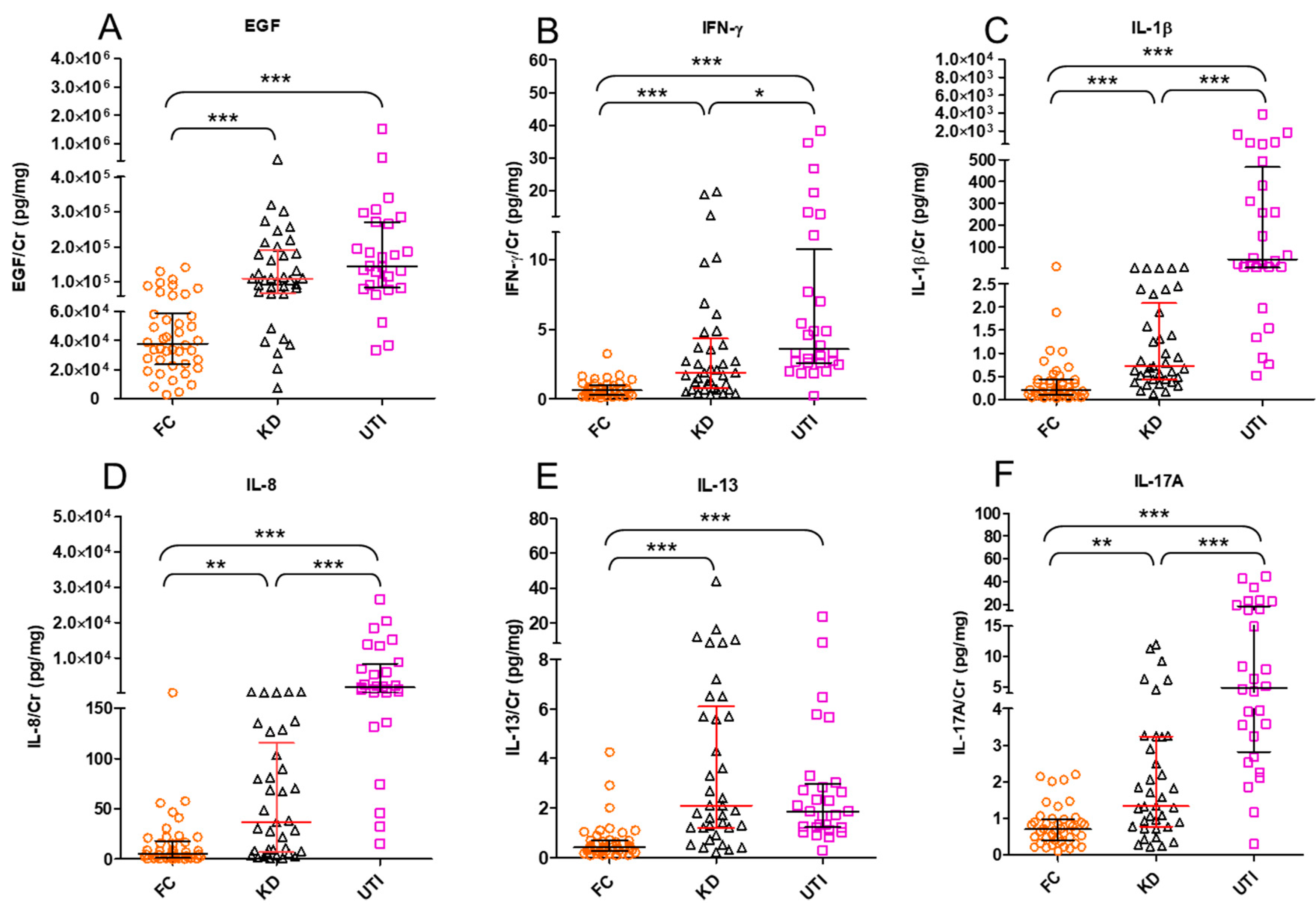
| Cytokines (pg/mg) | FC (n= 42) | KD (n= 37) | UTI (n= 28) |
|---|---|---|---|
| EGF | 38,043 (23,587, 59,132) *** | 109,703 (68,870, 191,054) | 144,115 (84,484, 269,474) |
| IFN-γ | 0.65 (0.28, 1.00) *** | 1.90 (0.75, 4.35) | 3.59 (2.59, 10.74) * |
| IL-1β | 0.21 (0.1, 0.43) *** | 0.72 (0.44, 2.08) | 43.32 (6.20, 465.3) *** |
| IL-2 | 0.33 (0.16, 0.51) ** | 0.88 (0.42, 1.66) | 0.69 (0.34, 1.01) |
| IL-4 | 2.52 (1.15, 4.67) *** | 9.32 (6.42, 16.16) | 9.04 (5.28, 22.44) |
| IL-5 | 0.48 (0.29, 0.66) *** | 2.00 (1.41, 3.01) | 1.50 (0.65, 2.25) |
| IL-6 | 1.32 (0.55, 4.68) ** | 81.71 (10.54, 219.8) | 5.28 (2.14, 12.36) *** |
| IL-8 | 5.34 (1.42, 17.93) ** | 36.81 (6.95, 115.4) | 1713 (180.7, 8324) *** |
| IL-9 | 2.45 (1.30, 3.80) *** | 8.98 (5.27, 14.20) | 5.85 (3.73, 10.49) |
| IL-10 | 1.7 (0.85, 2.89) *** | 10.17 (7.06, 27.18) | 6.00 (2.80, 16.35) |
| IL-13 | 0.40 (0.25, 0.70) *** | 2.10 (1.20, 6.10) | 1.86 (1.22, 2.98) |
| IL-17A | 0.70 (0.39, 0.99) ** | 1.34 (0.78, 3.24) | 4.88 (2.82, 18.69) *** |
| IL-33 | 18.43 (7.32, 38.29) ** | 354 (229, 668.8) | 54.50 (17.85, 165.7) *** |
| IP-10 | 279.4 (41.88, 920) * | 1259 (264.7, 5723) | 1312 (107.1, 5115) |
| MCP-1 | 849.1 (355.8, 1926) | 4836 (2440, 14,231) | 2441 (667.3, 3469) ** |
| MIP-1β | 6.90 (2.45, 13.20) *** | 87.66 (27.70, 126.3) | 31.74 (12.81, 50.46) ** |
| TNF-α | 0.50 (0.26, 0.92) *** | 12.47 (2.05, 68.96) | 1.16 (0.73, 2.89) *** |
| VEGF | 45.58 (2.33, 103.8) *** | 258.6 (132.1, 498.4) | 145.4 (64.00, 374.4) |
| Cytokines (pg/mg) | Groups | Initial Analysis | Logistic Regression (Adjusting for Age) | |||||
|---|---|---|---|---|---|---|---|---|
| Median | IQR | P | OR | 95% CI | p * | |||
| Lower | Upper | |||||||
| EGF | FC | 38,043 | (23,587, 59,132) | <0.001 | 0.997 | 0.995 | 0.998 | <0.001 |
| KD | 109,703 | (68,870, 191,054) | ||||||
| UTI | 144,115 | (84,484, 269,474) | 1.000 | 1.000 | 1.000 | 0.827 | ||
| IFN-γ | FC | 0.65 | (0.28, 1.00) | <0.001 | 0.216 | 0.097 | 0.479 | <0.001 |
| KD | 1.90 | (0.75, 4.35) | ||||||
| UTI | 3.59 | (2.59, 10.74) | 1.008 | 0.927 | 1.096 | 0.853 | ||
| IL-1β | FC | 0.21 | (0.10, 0.43) | <0.001 | 0.666 | 0.385 | 1.154 | 0.148 |
| KD | 0.72 | (0.44, 2.08) | ||||||
| UTI | 43.32 | (6.20, 465.3) | 1.282 | 1.008 | 1.631 | 0.043 | ||
| IL-8 | FC | 5.34 | (1.42, 17.93) | <0.001 | 0.978 | 0.963 | 0.994 | 0.006 |
| KD | 36.81 | (6.95, 115.4) | ||||||
| UTI | 1713 | (180.7, 8324) | 1.007 | 0.999 | 1.014 | 0.079 | ||
| IL-13 | FC | 0.40 | (0.25, 0.70) | <0.001 | 0.258 | 0.122 | 0.543 | <0.001 |
| KD | 2.10 | (1.20, 6.10) | ||||||
| UTI | 1.86 | (1.22, 2.98) | 0.904 | 0.783 | 1.043 | 0.165 | ||
| IL-17A | FC | 0.70 | (0.39, 0.99) | <0.001 | 0.286 | 0.136 | 0.602 | 0.001 |
| KD | 1.34 | (0.78, 3.24) | ||||||
| UTI | 4.88 | (2.82, 18.69) | 1.101 | 0.951 | 1.274 | 0.198 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, H.-C.; Kuo, H.-C.; Yu, H.-R.; Huang, H.-C.; Chang, J.-C.; Lin, I.-C.; Chen, I.-L. Profile of Urinary Cytokines in Kawasaki Disease: Non-Invasive Markers. Diagnostics 2021, 11, 1857. https://doi.org/10.3390/diagnostics11101857
Huang H-C, Kuo H-C, Yu H-R, Huang H-C, Chang J-C, Lin I-C, Chen I-L. Profile of Urinary Cytokines in Kawasaki Disease: Non-Invasive Markers. Diagnostics. 2021; 11(10):1857. https://doi.org/10.3390/diagnostics11101857
Chicago/Turabian StyleHuang, Hsin-Chun, Ho-Chang Kuo, Hong-Ren Yu, Hui-Chen Huang, Jen-Chieh Chang, I-Chun Lin, and I-Lun Chen. 2021. "Profile of Urinary Cytokines in Kawasaki Disease: Non-Invasive Markers" Diagnostics 11, no. 10: 1857. https://doi.org/10.3390/diagnostics11101857
APA StyleHuang, H.-C., Kuo, H.-C., Yu, H.-R., Huang, H.-C., Chang, J.-C., Lin, I.-C., & Chen, I.-L. (2021). Profile of Urinary Cytokines in Kawasaki Disease: Non-Invasive Markers. Diagnostics, 11(10), 1857. https://doi.org/10.3390/diagnostics11101857