Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines


 ,
,  ,
, 
 ,
,  ,
,  and
and
Abstract
1. Introduction
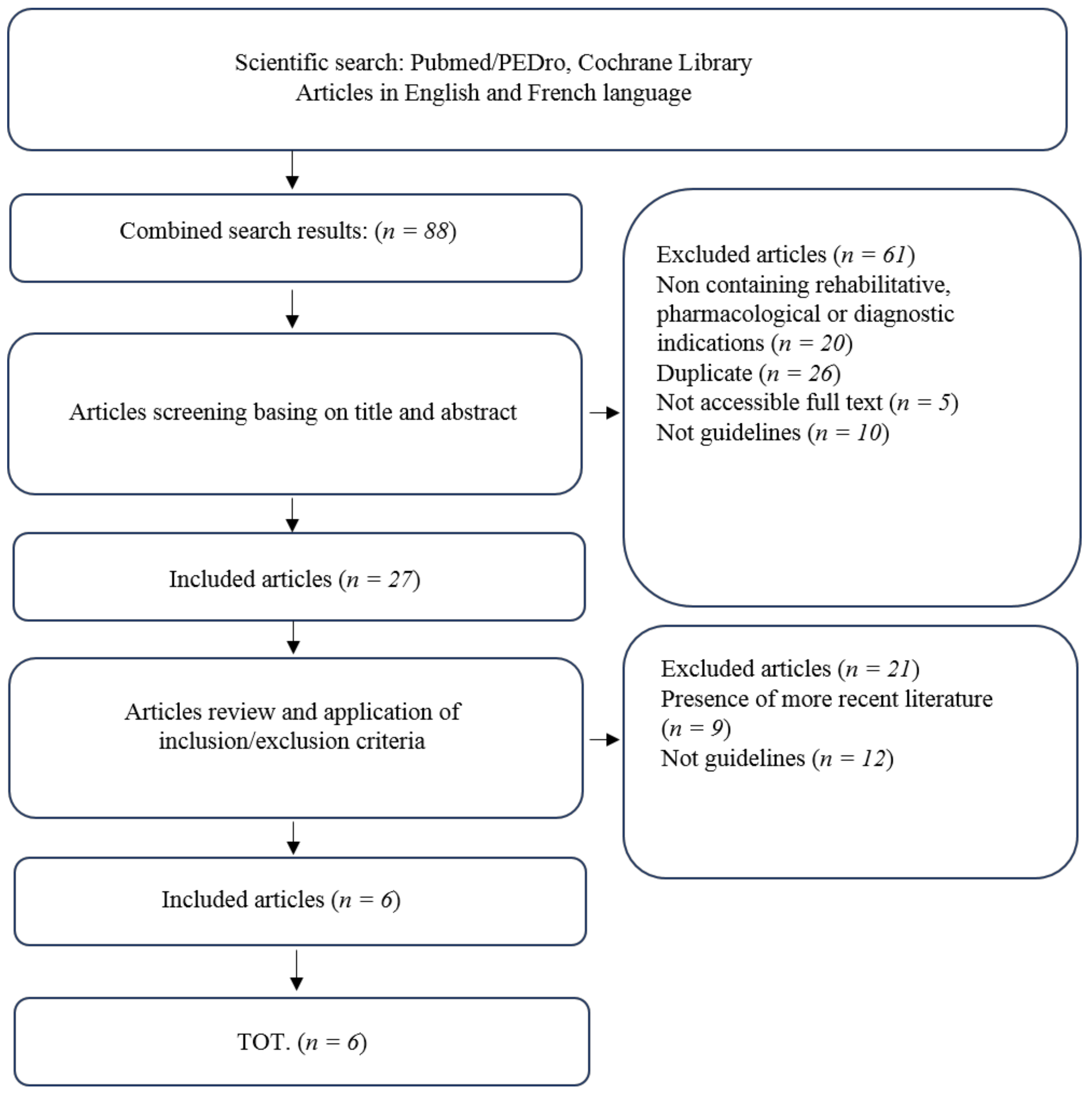
2. Materials and Methods
PICO
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Scholz, J.; Finnerup, N.B.; Attal, N.; Aziz, Q.; Baron, R.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Cruccu, G.; Davis, K.D.; et al. Classification Committee of the Neuropathic Pain Special Interest Group (NeuPSIG). The IASP classification of chronic pain for ICD-11: Chronic neuropathic pain. Pain 2019, 160, 53–59. [Google Scholar] [CrossRef]
- Mannion, R.; Woolf, C. Pain mechanisms and management: A central perspective. Clin. J. Pain 2000, 16, 144–156. [Google Scholar] [CrossRef]
- Binder, A.; Baron, R. The Pharmacological Therapy of Chronic Neuropathic Pain. Dtsch. Arztebl. Int. 2016, 113, 616–625. [Google Scholar] [CrossRef]
- Deng, Y.; Luo, L.; Hu, Y.; Fang, K.; Liu, J. Clinical practice guidelines for the management of neuropathic pain: A systematic review. BMC Anesthesiol. 2016, 16, 12. [Google Scholar] [CrossRef]
- Van Hecke, O.; Austin, S.K.; Khan, R.A.; Smith, B.H.; Torrance, N. Neuropathic pain in the general population: A systematic review of epidemiological studies. Pain 2014, 155, 654–662. [Google Scholar] [CrossRef]
- Bates, D.; Schultheis, B.C.; Hanes, M.C.; Jolly, S.M.; Chakravarthy, K.V.; Deer, T.R.; Levy, R.M.; Hunter, C.W. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. (Malden Mass.) 2019, 20 (Suppl. 1), S2–S12. [Google Scholar] [CrossRef]
- Zilliox, L.A. Neuropathic Pain. Contin. (Minneap. Minn.) 2017, 23, 512–532. [Google Scholar]
- Duehmke, R.M.; Derry, S.; Wiffen, P.J.; Bell, R.F.; Aldington, D.; Moore, R.A. Tramadol for neuropathic pain in adults. Cochrane Database Syst. Rev. 2017, 6, CD003726. [Google Scholar]
- Masiero, S.; Litwocenko, S.; Agostini, F. On behalf section of Rehabilitation in Environmental Thermal for Italian Society of Physical Medicine and Rehabilitation. Rehabilitation in an Italian thermal setting: A new therapeutic strategy for patients with musculoskeletal disability-the results of an Italian survey. Int. J. Biometeorol. 2020, 64, 951–954. [Google Scholar]
- Seccia, R.; Boresta, M.; Fusco, F.; Tronci, E.; Di Gemma, E.; Palagi, L.; Mangone, M.; Agostini, F.; Bernetti, A.; Santilli, V.; et al. Data of patients undergoing rehabilitation programs. Data Brief. 2020, 30, 105419. [Google Scholar]
- Noriko, N.; Masahiro, N. Management of neuropathic pain. J. Gen. Fam. Med. 2017, 18, 56–60. [Google Scholar]
- Acevedo, J.C.; Amaya, A.; Casasola, O.; Chinchilla, N.; De Giorgis, M.; Florez, S.; Genis, M.A.; Gomez-Barrios, J.V.; Hernández, J.J.; Ibarra, E.; et al. Guidelines for the diagnosis and management of neuropathic pain: Consensus of a group of Latin American experts. J. Pain Palliat. Care Pharmacother. 2009, 23, 261–281. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Scholz, J.; Attal, N.; Baron, R.; Haanpää, M.; Hansson, P.; Raja, S.N.; Rice, A.S.; Rief, W.; Rowbotham, M.C.; et al. Neuropathic pain needs systematic classification. Eur. J. Pain 2013, 17, 953–956. [Google Scholar] [CrossRef]
- Haanpää, M.; Attal, N.; Backonja, M.; Baron, R.; Bennett, M.; Bouhassira, D.; Cruccu, G.; Hansson, P.; Haythornthwaite, J.A.; Iannetti, G.D.; et al. NeuPSIG guidelines on neuropathic pain assessment. Pain 2011, 152, 14–27. [Google Scholar] [CrossRef]
- Casale, R.; La Manna, A.; Salvini, S.; Maini, M.; Ceccherelli, F.; Frazzitta, G. La riabilitazione delle neuropatie periferiche. Indicazioni per un percorso diagnostico-riabilitativo [Peripheral neuropathy rehabilitation. Indications for a diagnostic-rehabilitation approach]. G. Ital. Med. Lav. Ergon. 2003, 25, 456–464. [Google Scholar] [PubMed]
- Watson, J.C.; Dyck, P.J. Peripheral Neuropathy: A Practical Approach to Diagnosis and Symptom Management. Mayo Clin. Proc. 2015, 90, 940–951. [Google Scholar] [CrossRef]
- Pogemiller, K.; Garibay, E.; Pierz, K.; Acsadi, G.; Õunpuu, S. Comparison of gait patterns and functional measures between Charcot-Marie-Tooth disease type I and II in children to young adults. Gait Posture 2020, 77, 236–242. [Google Scholar] [CrossRef]
- Henderson, A.D.; Johnson, A.W.; Ridge, S.T.; Egbert, J.S.; Curtis, K.P.; Berry, L.J.; Bruening, D.A. Diabetic Gait Is Not Just Slow Gait: Gait Compensations in Diabetic Neuropathy. J. Diabetes Res. 2019, 2019, 4512501. [Google Scholar] [CrossRef]
- Gnanasundaram, S.; Ramalingam, P.; Das, B.N.; Viswanathan, V. Gait changes in persons with diabetes: Early risk marker for diabetic foot ulcer. Foot Ankle Surg. 2020, 26, 163–168. [Google Scholar] [CrossRef]
- Basic-Kes, V.; Demarin, V. Recommendations for treatment of neuropathic pain. Acta Med. Croat. 2008, 62, 237–240. [Google Scholar]
- Freynhagen, R.; Bennett, M. Diagnosis and management of neuropathic pain. BMJ 2009, 339, 3002. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Cruccu, G.; Aziz, T.Z.; Garcia-Larrea, L.; Hansson, P.; Jensen, T.S.; Lefaucheur, J.P.; Simpson, B.A.; Taylor, R.S. EFNS guidelines on neurostimulation therapy for neuropathic pain. Eur. J. Neurol. 2007, 14, 952–970. [Google Scholar] [CrossRef]
- Demarin, V.; Basić-Kes, V.; Zavoreo, I.; Bosnar-Puretić, M.; Rotim, K.; Lupret, V.; Perić, M.; Ivanec, Z.; Fumić, L.; Lusić, I.; et al. Recommendations for neuropathic pain treatment. Acta Clin. Croat. 2008, 47, 181–191. [Google Scholar]
- Martinez, V.; Attal, N.; Bouhassira, D.; Lantéri-Minet, M. Chronic neuropathic pain: Diagnosis, evaluation and treatment in outpatient services. Guidelines for clinical practice of the French Society for the Study and Treatment of Pain. Douleur Analg. 2010, 23, 51–66. [Google Scholar] [CrossRef]
- Bril, V.; England, J.; Franklin, G.M.; Backonja, M.; Cohen, J.; Del Toro, D.; Feldman, E.; Iverson, D.J.; Perkins, B.; Russell, J.W.; et al. Evidence-based guideline: Treatment of painful diabetic neuropathy: Report of the American Academy of Neurology, the American Association of Neuromuscular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Neurology 2011, 76, 1758–1765. [Google Scholar] [CrossRef]
- Chetty, S.; Baalbergen, E.; Bhigjee, A.I.; Kamerman, P.; Ouma, J.; Raath, R.; Raff, M.; Salduker, S. Clinical practice guidelines for management of neuropathic pain: Expert panel recommendations for South Africa. S. Afr. Med. J. 2012, 102, 312–325. [Google Scholar] [CrossRef]
- Cohen, S.P.; Hooten, W.M. Advances in the diagnosis and management of neck pain. BMJ 2017, 358, j3221. [Google Scholar] [CrossRef]
- Damiani, C.; Mangone, M.; Paoloni, M.; Goffredo, M.; Franceschini, M.; Servidio, M.; Pournajaf, S.; Santilli, V.; Agostini, F.; Bernetti, A. Trade-Offs with rehabilitation Effectiveness (REs) and Efficiency (REy) in a sample of Italian disabled persons in a in post-acuity rehabilitation unit. Ann Ig 2020, 32, 327–335. [Google Scholar]
- De Sire, A.; Baricich, A.; Minetto, M.A.; Cisari, C.; Invernizzi, M. Low back pain related to a sacral insufficiency fracture: Role of paravertebral oxygen-ozone therapy in a paradigmatic case of nociplastic pain. Funct. Neurol. 2019, 34, 119–122. [Google Scholar] [PubMed]


{kind=link}
| No | Title, Year | Authors | Journal | Main Findings |
|---|---|---|---|---|
| 1 | EFNS guidelines on neurostimulation therapy for neuropathic pain, 2007. | Cruccu, G.; et al [24] | Eur J Neurol | TENS may be superior to placebo and is suitable as preliminary or add-on therapy. |
| 2 | Recommendations for neuropathic pain treatment, 2008. | Demarin, V.; et al [25] | Acta Clin Croat | Multidisciplinary intervention is suggested. TENS is superior to placebo in painful diabetic neuropathy. |
| 3 | Chronic neuropathic pain: diagnosis, evaluation and treatment in outpatient services. Guidelines for clinical practice of the French Society for the Study and Treatment of Pain, 2010. | Martinez, V.; et al [26] | Douleur analg | TENS, spinal cord stimulation and cognitive behavioral therapy are suggested for neuropathic pain treatment. |
| 4 | Evidence-based guideline: Treatment of painful diabetic neuropathy: report of the American Academy of Neurology, the American Association of Neuromuscular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation, 2011. | Bril, V.; et al [27] | Neurology | Percutaneous nerve stimulation is recommended for painful diabetic neuropathy. |
| 5 | Clinical practice guidelines for management of neuropathic pain: expert panel recommendations for South Africa, 2012. | Chetty, S.; et al [28] | S Afr Med J | A combination of psychotherapy, TENS and physiotherapy is suggested for neuropathic pain treatment in a context of multidisciplinary approach. |
| 6 | Guidelines for the diagnosis and management of neuropathic pain: consensus of a group of Latin American experts, 2009. | Acevedo, J.C.; et al [12] | J Pain Palliat Care Pharmacother | An interdisciplinary management including rehabilitative intervention is suggested for neuropathic pain treatment. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernetti, A.; Agostini, F.; de Sire, A.; Mangone, M.; Tognolo, L.; Di Cesare, A.; Ruiu, P.; Paolucci, T.; Invernizzi, M.; Paoloni, M. Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines. Diagnostics 2021, 11, 74. https://doi.org/10.3390/diagnostics11010074
Bernetti A, Agostini F, de Sire A, Mangone M, Tognolo L, Di Cesare A, Ruiu P, Paolucci T, Invernizzi M, Paoloni M. Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines. Diagnostics. 2021; 11(1):74. https://doi.org/10.3390/diagnostics11010074
Chicago/Turabian StyleBernetti, Andrea, Francesco Agostini, Alessandro de Sire, Massimiliano Mangone, Lucrezia Tognolo, Annalisa Di Cesare, Pierangela Ruiu, Teresa Paolucci, Marco Invernizzi, and Marco Paoloni. 2021. "Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines" Diagnostics 11, no. 1: 74. https://doi.org/10.3390/diagnostics11010074
APA StyleBernetti, A., Agostini, F., de Sire, A., Mangone, M., Tognolo, L., Di Cesare, A., Ruiu, P., Paolucci, T., Invernizzi, M., & Paoloni, M. (2021). Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines. Diagnostics, 11(1), 74. https://doi.org/10.3390/diagnostics11010074