Body Mass Index in Patients Treated with Cabozantinib for Advanced Renal Cell Carcinoma: A New Prognostic Factor?


 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Treatment Regimens and Statistical Analysis
3. Results
3.1. Study Population
3.2. Response to Therapy and Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Cancer Facts and Statistics. Available online: http://www.cancer.org/research/cancerfactsstatistics/cancerfactsfigures2020 (accessed on 22 October 2020).
- Santoni, M.; Piva, F.; Porta, C.; Bracarda, S.; Heng, D.Y.; Matrana, M.R.; Grande, E.; Mollica, V.; Aurilio, G.; Rizzo, M.; et al. Artificial Neural Networks as a way to predict future Kidney Cancer incidence in the United States. Clin. Genitourin Cancer 2020, 10, S1558–S7673. [Google Scholar] [CrossRef] [PubMed]
- Aurilio, G.; Piva, F.; Santoni, M.; Cimadamore, A.; Sorgentoni, G.; Beltran, A.L.; Cheng, L.; Battelli, N.; Nolè, F.; Montironi, R. The Role of Obesity in Renal Cell Carcinoma Patients: Clinical-Pathological Implications. Int. J. Mol. Sci. 2019, 20, 5683. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Indini, A.; de Luca, M.; Merelli, B.; Mariuk-Jarema, A.; Teterycz, P.; Rogala, P.; Lugowska, I.; Cybulska-Stopa, B.; Labianca, A.; et al. Body mass index (BMI) and outcome of metastatic melanoma patients receiving targeted therapy and immunotherapy: A multicenter international retrospective study. J. Immunother. Cancer 2020, 8, e001117. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, A.; Ricciuti, B.; Tiseo, M.; Bria, E.; Banna, G.L.; Aerts, J.G.J.V.; Barbieri, F.; Giusti, R.; Cortinovis, D.L.; Migliorino, M.R.; et al. Baseline BMI and BMI variation during first line pembrolizumab in NSCLC patients with a PD-L1 expression ≥ 50%: A multicenter study with external validation. J. Immunother. Cancer 2020, 8, e001403. [Google Scholar] [CrossRef]
- Sanchez, A.; Furberg, H.; Kuo, F.; Vuong, L.; Ged, Y.; Patil, S.; Ostrovnaya, I.; Petruzella, S.; Reising, A.; Patel, P.; et al. Transcriptomic signatures related to the obesity paradox in patients with clear cell renal cell carcinoma: A cohort study. Lancet Oncol. 2020, 21, 283–293. [Google Scholar] [CrossRef]
- Wang, Z.; Aguilar, E.G.; Luna, J.I.; Dunai, C.; Khuat, L.T.; Le, C.T.; Mirsoian, A.; Minnar, C.M.; Stoffel, K.M.; Sturgill, I.R.; et al. Paradoxicaleffects of obesityon T cell functionduring tumor progression and PD-1 checkpoint blockade. Nat. Med. 2019, 25, 141–151. [Google Scholar] [CrossRef]
- Santoni, M.; Cortellini, A.; Buti, S. Unlocking the secret of the obesity paradox in renal tumours. Lancet Oncol. 2020, 21, 194–196. [Google Scholar] [CrossRef]
- Di Nunno, V.; Cubelli, M.; Massari, F. The role of the MET/AXL pathway as a new target for multikinase inhibitors in renal cell carcinoma. Expert Rev. Precis. Med. Drug Dev. 2017, 2, 169–175. [Google Scholar] [CrossRef]
- Santoni, M.; Heng, D.Y.; Bracarda, S.; Procopio, G.; Milella, M.; Porta, C.; Matrana, M.R.; Cartenì, G.; Crabb, S.J.; de Giorgi, U.; et al. Real-World Data on Cabozantinib in Previously Treated Patients with Metastatic Renal Cell Carcinoma: Focus on Sequences and Prognostic Factors. Cancers (Basel) 2019, 12, 84. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual; Springer International Publishing: Cham, Switzerland, 2017; ISBN 978-3-319-40617-6. [Google Scholar]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef]
- Ljungberg, B.; Albiges, L.; Ghanem, Y.A.; Bensalah, K.; Dabestani, S.; Pello, S.F.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2019 Update. Eur. Urol. 2019, 75, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; jan Bogaerts Chen, A.; Dancey, J.; Hayes, W.; et al. RECIST 1.1-Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Frontera, O.A.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef]
- Martini, D.J.; Shabto, J.M.; Liu, Y.; Carthon, B.C.; Speak, A.; Hitron, E.; Russler, G.; Caulfield, S.; Ogan, K.; Harris, W.; et al. Body mass index (BMI) and toxicities and association with clinical outcomes (CO) in metastatic renal cell carcinoma (mRCC) patients (pts) treated with cabozantinib (cabo). J. Clin. Oncol. 2019, 37 (Suppl. 7), 613. [Google Scholar] [CrossRef]
- De Giorgi, U.; Procopio, G.; Giannarelli, D.; Sabbatini, R.; Bearz, A.; Buti, S.; Basso, U.; Mitterer, M.; Ortega, C.; Bidoli, P.; et al. Association of Systemic Inflammation Index and Body Mass Index with Survival in Patients with Renal Cell Cancer Treated with Nivolumab. Clin. Cancer Res. 2019, 25, 3839–3846. [Google Scholar] [CrossRef]
- Bruna, F.A.; Romeo, L.R.; Arbocco, F.C.V.; Contador, D.; Gómez, S.; Santiano, F.; Sasso, C.V.; Zyla, L.; Fontana, C.L.; Calvo, J.C.; et al. Human renal adipose tissue from normal and tumor kidney: Its influence on renal cell carcinoma. Oncotarget 2019, 10, 5454–5467. [Google Scholar] [CrossRef]
- Arbocco, F.C.V.; Laur, J.D.L.; Romeo, L.R.; Giorlando, N.; Bruna, F.A.; Contador, D.E.; Fontana, G.L.; Santiano, F.E.; Sasso, C.V.; Zyla, L.E.; et al. Human renal adipose tissue induces the invasion and progression of renal cell carcinoma. Oncotarget 2017, 8, 94223–94234. [Google Scholar] [CrossRef]
- Horiguchi, A.; Sumitomo, M.; Asakuma, J.; Asano, T.; Zheng, R.; Asano, T.; Nanus, D.M.; Hayakawa, M. Increased serum leptin levels and over expression of leptin receptors are associated with the invasion and progression of renal cell carcinoma. J. Urol. 2006, 176, 1631–1635. [Google Scholar] [CrossRef]
- Cancello, R.; Henegar, C.; Viguerie, N.; Taleb, S.; Poitou, C.; Rouault, C.; Coupaye, M.; Pelloux, V.; Hugol, D.; Bouillot, J.C.; et al. Reduction of macrophage infiltration and chemoattractant gene expression changes in white adipose tissue of morbidly obese subjects after surgery-induced weight loss. Diabetes 2005, 54, 2277–2286. [Google Scholar] [CrossRef] [PubMed]
- Gariballa, S.; Alkaabi, J.; Yasin, J.; Essa, A.A. Total adiponectin in overweight and obese subjects and its response to visceral fat loss. BMC Endocr. Disord. 2019, 19, 55. [Google Scholar] [CrossRef] [PubMed]
- Kleinmann, N.; Duivenvoorden, W.C.M.; Hopmans, S.N.; Beatty, L.K.; Qiao, S.; Gallino, D.; Lhotak, S.; Daya, D.; Paschos, A.; Austin, R.C.; et al. Underactivation of the adiponectin-adiponectin receptor 1 axis in clear cell renal cell carcinoma: Implications for progression. Clin. Exp. Metastasis 2014, 31, 169–183. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Overall 224 (%) | BMI ≥ 25 119 (%) | BMI < 25 105 (%) | p |
|---|---|---|---|---|
| Gender | 0.657 | |||
| Male | 160 (71) | 87 (73) | 73 (70) | |
| Female | 64 (29) | 32 (27) | 32 (30) | |
| Age, years (y) | 63 | 63 | 63 | - |
| Range | 25–86 | 31–86 | 25–85 | |
| Karnofsky performance status Score > 70 | 211 (94) | 114 (96) | 97 (92) | 0.421 |
| Metastatic at diagnosis | 114 (51) | 57 (48) | 57 (54) | 0.412 |
| Past nephrectomy | 173 (77) | 92 (77) | 81 (77) | 0.897 |
| Clear cell histology | 193 (86) | 99 (83) | 94 (90) | 0.240 |
| IMDC risk stratification | 0.219 | |||
| Favorable risk | 50 (22) | 29 (24) | 21 (20) | |
| Intermediate risk | 134 (60) | 65 (55) | 69 (66) | |
| Poor risk | 40 (18) | 25 (21) | 15 (14) | |
| Common sites of metastasis | ||||
| Lung | 145 (65) | 77 (65) | 68 (65) | 0.896 |
| Lymph nodes | 115 (51) | 63 (53) | 52 (50) | 0.706 |
| Bone | 63 (28) | 34 (29) | 29 (28) | 0.993 |
| Liver | 42 (19) | 15 (13) | 20 (19) | 0.254 |
| Brain | 17 (8) | 7 (6) | 10 (10) | 0.439 |
| ≥2 Metastatic sites | 135 (60) | 69 (58) | 66 (63) | 0.458 |
| Patients | Overall | BMI ≥ 25 | BMI < 25 | p |
|---|---|---|---|---|
| 224 (%) | 119 (%) | 105 (%) | ||
| First-line therapy | 0.979 | |||
| Sunitinib | 121 (54) | 64 (54) | 57 (54) | |
| Pazopanib | 73 (33) | 38 (32) | 35 (33) | |
| Immunocombinations | 9 (4) | 5 (4) | 4 (4) | |
| Other | 21 (9) | 12 (10) | 9 (9) | |
| Second-line therapy | 0.862 | |||
| Cabozantinib | 113 (50) | 62 (52) | 51 (49) | |
| Nivolumab | 89 (40) | 46 (39) | 43 (41) | |
| Other | 22 (10) | 11 (9) | 11 (10) | |
| Third-line therapy | 0.982 | |||
| Cabozantinib | 111 (50) | 57 (48) | 54 (51) | |
| Nivolumab | 36 (16) | 19 (16) | 17 (16) | |
| Other | 15 (7) | 8 (7) | 7 (6) | |
| Response to 2nd-line cabozantinib | 0.916 | |||
| CR/PR | 31 (27) | 18 (15) | 13 (12) | |
| SD | 54 (48) | 29 (26) | 25 (22) | |
| PD | 28 (25) | 15 (13) | 13 (12) | |
| Response to 3rd-line cabozantinib | 0.127 | |||
| CR/PR | 32 (29) | 18 (16) | 14 (13) | |
| SD | 37 (33) | 14 (13) | 23 (20) | |
| PD | 42 (38) | 25 (17) | 17 (21) | |
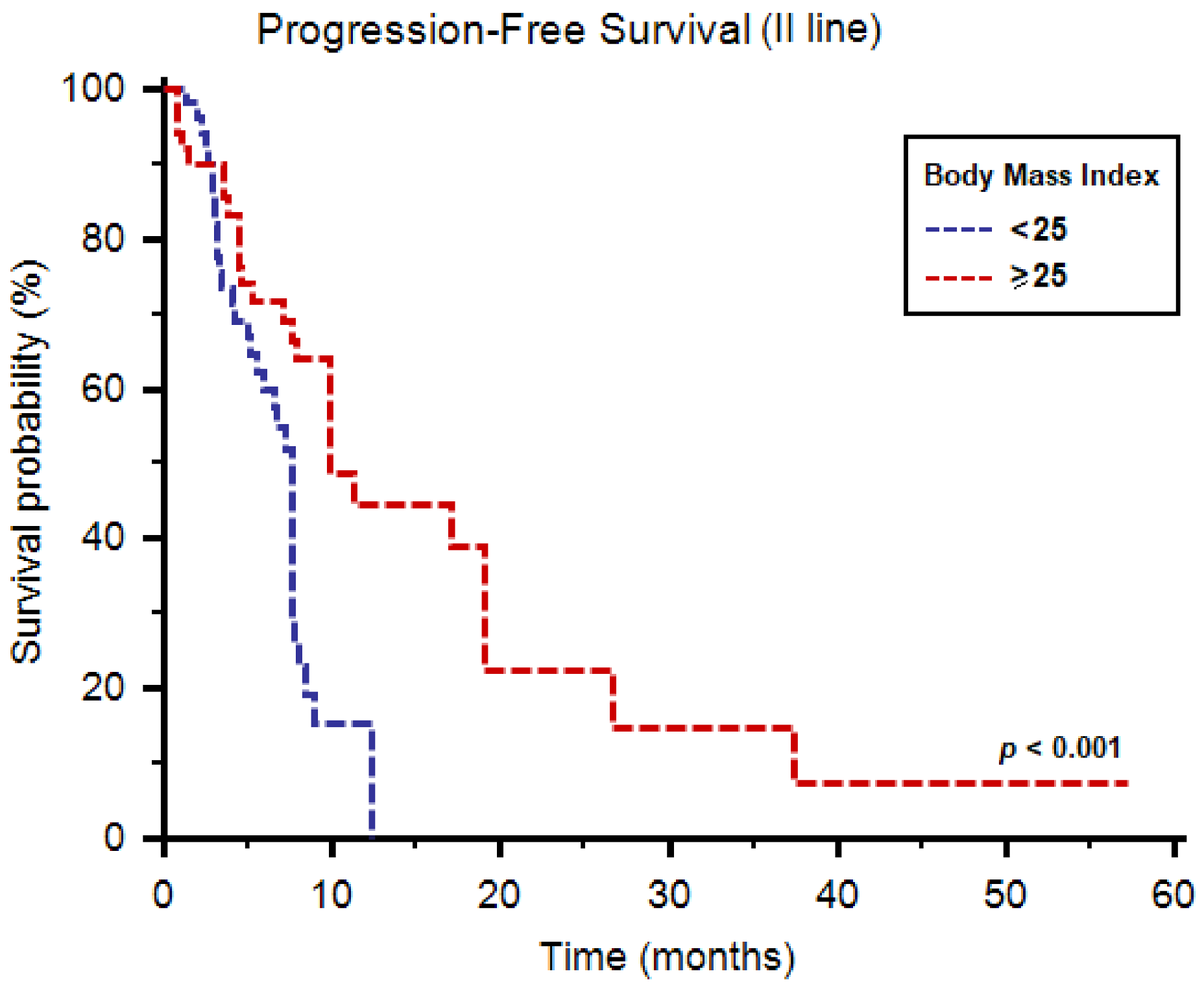
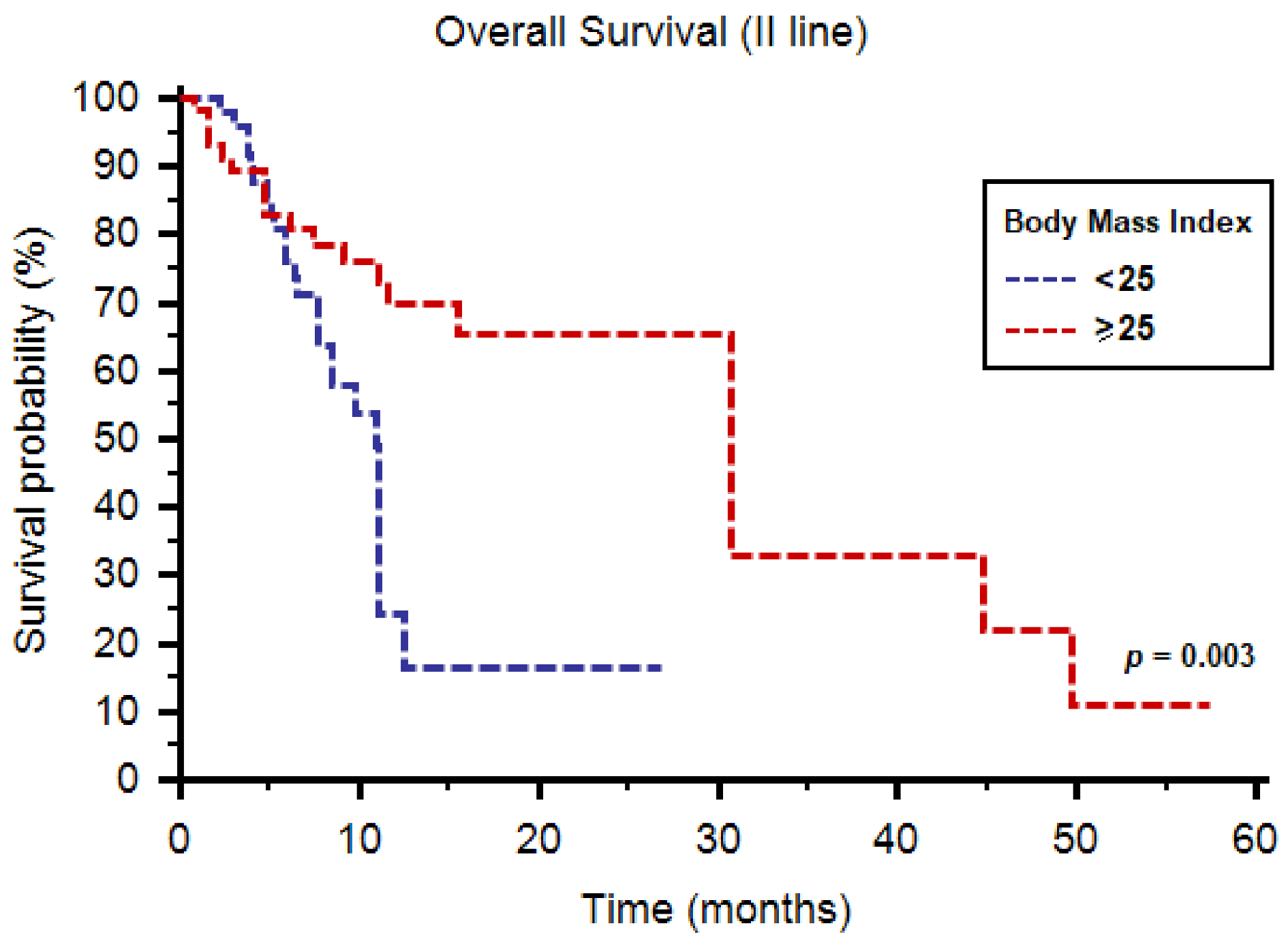
| 1y-OS (second-line cabozantinib) | 73 (65) | 47 (76) | 27 (53) | 0.019 |
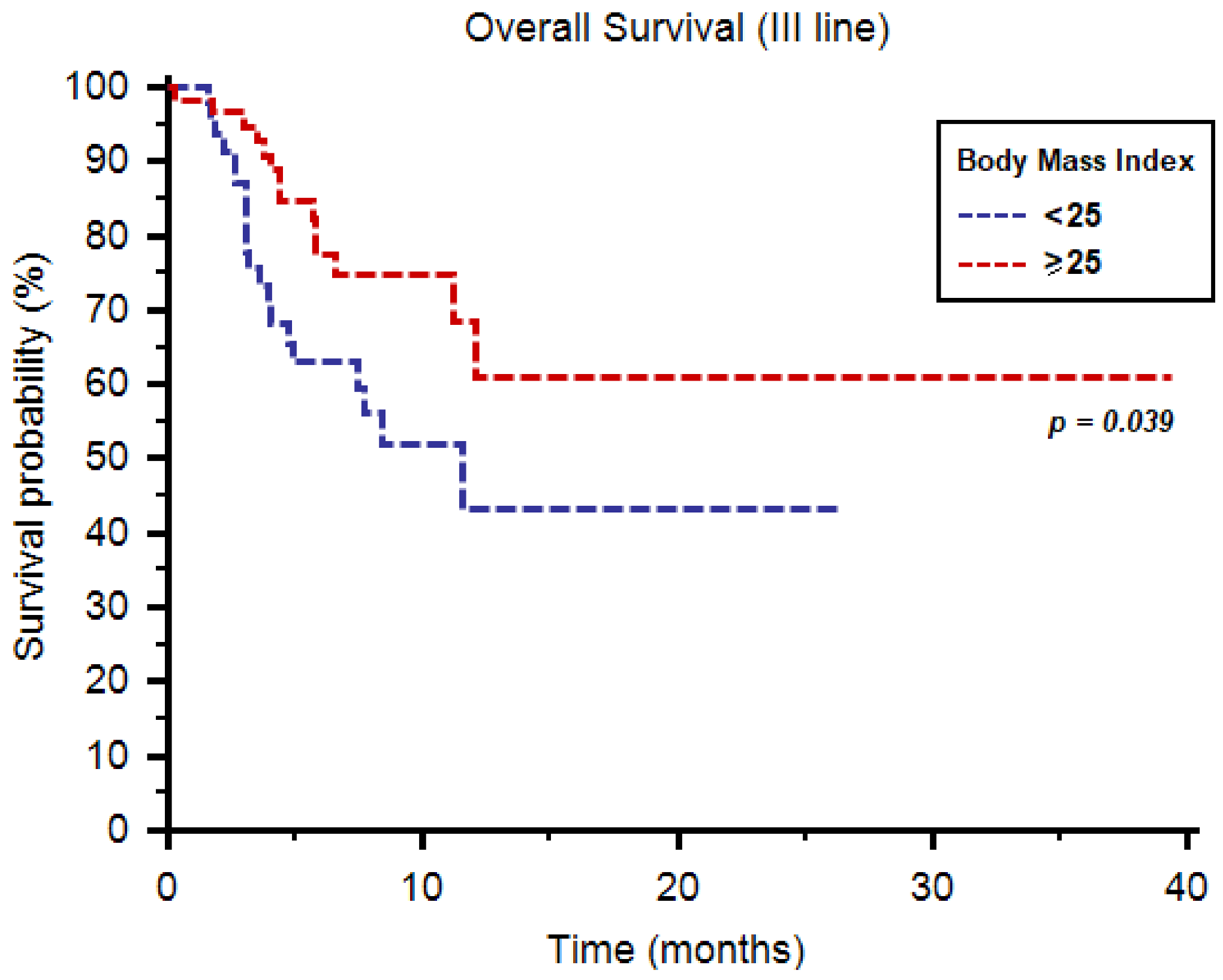
| 1y-OS (third-line cabozantinib) | 22 (20) | 16 (28) | 6 (11) | 0.045 |
| PFS | Univariate Cox Regression | Multivariable Cox Regression | ||
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Age (≥70 y vs. <70 y) | 1.31 (0.78–2.21) | 0.306 | ||
| Gender (M/F) | 1.17 (0.69–2.00) | 0.563 | ||
| Number of metastatic sites | 0.99 (0.78–1.27) | 0.930 | ||
| Lung metastases | 0.86 (0.59–1.47) | 0.783 | ||
| Liver metastases | 1.42 (0.77–2.51) | 0.459 | ||
| Bone metastases | 1.99 (1.08–3.18) | 0.112 | ||
| IMDC prognostic group | 2.08 (1.26–3.44) | 0.004 | 2.09 (1.29–3.37) | 0.003 |
| BMI (≥25 vs. <25) | 0.90 (0.84–0.97) | 0.005 | 0.37 (0.20–0.68) | 0.002 |
| OS | Univariate Cox Regression | Multivariable Cox Regression | ||
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Age (≥70 y vs. <70 y) | 0.78 (0.41–1.49) | 0.459 | ||
| Gender (M/F) | 1.46 (0.80–2.67) | 0.219 | ||
| Number of metastatic sites | 1.08 (0.81–1.44) | 0.613 | ||
| Lung metastases | 0.82 (0.51–1.33) | 0.424 | ||
| Liver metastases | 1.39 (0.80–2.39) | 0.244 | ||
| Bone metastases | 2.11 (1.32–3.40 | 0.051 | ||
| IMDC prognostic group | 1.85 (1.02–3.34) | 0.042 | 2.09 (1.29–3.37) | 0.003 |
| BMI (≥25 vs. <25) | 0.90 (0.83–0.98) | 0.018 | 0.38 (0.22–0.69) | 0.046 |
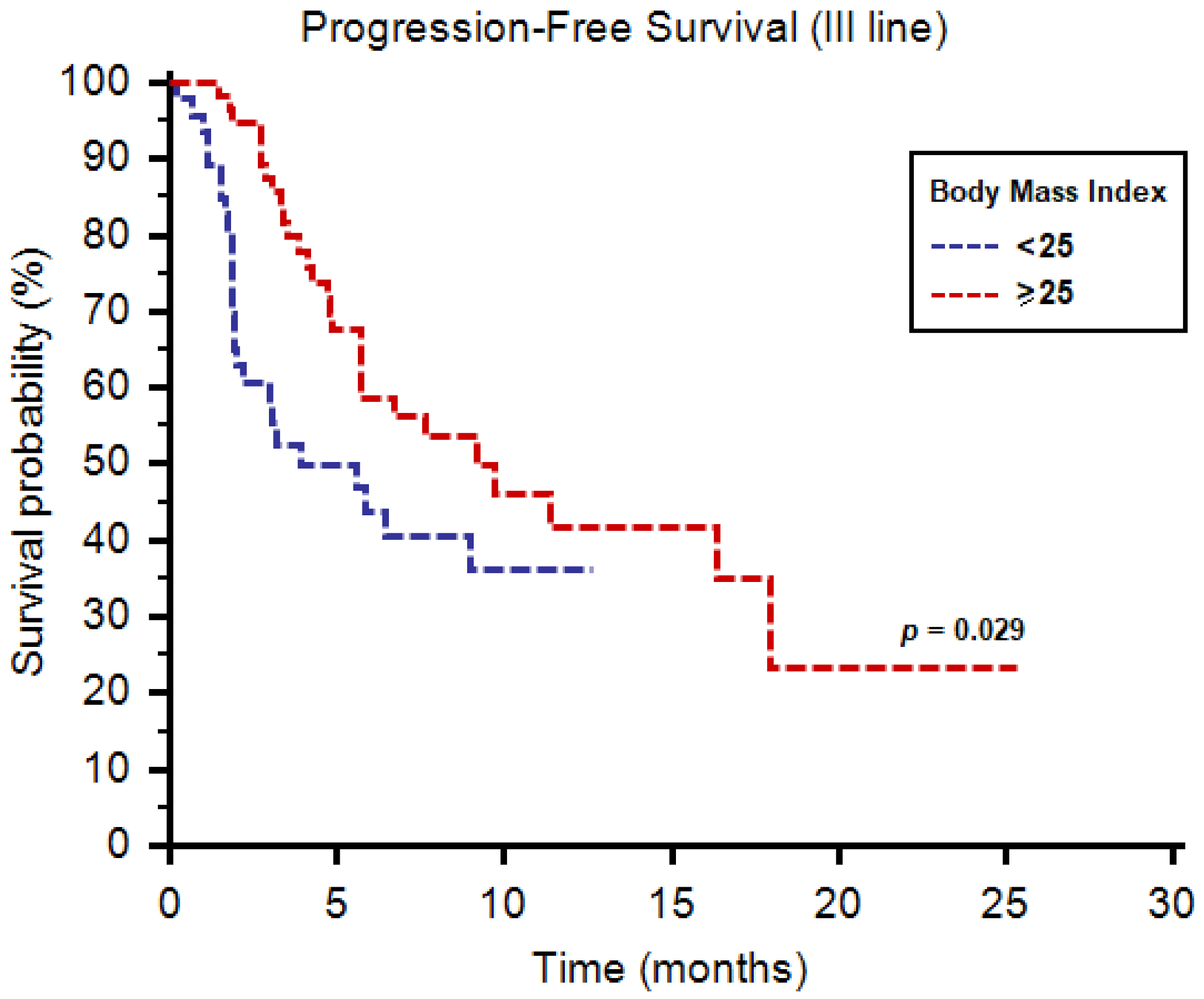
| PFS | Univariate Cox Regression | Multivariable Cox Regression | ||
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Age (≥70 y vs. <70 y) | 0.59 (0.31–1.11) | 0.102 | ||
| Gender (M/F) | 0.86 (0.46–1.61) | 0.645 | ||
| Number of metastatic sites | 1.40 (1.10–1.80) | 0.007 | 1.35 (1.04–1.74) | 0.021 |
| Lung metastases | 0.86 (0.67–1.91) | 0.672 | ||
| Liver metastases | 1.75 (0.84–2.88) | 0.594 | ||
| Bone metastases | 1.87 (0.96–3.98) | 0.317 | ||
| IMDC prognostic group | 1.18 (0.76–1.82) | 0.458 | ||
| BMI (≥25 vs. <25) | 0.55 (0.32–0.95) | 0.031 | 0.52 (0.32–0.95) | 0.020 |
| OS | Univariate Cox Regression | Multivariable Cox Regression | ||
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Age (≥70 y vs. <70 y) | 0.34 (0.12–0.96) | 0.042 | 0.70 (0.51–1.05) | 0.074 |
| Gender (M/F) | 1.12 (0.52–2.39) | 0.776 | ||
| Number of metastatic sites | 1.29 (0.94–1.76) | 0.120 | ||
| Lung metastases | 0.91 (0.64–1.57) | 0.458 | ||
| Liver metastases | 1.82 (0.73–2.86) | 0.632 | ||
| Bone metastases | 1.91 (1.08–3.41) | 0.351 | ||
| IMDC prognostic group | 1.51 (0.87–2.64) | 0.144 | ||
| BMI (≥25 vs, <25) | 0.35 (0.18–0.70) | 0.003 | 0.32 (0.16–0.65) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santoni, M.; Massari, F.; Bracarda, S.; Procopio, G.; Milella, M.; De Giorgi, U.; Basso, U.; Aurilio, G.; Incorvaia, L.; Martignetti, A.; et al. Body Mass Index in Patients Treated with Cabozantinib for Advanced Renal Cell Carcinoma: A New Prognostic Factor? Diagnostics 2021, 11, 138. https://doi.org/10.3390/diagnostics11010138
Santoni M, Massari F, Bracarda S, Procopio G, Milella M, De Giorgi U, Basso U, Aurilio G, Incorvaia L, Martignetti A, et al. Body Mass Index in Patients Treated with Cabozantinib for Advanced Renal Cell Carcinoma: A New Prognostic Factor? Diagnostics. 2021; 11(1):138. https://doi.org/10.3390/diagnostics11010138
Chicago/Turabian StyleSantoni, Matteo, Francesco Massari, Sergio Bracarda, Giuseppe Procopio, Michele Milella, Ugo De Giorgi, Umberto Basso, Gaetano Aurilio, Lorena Incorvaia, Angelo Martignetti, and et al. 2021. "Body Mass Index in Patients Treated with Cabozantinib for Advanced Renal Cell Carcinoma: A New Prognostic Factor?" Diagnostics 11, no. 1: 138. https://doi.org/10.3390/diagnostics11010138
APA StyleSantoni, M., Massari, F., Bracarda, S., Procopio, G., Milella, M., De Giorgi, U., Basso, U., Aurilio, G., Incorvaia, L., Martignetti, A., Rizzo, M., Cartenì, G., Grande, E., Matrana, M. R., Crabb, S. J., Vau, N., Sorgentoni, G., Cimadamore, A., Montironi, R., & Battelli, N. (2021). Body Mass Index in Patients Treated with Cabozantinib for Advanced Renal Cell Carcinoma: A New Prognostic Factor? Diagnostics, 11(1), 138. https://doi.org/10.3390/diagnostics11010138