Design, Development, and Multi-Characterization of an Integrated Clinical Transrectal Ultrasound and Photoacoustic Device for Human Prostate Imaging

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
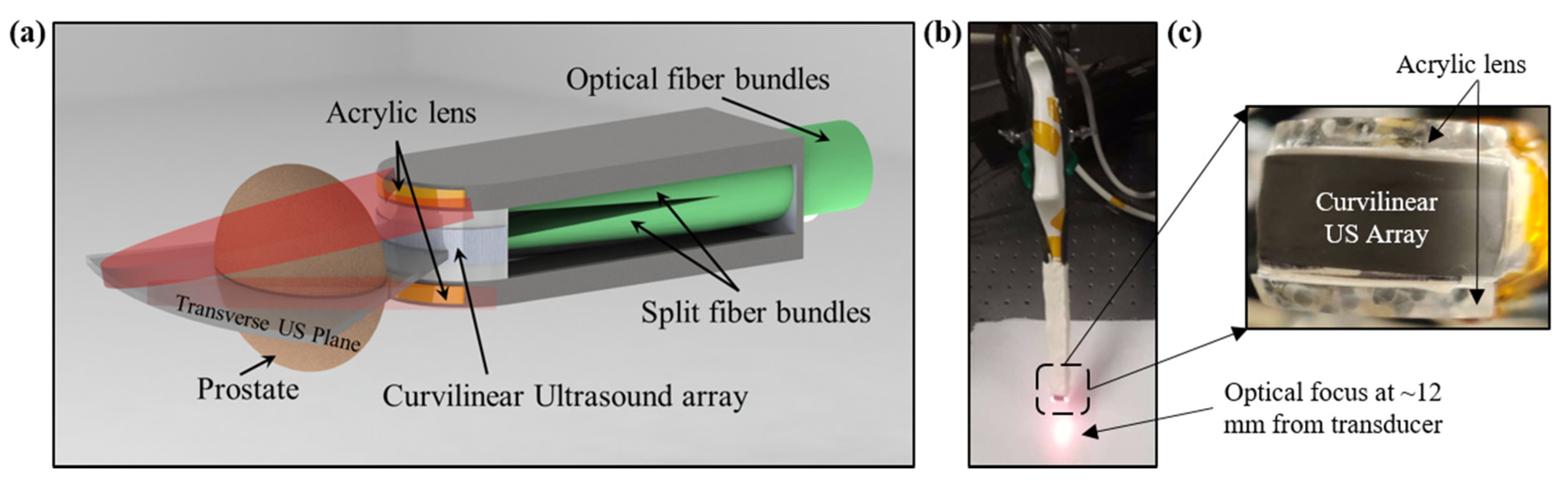
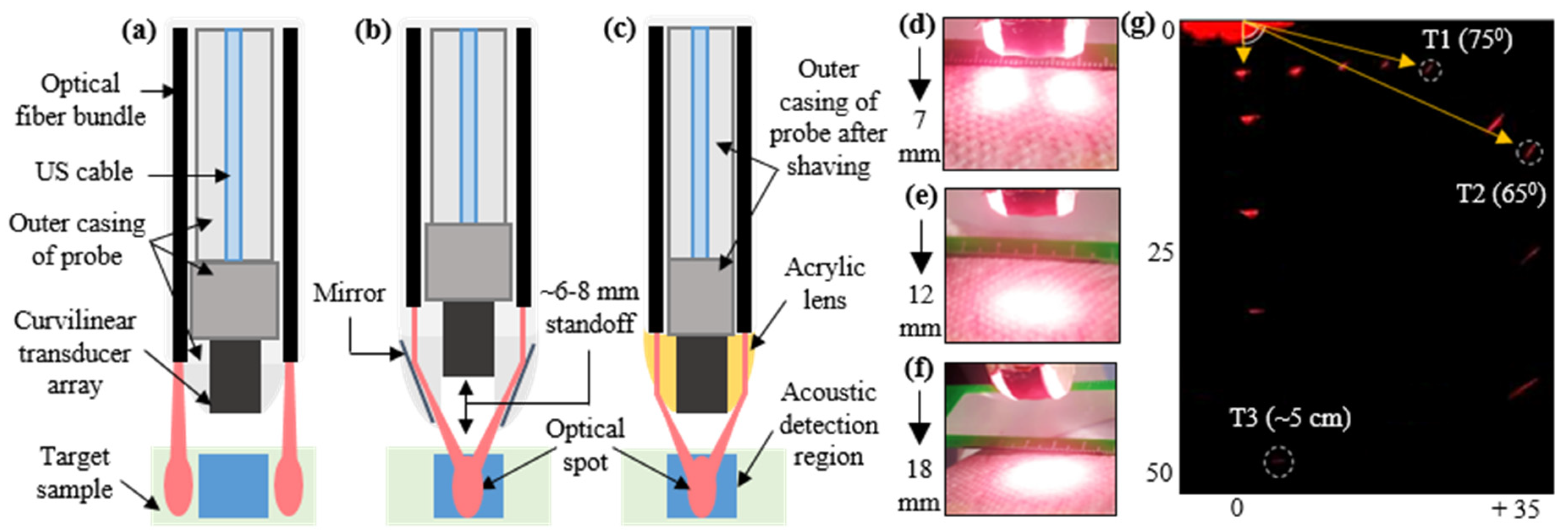
2.1. Design and Development of TRUSPA Device
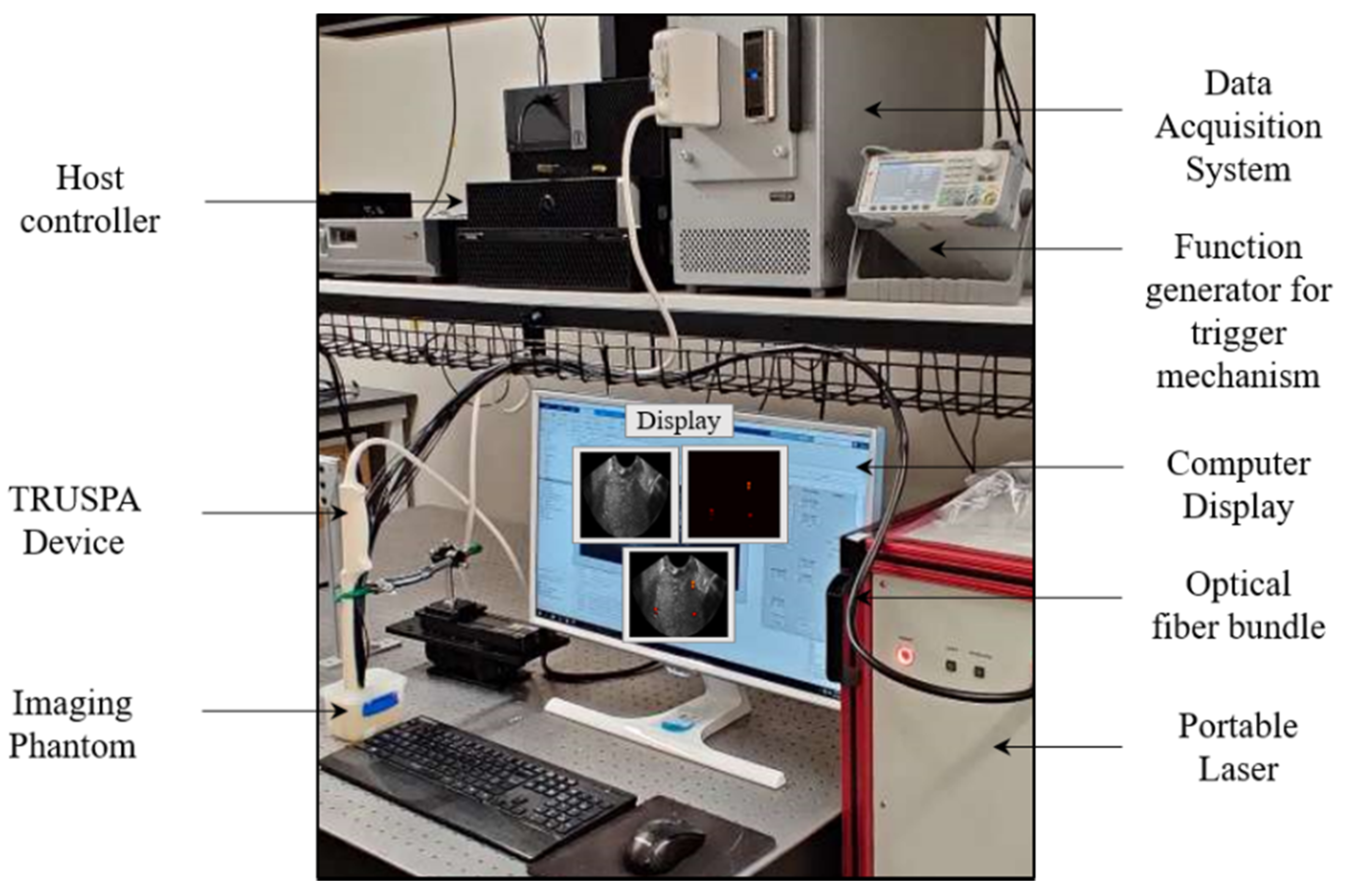
2.2. TRUSPA Imaging System: Experimental Setup
3. Experiments and Results
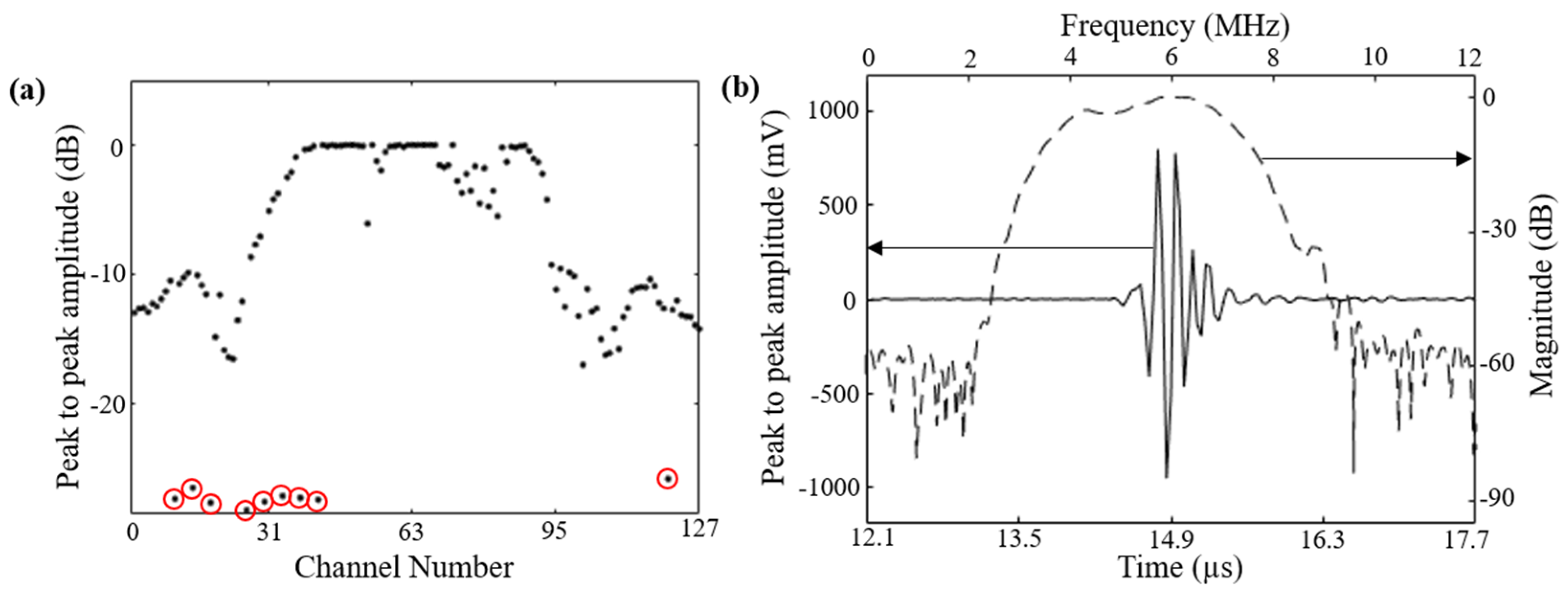
3.1. Characterization: Evaluation of 128-Element Curviliear Transducer Array
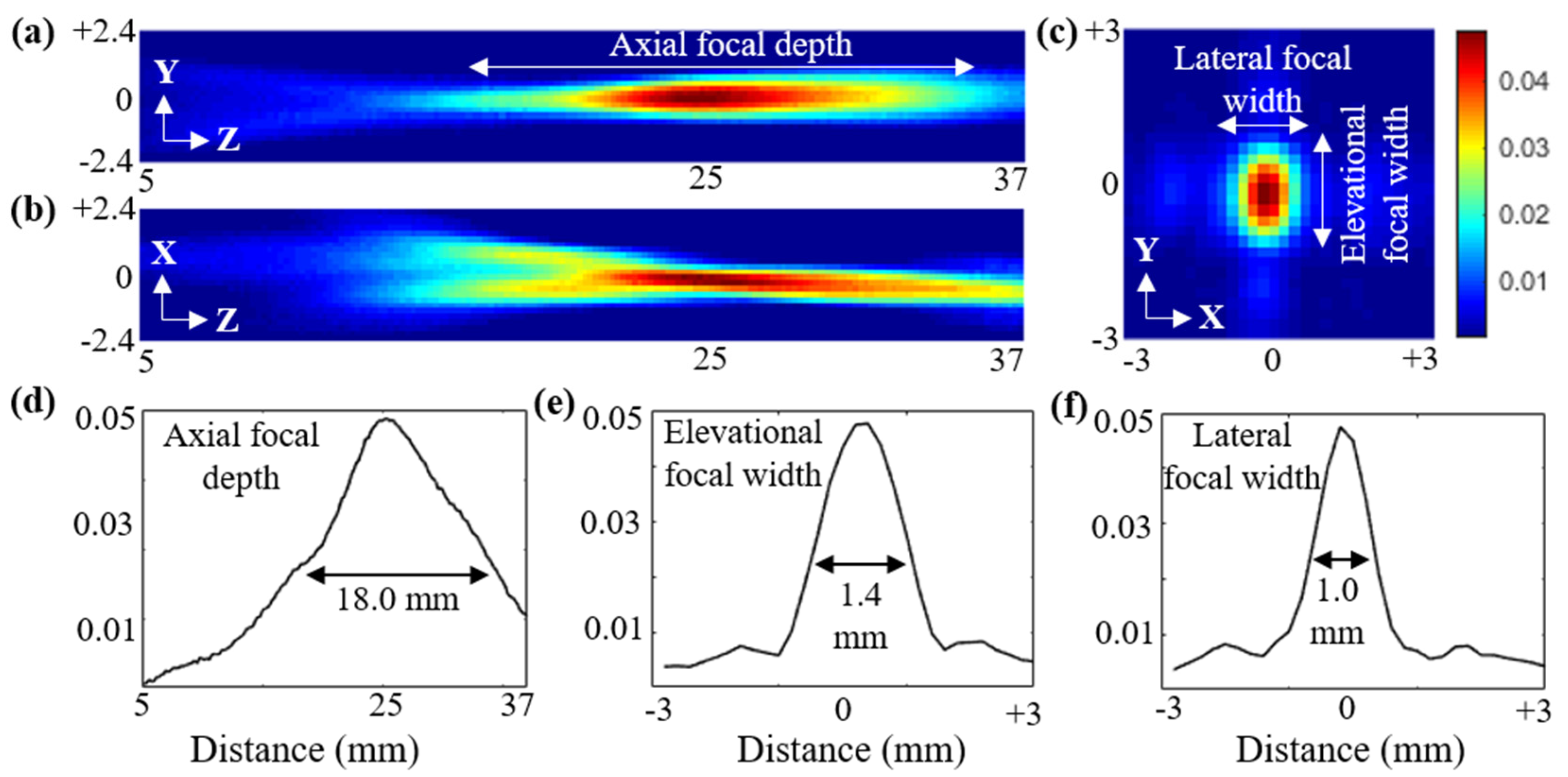
3.2. Characterization: Ultrasound Field Characterizations
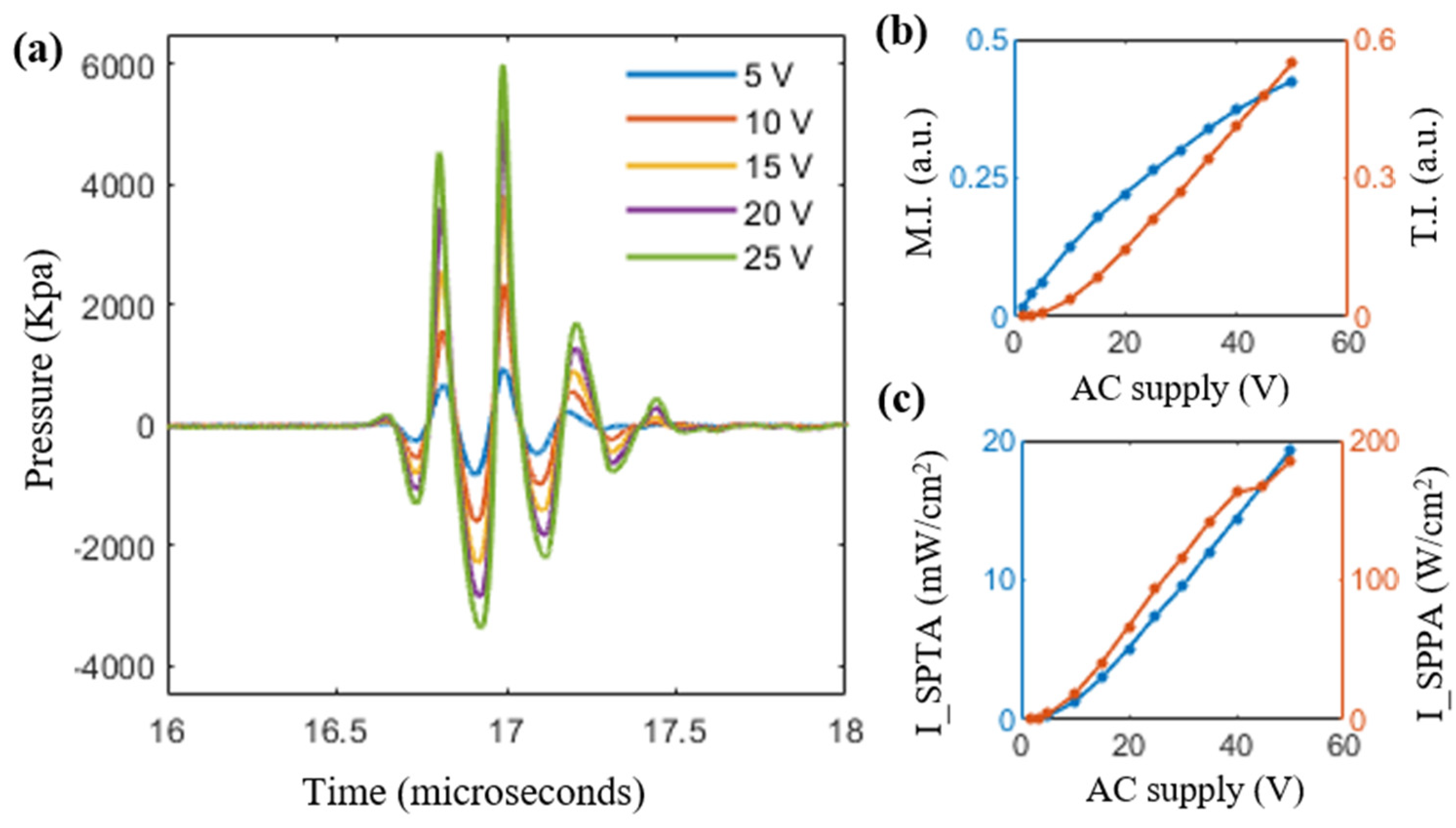
3.3. Evaluation of Safety Parameters
3.4. Optical Fluence and PAI Field-of-View Characterization
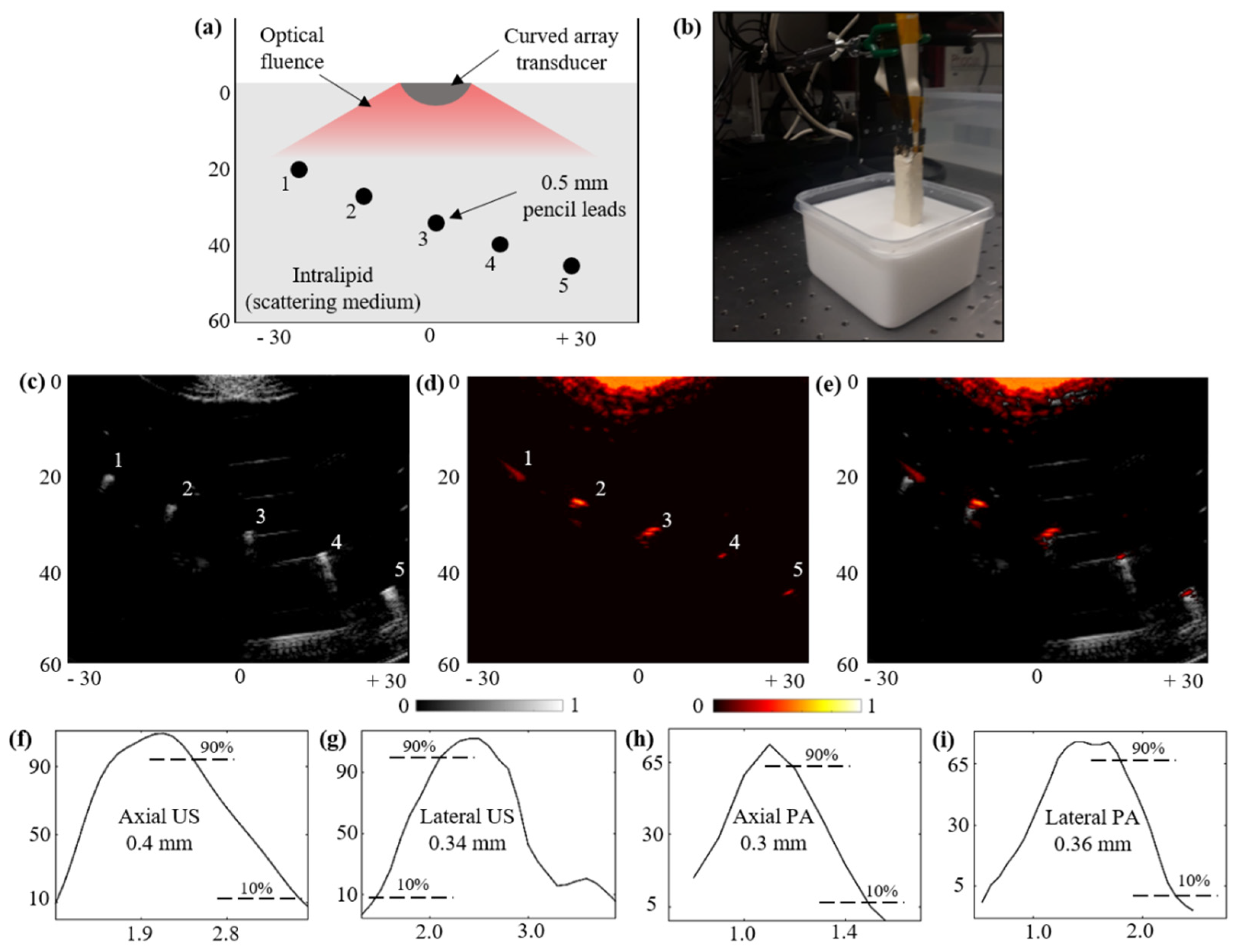
3.5. Structural Imaging Capabilities over a Scattering Phantom:
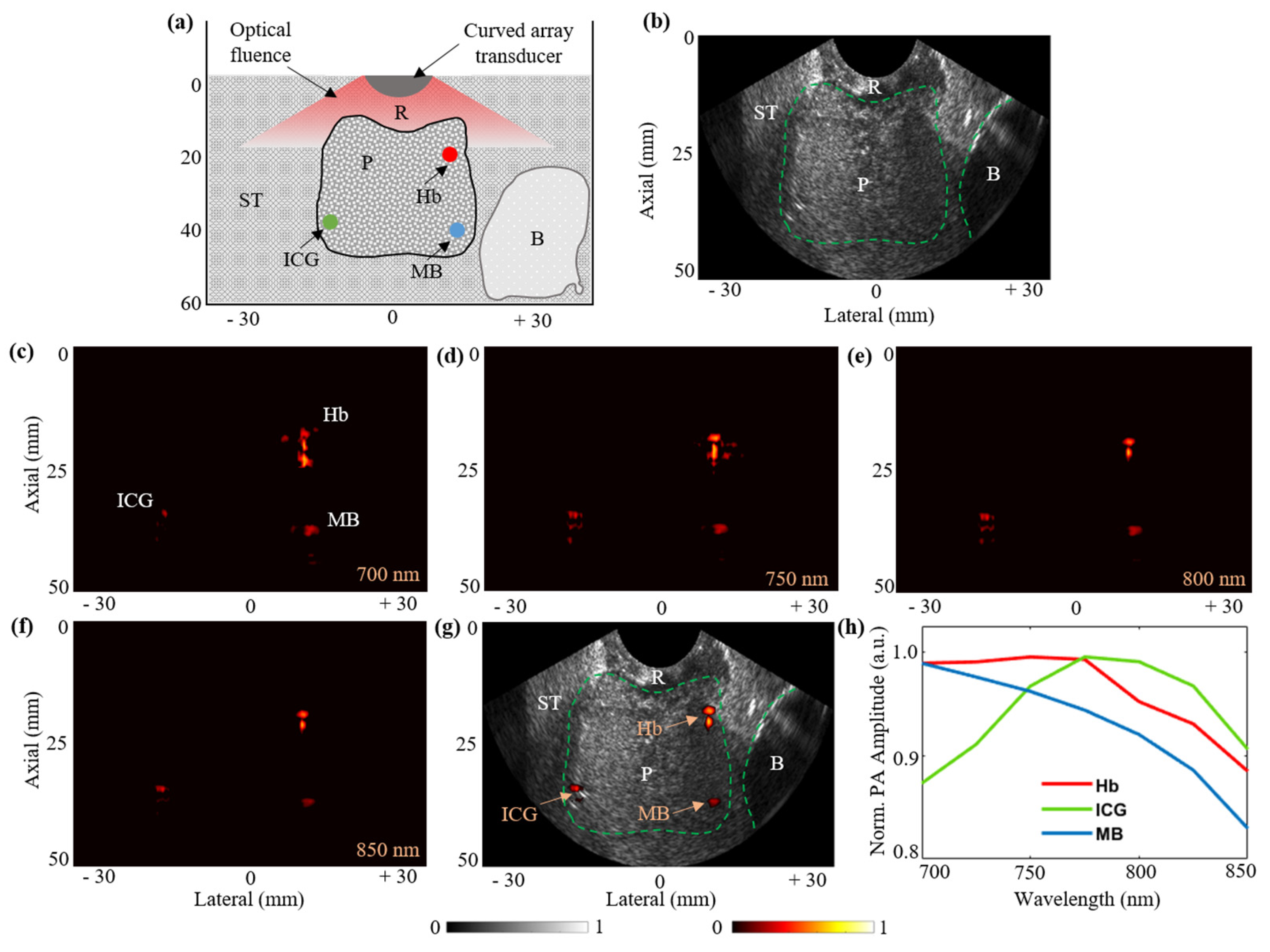
3.6. Functional Imaging Capabilities with Prostate Tissue-Mimicking Phantom:
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| PA | Photoacoustic |
| US | Ultrasound |
| PAI | Photoacoustic Imaging |
| PCa | Prostate Cancer |
| FOV | Field of View |
| TRUS | Transrectal Ultrasound |
| TRUSPA | Transrectal Ultrasound and Photoacoustic |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Culp, M.B.; Soerjomataram, I.; Efstathiou, J.A.; Bray, F.; Jemal, A. Recent global patterns in prostate cancer incidence and mortality rates. Eur. Urol. 2020, 77, 38–52. [Google Scholar] [CrossRef] [PubMed]
- Deuker, M.; Stolzenbach, L.F.; Pecoraro, A.; Rosiello, G.; Luzzago, S.; Tian, Z.; Saad, F.; Felix, K.H.; Karakiewicz, P.I. PSA, stage, grade and prostate cancer specific mortality in Asian American patients relative to Caucasians according to the United States Census Bureau race definitions. World J. Urol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fleshner, N.E.; O’Sullivan, M.; Fair, W.R. Prevalence and predictors of a positive repeat transrectal ultrasound guided needle biopsy of the prostate. J. Urol. 1997, 158, 505–509. [Google Scholar] [CrossRef]
- Rabbani, F.; Stroumbakis, N.; Kava, B.R.; Cookson, M.S.; Fair, W.R. Incidence and clinical significance of false-negative sextant prostate biopsies. J. Urol. 1998, 159, 1247–1250. [Google Scholar] [CrossRef]
- Taira, A.V.; Merrick, G.S.; Galbreath, R.W.; Andreini, H.; Taubenslag, W.; Curtis, R.; Butler, W.M.; Adamovich, E.; Wallner, K.E. Performance of transperineal template-guided mapping biopsy in detecting prostate cancer in the initial and repeat biopsy setting. Prostate Cancer Prostatic Dis. 2010, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Ehdaie, B.; Shariat, S.F. Magnetic Resonance Imaging–Targeted Prostate Biopsy: Back to the Future. Eur. Urol. 2013, 63, 141–142. [Google Scholar] [CrossRef]
- Moore, C.M.; Robertson, N.L.; Arsanious, N.; Middleton, T.; Villers, A.; Klotz, L.; Taneja, S.S.; Emberton, M. Image-guided prostate biopsy using magnetic resonance imaging–derived targets: A systematic review. Eur. Urol. 2013, 63, 125–140. [Google Scholar] [CrossRef]
- Siddiqui, M.M.; Rais-Bahrami, S.; Truong, H.; Stamatakis, L.; Vourganti, S.; Nix, J.; Hoang, A.N.; Walton-Diaz, A.; Shuch, B.; Weintraub, M.; et al. Magnetic resonance imaging/ultrasound–fusion biopsy significantly upgrades prostate cancer versus systematic 12-core transrectal ultrasound biopsy. Eur. Urol. 2013, 64, 713–719. [Google Scholar] [CrossRef]
- Cheikh, A.B.; Girouin, N.; Colombel, M.; Maréchal, J.M.; Gelet, A.; Bissery, A.; Rabilloud, M.; Lyonnet, D.; Rouvière, O. Evaluation of T2-weighted and dynamic contrast-enhanced MRI in localizing prostate cancer before repeat biopsy. Eur. Radiol. 2009, 19, 770–778. [Google Scholar] [CrossRef]
- Padhani, A.R.; Gapinski, C.J.; Macvicar, D.A.; Parker, G.J.; Suckling, J.; Revell, P.B.; Leach, M.O.; Dearnaley, D.P.; Husband, J.E. Dynamic contrast enhanced MRI of prostate cancer: Correlation with morphology and tumour stage, histological grade and PSA. Clin. Radiol. 2000, 55, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Tomlins, S.A.; Day, J.R.; Lonigro, R.J.; Hovelson, D.H.; Siddiqui, J.; Kunju, L.P.; Dunn, R.L.; Meyer, S.; Hodge, P.; Groskopf, J.; et al. Urine TMPRSS2: ERG plus PCA3 for individualized prostate cancer risk assessment. Eur. Urol. 2016, 70, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Cann, G.M.; Gulzar, Z.G.; Cooper, S.; Li, R.; Luo, S.; Tat, M.; Stuart, S.; Schroth, G.; Srinivas, S.; Ronaghi, M.; et al. mRNA-Seq of single prostate cancer circulating tumor cells reveals recapitulation of gene expression and pathways found in prostate cancer. PLoS ONE 2012, 7, e49144. [Google Scholar] [CrossRef] [PubMed]
- Palmeri, M.L.; Glass, T.J.; Miller, Z.A.; Rosenzweig, S.J.; Buck, A.; Polascik, T.J.; Gupta, R.T.; Brown, A.F.; Madden, J.; Nightingale, K.R. Identifying clinically significant prostate cancers using 3-D in vivo acoustic radiation force impulse imaging with whole-mount histology validation. Ultrasound Med. Biol. 2016, 42, 1251–1262. [Google Scholar] [CrossRef]
- Nelson, S.J.; Kurhanewicz, J.; Vigneron, D.B.; Larson, P.E.; Harzstark, A.L.; Ferrone, M.; Van Criekinge, M.; Chang, J.W.; Bok, R.; Park, I.; et al. Metabolic imaging of patients with prostate cancer using hyperpolarized [1-13C] pyruvate. Sci. Transl. Med. 2013, 5, 198ra108. [Google Scholar] [CrossRef] [PubMed]
- Khansa, Z.; Haidar, M.B.; Neaimeh, N.; Korek, M. Comparison of PET imaging with a 68Ga-labelled PSMA ligand versus 18F-choline PET/CT for the diagnosis of Prostate Cancer & Radioprotection for involved personnel. Health Technol. 2019, 9, 607–613. [Google Scholar]
- Levi, J.; Sathirachinda, A.; Gambhir, S.S. A high-affinity, high-stability photoacoustic agent for imaging gastrin-releasing peptide receptor in prostate cancer. Clin. Cancer Res. 2014, 20, 3721–3729. [Google Scholar] [CrossRef]
- Beard, P. Biomedical photoacoustic imaging. Interface Focus 2011, 1, 602–631. [Google Scholar] [CrossRef]
- Luke, G.P.; Yeager, D.; Emelianov, S.Y. Biomedical applications of photoacoustic imaging with exogenous contrast agents. Ann. Biomed. Eng. 2012, 40, 422–437. [Google Scholar] [CrossRef]
- Huang, W.; Chen, R.; Peng, Y.; Duan, F.; Huang, Y.; Guo, W.; Chen, X.; Nie, L. In vivo quantitative photoacoustic diagnosis of gastric and intestinal dysfunctions with a broad pH-responsive sensor. ACS Nano 2019, 13, 9561–9570. [Google Scholar] [CrossRef]
- Wang, X.; Roberts, W.W.; Carson, P.L.; Wood, D.P.; Fowlkes, J.B. Photoacoustic tomography: A potential new tool for prostate cancer. Biomed. Opt. Express 2010, 1, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.A.L.; Kuo, N.P.; Song, D.Y.; Kang, J.U.; Boctor, E.M. In vivo visualization of prostate brachytherapy seeds with photoacoustic imaging. J. Biomed. Opt. 2014, 19, 126011. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, A.; Tsujita, K.; Irisawa, K.; Kasamatsu, T.; Hirota, K.; Kawaguchi, M.; Shinchi, M.; Ito, K.; Asano, T.; Shinmoto, H.; et al. A pilot study of photoacoustic imaging system for improved real-time visualization of neurovascular bundle during radical prostatectomy. Prostate 2016, 76, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Xing, M.; Cong, B.; Qiu, C.; He, D.; Wang, C.; Xiao, Y.; Yin, T.; Shao, M.; Qiu, W.; et al. In vivo transrectal imaging of canine prostate with a sensitive and compact handheld transrectal array photoacoustic probe for early diagnosis of prostate cancer. Biomed. Opt. Express 2019, 10, 1707–1717. [Google Scholar] [CrossRef] [PubMed]
- Kothapalli, S.R.; Sonn, G.A.; Choe, J.W.; Nikoozadeh, A.; Bhuyan, A.; Park, K.K.; Cristman, P.; Fan, R.; Moini, A.; Lee, B.C.; et al. Simultaneous transrectal ultrasound and photoacoustic human prostate imaging. Sci. Transl. Med. 2019, 11, eaav2169. [Google Scholar] [CrossRef]
- Kothapalli, S.R.; Ma, T.J.; Vaithilingam, S.; Oralkan, Ö.; Khuri-Yakub, B.T.; Gambhir, S.S. Deep tissue photoacoustic imaging using a miniaturized 2-D capacitive micromachined ultrasonic transducer array. IEEE Trans. Biomed. Eng. 2012, 59, 1199–1204. [Google Scholar] [CrossRef]
- Wu, X.; Sanders, J.L.; Zhang, X.; Yamaner, F.Y.; Oralkan, Ö. An FPGA-based backend system for intravascular photoacoustic and ultrasound imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2018, 66, 45–56. [Google Scholar] [CrossRef]
- Dangi, A.; Cheng, C.Y.; Agrawal, S.; Tiwari, S.; Datta, G.R.; Benoit, R.R.; Pratap, R.; Trolier-Mckinstry, S.; Kothapalli, S.R. A Photoacoustic Imaging Device using Piezoelectric Micromachined Ultrasound Transducers (PMUTs). IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 67, 801–809. [Google Scholar] [CrossRef]
- Dangi, A.; Agrawal, S.; Tiwari, S.; Jadhav, S.; Cheng, C.; Datta, G.R.; Trolier-McKinstry, S.; Pratap, R.; Kothapalli, S.R. Ring PMUT array based miniaturized photoacoustic endoscopy device. In Photons Plus Ultrasound: Imaging and Sensing; International Society for Optics and Photonics: Bellingham, WA, USA, 2019; Volume 10878, p. 1087811. [Google Scholar]
- Şen, T.; Tüfekçioğlu, O.; Koza, Y. Mechanical index. Anatol. J. Cardiol. 2015, 15, 334. [Google Scholar] [CrossRef]
- Nelson, T.R.; Fowlkes, J.B.; Abramowicz, J.S.; Church, C.C. Ultrasound Biosafety Considerations for the Practicing Sonographer and Sonologist. J Ultrasound Med. 2009, 28, 139–150. [Google Scholar] [CrossRef]
- Fomenko, A.; Neudorfer, C.; Dallapiazza, R.F.; Kalia, S.K.; Lozano, A.M. Low-intensity ultrasound neuromodulation: An overview of mechanisms and emerging human applications. Brain Stimul. 2018, 11, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Bigelow, T.A.; Church, C.C.; Sandstrom, K.; Abbott, J.G.; Ziskin, M.C.; Edmonds, P.D.; Herman, B.; Thomenius, K.E.; Teo, T.J. The thermal index: Its strengths, weaknesses, and proposed improvements. J. Ultrasound Med. 2011, 30, 714–734. [Google Scholar] [CrossRef] [PubMed]
- Laser Institute of America. American National Standard for Safe Use of Lasers; American National Standards Institute, Inc.: New York, NY, USA, 2000. [Google Scholar]
- OMLC Website. Available online: http://omlc.org/spectra/index.html (accessed on 15 June 2020).
- Martino, P.; Galosi, A.B. Practical recommendations for performing ultrasound scanning in the urological and andrological fields. In Atlas of Ultrasonography in Urology, Andrology, and Nephrology; Springer: Cham, Switzerland, 2017; pp. 695–728. [Google Scholar]
- Martin, C.J.; Sutton, D.G. Practical radiation protection in healthcare. In Medical Physics; Oxford University Press: New York NY, USA, 2015; p. 995. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Supplied AC Voltage (Volts) | Peak Negative Voltage (mV) | Peak Negative Pressure (MPa) | De-Rated Pressure (MPa) | Mechanical Index (MI) | ISPTA (mW/cm2) | ISPPA (W/cm2) | Thermal Index (TI) |
|---|---|---|---|---|---|---|---|
| 1.6 | 10.7 | 0.2192 | 0.0418 | 0.0170 | 0.01 | 0.22 | 0.0003 |
| 3.2 | 25.1 | 0.5172 | 0.0986 | 0.0402 | 0.09 | 1.43 | 0.0026 |
| 5.0 | 40.0 | 0.8234 | 0.1569 | 0.0641 | 0.27 | 3.97 | 0.0077 |
| 10.0 | 78.2 | 1.6085 | 0.3065 | 0.1251 | 1.3 | 18.26 | 0.0371 |
| 15.0 | 111.7 | 2.2981 | 0.4379 | 0.1788 | 2.99 | 40.64 | 0.0854 |
| 20.0 | 138.9 | 2.8578 | 0.5446 | 0.2223 | 5.12 | 66.88 | 0.1463 |
| 25.0 | 164.3 | 3.3800 | 0.6440 | 0.2629 | 7.44 | 93.50 | 0.2126 |
| 30.0 | 188.6 | 3.8805 | 0.7394 | 0.3019 | 9.54 | 116.54 | 0.2726 |
| 35.0 | 212.0 | 4.3628 | 0.8313 | 0.3394 | 12.04 | 141.61 | 0.3440 |
| 40.0 | 233.0 | 4.7936 | 0.9134 | 0.3729 | 14.43 | 162.45 | 0.4123 |
| 45.0 | 250.2 | 5.1479 | 0.9809 | 0.4005 | 16.82 | 167.01 | 0.4806 |
| 50.0 | 265.3 | 5.4585 | 1.0401 | 0.4246 | 19.23 | 184.91 | 0.54940 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agrawal, S.; Johnstonbaugh, K.; Clark, J.Y.; Raman, J.D.; Wang, X.; Kothapalli, S.-R. Design, Development, and Multi-Characterization of an Integrated Clinical Transrectal Ultrasound and Photoacoustic Device for Human Prostate Imaging. Diagnostics 2020, 10, 566. https://doi.org/10.3390/diagnostics10080566
Agrawal S, Johnstonbaugh K, Clark JY, Raman JD, Wang X, Kothapalli S-R. Design, Development, and Multi-Characterization of an Integrated Clinical Transrectal Ultrasound and Photoacoustic Device for Human Prostate Imaging. Diagnostics. 2020; 10(8):566. https://doi.org/10.3390/diagnostics10080566
Chicago/Turabian StyleAgrawal, Sumit, Kerrick Johnstonbaugh, Joseph Y. Clark, Jay D. Raman, Xueding Wang, and Sri-Rajasekhar Kothapalli. 2020. "Design, Development, and Multi-Characterization of an Integrated Clinical Transrectal Ultrasound and Photoacoustic Device for Human Prostate Imaging" Diagnostics 10, no. 8: 566. https://doi.org/10.3390/diagnostics10080566
APA StyleAgrawal, S., Johnstonbaugh, K., Clark, J. Y., Raman, J. D., Wang, X., & Kothapalli, S.-R. (2020). Design, Development, and Multi-Characterization of an Integrated Clinical Transrectal Ultrasound and Photoacoustic Device for Human Prostate Imaging. Diagnostics, 10(8), 566. https://doi.org/10.3390/diagnostics10080566