

Enhancing Global Cognition and Executive Functions Through Water-Based Exercise in Mild Cognitive Impairment: A Randomized Controlled Trial
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
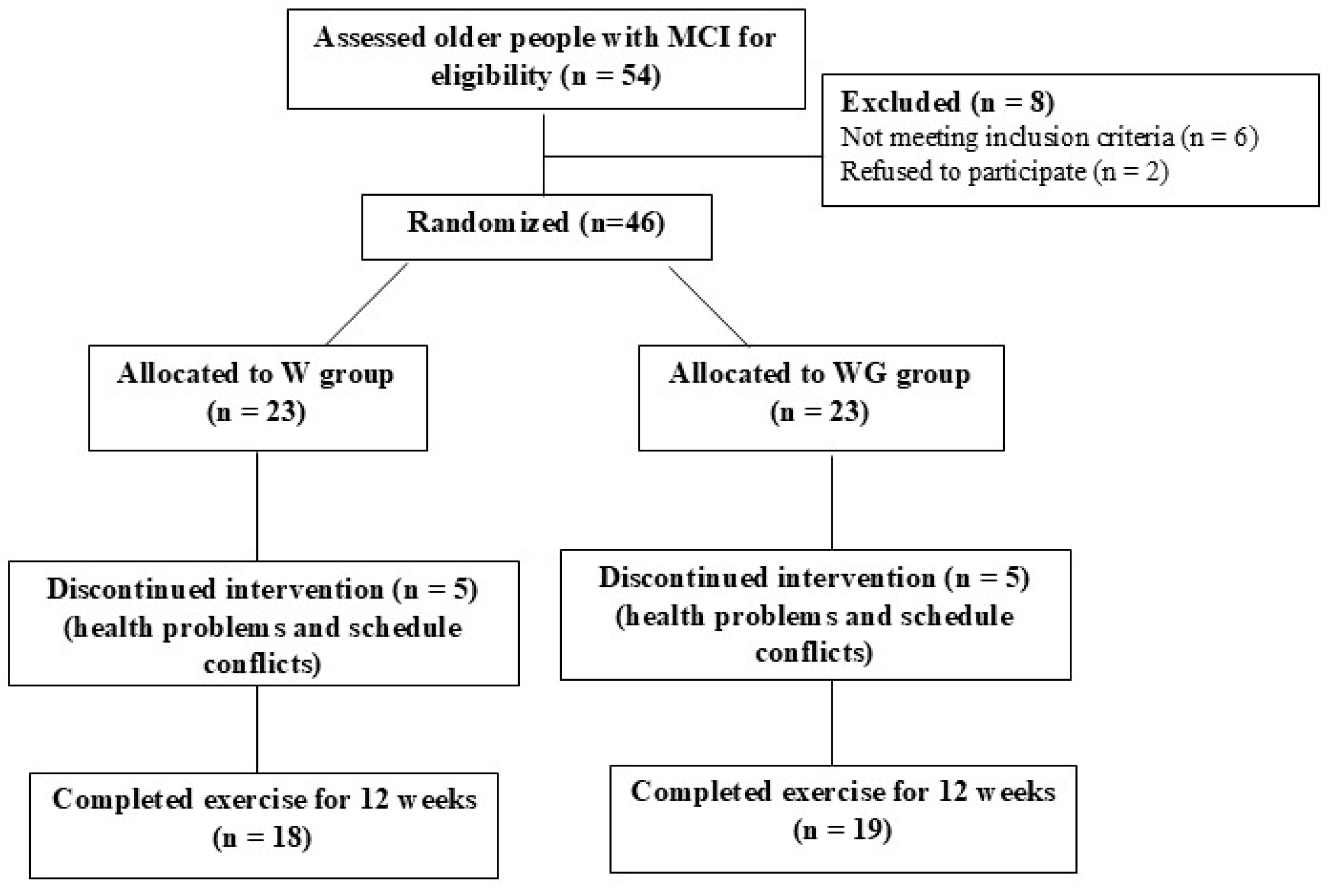
3.1. General Characteristics of Participants
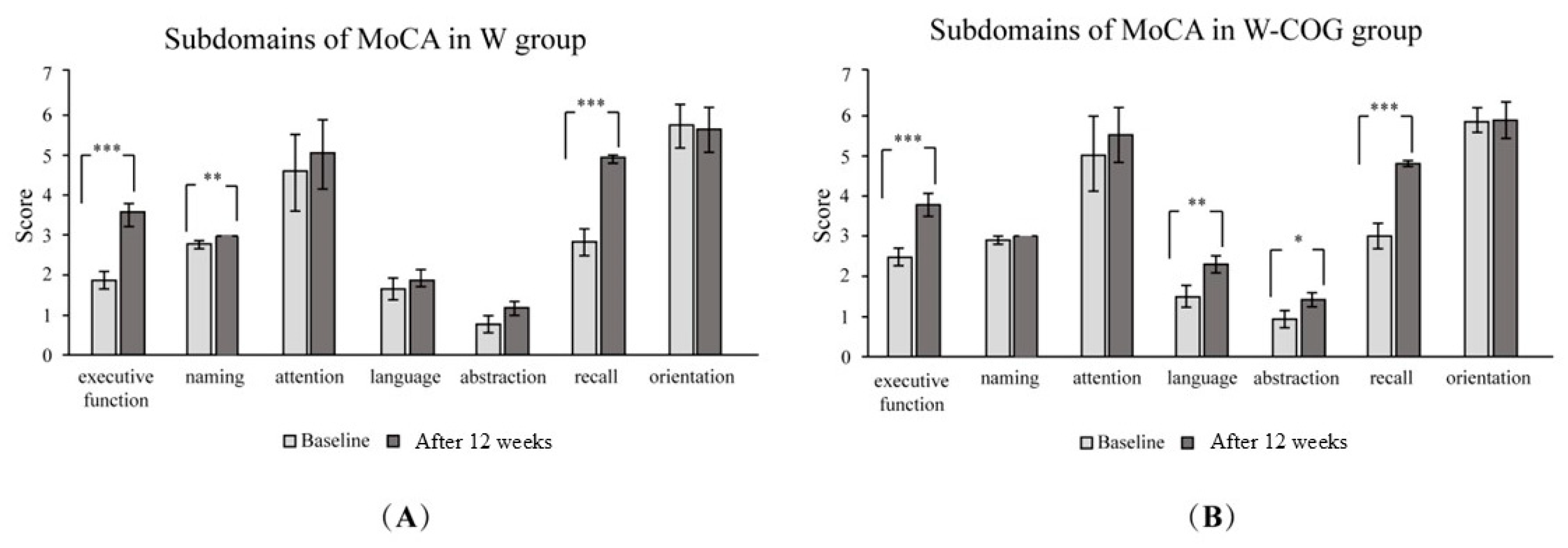
3.2. Cognitive Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Langa, K.M.; Levine, D.A. The Diagnosis and Management of Mild Cognitive Impairment: A Clinical Review. JAMA 2014, 312, 2551–2561. [Google Scholar] [CrossRef]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice Guideline Update Summary: Mild Cognitive Impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Petersen, R.C.; Morris, J.C. Mild Cognitive Impairment as a Clinical Entity and Treatment Target. Arch. Neurol. 2005, 62, 1160–1163. [Google Scholar] [CrossRef]
- Griffiths, J.; Thaikruea, L.; Wongpakaran, N.; Munkhetvit, P. Prevalence of Mild Cognitive Impairment in Rural Thai Older People, Associated Risk Factors and Their Cognitive Characteristics. Dement. Geriatr. Cogn. Dis. Extra 2020, 10, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Knopman, D.S.; Petersen, R.C. Mild Cognitive Impairment and Mild Dementia: A Clinical Perspective. Mayo Clin. Proc. 2014, 89, 1452–1459. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild Cognitive Impairment as a Diagnostic Entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Wahlund, L.-O.; Erkinjuntti, T.; Gauthier, S. Vascular Cognitive Impairment in Clinical Practice; Cambridge University Press: Cambridge, UK, 2009. [Google Scholar]
- Scarmeas, N.; Stern, Y. Cognitive Reserve and Lifestyle. J. Clin. Exp. Neuropsychol. 2003, 25, 625–633. [Google Scholar] [CrossRef]
- Jorm, A.F. History of Depression as a Risk Factor for Dementia: An Updated Review. Aust. N. Z. J. Psychiatry 2001, 35, 776–781. [Google Scholar] [CrossRef]
- Casagrande, M.; Forte, G.; Favieri, F.; Corbo, I. Sleep Quality and Aging: A Systematic Review on Healthy Older People, Mild Cognitive Impairment and Alzheimer’s Disease. Int. J. Environ. Res. Public Health 2022, 19, 8457. [Google Scholar] [CrossRef]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A Review of the Effects of Physical Activity and Exercise on Cognitive and Brain Functions in Older Adults. J. Aging Res. 2013, 2013, 657508. [Google Scholar] [CrossRef]
- Blondell, S.J.; Hammersley-Mather, R.; Veerman, J.L. Does Physical Activity Prevent Cognitive Decline and Dementia?: A Systematic Review and Meta-Analysis of Longitudinal Studies. BMC Public Health 2014, 14, 510. [Google Scholar] [CrossRef] [PubMed]
- Cammisuli, D.M.; Innocenti, A.; Franzoni, F.; Pruneti, C. Aerobic Exercise Effects upon Cognition in Mild Cognitive Impairment: A Systematic Review of Randomized Controlled Trials. Arch. Ital. Biol. 2017, 155, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Biazus-Sehn, L.F.; Schuch, F.B.; Firth, J.; de Souza Stigger, F. Effects of Physical Exercise on Cognitive Function of Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Arch. Gerontol. Geriatr. 2020, 89, 104048. [Google Scholar] [CrossRef] [PubMed]
- Law, C.-K.; Lam, F.M.; Chung, R.C.; Pang, M.Y. Physical Exercise Attenuates Cognitive Decline and Reduces Behavioural Problems in People with Mild Cognitive Impairment and Dementia: A Systematic Review. J. Physiother. 2020, 66, 9–18. [Google Scholar] [CrossRef]
- Yang, C.; Moore, A.; Mpofu, E.; Dorstyn, D.; Li, Q.; Yin, C. Effectiveness of Combined Cognitive and Physical Interventions to Enhance Functioning in Older Adults With Mild Cognitive Impairment: A Systematic Review of Randomized Controlled Trials. Gerontologist 2020, 60, 633–642. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Doi, T.; Park, H.; Tsutsumimoto, K.; Verghese, J.; Suzuki, T. Effects of Combined Physical and Cognitive Exercises on Cognition and Mobility in Patients With Mild Cognitive Impairment: A Randomized Clinical Trial. J. Am. Med. Dir. Assoc. 2018, 19, 584–591. [Google Scholar] [CrossRef]
- Hagovska, M.; Nagyova, I. The Transfer of Skills from Cognitive and Physical Training to Activities of Daily Living: A Randomised Controlled Study. Eur. J. Ageing 2017, 14, 133–142. [Google Scholar] [CrossRef]
- Combourieu Donnezan, L.; Perrot, A.; Belleville, S.; Bloch, F.; Kemoun, G. Effects of Simultaneous Aerobic and Cognitive Training on Executive Functions, Cardiovascular Fitness and Functional Abilities in Older Adults with Mild Cognitive Impairment. Ment. Health Phys. Act. 2018, 15, 78–87. [Google Scholar] [CrossRef]
- Delbroek, T.; Vermeylen, W.; Spildooren, J. The Effect of Cognitive-Motor Dual Task Training with the Biorescue Force Platform on Cognition, Balance and Dual Task Performance in Institutionalized Older Adults: A Randomized Controlled Trial. J. Phys. Ther. Sci. 2017, 29, 1137–1143. [Google Scholar] [CrossRef]
- Lord, S.R.; Matters, B.; St George, R.; Thomas, M.; Bindon, J.; Chan, D.K.; Collings, A.; Haren, L. The Effects of Water Exercise on Physical Functioning in Older People. Australas. J. Ageing 2006, 25, 36–41. [Google Scholar] [CrossRef]
- Yamashina, Y.; Yokoyama, H.; Naghavi, N.; Hirasawa, Y.; Takeda, R.; Ota, A.; Imai, D.; Miyagawa, T.; Okazaki, K. Treadmill Walking in Water Induces Greater Respiratory Muscle Fatigue than Treadmill Walking on Land in Healthy Young Men. J. Physiol. Sci. 2016, 66, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild Cognitive Impairment: Clinical Characterization and Outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Meekum, S. Effect of Water-Based Exercise Combined with Cognitive Training on Cognitive and Physical Performance in Elderly with Mild Cognitive Impairment: A Randomized Controlled Trial. Master’s Thesis, Thammasat University, Bangkok, Thailand, 2024. [Google Scholar]
- Mulser, L.; Moreau, D. Effect of Acute Cardiovascular Exercise on Cerebral Blood Flow: A Systematic Review. Brain Res. 2023, 1809, 148355. [Google Scholar] [CrossRef]
- Huang, X.; Zhao, X.; Li, B.; Cai, Y.; Zhang, S.; Wan, Q.; Yu, F. Comparative Efficacy of Various Exercise Interventions on Cognitive Function in Patients with Mild Cognitive Impairment or Dementia: A Systematic Review and Network Meta-Analysis. J. Sport Health Sci. 2022, 11, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Farinha, C.; Teixeira, A.M.; Serrano, J.; Santos, H.; Campos, M.J.; Oliveiros, B.; Silva, F.M.; Cascante-Rusenhack, M.; Luís, P.; Ferreira, J.P. Impact of Different Aquatic Exercise Programs on Body Composition, Functional Fitness and Cognitive Function of Non-Institutionalized Elderly Adults: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 8963. [Google Scholar] [CrossRef]
- Campbell, E.B.; Delgadillo, M.; Lazzeroni, L.C.; Louras, P.N.; Myers, J.; Yesavage, J.; Fairchild, J.K. Cognitive Improvement Following Physical Exercise and Cognitive Training Intervention for Older Adults With MCI. J. Gerontol. A Biol. Sci. Med. Sci. 2023, 78, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Pinilla, F.; Ying, Z.; Roy, R.R.; Molteni, R.; Edgerton, V.R. Voluntary Exercise Induces a BDNF-Mediated Mechanism That Promotes Neuroplasticity. J. Neurophysiol. 2002, 88, 2187–2195. [Google Scholar] [CrossRef]
- de Melo Coelho, F.G.; Gobbi, S.; Andreatto, C.A.A.; Corazza, D.I.; Pedroso, R.V.; Santos-Galduróz, R.F. Physical Exercise Modulates Peripheral Levels of Brain-Derived Neurotrophic Factor (BDNF): A Systematic Review of Experimental Studies in the Elderly. Arch. Gerontol. Geriatr. 2013, 56, 10–15. [Google Scholar] [CrossRef]
- Thoenen, H. Neurotrophins and Neuronal Plasticity. Science 1995, 270, 593–598. [Google Scholar] [CrossRef]
- Kim, Y.S.; Shin, S.K.; Hong, S.B.; Kim, H.J. The Effects of Strength Exercise on Hippocampus Volume and Functional Fitness of Older Women. Exp. Gerontol. 2017, 97, 22–28. [Google Scholar] [CrossRef]
- Schaeffer, E.; Roeben, B.; Granert, O.; Hanert, A.; Liepelt-Scarfone, I.; Leks, E.; Otterbein, S.; Saraykin, P.; Busch, J.-H.; Synofzik, M.; et al. Effects of Exergaming on Hippocampal Volume and Brain-Derived Neurotrophic Factor Levels in Parkinson’s Disease. Eur. J. Neurol. 2022, 29, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Senior, G.; Piovesana, A.; Beaumont, P. Discrepancy Analysis and Australian Norms for the Trail Making Test. Clin. Neuropsychol. 2018, 32, 510–523. [Google Scholar] [CrossRef] [PubMed]
- García-Madruga, J.A.; Gómez-Veiga, I.; Vila, J.Ó. Executive Functions and the Improvement of Thinking Abilities: The Intervention in Reading Comprehension. Front. Psychol. 2016, 7, 58. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Friedman, L.; Ashford, J.W.; Kraemer, H.C.; Mumenthaler, M.S.; Noda, A.; Hoblyn, J. Acetylcholinesterase Inhibitor in Combination with Cognitive Training in Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2008, 63, P288–P294. [Google Scholar] [CrossRef]
- Carter, H.H.; Spence, A.L.; Pugh, C.J.A.; Ainslie, P.; Naylor, L.H.; Green, D.J. Cardiovascular Responses to Water Immersion in Humans: Impact on Cerebral Perfusion. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2014, 306, R636–R640. [Google Scholar] [CrossRef]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical Activity to Improve Cognition in Older Adults: Can Physical Activity Programs Enriched with Cognitive Challenges Enhance the Effects? A Systematic Review and Meta-Analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef]
- Zhu, H.-Q.; Luo, J.; Wang, X.-Q.; Zhang, X.-A. Non-Invasive Brain Stimulation for Osteoarthritis. Front. Aging Neurosci. 2022, 14, 987732. [Google Scholar] [CrossRef]
- Perrot, A.; Maillot, P. Factors for Optimizing Intervention Programs for Cognition in Older Adults: The Value of Exergames. NPJ Aging 2023, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Hiyamizu, M.; Morioka, S.; Shomoto, K.; Shimada, T. Effects of Dual Task Balance Training on Dual Task Performance in Elderly People: A Randomized Controlled Trial. Clin. Rehabil. 2012, 26, 58–67. [Google Scholar] [CrossRef]
- GrÉGoire, J.; Van Der Linden, M. Effect of Age on Forward and Backward Digit Spans. Aging Neuropsychol. Cogn. 1997, 4, 140–149. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics (Mean ± SD) | W Group (n = 18) | W-COG Group (n = 19) | t (Test)/x2 | p-Value |
|---|---|---|---|---|
| Age, yrs. | 68.39 ± 3.35 | 69.68 ± 3.85 | −1.09 | 0.283 |
| Weight, kg | 61.33 ± 8.76 | 56.36 ± 8.79 | 1.72 | 0.094 |
| Height, cm | 156.89 ± 5.94 | 155.68 ± 6.15 | 0.61 | 0.549 |
| Body mass index, kg/m2 | 24.60 ± 4.31 | 23.62 ± 2.70 | 0.82 | 0.4120 |
| % skeletal mass | 23.02 ± 2.91 | 22.81 ± 2.20 | 0.26 | 0.799 |
| % fat | 35.29 ± 5.75 | 35.60 ± 3.78 | −0.19 | 0.849 |
| MoCA scores | 21.61 ± 2.09 | 22.37 ± 1.16 | −1.35 | 0.188 |
| Resting HR, bpm | 76.94 ± 14.89 | 77.11 ± 9.79 | −1.01 | 0.320 |
| Gender (n) | 0.424 # | 0.515 | ||
| Female:male | 16:2 | 18:1 | ||
| Education background, n (%) | 1.53 # | 0.465 | ||
| - Primary school | 13 (72.2%) | 10 (52.6%) | ||
| - Secondary school | 3 (16.7%) | 5 (26.3%) | ||
| - University | 2 (11.1%) | 4 (21.1%) | ||
| Underlying diseases (n) | 3.695 # | 0.296 | ||
| 0:1:2: ≥ 3 | 3:5:5:5 | 7:7:3:2 | ||
| Exercise behavior, n (%) | 0.232 # | 0.630 | ||
| <3 days/week | 9 (50%) | 8 (42.1%) | ||
| ≥3 days/week | 9 (50%) | 11 (57.9%) | ||
| Cognitive Tests | Water-Based Exercise (n = 18) Mean ± SD | Significant Within W Gr. | Water-Based Exercise Combined with Cognitive Training (n = 19) Mean ± SD | Significant Within W-COG Gr. | Significant Between W and W-COG Grs. | ||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 12 Weeks | Mean Dif. | Baseline | 12 Weeks | Mean Dif. | ||||
| Montreal Cognitive Assessment (MoCA; score) | 21.88 ± 1.79 (n = 17) | 26.25 ± 2.46 *** (n = 17) | 4.37 ± 0.67 | F (1, 35) = 74.544, p < 0.001, ηp2 = 0.682 | 22.37 ± 1.16 | 27.32 ± 2.08 *** | 4.95 ± 0.92 | F (1, 35) = 92.803, p < 0.001, ηp2 = 0.726 | F (1, 35) = 2.365, p = 0.133, ηp2 = 0.063 |
| Digit Span Forward Test (DSFT; digit) | 7.44 ± 1.04 | 7.78 ± 0.87 | 0.34 ± 0.17 | F (1, 35) = 1.646, p = 0.208, ηp2 = 0.045 | 7.11 ± 1.15 | 7.26 ± 0.87 | 0.15 ± 0.28 | F (1, 35) = 0.390, p = 0.536, ηp2 = 0.011 | F (1, 35) = 3.197, p = 0.082, ηp2 = 0.084 |
| Digit Span Backward Test (DSBT; digit) | 3.44 ± 0.78 | 3.5 ± 0.61 | 0.06 ± 0.17 | F (1, 34) = 0.042, p = 0.839, ηp2 = 0.001 | 3.72 ± 0.89 (n = 18) | 3.72 ± 1.63 (n = 18) | 0 ± 0.74 | F (1, 34) = 0.000, p = 1.000, ηp2 = 0.000 | F (1, 34) = 0.279, p = 0.601, ηp2 = 0.008 |
| Stroop Color and Word Test (SCWT; time) | 62.81 ± 21.42 (n = 16) | 77.5 ± 26.58 (n = 16) | 14.69 ± 5.16 | F (1, 32) = 1.420, p = 0.242, ηp2 = 0.042 | 65.61 ± 34.64 (n = 18) | 55.44 ± 23.52 (n = 18) | 10.17 ± 11.12 | F (1, 32) = 2.188, p = 0.149, ηp2 = 0.064 | F (1, 32) = 3.492, p = 0.071, ηp2 = 0.098 |
| Trail-Making Test Part A (TMT-A; time) | 65.72 ± 23.25 | 51.11 ± 14.32 ** | 14.61 ± 8.93 | F (1, 34) = 11.130, p = 0.002, ηp2 = 0.247 | 57.44 ± 20.07 (n = 18) | 47.78 ± 19.05 * (n = 18) | 9.66 ± 1.02 | F (1, 34) = 4.872, p = 0.034, ηp2 = 0.125 | F (1, 34) = 0.352, p = 0.557, ηp2 = 0.010 |
| Trail-Making Test Part B (TMT-B; time) | 186.56 ± 72.40 | 178.33 ± 69.28 | 8.23 ± 3.12 | F (1, 33) = 0.670, p = 0. 419, ηp2 = 0.020 | 153.63 ± 68.80 | 125.63 ± 65.86 | 28 ± 2.94 a *, b * | F (1, 33) = 2.057, p = 0. 161, ηp2 = 0.059 | a: F (1, 33) = 5.613, p = 0.024, ηp2 = 0.142 b: F (1, 33) = 5.813, p = 0.021, ηp2 = 0.146 |
| Trail-Making Test Part B-A (TMT B-A; time) | 86.89 ± 49.76 | 102.61 ± 52.90 | 6.39 ± 79.50 | F (1, 33) = 0.010, p = 0.921, ηp2 = 0.000 | 127.79 ± 62.21 | 97.79 ± 59.53 | 21.16 ± 48.31 c * | F (1, 33) = 1.331, p = 0.257, ηp2 = 0.039 | F (1, 33) = 6.775, p = 0.014, ηp2 = 0.170 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meekum, S.; Yuenyongchaiwat, K.; Luangpon, N.; Keawutan, P.; Kooncumchoo, P. Enhancing Global Cognition and Executive Functions Through Water-Based Exercise in Mild Cognitive Impairment: A Randomized Controlled Trial. Life 2025, 15, 420. https://doi.org/10.3390/life15030420
Meekum S, Yuenyongchaiwat K, Luangpon N, Keawutan P, Kooncumchoo P. Enhancing Global Cognition and Executive Functions Through Water-Based Exercise in Mild Cognitive Impairment: A Randomized Controlled Trial. Life. 2025; 15(3):420. https://doi.org/10.3390/life15030420
Chicago/Turabian StyleMeekum, Sutaya, Kornanong Yuenyongchaiwat, Nongnuch Luangpon, Piyapa Keawutan, and Patcharee Kooncumchoo. 2025. "Enhancing Global Cognition and Executive Functions Through Water-Based Exercise in Mild Cognitive Impairment: A Randomized Controlled Trial" Life 15, no. 3: 420. https://doi.org/10.3390/life15030420
APA StyleMeekum, S., Yuenyongchaiwat, K., Luangpon, N., Keawutan, P., & Kooncumchoo, P. (2025). Enhancing Global Cognition and Executive Functions Through Water-Based Exercise in Mild Cognitive Impairment: A Randomized Controlled Trial. Life, 15(3), 420. https://doi.org/10.3390/life15030420