
Prognostic and Clinical Significance of PD-L1, EGFR and Androgen Receptor (AR) Expression in Triple-Negative Breast Cancer (TNBC) Patients

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Tissue Samples
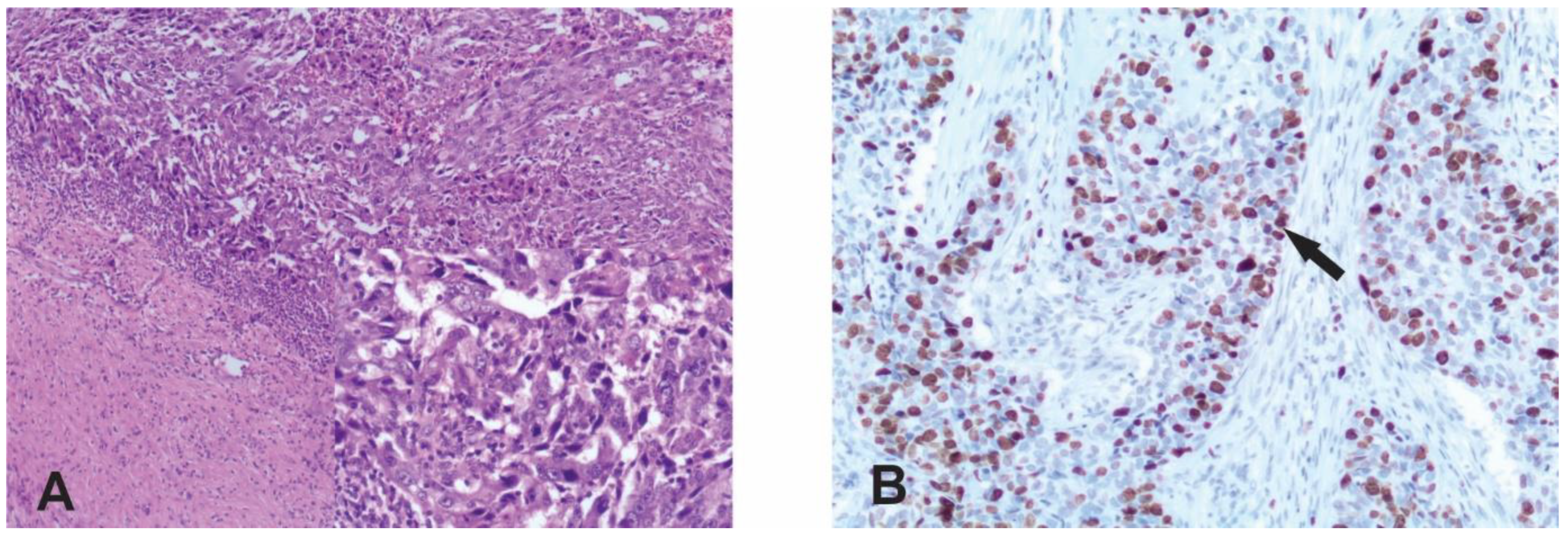
2.2. Immunohistochemistry
2.3. Evaluation of Staining
2.4. Statistical Analysis
3. Results
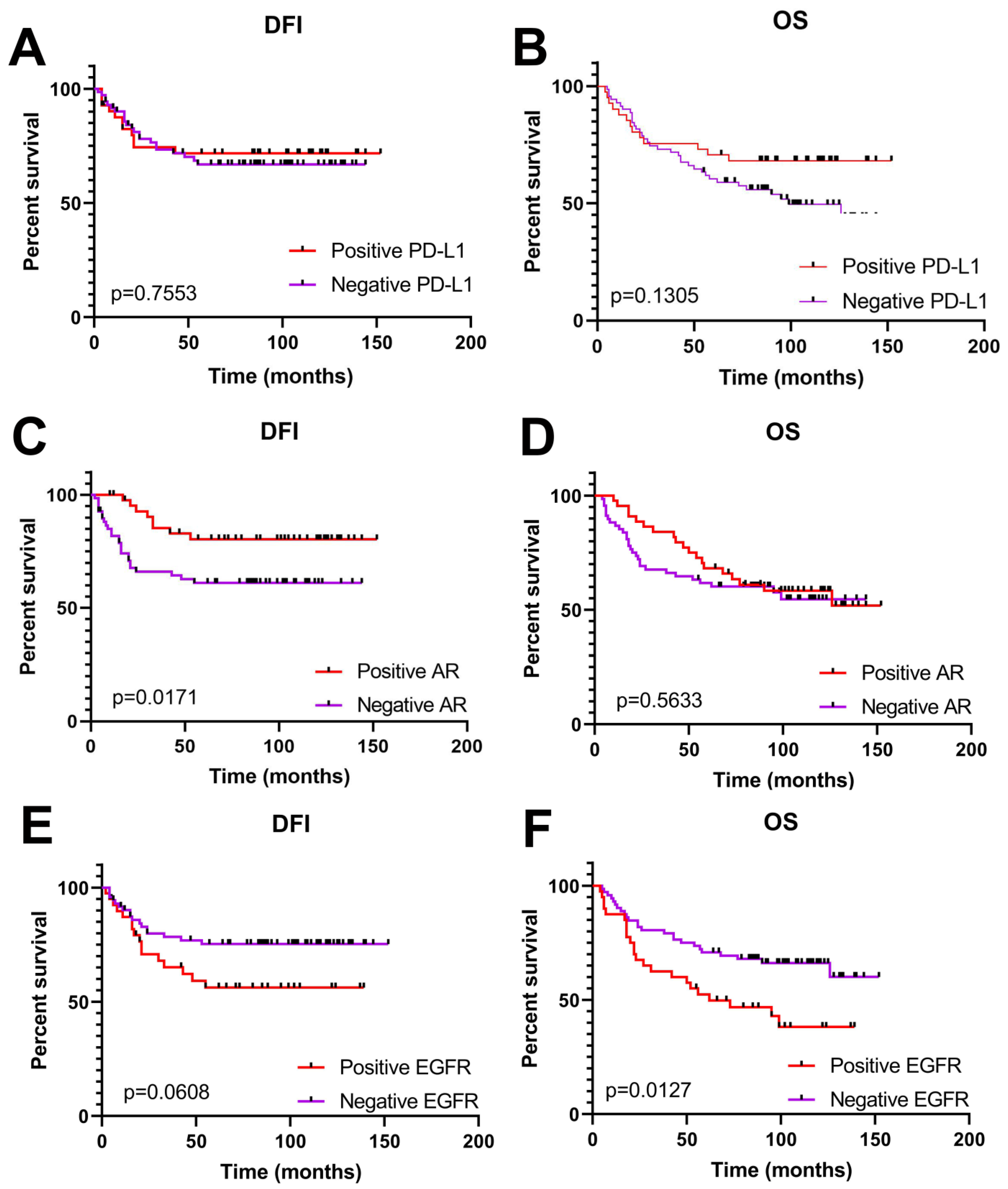
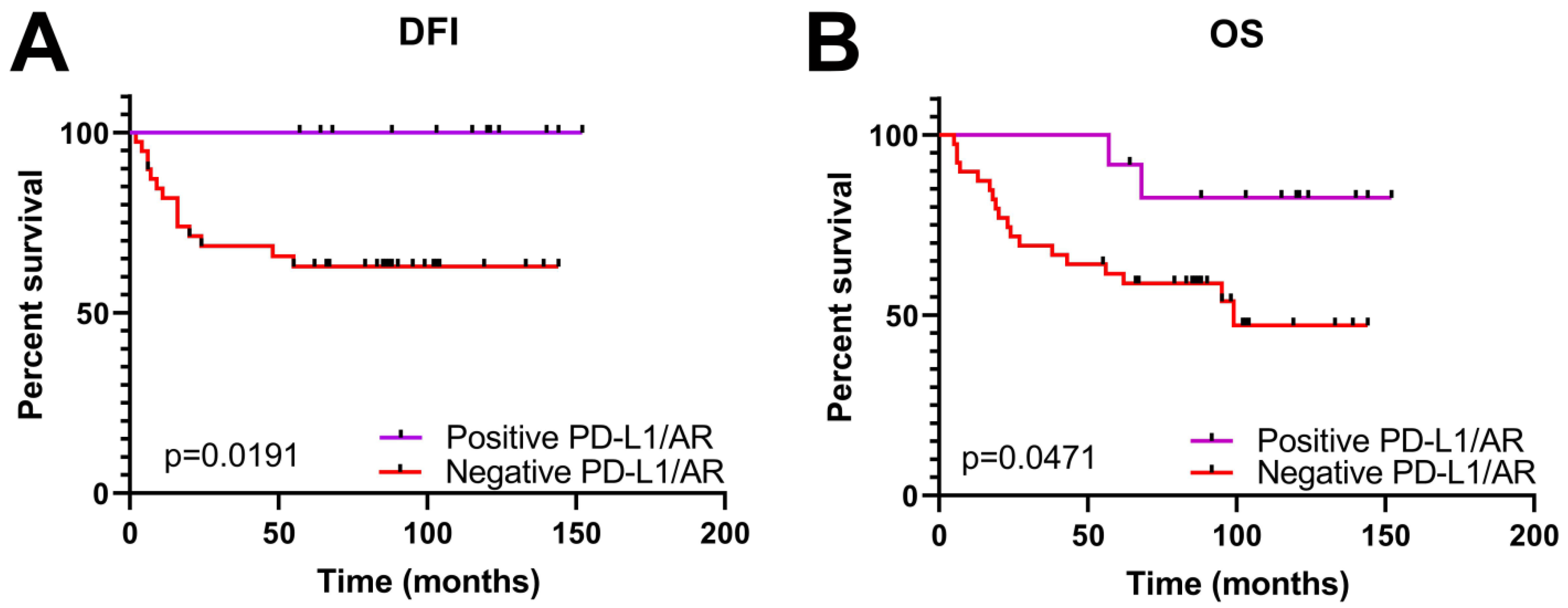
Clinical Significance of PD-L1, AR and EGFR Expression in TNBC Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Zagami, P.; Carey, L.A. Triple negative breast cancer: Pitfalls and progress. npj Breast Cancer 2022, 8, 95. [Google Scholar] [CrossRef]
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin. Cancer Res. 2007, 13, 4429–4434. [Google Scholar] [CrossRef]
- Kennecke, H.; Yerushalmi, R.; Woods, R.; Cheang, M.C.; Voduc, D.; Speers, C.H.; Nielsen, T.O.; Gelmon, K. Metastatic behavior of breast cancer subtypes. J. Clin. Oncol. 2010, 28, 3271–3277. [Google Scholar] [CrossRef] [PubMed]
- Nedeljković, M.; Damjanović, A. Mechanisms of Chemotherapy Resistance in Triple-Negative Breast Cancer—How We Can Rise to the Challenge. Cells 2019, 8, 957. [Google Scholar] [CrossRef] [PubMed]
- Herrera Juarez, M.; Tolosa Ortega, P.; Sanchez de Torre, A.; Ciruelos Gil, E. Biology of the Triple-Negative Breast Cancer: Immunohistochemical, RNA, and DNA Features. Breast Care 2020, 15, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wu, J.; Zhang, P.; Fei, X.; Zong, Y.; Chen, X.; Huang, O.; He, J.-R.; Chen, W.; Li, Y.; et al. Prognostic and predictive value of Ki-67 in triple-negative breast cancer. Oncotarget 2016, 7, 31079–31087. [Google Scholar] [CrossRef] [PubMed]
- Thike, A.A.; Chong, L.Y.Z.; Cheok, P.Y.; Li, H.H.; Yip, G.W.C.; Bay, B.H.; Tse, G.M.K.; Iqbal, J.; Tan, P.H. Loss of androgen receptor expression predicts early recurrence in triple-negative and basallike breast cancer. Mod. Pathol. 2014, 27, 352–360. [Google Scholar] [CrossRef]
- Rampurwala, M.; Wisinski, K.B.; O’Regan, R. Role of the androgen receptor in triple-negative breast cancer. Clin. Adv. Hematol. Oncol. 2016, 14, 186–193. [Google Scholar]
- Chen, M.; Yang, Y.; Xu, K.; Li, L.; Huang, J.; Qiu, F. Androgen Receptor in Breast Cancer: From Bench to Bedside. Front. Endocrinol. 2020, 11, 573. [Google Scholar] [CrossRef]
- Gumuskaya, B.; Alper, M.; Hucumenoglu, S.; Altundag, K.; Uner, A.; Guler, G. EGFR expression and gene copy number in triple-negative breast carcinoma. Cancer Genet. Cytogenet. 2010, 203, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Heinlein, C.A.; Chang, C. Androgen receptor in prostate cancer. Endocr Rev. 2004, 25, 276–308. [Google Scholar] [CrossRef] [PubMed]
- Pignon, J.C.; Koopmansch, B.; Nolens, G.; Delacroix, L.; Waltregny, D.; Winkler, R. Androgen Receptor Controls EGFR and ERBB2 Gene Expression at Different Levels in Prostate Cancer Cell Lines. Cancer Res. 2009, 69, 2941–2949. [Google Scholar] [CrossRef] [PubMed]
- Fard, S.S.; Saliminejad, K.; Sotoudeh, M.; Soleimanifard, N.; Kouchaki, S.; Yazdanbod, M.; Mahmoodzadeh, H.; Ghavamzadeh, A.; Malekzadeh, R.; Chahardouli, B.; et al. The Correlation between EGFR and Androgen Receptor Pathways: A Novel Potential Prognostic Marker in Gastric Cancer. Anti Cancer Agents Med. Chem. 2019, 19, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, T.S.; HuLieskovan, S.; Ribas, A. Mechanisms of resistance to PD1 and PDL1 blockade. Cancer J. 2018, 24, 4753. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.; Gatti-Mays, M.E.; Kalinsky, K.; Korde, L.A.; Sharon, E.; Amiri-Kordestani, L.; Mittendorf, E.A. Current landscape of immunotherapy in breast cancer: A review. JAMA Oncol. 2019, 5, 1205–1214. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, S.R.; Ellis, I.O.; Schnitt Tan, P.H.; van de Vijver, M.J. WHO Classification of Tumours of the Breast, 4th ed.; IARC Press: Lyon, France, 2012. [Google Scholar]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; International Union Against Cancer Wiley–Blackwell: Geneva, Switzerland, 2009. [Google Scholar]
- Allred, D.C.; Harvey, J.M.; Berardo, M.; Clark, G.M. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod. Pathol. 1998, 11, 155–168. [Google Scholar] [PubMed]
- Dias, K.; Dvorkin-Gheva, A.; Hallett, R.M.; Wu, Y.; Hassell, J.; Pond, G.R.; Levine, M.; Whelan, T.; Bane, A.L. Claudin-Low Breast Cancer; Clinical & Pathological Characteristics. PLoS ONE 2017, 12, e0168669. [Google Scholar]
- Hammond, M.E.H.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College of American Pathologists Guideline Recommendation for Immunohistochemical Testing of Estrogen and Progesterone receptors in Breast Cancer. J. Clin. Oncol. 2010, 28, 2784–2795. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for Human Epidermal Growth Factor receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologist Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef] [PubMed]
- HerceptTest™. For Determination of HER2 Protein Overexpression. In Catalog Products and Services; DAKO: Jena, Germany, 2007; pp. 86–87. [Google Scholar]
- Denkert, C.; Loibl, S.; Müller, B.M.; Eidtmann, H.; Schmitt, W.D.; Eiermann, W.; Gerber, B.; Tesch, H.; Hilfrich, J.; Huober, J.; et al. Ki67 levels as predictive and prognostic parameters in pretherapeutic breast cancer core biopsies: A translational investigation in the neoadjuvant GeparTrio trial. Ann. Oncol. 2013, 24, 2786–2793. [Google Scholar] [CrossRef] [PubMed]
- McGhan, L.J.; McCullough, A.E.; Protheroe, C.A.; Dueck, A.C.; Lee, J.J.; Nunez-Nateras, R.; Castle, E.P.; Gray, R.J.; Wasif, N.; Goetz, M.P.; et al. Androgen receptor-positive triple negative breast cancer: A unique breast cancer subtype. Ann. Surg. Oncol. 2014, 21, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Dako Agilent Tehnologies. PD-L1 IHC 22C3 pharmDx Interpretation Manual—Triple Negative Breast Cancer (TNBC); DAKO Agilend: Jena, Germany, 2020; p. 24. [Google Scholar]
- Keir, M.E.; Liang, S.C.; Guleria, I.; Latchman, Y.E.; Qipo, A.; Albacker, L.A.; Koulmanda, M.; Freeman, G.J.; Sayegh, M.H.; Sharpe, A.H. Tissue expression of PD-L1 mediates peripheral T cell tolerance. J. Exp. Med. 2006, 203, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Stanowska, O.; Kuczkiewicz-Siemion, O.; Debowska, M.; Olszewski, W.P.; Jagiełło-Gruszfeld, A.; Tysarowski, A.; Prochorec-Sobieszek, M. PD-L1-Positive High-Grade Triple-Negative Breast Cancer Patients Respond Better to Standard Neoadjuvant Treatment—A Retrospective Study of PD-L1 Expression in Relation to Different Clinicopathological Parameters. J. Clin. Med. 2022, 11, 5524. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhu, H.; Zhou, Y.; Mao, F.; Lin, Y.; Pan, B.; Zhang, X.; Xu, Q.; Huang, X.; Sun, Q. Prognostic Value of PD-L1 in Breast Cancer: A Meta-Analysis. Breast J. 2017, 23, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Sabatier, R.; Finetti, P.; Mamessier, E.; Adelaide, J.; Chaffanet, M.; Ali, H.; Viens, P.; Caldas, C.; Birnbaum, D.; Bertucci, F. Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget 2015, 6, 5449–5464. [Google Scholar] [CrossRef] [PubMed]
- Astvatsaturyan, K.; Yue, Y.; Walts, A.E.; Bose, S. Androgen receptor positive triple negative breast cancer: Clinicopathologic, prognostic, and predictive features. PLoS ONE 2018, 13, e0197827. [Google Scholar] [CrossRef] [PubMed]
- Hackbart, H.; Cui, X.; Lee, J.S. Androgen receptor in breast cancer and its clinical implication. Transl. Breast Cancer Res. 2023, 4, 30. [Google Scholar] [CrossRef]
- Dubrava, A.L.; Kyaw, P.S.P.; Newman, J.; Pringle, J.; Westhuyzen, J.; La Hera Fuentes, G.; Shakespeare, T.P.; Sakalkale, R.; Aherne, N.J. Androgen Receptor Status in Triple Negative Breast Cancer: Does It Correlate with Clinicopathological Characteristics? Breast Cancer; Dove Med Press: Macclesfield, UK, 2023; Volume 11, pp. 359–371. [Google Scholar]
- Tung, N.; Garber, J.E.; Hacker, M.R.; Torous, V.; Freeman, G.J.; Poles, E.; Rodig, S.; Alexander, B.; Lee, L.; Collins, L.C.; et al. Prevalence and predictors of androgen receptor and programmed death-ligand 1 in BRCA1-associated and sporadic triple-negative breast cancer. NPJ Breast Cancer 2016, 2, 16002. [Google Scholar] [CrossRef]
- Quan, Z.; Yang, Y.; Zheng, H.; Zhan, Y.; Luo, J.; Ning, Y.; Fan, S. Clinical implications of the interaction between PD-1/PD-L1 and PI3K/AKT/mTOR pathway in progression and treatment of non-small cell lung cancer. J. Cancer. 2022, 13, 3434–3443. [Google Scholar] [CrossRef] [PubMed]
- Prvanović, M.; Nedeljković, М.; Tanić, N.; Tomić, T.; Terzić, T.; Milovanović, Z.; Maksimović, Z.; Tanić, N. Role of PTEN, PI3K, and mTOR in Triple-Negative Breast Cancer. Life 2021, 11, 1247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | np (%) |
|---|---|
| Age at diagnosis | |
| <50 | 99 (79.2) |
| ≥50 | 26 (20.8) |
| Tumor type | |
| Ductal | 79 (63.2) |
| Lobular | 16 (12.8) |
| Mixed (ductal/lobular) | 11 (8.8) |
| Other * | 19 (15.2) |
| Tumor size (cm) | |
| ≤2 | 38 (30.4) |
| 2 -5 | 76 (60.8) |
| ≥5 | 11 (8.8) |
| Tumor grade | |
| G2 | 58 (46.4) |
| G3 | 67 (53.6) |
| Nuclear grade | |
| NG1 | 5 (4) |
| NG2 | 51 (40.8) |
| NG3 | 69 (55.2) |
| Lymph node status | |
| Negative | 79 (63.2) |
| Positive | 45 (36) |
| Unknown | 1 (0.8) |
| Locoregional reccurance | |
| No | 112 (89.6) |
| Yes | 13 (10.4) |
| Distant metastases | |
| No | 96 (76.8) |
| Yes | 29 (23.2) |
| PD-L1 | AR | EGFR | |||||||
|---|---|---|---|---|---|---|---|---|---|
| np (%) | np (%) | np (%) | |||||||
| Parameters | Negative | Positive | p value | Negative | Positive | p value | Negative | Positive | p value |
| 75 (60) | 50 (40) | 79 (63) | 46 (37) | 83 (66) | 42 (34) | ||||
| Tumor size | |||||||||
| ≤2 cm | 23 (30) | 15 (30) | 0.6417 | 21 (26) | 17 (37) | 0.4657 | 27 (33) | 11 (24) | 0.5844 |
| 2 -5 cm | 44 (59) | 32 (64) | 51 (65) | 25 (54) | 50 (60) | 26 (62) | |||
| >5 cm | 8 (11) | 3 (6) | 7 (9) | 4 (9) | 6 (7) | 5 (14) | |||
| Tumor grade | |||||||||
| G2 | 45 (60) | 13 (26) | 0.0002 | 31 (39) | 27 (59) | 0.0419 | 36 (43) | 22 (52) | 0.3505 |
| G3 | 30 (40) | 37 (74) | 48 (61) | 19 (41) | 47 (57) | 20 (48) | |||
| Nuclear grade | |||||||||
| NG1 | 4 (5) | 1 (2) | 0.0007 | 4 (5) | 1 (2) | 0.2425 | 2 (2) | 3 (7) | 0.3796 |
| NG2 | 40 (54) | 11 (22) | 28 (35) | 23 (50) | 33 (40) | 18 (43) | |||
| NG3 | 31 (41) | 38 (76) | 47 (60) | 22 (48) | 48 (58) | 21 (50) | |||
| Lymph node status | |||||||||
| Negative | 45 (60) | 34 (69) | 0.3416 | 51 (65) | 28 (61) | 0.6998 | 55 (67) | 24 (57) | 0.3255 |
| Positive | 30 (40) | 15 (31) | 27 (35) | 18 (39) | 27 (33) | 18 (43) | |||
| N stage | |||||||||
| N0 | 45 (60) | 34 (69) | 0.5684 | 51 (65) | 28 (61) | 0.4912 | 55 (67) | 24 (57) | 0.4946 |
| N1 | 24 (32) | 12 (25) | 23 (30) | 13 (28) | 21 (26) | 15 (36) | |||
| N2 and N3 | 6 (8) | 3 (6) | 4 (5) | 5 (11) | 6 (7) | 3 (7) | |||
| Metastases | |||||||||
| No | 57 (76) | 39 (78) | 0.8322 | 57 (72) | 39 (85) | 0.1273 | 69 (83) | 27 (64) | 0.0249 |
| Yes | 18 (24) | 11 (22) | 22 (28) | 7 (15) | 14 (17) | 15 (36) | |||
| Locoreg. reccurence | |||||||||
| No | 63 (84) | 49 (98) | 0.0146 | 69 (87) | 43 (93) | 0.368 | 75 (90) | 37 (88) | 0.7597 |
| Yes | 12 (16) | 1 (2) | 10 (13) | 3 (7) | 8 (10) | 5 (12) | |||
| Adjuvant radiotherapy | |||||||||
| No | 28 (37) | 16 (33) | 0.7008 | 27 (34) | 17 (38) | 0.8457 | 27 (34) | 17 (40) | 0.5524 |
| Yes | 46 (63) | 32 (67) | 50 (66) | 28 (62) | 53 (66) | 25 (60) | |||
| Ki67 | |||||||||
| ≤15% | 14 (19) | 2 (4) | 0.0148 | 1 (1) | 15 (32) | <0.0001 | 11 (13) | 5 (12) | 0.1831 |
| 16–30% | 8 (11) | 2 (4) | 4 (5) | 6 (14) | 4 (5) | 6 (14) | |||
| >30% | 53 (70) | 46 (92) | 74 (94) | 25 (54) | 68 (82) | 31 (74) | |||
| PD-L1/AR Expression | |||
|---|---|---|---|
| np (%) | |||
| Parameters | Negative | Positive | p value |
| 42 (76) | 13 (24) | ||
| Tumor size | |||
| ≤2 cm | 10 (24) | 4 (31) | 0.8344 |
| 2–5 | 27 (64) | 8 (62) | |
| >5 cm | 5 (12) | 1 (7) | |
| Tumor grade | |||
| G2 | 20 (48) | 2 (15) | 0.0533 |
| G3 | 22 (52) | 11 (85) | |
| Nuclear grade | |||
| NG1 | 3 (7) | 0 (0) | 0.0242 |
| NG2 | 18 (43) | 1 (7) | |
| NG3 | 21 (50) | 12 (93) | |
| Lymph nodes status | |||
| Negative | 28 (67) | 11 (85) | 0.3037 |
| Positive | 14 (33) | 2 (15) | |
| N stage | |||
| N0 | 28 (67) | 11 (85) | 0.2955 |
| N1 | 12 (28) | 1 (7) | |
| N2 and N3 | 2 (5) | 1 (7) | |
| Metastases | |||
| No | 31 (74) | 13 (100) | 0.0497 |
| Yes | 11 (26) | 0 (0) | |
| Locoreg. reccurence | |||
| No | 33 (79) | 13 (100) | 0.0961 |
| Yes | 9 (21) | 0 (0) | |
| Adjuvant radiotherapy | |||
| No | 15 (36) | 4 (33) | >0.9999 |
| Yes | 26 (64) | 8 (67) | |
| Ki67 | |||
| ≤15% | 0 (0) | 1 (7) | 0.1452 |
| 16–30% | 2 (5) | 0 (0) | |
| >30% | 40 (95) | 12 (93) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medić-Milijić, N.; Jovanić, I.; Nedeljković, M.; Marković, I.; Spurnić, I.; Milovanović, Z.; Ademović, N.; Tomić, T.; Tanić, N.; Tanić, N. Prognostic and Clinical Significance of PD-L1, EGFR and Androgen Receptor (AR) Expression in Triple-Negative Breast Cancer (TNBC) Patients. Life 2024, 14, 682. https://doi.org/10.3390/life14060682
Medić-Milijić N, Jovanić I, Nedeljković M, Marković I, Spurnić I, Milovanović Z, Ademović N, Tomić T, Tanić N, Tanić N. Prognostic and Clinical Significance of PD-L1, EGFR and Androgen Receptor (AR) Expression in Triple-Negative Breast Cancer (TNBC) Patients. Life. 2024; 14(6):682. https://doi.org/10.3390/life14060682
Chicago/Turabian StyleMedić-Milijić, Nataša, Irena Jovanić, Milica Nedeljković, Ivan Marković, Igor Spurnić, Zorka Milovanović, Nejla Ademović, Tijana Tomić, Nasta Tanić, and Nikola Tanić. 2024. "Prognostic and Clinical Significance of PD-L1, EGFR and Androgen Receptor (AR) Expression in Triple-Negative Breast Cancer (TNBC) Patients" Life 14, no. 6: 682. https://doi.org/10.3390/life14060682
APA StyleMedić-Milijić, N., Jovanić, I., Nedeljković, M., Marković, I., Spurnić, I., Milovanović, Z., Ademović, N., Tomić, T., Tanić, N., & Tanić, N. (2024). Prognostic and Clinical Significance of PD-L1, EGFR and Androgen Receptor (AR) Expression in Triple-Negative Breast Cancer (TNBC) Patients. Life, 14(6), 682. https://doi.org/10.3390/life14060682