
Medication Overuse Headaches among Children—The Contribution of Migraine and TTH

 ,
,  ,
,
Abstract
:1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guidetti, V.; Galli, F. Evolution of Headache in Childhood and Adolescence: An 8-Year Follow-Up. Cephalalgia Int. J. Headache 1998, 18, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, G.; Suzuki, S.; Takeshita, M.; Go, S.; Morishita, N.; Takamatsu, T.; Daida, A.; Morichi, S.; Ishida, Y.; Oana, S.; et al. Effectiveness of Low-Dose Riboflavin as a Prophylactic Agent in Pediatric Migraine. Brain Dev. 2020, 42, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Vides-Rosales, M. Pediatric Medication-Overuse Headache and Global Headache Research. A Systematic Review. Semin. Pediatr. Neurol. 2021, 40, 100937. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.-C.; Dodick, D.; Evers, S.; Holle, D.; Jensen, R.H.; Lipton, R.B.; Porreca, F.; Silberstein, S.; Schwedt, T. Pathophysiology, Prevention, and Treatment of Medication Overuse Headache. Lancet Neurol. 2019, 18, 891–902. [Google Scholar] [CrossRef] [PubMed]
- Find, N.L.; Terlizzi, R.; Munksgaard, S.B.; Bendtsen, L.; Tassorelli, C.; Nappi, G.; Katsarava, Z.; Lainez, M.; Goicochea, M.T.; Shand, B.; et al. Medication Overuse Headache in Europe and Latin America: General Demographic and Clinical Characteristics, Referral Pathways and National Distribution of Painkillers in a Descriptive, Multinational, Multicenter Study. J. Headache Pain 2015, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Manack, A.; Ricci, J.A.; Chee, E.; Turkel, C.C.; Winner, P. Prevalence and Burden of Chronic Migraine in Adolescents: Results of the Chronic Daily Headache in Adolescents Study (C-DAS). Headache 2011, 51, 693–706. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.; Hayes, J.; Pakalnis, A. A Randomized Trial of Telephone-Based Motivational Interviewing for Adolescent Chronic Headache with Medication Overuse. Cephalalgia Int. J. Headache 2014, 34, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Kemper, K.J.; Heyer, G.; Pakalnis, A.; Binkley, P.F. What Factors Contribute to Headache-Related Disability in Teens? Pediatr. Neurol. 2016, 56, 48–54. [Google Scholar] [CrossRef]
- Lau, C.I.; Chen, W.-H.; Wang, H.-C.; Walsh, V. Decision-Making Impairment under Ambiguity but Not under Risk May Underlie Medication Overuse in Patients with Chronic Migraine. Headache 2023, 63, 822–833. [Google Scholar] [CrossRef]
- Constantinidis, T.S.; Arvaniti, C.; Fakas, N.; Rudolf, J.; Kouremenos, E.; Giannouli, E.; Mitsikostas, D.D. Hellenic Headache Society The Prevalence and Burden of Medication Overuse Headache in Greece. Cephalalgia Int. J. Headache 2023, 43, 3331024231184909. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd Edition. Cephalalgia Int. J. Headache 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- Westergaard, M.L.; Hansen, E.H.; Glümer, C.; Olesen, J.; Jensen, R.H. Definitions of Medication-Overuse Headache in Population-Based Studies and Their Implications on Prevalence Estimates: A Systematic Review. Cephalalgia Int. J. Headache 2014, 34, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Ew, L.; Ai, S. Medication Overuse Headache: The Trouble with Prevalence Estimates. Cephalalgia Int. J. Headache 2020, 40, 3–5. [Google Scholar] [CrossRef]
- Westergaard, M.L.; Glümer, C.; Hansen, E.H.; Jensen, R.H. Prevalence of Chronic Headache with and without Medication Overuse: Associations with Socioeconomic Position and Physical and Mental Health Status. Pain 2014, 155, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.-C.; Limmroth, V. Medication-Overuse Headache: A Worldwide Problem. Lancet Neurol. 2004, 3, 475–483. [Google Scholar] [CrossRef]
- Soee, A.-B.L.; Skov, L.; Skovgaard, L.T.; Thomsen, L.L. Headache in Children: Effectiveness of Multidisciplinary Treatment in a Tertiary Paediatric Headache Clinic. Cephalalgia Int. J. Headache 2013, 33, 1218–1228. [Google Scholar] [CrossRef]
- Papetti, L.; Salfa, I.; Battan, B.; Moavero, R.; Termine, C.; Bartoli, B.; Di Nunzio, F.; Tarantino, S.; Alaimo Di Loro, P.; Vigevano, F.; et al. Features of Primary Chronic Headache in Children and Adolescents and Validity of Ichd 3 Criteria. Front. Neurol. 2019, 10, 92. [Google Scholar] [CrossRef]
- Heyer, G.L.; Idris, S.A. Does Analgesic Overuse Contribute to Chronic Post-Traumatic Headaches in Adolescent Concussion Patients? Pediatr. Neurol. 2014, 50, 464–468. [Google Scholar] [CrossRef]
- Munksgaard, S.B.; Bendtsen, L.; Jensen, R.H. Treatment-Resistant Medication Overuse Headache Can Be Cured. Headache 2012, 52, 1120–1129. [Google Scholar] [CrossRef] [PubMed]
- Genizi, J.; Lahat, E.; Zelnik, N.; Mahajnah, M.; Ravid, S.; Shahar, E. Childhood-Onset Idiopathic Intracranial Hypertension: Relation of Sex and Obesity. Pediatr. Neurol. 2007, 36, 247–249. [Google Scholar] [CrossRef]
- Genizi, J.; Srugo, I.; Kerem, N.C. The Cross- Ethnic Variations in the Prevalence of Headache and Other Somatic Complaints among Adolescents in Northern Israel. J. Headache Pain 2013, 14, 21. [Google Scholar] [CrossRef]
- Wöber, C.; Wöber-Bingöl, Ç.; Uluduz, D.; Aslan, T.S.; Uygunoglu, U.; Tüfekçi, A.; Alp, S.I.; Duman, T.; Sürgün, F.; Emir, G.K.; et al. Undifferentiated Headache: Broadening the Approach to Headache in Children and Adolescents, with Supporting Evidence from a Nationwide School-Based Cross-Sectional Survey in Turkey. J. Headache Pain 2018, 19, 18. [Google Scholar] [CrossRef]
- Genizi, J.; Bugdnoskya, V.; Aboud, A.; Segal, I.; Assaf, N.; Srugo, I.; Kerem, N.C. Migraine and Tension-Type Headache Among Children and Adolescents: Application of International Headache Society Criteria in a Clinical Setting. J. Child Neurol. 2021, 36, 618–624. [Google Scholar] [CrossRef]
- Togha, M.; Rafiee, P.; Ghorbani, Z.; Khosravi, A.; Şaşmaz, T.; Akıcı Kale, D.; Uluduz, D.; Steiner, T.J. The Prevalence of Headache Disorders in Children and Adolescents in Iran: A Schools-Based Study. Cephalalgia Int. J. Headache 2022, 42, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Limmroth, V.; Katsarava, Z.; Fritsche, G.; Przywara, S.; Diener, H.-C. Features of Medication Overuse Headache Following Overuse of Different Acute Headache Drugs. Neurology 2002, 59, 1011–1014. [Google Scholar] [CrossRef] [PubMed]
- Thorlund, K.; Sun-Edelstein, C.; Druyts, E.; Kanters, S.; Ebrahim, S.; Bhambri, R.; Ramos, E.; Mills, E.J.; Lanteri-Minet, M.; Tepper, S. Risk of Medication Overuse Headache across Classes of Treatments for Acute Migraine. J. Headache Pain 2016, 17, 107. [Google Scholar] [CrossRef] [PubMed]
- Ayzenberg, I.; Obermann, M.; Nyhuis, P.; Gastpar, M.; Limmroth, V.; Diener, H.C.; Kaube, H.; Katsarava, Z. Central Sensitization of the Trigeminal and Somatic Nociceptive Systems in Medication Overuse Headache Mainly Involves Cerebral Supraspinal Structures. Cephalalgia Int. J. Headache 2006, 26, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, A.; Serrao, M.; Sandrini, G.; Burstein, R.; Sances, G.; Rossi, P.; Bartolo, M.; Pierelli, F.; Nappi, G. Sensitisation of Spinal Cord Pain Processing in Medication Overuse Headache Involves Supraspinal Pain Control. Cephalalgia Int. J. Headache 2010, 30, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Coppola, G.; Currà, A.; Di Lorenzo, C.; Parisi, V.; Gorini, M.; Sava, S.L.; Schoenen, J.; Pierelli, F. Abnormal Cortical Responses to Somatosensory Stimulation in Medication-Overuse Headache. BMC Neurol. 2010, 10, 126. [Google Scholar] [CrossRef] [PubMed]
- Lai, T.-H.; Wang, S.-J. Neuroimaging Findings in Patients with Medication Overuse Headache. Curr. Pain Headache Rep. 2018, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, C.; Di Lorenzo, G.; Sances, G.; Ghiotto, N.; Guaschino, E.; Grieco, G.S.; Santorelli, F.M.; Casali, C.; Troisi, A.; Siracusano, A.; et al. Drug Consumption in Medication Overuse Headache Is Influenced by Brain-Derived Neurotrophic Factor Val66Met Polymorphism. J. Headache Pain 2009, 10, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Cargnin, S.; Viana, M.; Ghiotto, N.; Bianchi, M.; Sances, G.; Tassorelli, C.; Nappi, G.; Canonico, P.L.; Genazzani, A.A.; Terrazzino, S. Functional Polymorphisms in COMT and SLC6A4 Genes Influence the Prognosis of Patients with Medication Overuse Headache after Withdrawal Therapy. Eur. J. Neurol. 2014, 21, 989–995. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total | Migraine | TTH | Undifferentiated Type | ||
|---|---|---|---|---|---|
| Total cases | 1008 | 268 | 250 | 490 | |
| Gender | Male (%) | 480 (48) | 148 (55.1) | 102 (40.8) | 230 (47.1) |
| Female (%) | 528 (52) | 120 (44.9) | 148 (59.1) | 260 (53) | |
| Average age (years) | 11 | 11.5 | 11.23 | 10.46 |
| Characteristics | Medication Overuse Headache | p-Value | |
|---|---|---|---|
| No | Yes | ||
| n = 986 1 | n = 26 1 | ||
| Age | 10.9 (3.4) | 12.4 (3.0) | 0.024 |
| Gender | 0.033 | ||
| M | 474 (48%) | 7 (27%) | |
| F | 512 (52%) | 19 (73%) | |
| Headache type | 0.11 | ||
| Migraine | 262 (27%) | 6 (23%) | |
| Tension type | 241 (24%) | 11 (42%) | |
| Undifferentiated type | 483 (49%) | 9 (35%) | |
| Symptoms duration (months) | 12 (15) | 25 (28) | 0.04 |
| Characteristics | Medication Overuse Headache | p-Value | |
|---|---|---|---|
| No n = 986 1 | Yes n = 26 | ||
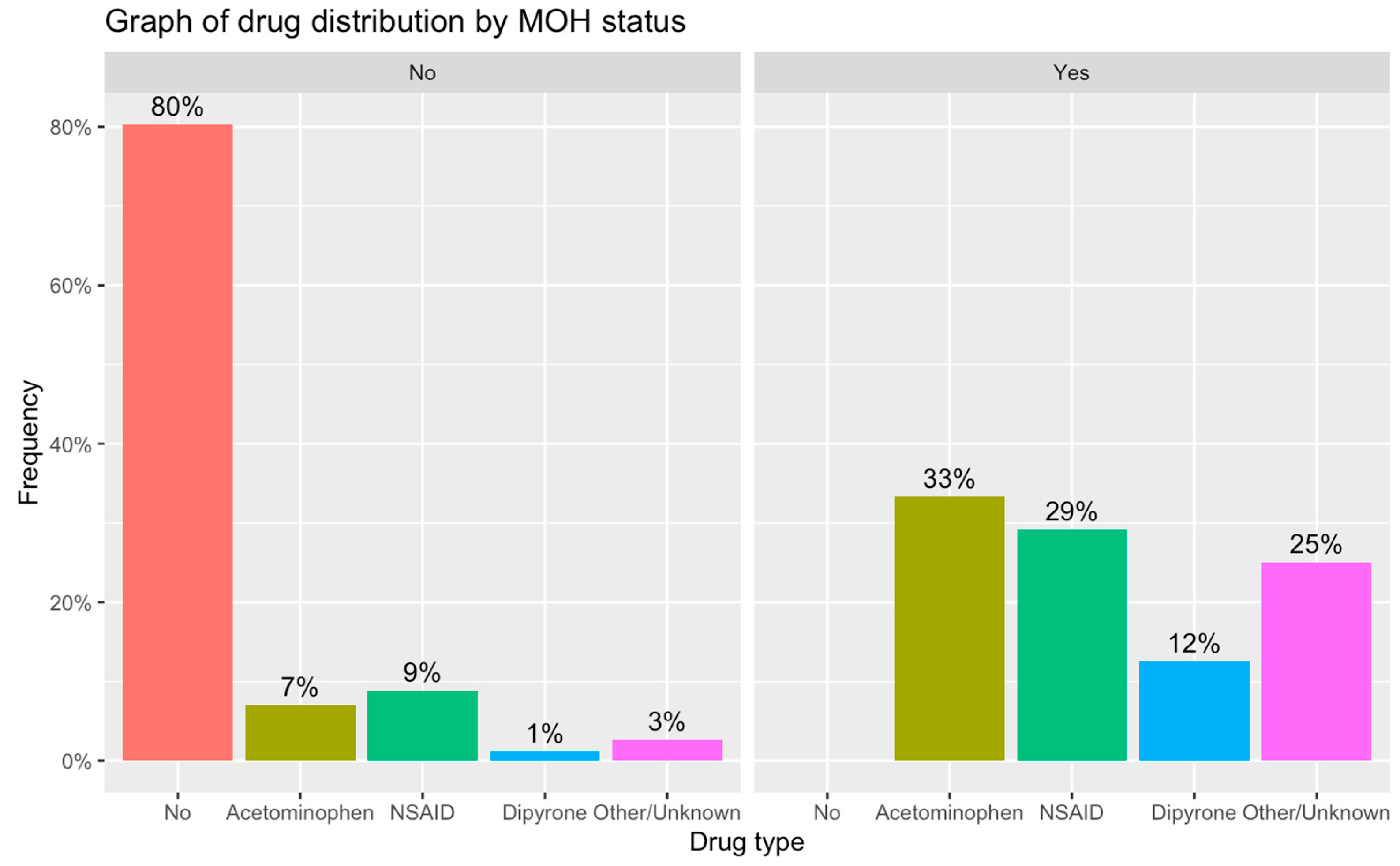
| Drug | <0.001 | ||
| No | 774 (80%) | 0 (0%) | |
| Acetaminophen | 68 (7.1%) | 8 (33%) | |
| NSAID | 85 (8.8%) | 7 (29%) | |
| Dipyrone | 11 (1.1%) | 3 (12%) | |
| Other/Unknown | 26 (2.7%) | 6 (25%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genizi, J.; Shnaider, M.; Yaniv, L.; Kerem, N.C.; Nathan, K.; Chistyakov, I. Medication Overuse Headaches among Children—The Contribution of Migraine and TTH. Life 2023, 13, 1902. https://doi.org/10.3390/life13091902
Genizi J, Shnaider M, Yaniv L, Kerem NC, Nathan K, Chistyakov I. Medication Overuse Headaches among Children—The Contribution of Migraine and TTH. Life. 2023; 13(9):1902. https://doi.org/10.3390/life13091902
Chicago/Turabian StyleGenizi, Jacob, Morya Shnaider, Liat Yaniv, Nogah C. Kerem, Keren Nathan, and Irina Chistyakov. 2023. "Medication Overuse Headaches among Children—The Contribution of Migraine and TTH" Life 13, no. 9: 1902. https://doi.org/10.3390/life13091902
APA StyleGenizi, J., Shnaider, M., Yaniv, L., Kerem, N. C., Nathan, K., & Chistyakov, I. (2023). Medication Overuse Headaches among Children—The Contribution of Migraine and TTH. Life, 13(9), 1902. https://doi.org/10.3390/life13091902