


Fresh Umbilical Cord Blood—A Source of Multipotent Stem Cells, Collection, Banking, Cryopreservation, and Ethical Concerns

 , ,
, ,
Abstract
1. Introduction
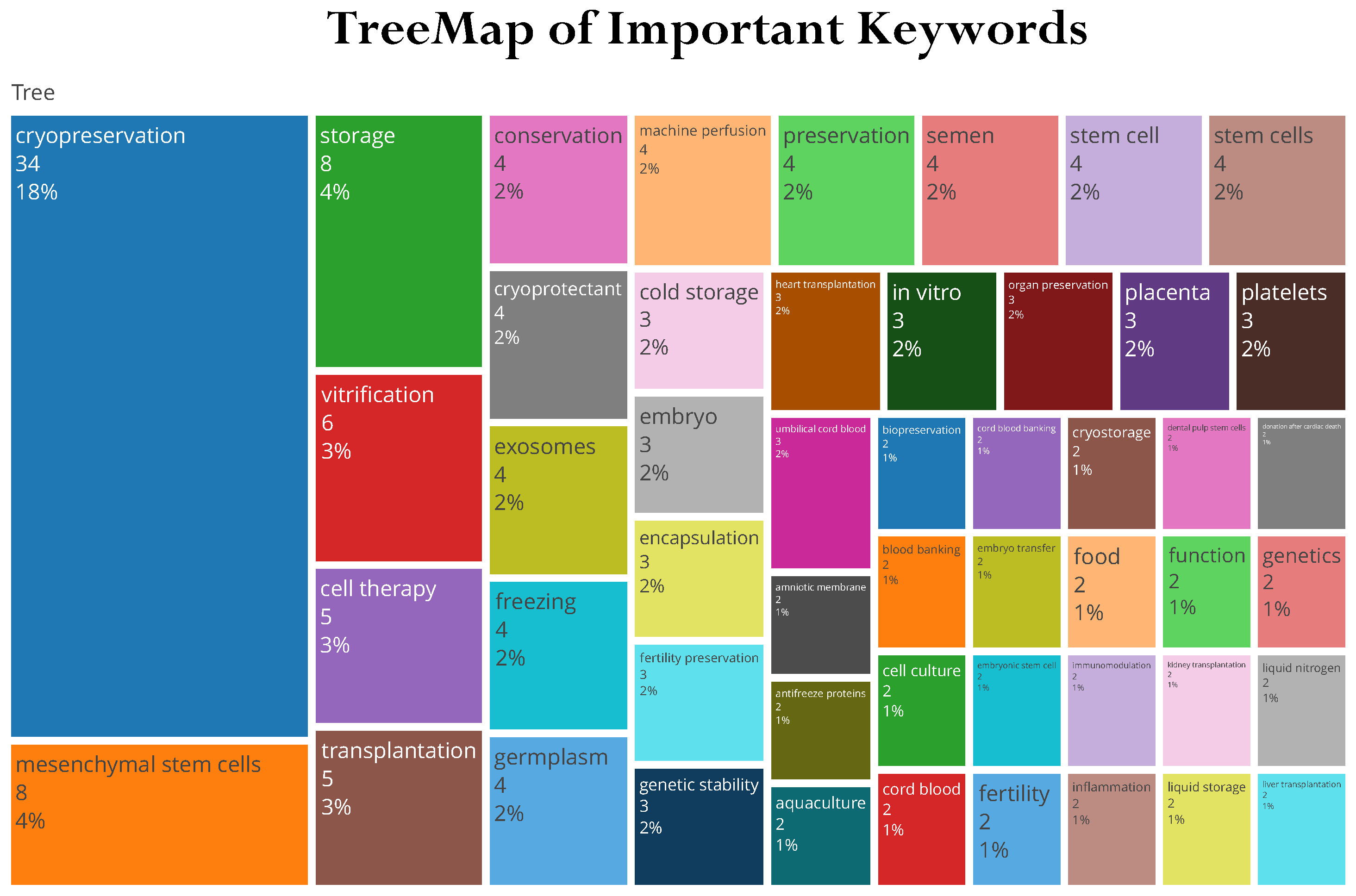
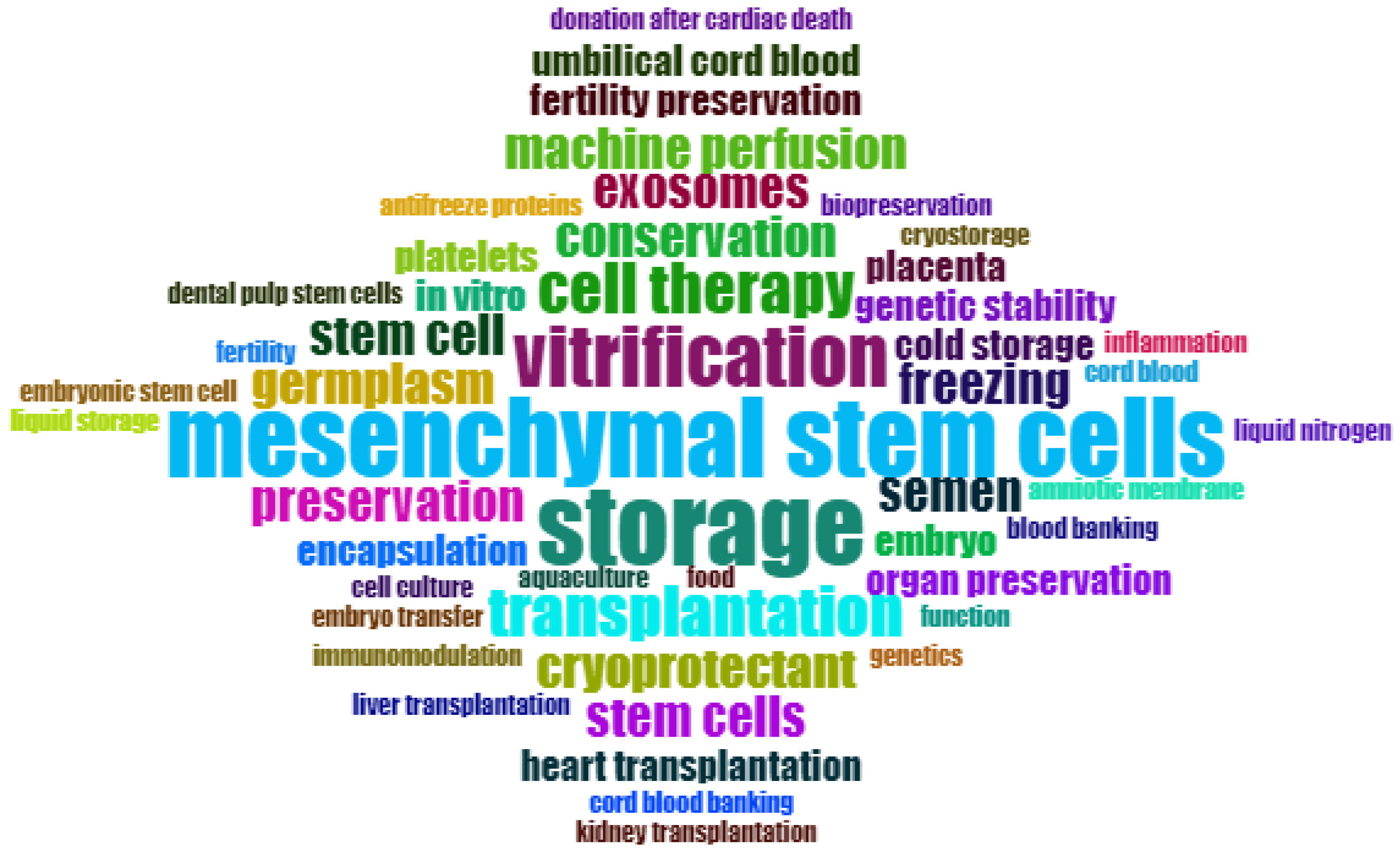
2. Brief Bibliometric Review
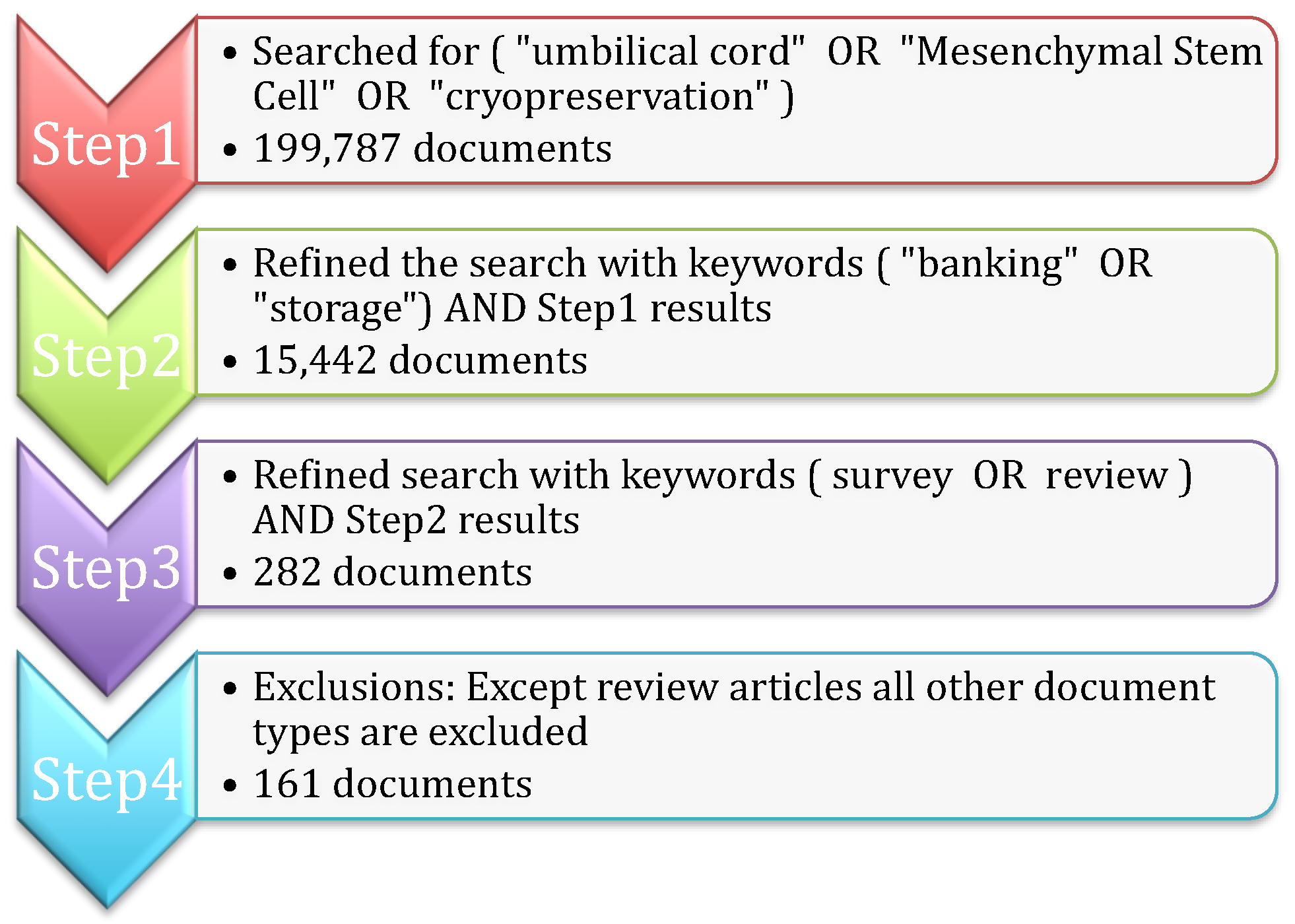
2.1. Data Collection
- Step 1: Initially, the search is carried out based on important keywords such as (“umbilical cord” OR “Mesenchymal Stem Cell” OR “cryopreservation”) in the title, abstract, and keywords of the Scopus repository. The search resulted in 199,787 research articles.
- Step 2: The search is further narrowed by considering additional keywords ( “banking” OR “storage”), along with the results of Step 1, 15,442 documents are obtained.
- Step 3: Since the study is focused only on survey articles, the search is further refined with the keywords ( survey OR review ) AND Step 2 results to obtain 282 articles.
- Step 4: All of the articles that belong to the research experiments, book chapters, and conference proceedings are excluded to obtain the final 161 review research articles.
2.2. Bibliometric Indictors
2.3. Salient Contribution of the Proposed Survey Article
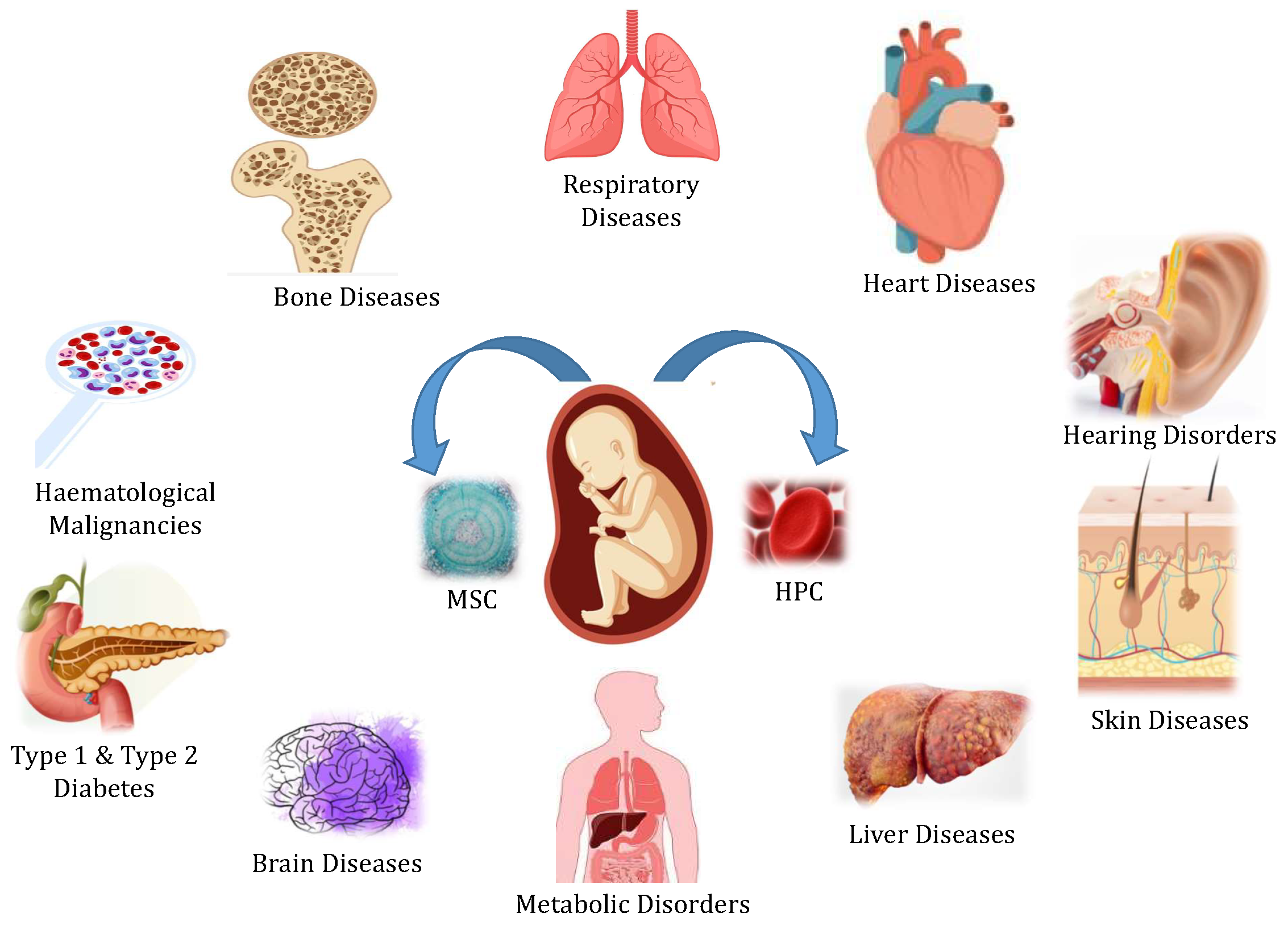
3. UCB as a Regenerative Medicine
3.1. Stem Cell Transplants
3.2. Ex Vivo Modulation Strategies to Enhance the Therapeutic Potential of UCB
3.3. Evolutions in the Use of Umbilical Cord Mesenchymal Stem Cells (MSCs)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Study Number | Condition | Sample Size | Notable Findings | Reference |
|---|---|---|---|---|
| 1. | Post-COVID-19 complications—pulmonary edema | 1 | UCB mesenchymal cells reduce inflammation, including cytokine storms in COVID-19 patients, as indicated by decreased IL-4, IL-6, and IL-10 levels. | [65] |
| 2. | COVID-19 with acute respiratory distress syndrome | 24 | Transfusing UCB stem cells safely increased patient survival to 91% (p = 0.015), and significantly improved recovery rates (0.03) by reducing cytokine storms. | [66] |
| 3. | Autism spectrum disorder (ASD) | 20 | Administering UCB mesenchymal stem cells was safe and effective in improving ASD. | [67] |
| 4. | Psoriasis | 7 | UCB MSC infusion had no side effects in 6 months of follow-up, increased Tregs and CD4+ memory T cells, and effectively treated 25% (2/8) and 66.7% (6/9) of male and female patients. | [68] |
| 5. | Neurological disorders | 100 | UCB MSC administration for neurological disorders was safe and effective, with minimal side effects noted in one-year patient follow-up. | [69] |
| 6. | Patients with muscular dystrophies | 22 | Two courses of 2–5 intravenous injections every two months significantly improved limb strength, stretching, bending, straightening, and gait (27.3%). | [70] |
| 7. | Rats with skin wounds | - | UCB-MSCs assist in regenerating skin appendages, nerves, and arteries, aiding wound closure and controlling collagen distribution. | [71] |
| 8. | Patients with alopecia lesions | 3 | No change was observed until day 53, and thereafter, minimal hair growth changes were detected in the first sample. The second patient showed significant hair growth on day 117 after transplantation By day 226, the third patient’s lesions had reduced, and they demonstrated remarkable hair growth. | [72] |
| 9. | Acute Myeloid Leukemia (AML) | 2963 | Allo-HCT from an unrelated donor produces superior results to cord blood transplantation. | [73] |
4. Collection and Cryopreservation of UCB
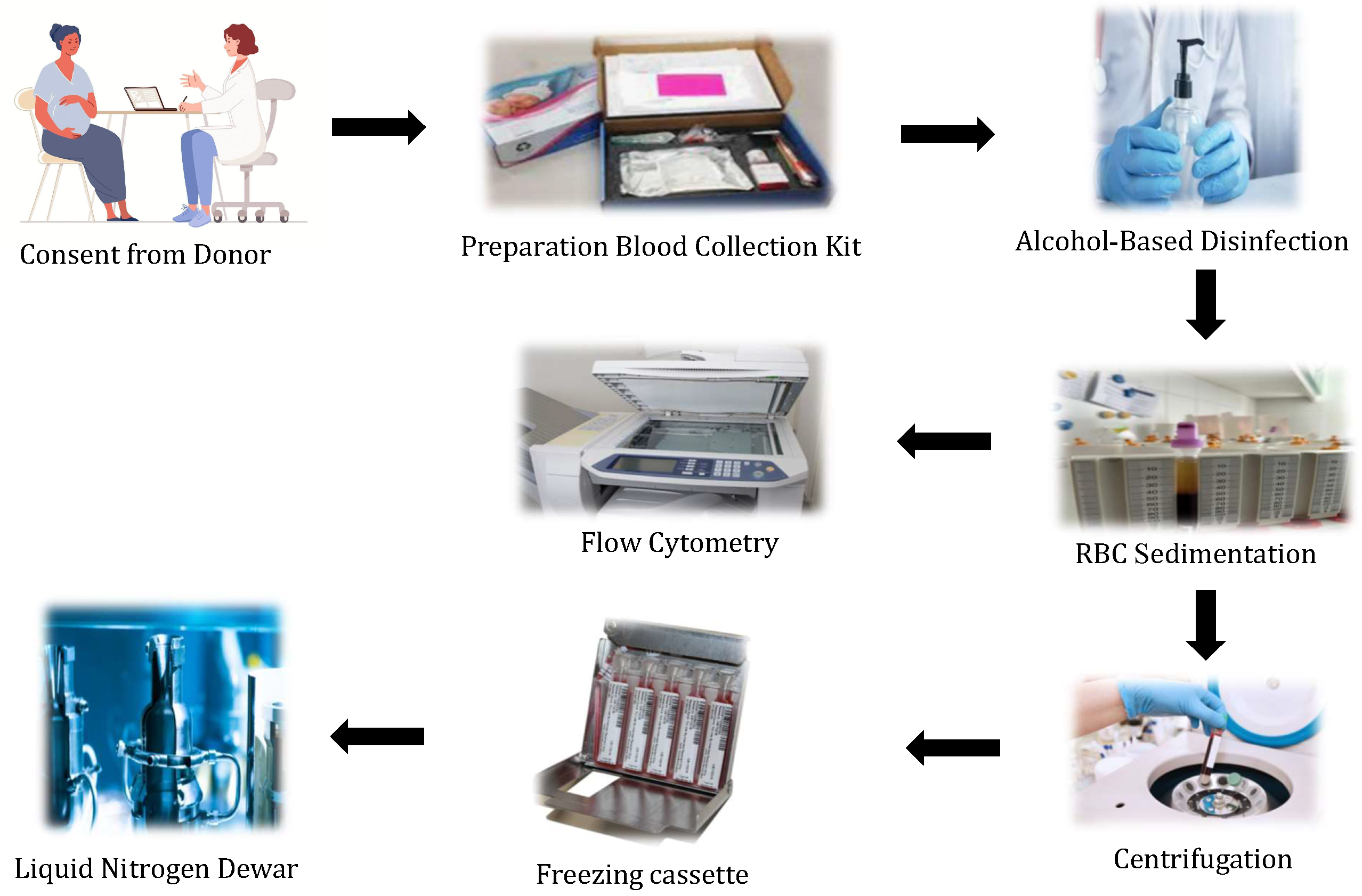
4.1. Umbilical Cord Blood Collection
4.2. Cryopreservation of Umbilical Cord Blood
5. Public and Private Umbilical Cord Blood Banking
- Jeevan Stem Cell Bank was founded in 1995 and is supported by the Tamil Nadu government. These banks primarily treat leukemia, thalassemia, and other hematological disorders.
- The Reliance Dhirubhai Ambani Life Sciences Center in Thane, Maharashtra, is supported by Reliance Life Sciences Pvt. Ltd. Free UCB; collection and storage services are provided.
- The School of Tropical Medicine (STM) established Kolkata’s first public cord blood bank.
- StemCyte Inc., Apollo Hospital Enterprises Ltd., and Cadila Pharmaceuticals Ltd. founded StemCyte India. The bank provides collection, processing, testing, and storage services for private and public umbilical cord blood units, and therapeutic applications.
- LifeCell was established in 2004 in technological collaboration with cryo-cell international. The primary goal of this bank was to assist patients in receiving lifesaving stem cell transplants to increase their chances of receiving the same stem cells.
6. Ethical Concerns in UCB Banking
Recommendations of Professional Organizations Regarding UCB
7. Discussion
7.1. UCB-Derived Mesenchymal Stem Cells: Benefits and Usage in Recent Research on Various Disease Conditions
7.2. Cryopreservation of UCB Cells: Understanding Their Biology and Functionality
7.3. Roles of Midwives and Obstetricians in UCB Collection
7.4. Hospital Protocols for the Safe and Efficient Collection of UCB
7.5. UCB Banks: Addressing Ethical Concerns in Establishment and Operation
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAP | American Academy of Pediatrics |
| ACOG | The American College of Obstetricians and Gynecologists |
| ASBMT | American Society of Bone Marrow Transplantation |
| ARDS | Acute respiratory distress syndrome |
| COPD | Chronic Obstructive Pulmonary Disease |
| CBUs | Cord Blood Units |
| CIBMTR | Center for International Blood and Bone Marrow Transplant Research |
| dmPGE2 | Dimethyl prostaglandin E2 |
| dUC | Differential Ultracentrifugation |
| DMSO | Dimethyl sulfoxide |
| ELISA | enzyme-linked immunosorbent assay |
| HCB | Human Cord Blood |
| HCT | Hematopoietic cell transplantation |
| HPCs | Hematopoietic progenitor cells |
| HLA | Human leukocyte antigen |
| HSCs | Hematopoietic stem cells |
| HIV | Human Immunodeficiency Virus |
| IDM | Infectious disease marker |
| MNC | Mononuclear cell |
| MSC | Mesenchymal stem cells |
| MDSs | Myelodysplastic Syndromes |
| nPES | Nanoplasmon-Enhanced Scattering |
| RBCs | Red blood cells |
| TNCs | Total Nucleated Cells |
| UCB | Umbilical Cord Blood |
References
- Zakrzewski, W.; Dobrzyński, M.; Szymonowicz, M.; Rybak, Z. Stem cells: Past, present, and future. Stem Cell Res. Ther. 2019, 10, 1–22. [Google Scholar]
- Burns, C.E.; Zon, L.I. Portrait of a stem cell. Dev. Cell 2002, 3, 612–613. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Preston, S.; Alison, M.; Forbes, S.; Direkze, N.; Poulsom, R.; Wright, N. The new stem cell biology: Something for everyone. Mol. Pathol. 2003, 56, 86. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Weiss, M.L.; Rao, M.S. In search of “stemness”. Exp. Hematol. 2004, 32, 585–598. [Google Scholar]
- McGuckin, C.P.; Forraz, N. Umbilical cord blood stem cells-an ethical source for regenerative medicine. Med. Law 2008, 27, 147. [Google Scholar]
- Vazin, T.; Freed, W.J. Human embryonic stem cells: Derivation, culture, and differentiation: A review. Restor. Neurol. Neurosci. 2010, 28, 589–603. [Google Scholar] [CrossRef]
- Meshorer, E. What are embryonic stem cells and how can they help us? Front. Young Minds 2020, 8, 32. [Google Scholar]
- Murata, M.; Kawabe, K.; Hatta, T.; Maeda, S.; Fujita, M. Current status of umbilical cord blood storage and provision to private biobanks by institutions handling childbirth in Japan. BMC Med. Ethics 2022, 23, 92. [Google Scholar]
- Gunning, J. Umbilical cord cell banking: An issue of self-interest versus altruism. Med. Law 2007, 26, 769. [Google Scholar]
- Gupta, A.O.; Wagner, J.E. Umbilical cord blood transplants: Current status and evolving therapies. Front. Pediatr. 2020, 8, 570282. [Google Scholar]
- Drew, D. Umbilical cord blood banking. Adv. Nurse Pract. 2005, 13 (Suppl. 2–6), quiz 7. [Google Scholar]
- Gluckman, E.; Broxmeyer, H.E.; Auerbach, A.D.; Friedman, H.S.; Douglas, G.W.; Devergie, A.; Esperou, H.; Thierry, D.; Socie, G.; Lehn, P.; et al. Hematopoietic reconstitution in a patient with Fanconi’s anemia by means of umbilical-cord blood from an HLA-identical sibling. N. Engl. J. Med. 1989, 321, 1174–1178. [Google Scholar] [PubMed]
- Ballen, K.; Verter, F.; Kurtzberg, J. Umbilical cord blood donation: Public or private? Bone Marrow Transplant. 2015, 50, 1271–1278. [Google Scholar] [PubMed]
- Dessels, C.; Alessandrini, M.; Pepper, M.S. Factors influencing the umbilical cord blood stem cell industry: An evolving treatment landscape. Stem Cells Transl. Med. 2018, 7, 643–650. [Google Scholar]
- de Latour, R.P.; Brunstein, C.G.; Porcher, R.; Chevallier, P.; Robin, M.; Warlick, E.; Xhaard, A.; Ustun, C.; Larghero, J.; Dhedin, N.; et al. Similar overall survival using sibling, unrelated donor, and cord blood grafts after reduced-intensity conditioning for older patients with acute myelogenous leukemia. Biol. Blood Marrow Transplant. 2013, 19, 1355–1360. [Google Scholar] [CrossRef]
- Tomblyn, M.B.; Arora, M.; Baker, K.S.; Blazar, B.R.; Brunstein, C.G.; Burns, L.J.; DeFor, T.E.; Dusenbery, K.E.; Kaufman, D.S.; Kersey, J.H.; et al. Myeloablative hematopoietic cell transplantation for acute lymphoblastic leukemia: Analysis of graft sources and long-term outcome. J. Clin. Oncol. 2009, 27, 3634. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; Finazzi, G.; Falanga, A. Myeloproliferative neoplasms and thrombosis. Blood J. Am. Soc. Hematol. 2013, 122, 2176–2184. [Google Scholar]
- Mallhi, K.K.; Smith, A.R.; DeFor, T.E.; Lund, T.C.; Orchard, P.J.; Miller, W.P. Allele-level HLA matching impacts key outcomes following umbilical cord blood transplantation for inherited metabolic disorders. Biol. Blood Marrow Transplant. 2017, 23, 119–125. [Google Scholar] [CrossRef]
- Smith, A.R.; Wagner, J.E. Alternative haematopoietic stem cell sources for transplantation: Place of umbilical cord blood. Br. J. Haematol. 2009, 147, 246–261. [Google Scholar] [CrossRef]
- Rink, B.; Miller, R.S.M. Umbilical cord blood banking. Comm. Opin. 2019, 771, 570282. [Google Scholar]
- Committee, A.L.T. Umbilical Cord Blood Collection Standard Operating Procedure. Available online: https://www.hanc.info/content/dam/hanc/documents/laboratory/actg-impaact-laboratory-manual/Umbilical-Cord-Blood-Collection.pdf (accessed on 19 December 2022).
- Broxmeyer, H.E.; Lee, M.R.; Hangoc, G.; Cooper, S.; Prasain, N.; Kim, Y.J.; Mallett, C.; Ye, Z.; Witting, S.; Cornetta, K.; et al. Hematopoietic stem/progenitor cells, generation of induced pluripotent stem cells, and isolation of endothelial progenitors from 21-to 23.5-year cryopreserved cord blood. Blood J. Am. Soc. Hematol. 2011, 117, 4773–4777. [Google Scholar]
- Navarrete, C.; Contreras, M. Cord blood banking: A historical perspective. Br. J. Haematol. 2009, 147, 236–245. [Google Scholar]
- Waller-Wise, R. Umbilical cord blood: Information for childbirth educators. J. Perinat. Educ. 2011, 20, 54–60. [Google Scholar]
- Webb, S. Banking on cord blood stem cells: New research will shed light on claims from commercial banks that cord blood–derived stem cells can be used in diseases beyond hematological disorders. Sarah Webb investigates. Nat. Biotechnol. 2013, 31, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Aria, M.; Cuccurullo, C. bibliometrix: An R-tool for comprehensive science mapping analysis. J. Inf. 2017, 11, 959–975. [Google Scholar]
- Alkindi, S.; Dennison, D. Umbilical cord blood banking and transplantation: A short review. Sultan Qaboos Univ. Med. J. 2011, 11, 455. [Google Scholar] [PubMed]
- Chakrabarty, P.; Rudra, S. Autologus or allogenic uses of umbilical cord blood whole or RBC transfusion-a review. Mymensingh Med. J. MMJ 2013, 22, 210–217. [Google Scholar]
- Allan, D.; Petraszko, T.; Elmoazzen, H.; Smith, S. A review of factors influencing the banking of collected umbilical cord blood units. Stem Cells Int. 2013, 2013, 463031. [Google Scholar] [CrossRef]
- Iafolla, M.A.; Tay, J.; Allan, D.S. Transplantation of umbilical cord blood–derived cells for novel indications in regenerative therapy or immune modulation: A scoping review of clinical studies. Biol. Blood Marrow Transplant. 2014, 20, 20–25. [Google Scholar]
- Nikougoftar, M. A review of procedures involved in human umbilical cord blood banking and transplantation. Iran. J. Blood Cancer (IJBC) 2014, 1, 37–42. [Google Scholar]
- Roura, S.; Pujal, J.M.; Gálvez-Montón, C.; Bayes-Genis, A. The role and potential of umbilical cord blood in an era of new therapies: A review. Stem Cell Res. Ther. 2015, 6, 123. [Google Scholar] [PubMed]
- Nitkin, C.R.; Bonfield, T.L. Concise review: Mesenchymal stem cell therapy for pediatric disease: Perspectives on success and potential improvements. Stem Cells Transl. Med. 2017, 6, 539–565. [Google Scholar]
- Nicodemou, A.; Danisovic, L. Mesenchymal stromal/stem cell separation methods: Concise review. Cell Tissue Bank. 2017, 18, 443–460. [Google Scholar] [PubMed]
- Tang, Y.; Zhou, Y.; Li, H.J. Advances in mesenchymal stem cell exosomes: A review. Stem Cell Res. Ther. 2021, 12, 71. [Google Scholar]
- Panda, B.; Sharma, Y.; Gupta, S.; Mohanty, S. Mesenchymal stem cell-derived exosomes as an emerging paradigm for regenerative therapy and nano-medicine: A comprehensive review. Life 2021, 11, 784. [Google Scholar] [PubMed]
- Gerdfaramarzi, M.S.; Bazmi, S.; Kiani, M.; Afshar, L.; Fadavi, M.; Enjoo, S.A. Ethical challenges of cord blood banks: A scoping review. J. Med. Life 2022, 15, 735. [Google Scholar] [CrossRef]
- Khaddour, K.; Hana, C.K.; Mewawalla, P. Hematopoietic stem cell transplantation. In StatPearls [Internet]; StatPearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]
- Pascutti, M.; Erkelens, M.; Nolte, M. Impact of viral infections on hematopoiesis: From beneficial to detrimental effects on bone marrow output. Front Immunol. 2016, 7, 364. [Google Scholar] [CrossRef]
- Theunissen, K.; Verfaillie, C.M. A multifactorial analysis of umbilical cord blood, adult bone marrow and mobilized peripheral blood progenitors using the improved ML-IC assay. Exp. Hematol. 2005, 33, 165–172. [Google Scholar] [CrossRef]
- Hildbrand, P.; Cirulli, V.; Prinsen, R.C.; Smith, K.A.; Torbett, B.E.; Salomon, D.R.; Crisa, L. The role of angiopoietins in the development of endothelial cells from cord blood CD34+ progenitors. Blood 2004, 104, 2010–2019. [Google Scholar] [CrossRef]
- Gluckman, E. Milestones in umbilical cord blood transplantation. Blood Rev. 2011, 25, 255–259. [Google Scholar]
- Liao, Y.; Geyer, M.B.; Yang, A.J.; Cairo, M.S. Cord blood transplantation and stem cell regenerative potential. Exp. Hematol. 2011, 39, 393–412. [Google Scholar] [CrossRef] [PubMed]
- Götherström, C.; Ringdén, O.; Tammik, C.; Zetterberg, E.; Westgren, M.; Le Blanc, K. Immunologic properties of human fetal mesenchymal stem cells. Am. J. Obstet. Gynecol. 2004, 190, 239–245. [Google Scholar] [CrossRef] [PubMed]
- North, T.E.; Goessling, W.; Walkley, C.R.; Lengerke, C.; Kopani, K.R.; Lord, A.M.; Weber, G.J.; Bowman, T.V.; Jang, I.H.; Grosser, T.; et al. Prostaglandin E2 regulates vertebrate haematopoietic stem cell homeostasis. Nature 2007, 447, 1007–1011. [Google Scholar] [CrossRef]
- Flynn, P.; Yingling, J.; Shoemaker, D. Converging technologies to enable induced pluripotent stem cells in drug discovery. Regen. Med. 2010, 5, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Malgieri, A.; Kantzari, E.; Patrizi, M.P.; Gambardella, S. Bone marrow and umbilical cord blood human mesenchymal stem cells: State of the art. Int. J. Clin. Exp. Med. 2010, 3, 248. [Google Scholar]
- Garbuzova-Davis, S.; Rodrigues, M.C.; Mirtyl, S.; Turner, S.; Mitha, S.; Sodhi, J.; Suthakaran, S.; Eve, D.J.; Sanberg, C.D.; Kuzmin-Nichols, N.; et al. Multiple intravenous administrations of human umbilical cord blood cells benefit in a mouse model of ALS. PLoS ONE 2012, 7, e31254. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Williams, K.J.; Picou, A.A.; Kish, S.L.; Giraldo, A.M.; Godke, R.A.; Bondioli, K.R. Isolation and characterization of porcine adipose tissue-derived adult stem cells. Cells Tissues Organs 2008, 188, 251–258. [Google Scholar] [CrossRef]
- Liao, H.T.; Chen, C.T. Osteogenic potential: Comparison between bone marrow and adipose-derived mesenchymal stem cells. World J. Stem Cells 2014, 6, 288. [Google Scholar] [CrossRef]
- Wang, J.; Cai, X.; Wang, Z.; Xu, Q.; Li, K.; Hua, C. Isolation and identification of exosomes from human adipose-derived mesenchymal stem cells. Chin. J. Tissue Eng. Res. 2019, 23, 2651. [Google Scholar]
- Cotten, C.M.; Murtha, A.P.; Goldberg, R.N.; Grotegut, C.A.; Smith, P.B.; Goldstein, R.F.; Fisher, K.A.; Gustafson, K.E.; Waters-Pick, B.; Swamy, G.K.; et al. Feasibility of autologous cord blood cells for infants with hypoxic-ischemic encephalopathy. J. Pediatr. 2014, 164, 973–979. [Google Scholar] [CrossRef]
- Vendrame, M.; Gemma, C.; Mesquita, D.D.; Collier, L.; Bickford, P.C.; Sanberg, C.D.; Sanberg, P.R.; Pennypacker, K.R.; Willing, A.E. Anti-inflammatory effects of human cord blood cells in a rat model of stroke. Stem Cells Dev. 2005, 14, 595–604. [Google Scholar] [CrossRef]
- Harris, D.T.; Badowski, M.; Ahmad, N.; Gaballa, M.A. The potential of cord blood stem cells for use in regenerative medicine. Expert Opin. Biol. Ther. 2007, 7, 1311–1322. [Google Scholar] [CrossRef]
- Taguchi, A.; Soma, T.; Tanaka, H.; Kanda, T.; Nishimura, H.; Yoshikawa, H.; Tsukamoto, Y.; Iso, H.; Fujimori, Y.; Stern, D.M.; et al. Administration of CD34+ cells after stroke enhances neurogenesis via angiogenesisin a mouse model. J. Clin. Investig. 2004, 114, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Nikfarjam, S.; Rezaie, J.; Zolbanin, N.M.; Jafari, R. Mesenchymal stem cell derived-exosomes: A modern approach in translational medicine. J. Transl. Med. 2020, 18, 449. [Google Scholar] [CrossRef]
- Kim, Y.J.; mi Yoo, S.; Park, H.H.; Lim, H.J.; Kim, Y.L.; Lee, S.; Seo, K.W.; Kang, K.S. Exosomes derived from human umbilical cord blood mesenchymal stem cells stimulates rejuvenation of human skin. Biochem. Biophys. Res. Commun. 2017, 493, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.; He, X.; Badowski, M.; Nicols, J. Regenerative medicine of the eye: A short review. In Stem Cell Repair and Regeneration; Imperial College Press: London, UK, 2008; Volume 3, pp. 211–225. [Google Scholar] [CrossRef]
- Laughlin, M.J.; Barker, J.; Bambach, B.; Koc, O.N.; Rizzieri, D.A.; Wagner, J.E.; Gerson, S.L.; Lazarus, H.M.; Cairo, M.; Stevens, C.E.; et al. Hematopoietic engraftment and survival in adult recipients of umbilical-cord blood from unrelated donors. N. Engl. J. Med. 2001, 344, 1815–1822. [Google Scholar] [CrossRef] [PubMed]
- Moodley, Y.; Atienza, D.; Manuelpillai, U.; Samuel, C.S.; Tchongue, J.; Ilancheran, S.; Boyd, R.; Trounson, A. Human umbilical cord mesenchymal stem cells reduce fibrosis of bleomycin-induced lung injury. Am. J. Pathol. 2009, 175, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Undale, A.H.; Westendorf, J.J.; Yaszemski, M.J.; Khosla, S. Mesenchymal stem cells for bone repair and metabolic bone diseases. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2009; Volume 84, pp. 893–902. [Google Scholar]
- Chorath, K.; Willis, M.; Morton-Gonzaba, N.; Moreira, A. Mesenchymal stem cells for sensorineural hearing loss: A systematic review of preclinical studies. Mol. Biol. Rep. 2020, 47, 4723–4736. [Google Scholar] [CrossRef]
- Sierra-Sánchez, Á.; Montero-Vilchez, T.; Quiñones-Vico, M.I.; Sanchez-Diaz, M.; Arias-Santiago, S. Current advanced therapies based on human mesenchymal stem cells for skin diseases. Front. Cell Dev. Biol. 2021, 9, 643125. [Google Scholar] [CrossRef]
- Zhang, Q.; Huang, K.; Lv, J.; Fang, X.; He, J.; Lv, A.; Sun, X.; Cheng, L.; Zhong, Y.; Wu, S.; et al. Case report: Human umbilical cord mesenchymal stem cells as a therapeutic intervention for a critically Ill Covid-19 patient. Front. Med. 2021, 8, 691329. [Google Scholar] [CrossRef] [PubMed]
- Lanzoni, G.; Linetsky, E.; Correa, D.; Messinger Cayetano, S.; Alvarez, R.A.; Kouroupis, D.; Alvarez Gil, A.; Poggioli, R.; Ruiz, P.; Marttos, A.C.; et al. Umbilical cord mesenchymal stem cells for COVID-19 acute respiratory distress syndrome: A double-blind, phase 1/2a, randomized controlled trial. Stem Cells Transl. Med. 2021, 10, 660–673. [Google Scholar] [CrossRef] [PubMed]
- Riordan, N.H.; Hincapié, M.L.; Morales, I.; Fernández, G.; Allen, N.; Leu, C.; Madrigal, M.; Paz Rodríguez, J.; Novarro, N. Allogeneic human umbilical cord mesenchymal stem cells for the treatment of autism spectrum disorder in children: Safety profile and effect on cytokine levels. Stem Cells Transl. Med. 2019, 8, 1008–1016. [Google Scholar] [CrossRef]
- Cheng, L.; Wang, S.; Peng, C.; Zou, X.; Yang, C.; Mei, H.; Li, C.; Su, X.; Xiao, N.; Ouyang, Q.; et al. Human umbilical cord mesenchymal stem cells for psoriasis: A phase 1/2a, single-arm study. Signal Transduct. Target. Ther. 2022, 7, 263. [Google Scholar] [CrossRef] [PubMed]
- Miao, X.; Wu, X.; Shi, W. Umbilical cord mesenchymal stem cells in neurological disorders: A clinical study. Indian J. Biochem. Biophys. 2015, 52, 140–146. [Google Scholar]
- Świątkowska-Flis, B.; Zdolińska-Malinowska, I.; Sługocka, D.; Boruczkowski, D. The use of umbilical cord-derived mesenchymal stem cells in patients with muscular dystrophies: Results from compassionate use in real-life settings. Stem Cells Transl. Med. 2021, 10, 1372–1383. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Pan, Y.; Liu, Y.; Li, X.; Tang, L.; Duan, M.; Li, J.; Zhang, G. Exosomes derived from human umbilical cord blood mesenchymal stem cells stimulate regenerative wound healing via transforming growth factor-β receptor inhibition. Stem Cell Res. Ther. 2021, 12, 434. [Google Scholar] [CrossRef]
- Ahn, H.; Lee, S.Y.; Jung, W.J.; Lee, K.H. Alopecia treatment using minimally manipulated human umbilical cord-derived mesenchymal stem cells: Three case reports and review of literature. World J. Clin. Cases 2021, 9, 3741. [Google Scholar] [CrossRef]
- Baron, F.; Labopin, M.; Ruggeri, A.; Ehninger, G.; Bonifazi, F.; Stelljes, M.; Sanz, J.; Stuhler, G.; Bosi, A.; Kröger, N.; et al. Umbilical cord blood versus unrelated donor transplantation in adults with primary refractory or relapsed acute myeloid leukemia: A report from Eurocord, the Acute Leukemia Working Party and the Cord Blood Committee of the Cellular Therapy and Immunobiology Working Party of the EBMT. Blood Cancer J. 2019, 9, 46. [Google Scholar]
- Broxmeyer, H.E.; Douglas, G.W.; Hangoc, G.; Cooper, S.; Bard, J.; English, D.; Arny, M.; Thomas, L.; Boyse, E.A. Human umbilical cord blood as a potential source of transplantable hematopoietic stem/progenitor cells. Proc. Natl. Acad. Sci. USA 1989, 86, 3828–3832. [Google Scholar] [CrossRef]
- Kielpinski, G.; Prinzi, S.; Duguid, J.; Du Moulin, G. Roadmap to approval: Use of an automated sterility test method as a lot release test for Carticel®, autologous cultured chondrocytes. Cytotherapy 2005, 7, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.; Schumacher, M.; Rychlik, S.; Booth, A.; Acevedo, A.; Rubinstein, P.; Bard, J.; Boyse, E. Collection, separation and cryopreservation of umbilical cord blood for use in transplantation. Bone Marrow Transplant. 1994, 13, 135–143. [Google Scholar] [PubMed]
- M-Reboredo, N.; Díaz, A.; Castro, A.; Villaescusa, R. Collection, processing and cryopreservation of umbilical cord blood for unrelated transplantation. Bone Marrow Transplant. 2000, 26, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.H.; Zarrabi, M.; Abroun, S.; Ahmadipanah, M.; Abbaspanah, B. Umbilical cord blood quality and quantity: Collection up to transplantation. Asian J. Transfus. Sci. 2019, 13, 79. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.K.; Eder, A.; Spitalnik, S.L.; Westhoff, C.M. Technical Manual; AABB: Bethesda, MD, USA, 2017. [Google Scholar]
- Solves, P.; Moraga, R.; Saucedo, E.; Perales, A.; Soler, M.; Larrea, L.; Mirabet, V.; Planelles, D.; Carbonell-Uberos, F.; Monleon, J.; et al. Comparison between two strategies for umbilical cord blood collection. Bone Marrow Transplant. 2003, 31, 269–273. [Google Scholar] [CrossRef]
- Tamburini, A.; Malerba, C.; Picardi, A.; Amadori, S.; Calugi, A. Placental/umbilical cord blood: Experience of St. Eugenio Hospital collection center. Transplant. Proc. 2005, 37, 2670–2672. [Google Scholar] [CrossRef]
- Nakagawa, R.; Watanabe, T.; Kawano, Y.; Kanai, S.; Suzuya, H.; Kaneko, M.; Watanabe, H.; Okamoto, Y.; Kuroda, Y.; Nakayama, T.; et al. Analysis of maternal and neonatal factors that influence the nucleated and CD34+ cell yield for cord blood banking. Transfusion 2004, 44, 262–267. [Google Scholar] [CrossRef]
- Jan, R.H.; Wen, S.H.; Shyr, M.H.; Chiang, B.L. Impact of maternal and neonatal factors on CD34+ cell count, total nucleated cells, and volume of cord blood. Pediatr. Transplant. 2008, 12, 868–873. [Google Scholar] [CrossRef]
- Bassiouny, M.; El-Chennawi, F.; Mansour, A.; Yahia, S.; Darwish, A. Optimal method for collection of umbilical cord blood: An E gyptian trial for a public cord blood bank. Transfusion 2015, 55, 1263–1268. [Google Scholar] [CrossRef]
- Harris, D.T. Cord blood banking for transplantation. Can. J. Clin. Med. 1997, 4, 4–12. [Google Scholar]
- Solves, P.; Mirabet, V.; Blanquer, A.; Delgado-Rosas, F.; Planelles, D.; Andrade, M.; Carbonell-Uberos, F.; Soler, M.A.; Roig, R. A new automatic device for routine cord blood banking: Critical analysis of different volume reduction methodologies. Cytotherapy 2009, 11, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Solves, P.; Mirabet, V.; Roig, R. Volume reduction in routine cord blood banking. Curr. Stem Cell Res. Ther. 2010, 5, 362–366. [Google Scholar] [CrossRef]
- Akel, S.; Regan, D.; Wall, D.; Petz, L.; McCullough, J. Current thawing and infusion practice of cryopreserved cord blood: The impact on graft quality, recipient safety, and transplantation outcomes. Transfusion 2014, 54, 2997–3009. [Google Scholar] [CrossRef]
- Hunt, C.J. Cryopreservation: Vitrification and controlled rate cooling. Stem Cell Bank. 2017, 1590, 41–77. [Google Scholar]
- Lane, T.; Plunkett, M.; Buenviaje, J.; Law, P.; Wu, L.; Patterson, H. Recovery of leukocytes in cord blood units after cryopreservation by controlled rate freeze in DMSO and storage in vapor phase liquid nitrogen. In Proceedings of the Blood; The American Society of Hematology: Washington, DC, USA, 2001; Volume 98, p. 180A. [Google Scholar]
- Lysak, D.; Brychtová, M.; Leba, M.; Čedíková, M.; Georgiev, D.; Jindra, P.; Vlas, T.; Holubova, M. Long-Term Cryopreservation Does Not Affect Quality of Peripheral Blood Stem Cell Grafts: A Comparative Study of Native, Short-Term and Long-Term Cryopreserved Haematopoietic Stem Cells. Cell Transplant. 2021, 30, 09636897211036004. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, P.; Dobrila, L.; Rosenfield, R.E.; Adamson, J.W.; Migliaccio, G.; Migliaccio, A.R.; Taylor, P.E.; Stevens, C.E. Processing and cryopreservation of placental/umbilical cord blood for unrelated bone marrow reconstitution. Proc. Natl. Acad. Sci. USA 1995, 92, 10119–10122. [Google Scholar] [CrossRef] [PubMed]
- Miura, J.; Minegishi, M.; Itoh, T.; Kitaura, T.; Fukawa, N.; Takahashi, H.; Suzuki, A.; Kudo, Y.; Narita, A.; Sato, Y.; et al. Quality evaluation of umbilical cord blood progenitor cells cryopreserved with a small-scale automated liquid nitrogen system. Cryobiology 2008, 57, 178–181. [Google Scholar] [CrossRef]
- Young, W. Plasma-depleted versus red cell-reduced umbilical cord blood. Cell Transplant. 2014, 23, 407–415. [Google Scholar] [CrossRef]
- Chow, R.; Lin, A.; Tonai, R.; Bolanos, R.; Connor, C.; Mendoza, A.; Heminger, R.; Chow, M.; Ho, E.; Kang, J.; et al. Cell recovery comparison between plasma depletion/reduction-and red cell reduction-processing of umbilical cord blood. Cytotherapy 2011, 13, 1105–1119. [Google Scholar] [CrossRef]
- Barker, J.N.; Weisdorf, D.J.; DeFor, T.E.; Blazar, B.R.; McGlave, P.B.; Miller, J.S.; Verfaillie, C.M.; Wagner, J.E. Transplantation of 2 partially HLA-matched umbilical cord blood units to enhance engraftment in adults with hematologic malignancy. Blood 2005, 105, 1343–1347. [Google Scholar] [CrossRef]
- Scaradavou, A.; Brunstein, C.G.; Eapen, M.; Le-Rademacher, J.; Barker, J.N.; Chao, N.; Cutler, C.; Delaney, C.; Kan, F.; Isola, L.; et al. Double unit grafts successfully extend the application of umbilical cord blood transplantation in adults with acute leukemia. Blood J. Am. Soc. Hematol. 2013, 121, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, B.; Marcon, A.R.; Caulfield, T. The law and problematic marketing by private umbilical cord blood banks. BMC Med. Ethics 2020, 21, 52. [Google Scholar] [CrossRef] [PubMed]
- Shearer, W.T.; Lubin, B.H.; Cairo, M.S.; Notarangelo, L.D.; Hord, J.; Crouch, G.; Hale, G.; Harper, J.; Lipton, J.; Rogers, Z.; et al. Cord blood banking for potential future transplantation. Pediatrics 2017, 140, e20172695. [Google Scholar] [CrossRef]
- Petrini, C. Umbilical cord blood collection, storage and use: Ethical issues. Blood Transfus. 2010, 8, 139. [Google Scholar]
- Viswanathan, C.; Kabra, P.; Nazareth, V.; Kulkarni, M.; Roy, A. India’s first public cord blood repository—Looking back and moving forward. Indian J. Hematol. Blood Transfus. 2009, 25, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Lin, S.J.; Cheng, P.J.; Kuo, M.L. The regulatory function of umbilical cord blood CD4+ CD25+ T cells stimulated with anti-CD3/anti-CD28 and exogenous interleukin (IL)-2 or IL-15. Pediatr. Allergy Immunol. 2009, 20, 624–632. [Google Scholar] [CrossRef]
- Mayani, H. Umbilical cord blood: Lessons learned and lingering challenges after more than 20 years of basic and clinical research. Arch. Med. Res. 2011, 42, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.A.; Boussiotis, V.A. Umbilical cord blood transplantation: Basic biology and clinical challenges to immune reconstitution. Clin. Immunol. 2008, 127, 286–297. [Google Scholar] [CrossRef]
- Da Silva, C.L.; Gonçalves, R.; Porada, C.D.; Ascensão, J.L.; Zanjani, E.D.; Cabral, J.M.; Almeida-Porada, G. Differences amid bone marrow and cord blood hematopoietic stem/progenitor cell division kinetics. J. Cell. Physiol. 2009, 220, 102–111. [Google Scholar] [CrossRef]
- Mayani, H.; Lansdorp, P.M. Biology of human umbilical cord blood-derived hematopoietic stem/progenitor cells. Stem Cells 1998, 16, 153–165. [Google Scholar] [CrossRef]
- Ballen, K.K.; Barker, J.N.; Stewart, S.K.; Greene, M.F.; Lane, T.A. Collection and preservation of cord blood for personal use. Biol. Blood Marrow Transplant. 2008, 14, 356–363. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Herlihy, M.M.; Delpapa, E.H. Obstetricians and their role in cord blood banking: Promoting a public model. Obstet. Gynecol. 2013, 121, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Committee on Obstetric Practice; Committee on Genetics. ACOG committee opinion number 399, February 2008: Umbilical cord blood banking. Obstet. Gynecol. 2008, 111, 475–477. [Google Scholar]
- Lubin, B.H.; Shearer, W.T. Cord blood banking for potential future transplantation. Pediatrics 2007, 119, 165–170. [Google Scholar]
- Walker, T.; Steckler, D.; Spellman, S.; Haven, D.; Welte, K.; Boo, M. Awareness and acceptance of public cord blood banking among practicing obstetricians in the United States. Transfusion 2012, 52, 787–793. [Google Scholar] [CrossRef]
- Wang, S.Y.; Hsu, M.L.; Huang, M.Z.; Hsu, H.C.; Tzeng, C.H.; Hung, J.H.; Ho, C.K. The activity in ex vivo expansion of cord blood myeloid progenitor cells before and after cryopreservation. Acta Haematol. 2001, 105, 38–44. [Google Scholar] [CrossRef]
- Katz, G.; Mills, A. Cord blood banking in France: Reorganising the national network. Transfus. Apher. Sci. 2010, 42, 307–316. [Google Scholar] [CrossRef]
- Frändberg, S.; Waldner, B.; Konar, J.; Rydberg, L.; Fasth, A.; Holgersson, J. High quality cord blood banking is feasible with delayed clamping practices. The eight-year experience and current status of the national Swedish Cord Blood Bank. Cell Tissue Bank. 2016, 17, 439–448. [Google Scholar] [CrossRef]
- Warwick, R.; Fehily, D. Ethics of cord blood banking. Curr. Obstet. Gynaecol. 2002, 12, 175–177. [Google Scholar] [CrossRef]
- Childress, J.F. Sources of stem cells: Ethical controversies and policy developments in the United States. Fetal Diagn. Ther. 2004, 19, 119–123. [Google Scholar] [CrossRef]
- Salvaterra, E.; Lecchi, L.; Gobbi, S.; Rebulla, P. The ethics of cord blood banking in light of ownership, informed consent, and solidarity. Cell Preserv. Technol. 2006, 4, 91–96. [Google Scholar] [CrossRef]
- Roqué, M.V.; Segarra, I.; Macpherson, I. Ethical Challenges of Germline Genetic Enhancement. Front. Genet. 2019, 10, 767. [Google Scholar]
- Ballen, K. Challenges in umbilical cord blood stem cell banking for stem cell reviews and reports. Stem Cell Rev. Rep. 2010, 6, 8–14. [Google Scholar] [CrossRef] [PubMed]








| Significant Contribution | Number of Papers Surveyed | Specific Study Topic | Short Falls | Ref. | Year |
|---|---|---|---|---|---|
| UBT use in Oman, and its benefits and drawbacks | 29 | UCB Stem Cell Transfer in Oman: Banking and Transplantation | Umbilical Cord Blood Banking and Stem Cell Transplantation | [27] | 2011 |
| Preservation of Cord Blood for autogenic/allogenic therapy | 54 | Adverse Effects of Transfusing Placental Red Blood Cells (RBCs) and Umbilical Cord Blood (UCB) | Clinical trial results and reviews must be accurately specified | [28] | 2013 |
| This study aids the clinician in deciding whether to bank the UCB | 31 | Current guidelines for cord blood unit selection have implications for transplantation and banking decisions, as reflected in graft adequacy measures | The source of stem cells, such as UCB, bone marrow, and placental products, can influence stem cell banking | [29] | 2013 |
| The future of UCB-derived cellular therapy | 39 | Clinical studies on umbilical cord blood-derived cell transplantation for regenerative therapy are the main focus | Advising on Changes in Banking Procedures for Umbilical Cord Blood (UCB) Stem Cells in Response to Emerging Cell Therapy Trends | [30] | 2013 |
| An overview of the procedures for banking cord blood | 52 | Transplanting multiple units or ex vivo transplantation can overcome the UCB transplant’s cell dose limitations | The abstract does not explain the accreditation guidelines for UCB banking quality | [31] | 2014 |
| This study thoroughly explains the current and potential clinical applications of UCB | 94 | Problems associated with UCB cryopreservation and processing | Umbilical cord MSCs in regenerative therapies | [32] | 2015 |
| Clinical trials in children using MSCs from various sources to treat diseases | 158 | MSC sources, therapies in clinical trials, route, dose, and timings | UCB MSC sources unclear, placental derivatives and amniotic fluid only treat 5 diseases | [33] | 2016 |
| This article guides clinicians on how to distinguish the MSCs from the UCB. | 60 | Current MSC separation techniques, their values, benefits, and constraints | ---- | [34] | 2017 |
| Improvements in mesenchymal stem cell (MSC) exosomes | 95 | Exosome characteristics and biological functions in clinical practice | Information about how to obtain MSC exosomes is insufficient | [35] | 2021 |
| Nanomedicine vesicles are utilized in both nanotherapeutics and as drug delivery systems | 161 | The use of nanomedicine vesicles in translational research—exosomes—to overcome limitations in cell-based therapies | Comprehensive comprehension of exosomes’ composition and mechanism are crucial for their proper clinical application, given the risk of off-target activity | [36] | 2021 |
| There is a call for policymakers and medical professionals to create clear ethical standards for UCB banks. | 52 | UCB banks’ ethical issues in collecting and preserving blood | Private and public banks need individual comparisons due to their unique challenges | [37] | 2022 |
| Donor Type | Cell Source | 2016, No. | 2016, Col % | 2017, No. | 2017, Col % | 2018, No. | 2018, Col % | 2019, No. | 2019, Col % | 2020, No. | 2020, Col % |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Allogenic | Bone Marrow | 2011 | 23 | 2071 | 23 | 2179 | 23 | 2014 | 21 | 1507 | 17 |
| Allogenic | Cord Blood | 682 | 8 | 621 | 7 | 557 | 6 | 512 | 5 | 422 | 5 |
| Allogenic | Peripheral Blood | 6065 | 69 | 6343 | 70 | 6580 | 71 | 6865 | 73 | 7097 | 79 |
| Autologous | Bone Marrow | 22 | <1 | 35 | <1 | 27 | <1 | 23 | <1 | 22 | <1 |
| Autologous | Cord Blood | 0 | 0 | 0 | 0 | 4 | <1 | 2 | <1 | 1 | <1 |
| Autologous | Peripheral Blood | 12,847 | 100 | 13,337 | 100 | 13,477 | 100 | 13,710 | 100 | 12,951 | 100 |
| Status | Category | Disease Conditions | Transplantation Type | Identifier | Participants | Phase |
|---|---|---|---|---|---|---|
| Completed | Metabolic disorders | Type 1 Diabetes | Autogenic | NCT00873925 | 23 children | 1 |
| Unknown | Type 1 Diabetes | Autogenic | NCT00989547 | 18 | 1 | |
| Recruiting | Type 2 Diabetes | Allogenic | NCT03835312 | 50 | NA | |
| Recruiting | Type 2 Diabetes | Allogenic | NCT04441658 | 30 | 1, 2 | |
| Recruiting | Type 2 Diabetes | Allogenic | NCT04501341 | 15 | 1, 2 | |
| Completed | Hematological Disorders | Sickle Cell Disease Transfusion Dependent Alpha- or Beta-Thalassemia | Allogenic | NCT02179359 | 25 | NA |
| Recruiting | Hematological Malignancies | Acute Erythroid and Lymphoblastic Leukemia | Autologous or allogenic | NCT04083170 | 10 | 2 |
| Recruiting | Leukemia, Myelomonocytic, Acute | Allogenic | NCT04687657 | 20 | 1 | |
| Recruiting | Severe Aplastic Anemia and Hypoplastic MDS | Allogenic | NCT03173937 | 37 | 1, 2 | |
| Recruiting | COVID-19 diseases | COVID-19 Infection | Allogenic | NCT04565665 | 70 participants | 1, 2 |
| Not yet recruiting | COVID-19-Associated ARDS | Allogenic | NCT05092724 | 20 | NA | |
| Recruiting | COVID, Pulmonary Infection, Sars-CoV2 | Allogenic | NCT04457609 | 40 | 1 | |
| Suspended | Ear Disorders | Hearing Loss | Autologous | NCT01343394 | 10 | 1 |
| Completed | Sensorineural Hearing Loss | Autologous | NCT02038972 | 11 | 1, 2 | |
| Recruiting | Heart Diseases | Congenital Heart Disease, SRV Dependent | Autologous | NCT04907526 | 30 | 1 |
| Active, not recruiting | Congenital Heart Disease, SRV Dependent | Autologous | NCT03431480 | 1 | 1 | |
| Completed | Hypoplastic Left Heart Syndrome | Autologous | NCT01883076 | 30 | 1 | |
| Completed | Autism | Autism | Autologous | NCT01638819 | 30 | 2 |
| Completed | Autism Spectrum Disorder | Allogenic | NCT04710810 | 30 | 1 | |
| Completed | Neurological disorders | Cerebral Palsy | Allogenic | NCT03826498 | 40 | 2 |
| Completed | Dementia of the Alzheimer’s Type | Autogenic | NCT01696591 | 9 | 1 | |
| Completed | Stroke | Autogenic | NCT03004976 | 83 | 2 | |
| Recruiting | Spinal Cord Injuries | Autogenic | NCT03979742 | 18 | 2 | |
| Unknown | Ischemic Stroke and Cerebral Infarction | Autogenic | NCT01438593 | 6 | 1 | |
| Withdrawn | Arterial Ischemic Stroke (AIS) in Children | Autogenic | NCT01700166 | 0 | 1 | |
| Unknown | Neonatal Hypoxic- ischaemic Encephalopathy | Autogenic | NCT02881970 | 20 | 1, 2 | |
| Completed | Skin Diseases | Androgenic Alopecia | Allogenic | NCT03676400 | 84 | NA |
| Unknown | Diabetic Foot and Critical Limb Ischemia | Allogenic | NCT01216865 | 50 | 1, 2 | |
| Terminated | Epidermolysis Bullosa | Autogenic | NCT00881556 | 3 | Early Phase 1 | |
| Recruiting | Liver and GI Diseases | Primary Biliary Cirrhosis | Allogenic | NCT04522869 | 34 | 1, 2 |
| Recruiting | Hepatitis B | Allogenic | NCT03826433 | 20 | 1 | |
| Recruiting | Liver Cirrhosis | Allogenic | NCT05331872 | 20 | 1 | |
| Recruiting | Neonatal Necrotizing Enterocolitis | Autogenic | NCT05138276 | 60 | Early Phase 1 | |
| Recruiting | Growth and Development | Autogenic | NCT05138276 | 60 | Early Phase 1 | |
| Recruiting | Preterm Infants | Autogenic | NCT05138276 | 60 | Early Phase 1 | |
| Recruiting | Nutrition | Autogenic | NCT05138276 | 60 | Early Phase 1 | |
| Recruiting | Ulcerative Colitis | Allogenic | NCT04882683 | 50 | NA | |
| Unknown | Crohn’s Disease | Allogenic | NCT02000362 | 24 | 1, 2 | |
| Completed | Bone disorders | Severe Osteopetrosis | Allogenic | NCT00775931 | 7 | 2, 3 |
| Suspended | Osteonecrosis of Femoral Head | Allogenic | NCT03180463 | 30 | 1, 2 | |
| Recruiting | Congenital Bone Marrow Failure Syndromes | Allogenic | NCT01962415 | 100 | 2 | |
| Completed | Respiratory tract diseases | Bronchopulmonary Dysplasia | Allogenic | NCT02381366 | 12 | 1, 2 |
| Completed | Allogenic | NCT01297205 | 9 | 1 | ||
| Completed | Respiratory Tract Infections | Allogenic | NCT02023788 | 8 | NA | |
| Completed | Premature Birth of Newborn | Allogenic | NCT02023788 | 8 | NA | |
| Not yet recruiting | Severe Acute Respiratory Syndrome (SARS) Pneumonia | Allogenic | NCT04299152 | 20 | 2 | |
| Recruiting | COPD | Allogenic | NCT04433104 | 40 | NA |
| Private or public ownership of the banks | Major investigations have been conducted to determine whether or not the owners of private banks work for only commercial interests. Another concern relates to the ownership of stem cells by commercial and public banks, the methods for obtaining services from these banks, and the design of justice for access to bank services. It has been observed that private banks work to increase their economic capital, while general banks assist those in need. |
| Informed consent | Fifteen articles mentioned the requirement of informed consent from the donors and receivers. Obtaining informed consent before doing any investigative or therapeutic actions on patients is a concept that has been introduced previously in the medical field. It is one of the most important foundational concepts in the medical industry, and it will result in favorable ethical and moral outcomes. It is one of the most critical aspects of the patient’s right to donate UCB to the banks. It will give patients a better understanding of UCB collection and storage advantages. |
| Justice to access the services | The UCB stem cell banks are obligated to provide equal assistance to the needy; they must not work solely for economic gain. Equality is a crucial criterion or indicator for determining the success of health-related challenges. One of the primary concerns is that everyone should benefit from these services, regardless of their social or economic status. |
| Conflicts of interest | Three studies in our review mentioned the conflict of interest involved in the umbilical cord blood banking process. Corruption is the primary source of conflicts of interest. Conflicts of interest must be avoided and managed. When an organization or center’s interests collide with the lives and health of individuals, the conflict of interest is highlighted. |
| Social Problems | People’s perspectives on health concerns are essential in determining the success of any endeavor. Many studies have found that people need to be properly informed about UCB banks and their services. Efforts must be made to promote the process of UCB banking and to improve people’s perceptions of it by offering training. This is so that people can access suitable services, and so that healthcare professionals can be motivated to expand UCB operations in the health sector. People in some countries do not have a positive attitude toward banking because they may have received little or wrong facts about UCB banking. |
| Confidentiality | The actions of confidentiality in the hospital are a fundamental entitlement for patients, that cannot be taken away from them. According to the findings of the three surveys, many people voiced concerns about the confidentiality of their personal information in such banks. Doubts were expressed that their cells may be employed for something else. Donors and recipients were also concerned that their personal information might be shared with someone else. According to certain studies, the bank’s operations should be transparent. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devi, S.; Bongale, A.M.; Tefera, M.A.; Dixit, P.; Bhanap, P. Fresh Umbilical Cord Blood—A Source of Multipotent Stem Cells, Collection, Banking, Cryopreservation, and Ethical Concerns. Life 2023, 13, 1794. https://doi.org/10.3390/life13091794
Devi S, Bongale AM, Tefera MA, Dixit P, Bhanap P. Fresh Umbilical Cord Blood—A Source of Multipotent Stem Cells, Collection, Banking, Cryopreservation, and Ethical Concerns. Life. 2023; 13(9):1794. https://doi.org/10.3390/life13091794
Chicago/Turabian StyleDevi, Seeta, Anupkumar M. Bongale, Minyechil Alehegn Tefera, Prashant Dixit, and Prasad Bhanap. 2023. "Fresh Umbilical Cord Blood—A Source of Multipotent Stem Cells, Collection, Banking, Cryopreservation, and Ethical Concerns" Life 13, no. 9: 1794. https://doi.org/10.3390/life13091794
APA StyleDevi, S., Bongale, A. M., Tefera, M. A., Dixit, P., & Bhanap, P. (2023). Fresh Umbilical Cord Blood—A Source of Multipotent Stem Cells, Collection, Banking, Cryopreservation, and Ethical Concerns. Life, 13(9), 1794. https://doi.org/10.3390/life13091794