
Mild Hyperbaric Oxygen Exposure Enhances Peripheral Circulatory Natural Killer Cells in Healthy Young Women

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design and Participants
2.2. Sample Size and Power Calculation
2.3. Experimental Protocol
2.4. Measurements
2.4.1. Participants Characteristics
2.4.2. Electrocardiography Analysis
2.4.3. Flow-Cytometric Analysis
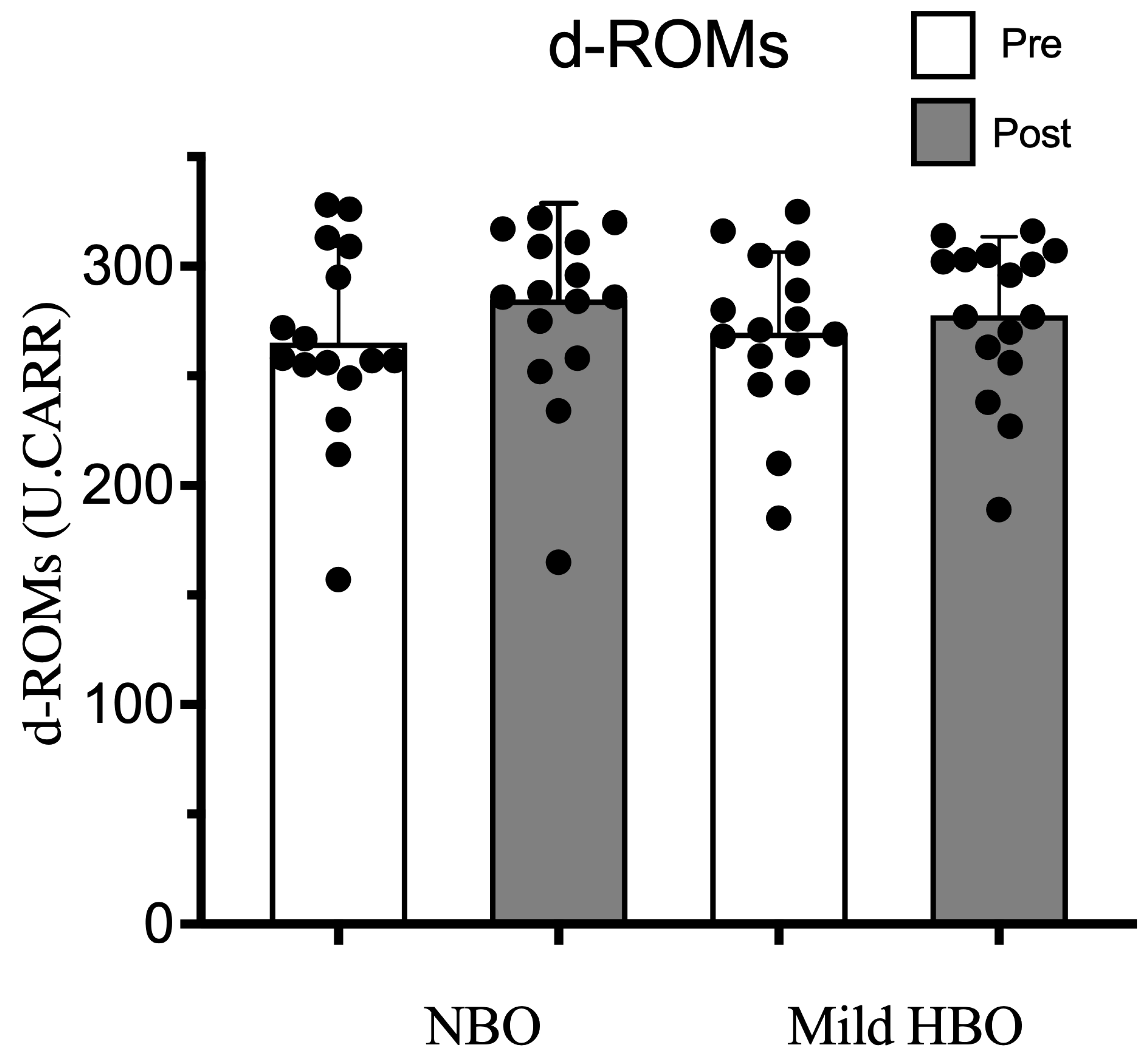
2.4.4. Oxidative Stress Measured by the d-ROMs Test
2.4.5. Cytokine Analysis
- IL-6
- 2.
- IL-12p70
2.4.6. Changes in Plasma Volume Calculations
2.4.7. Statistical Analyses
3. Results
3.1. Parasympathetic Activity
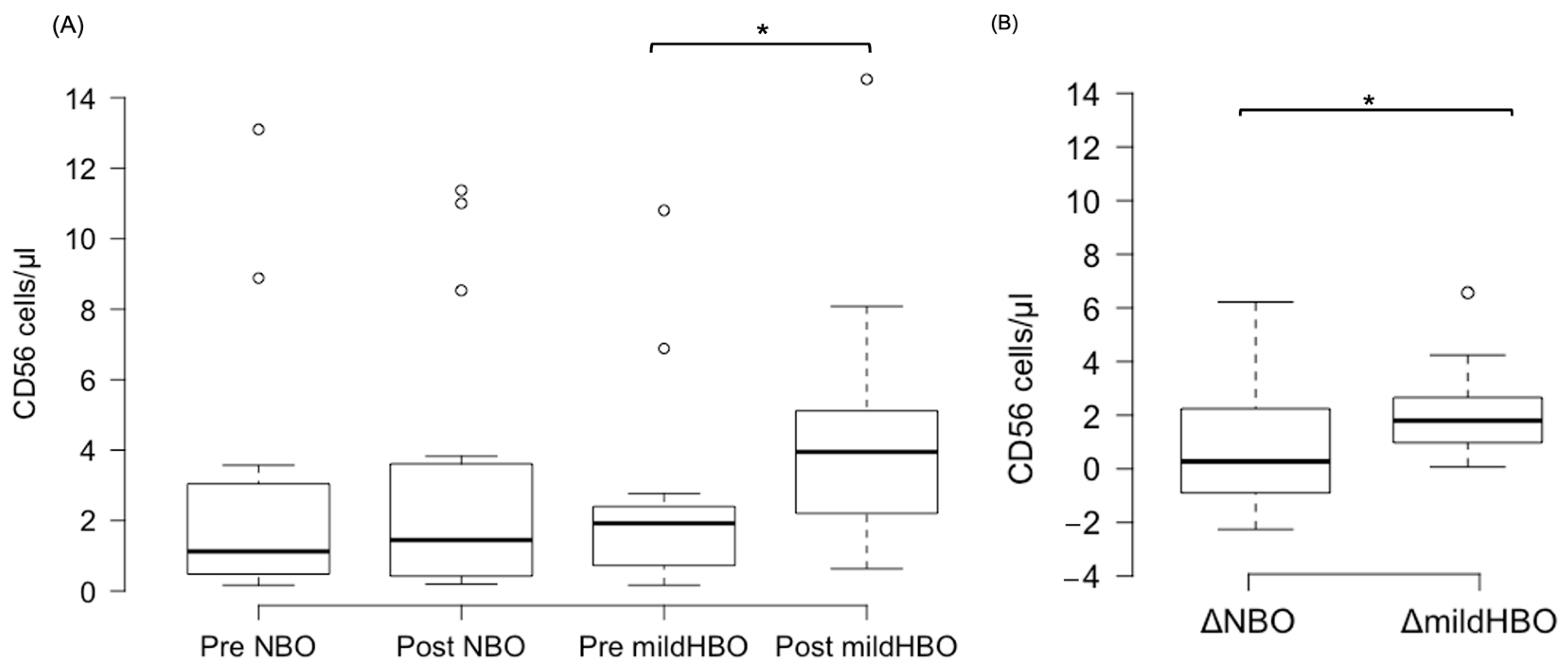
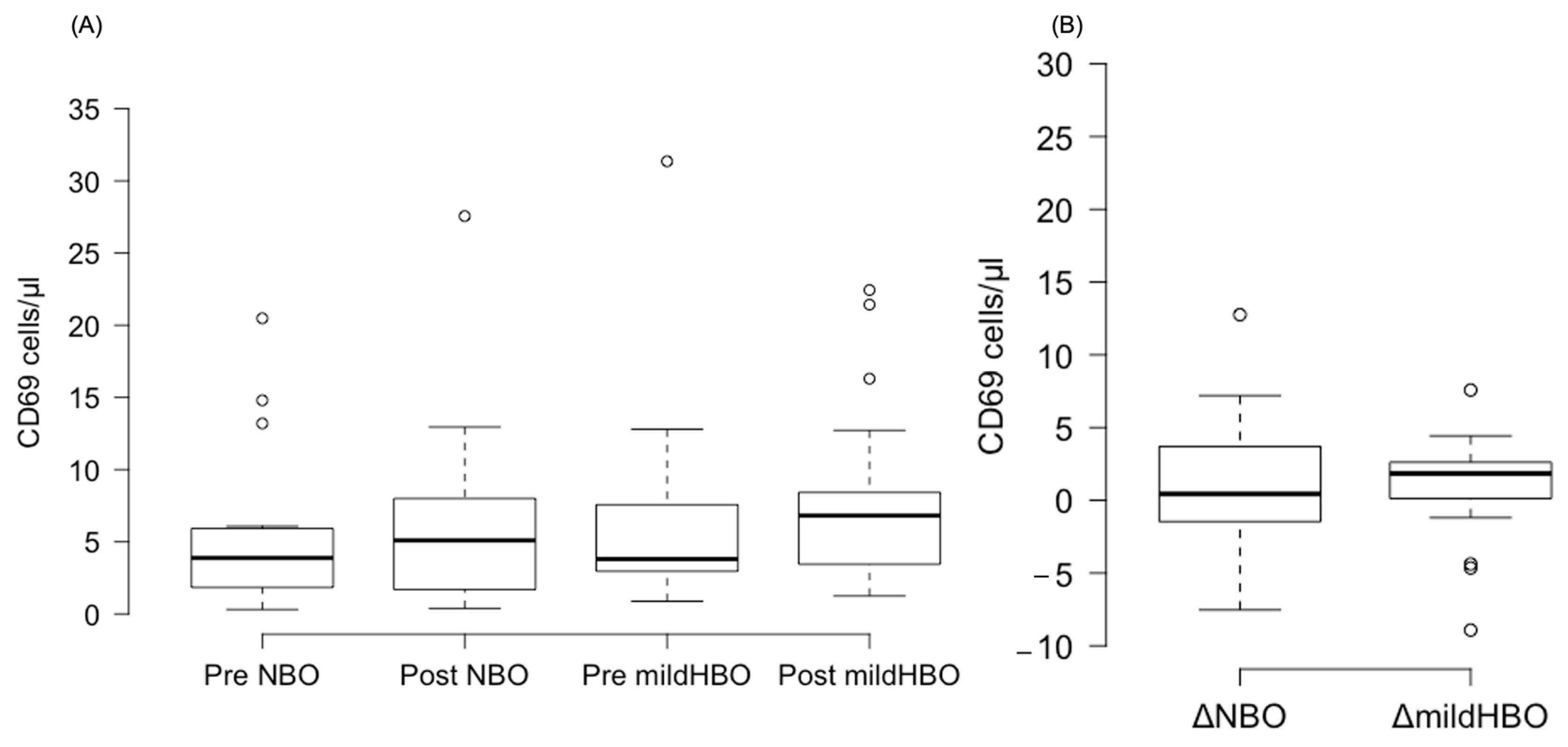
3.2. NK Cells and Activation NK Cell Marker
3.3. d-ROMs, a Measure of Oxidative Stress
3.4. Cytokines
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stirban, A.; Lentrodt, S.; Nandrean, S.; Pop, A.; Tschoepe, D.; Scherbaum, W.A. Functional Changes in Microcirculation during Hyperbaric and Normobaric Oxygen Therapy. Undersea Hyperb. Med. 2009, 36, 381–390. [Google Scholar] [PubMed]
- Bhutani, S.; Vishwanath, G. Hyperbaric Oxygen and Wound Healing. Indian J. Plast. Surg. 2012, 45, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Akarsu, S.; Tekin, L.; Ay, H.; Çarli, A.B.; Tok, F.; Şimşek, K.; Kiralp, M.Z. The Efficacy of Hyperbaric Oxygen Therapy in the Management of Chronic Fatigue Syndrome. Undersea Hyperb. Med. 2013, 40, 197–200. [Google Scholar]
- Demchenko, I.T.; Zhilyaev, S.Y.; Moskvin, A.N.; Krivchenko, A.I.; Piantadosi, C.A.; Allen, B.W. Baroreflex-Mediated Cardiovascular Responses to Hyperbaric Oxygen. J. Appl. Physiol. 2013, 115, 819–828. [Google Scholar] [CrossRef]
- Heitkemper, M.; Burr, R.L.; Jarrett, M.; Hertig, V.; Lustyk, M.K.; Bond, E.F. Evidence for Autonomic Nervous System Imbalance in Women with Irritable Bowel Syndrome. Dig. Dis. Sci. 1998, 43, 2093–2098. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Lavin, M.; Hermosillo, A.G. Autonomic Nervous System Dysfunction May Explain the Multisystem Features of Fibromyalgia. Semin. Arthritis Rheum. 2000, 29, 197–199. [Google Scholar] [CrossRef]
- Ilagan, R.; Winarski, M.; Lagina, A. Indications for Emergent Hyperbaric Oxygen Therapy. Curr. Emerg. Hosp. Med. Rep. 2022, 10, 134–142. [Google Scholar] [CrossRef]
- Hamilton-Farrell, M.; Bhattacharyya, A. Barotrauma. Injury 2004, 35, 359–370. [Google Scholar] [CrossRef]
- Narkowicz, C.K.; Vial, J.H.; Mccartney, P.W. Hyperbaric Oxygen Therapy Increases Free Radical Levels in the Blood of Humans. Free Radic. Res. Commun. 1993, 19, 71–80. [Google Scholar] [CrossRef]
- Moon, R.E.; Camporesi, E.M. Respiratory Monitoring. In Anesthesia, 5th ed.; Elsevier Churchill Livingstone: Philadelphia, PA, USA, 2000; pp. 1255–1295. [Google Scholar]
- Plafki, C.; Peters, P.; Almeling, M.; Welslau, W.; Busch, R. Complications and Side Effects of Hyperbaric Oxygen Therapy. Aviat. Space Environ. Med. 2000, 71, 119–124. [Google Scholar] [PubMed]
- Heyboer, M. Hyperbaric Oxygen Therapy Side Effects—Where Do We Stand? J. Am. Coll. Clin. Wound Spec. 2016, 8, 2–3. [Google Scholar] [CrossRef]
- Thom, S.R. Oxidative Stress Is Fundamental to Hyperbaric Oxygen Therapy. J. Appl. Physiol. 2009, 106, 988–995. [Google Scholar] [CrossRef] [PubMed]
- Dennog, C.; Hartmann, A.; Frey, G.; Speit, G. Detection of DNA Damage after Hyperbaric Oxygen (HBO) Therapy. Mutagenesis 1996, 11, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, A. Mild Hyperbaric Oxygen: Mechanisms and Effects. J. Physiol. Sci. 2019, 69, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Takemura, A.; Ishihara, A. Mild Hyperbaric Oxygen Inhibits Growth-Related Decrease in Muscle Oxidative Capacity of Rats with Metabolic Syndrome. J. Atheroscler. Thromb. 2017, 24, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Aoki, N.; Adachi, T.; Tsujimoto, G.; Gu, N.; Matsunaga, T.; Kikuchi, N.; Tsuda, K.; Ishihara, A. Hyperbaric Exposure with High Oxygen Concentration Inhibits Growth-Associated Increase in the Glucose Level of Diabetic Goto-Kakizaki Rats. Diabetes Obes. Metab. 2006, 8, 714–715. [Google Scholar] [CrossRef]
- Nagatomo, F.; Fujino, H.; Takeda, I.; Ishihara, A. Effects of Hyperbaric Oxygenation on Blood Pressure Levels of Spontaneously Hypertensive Rats. Clin. Exp. Hypertens. 2010, 32, 193–197. [Google Scholar] [CrossRef]
- Ishihara, A.; Nagatomo, F.; Fujino, H.; Kondo, H. Exposure to Mild Hyperbaric Oxygen Increases Blood Flow and Resting Energy Expenditure but Not Oxidative Stress. J. Sci. Res. Rep. 2014, 3, 1886–1896. [Google Scholar] [CrossRef]
- Nisa, B.U.; Hirabayashi, T.; Maeshige, N.; Kondo, H.; Fujino, H. Beneficial Effects of Mild Hyperbaric Oxygen Exposure on Microcirculation in Peripheral Tissues in Healthy Subjects: Pilot Study. J. Sports Med. Phys. Fit. 2022, 62, 1600–1604. [Google Scholar] [CrossRef]
- Kenney, M.J.; Ganta, C.K. Autonomic Nervous System and Immune System Interactions. Compr. Physiol. 2014, 4, 1177–1200. [Google Scholar] [CrossRef]
- Rinner, I.; Felsner, P.; Falus, A.; Skreiner, E.; Kukulansky, T.; Globerson, A.; Hirokawa, K.; Schauenstein, K. Cholinergic Signals to and from the Immune System. Immunol. Lett. 1995, 44, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Ulloa, L. The Vagus Nerve and the Nicotinic Anti-Inflammatory Pathway. Nat. Rev. Drug Discov. 2005, 4, 673–684. [Google Scholar] [CrossRef]
- van Erp, E.A.; van Kampen, M.R.; van Kasteren, P.B.; de Wit, J. Viral Infection of Human Natural Killer Cells. Viruses 2019, 11, 243. [Google Scholar] [CrossRef]
- Morimoto, K.; Takeshita, T.; Inoue-Sakurai, C.; Maruyama, S. Lifestyles and Mental Health Status Are Associated with Natural Killer Cell and Lymphokine-Activated Killer Cell Activities. Sci. Total Environ. 2001, 270, 3–11. [Google Scholar] [CrossRef]
- Inoue, C.; Takeshita, T.; Kondo, H.; Morimoto, K. Cigarette Smoking Is Associated with the Reduction of Lymphokine-Activated Killer Cell and Natural Killer Cell Activities. Environ. Health Prev. Med. 1996, 1, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Daniela, M.; Catalina, L.; Ilie, O.; Paula, M.; Daniel-Andrei, I.; Ioana, B. Effects of Exercise Training on the Autonomic Nervous System with a Focus on Anti-Inflammatory and Antioxidants Effects. Antioxidants 2022, 11, 350. [Google Scholar] [CrossRef] [PubMed]
- Moldoveanu, A.I.; Shephard, R.J.; Shek, P.N. The Cytokine Response to Physical Activity and Training. Sports Med. 2001, 31, 115–144. [Google Scholar] [CrossRef] [PubMed]
- Krog, J.; Tønnesen, E.; Jepsen, C.F.; Parner, E.; Segadal, K.; Hope, A.; Ulvik, R.J.; Hokland, M.E. Natural Killer Cells as Biomarkers of Hyperbaric Stress During a Dry Heliox Saturation Dive. Aviat. Space Environ. Med. 2010, 81, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Dupont, W.D.; Plummer, W.D. Power and Sample Size Calculations: A Review and Computer Program. Control. Clin. Trials 1990, 11, 116–128. [Google Scholar] [CrossRef]
- Evans, S.R. Clinical Trial Structures. J. Exp. Stroke Transl. Med. 2010, 3, 8. [Google Scholar] [CrossRef]
- Omagari, K.; Kumamoto, R.; Koyama, Y.; Suzuta, M.; Taniguchi, A.; Fukuda, A.; Iwami, M.; Koba, K.; Kawaguchi, A.; Otsuka, K. Prevalence of Chronic Constipation and Irritable Bowel Syndrome, and Their Overlap, among Female Undergraduate Students in Japan. OBM Hepatol. Gastroenterol. 2020, 4, 18. [Google Scholar] [CrossRef]
- Chang, W.L.; Hou, C.J.Y.; Wei, S.P.; Tsai, J.P.; Chen, Y.J.; Chen, M.L.; Chuech, C.C.; Hung, C.L.; Huang, M.Y.; Lee, C.H.; et al. Utilization and Clinical Feasibility of a Handheld Remote Electrocardiography Recording Device in Cardiac Arrhythmias and Atrial Fibrillation: A Pilot Study. Int. J. Gerontol. 2015, 9, 206–210. [Google Scholar] [CrossRef]
- Morimoto, M.; Satomura, S.; Hashimoto, T.; Ito, E.; Kyotani, S. Oxidative Stress Measurement and Prediction of Epileptic Seizure in Children and Adults with Severe Motor and Intellectual Disabilities. J. Clin. Med. Res. 2016, 8, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Van Beaumont, W. Evaluation of Hemoconcentration from Hematocrit Measurements. J. Appl. Physiol. 1972, 32, 712–713. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.d.O.; Franco, O.S.; Borges, M.M.; Martins, C.N.; Guerreiro, L.F.; da Rosa, C.E.; Paulitsch, F.d.S.; Perez, W.; da Silva, A.M.V.; Signori, L.U. The Importance of Adjustments for Changes in Plasma Volume in the Interpretation of Hematological and Inflammatory Responses after Resistance Exercise. J. Exerc. Physiol. Online 2014, 17, 72–83. [Google Scholar]
- Sherk, V.D.; Chrisman, C.; Smith, J.; Young, K.C.; Singh, H.; Bemben, M.G.; Bemben, D.A. Acute Bone Marker Responses to Whole-Body Vibration and Resistance Exercise in Young Women. J. Clin. Densitom. 2013, 16, 104–109. [Google Scholar] [CrossRef]
- Heyboer, M.; Milovanova, T.N.; Wojcik, S.; Grant, W.; Chin, M.; Hardy, K.R.; Lambert, D.S.; Logue, C.; Thom, S.R. CD34+/CD45-Dim Stem Cell Mobilization by Hyperbaric Oxygen—Changes with Oxygen Dosage. Stem Cell Res. 2014, 12, 638–645. [Google Scholar] [CrossRef]
- Hadanny, A.; Efrati, S. The Hyperoxic-Hypoxic Paradox. Biomolecules 2020, 10, 958. [Google Scholar] [CrossRef]
- Shandley, S.; Wolf, E.G.; Schubert-Kappan, C.M.; Baugh, L.M.; Richards, M.F.; Prye, J.; Arizpe, H.M.; Kalns, J. Increased Circulating Stem Cells and Better Cognitive Performance in Traumatic Brain Injury Subjects following Hyperbaric Oxygen Therapy. Undersea Hyperb. Med. 2017, 44, 257–269. [Google Scholar] [CrossRef]
- Hehenberger, K.; Brismar, K.; Lind, F.; Kratz, G. Dose-Dependent Hyperbaric Oxygen Stimulation of Human Fibroblast Proliferation. Wound Repair Regen. 1997, 5, 147–150. [Google Scholar] [CrossRef]
- Sahni, T.; Hukku, S.; Jain, M.; Prasad, A.; Prasad, R.; Singh, K. Recent Advances in Hyperbaric Oxygen Therapy. Med. Updat. 2004, 14, 632–639. [Google Scholar]
- Mori, H.; Nishijo, K.; Kawamura, H.; Abo, T. Unique Immunomodulation by Electro-Acupuncture in Humans Possibly via Stimulation of the Autonomic Nervous System. Neurosci. Lett. 2002, 320, 21–24. [Google Scholar] [CrossRef]
- Mathieu, D.; Favory, R.; Collet, F.; Linke, J.-C.; Wattel, F. Physiologic Effects of Hyperbaric Oxygen on Hemodynamics and Microcirculation. In Handbook on Hyperbaric Medicine; Mathieu, D., Ed.; Springer: Dordrecht, The Netherlands, 2006; pp. 75–101. ISBN 978-1-4020-4448-9. [Google Scholar]
- Chateau-Degat, M.L.; Belley, R. Hyperbaric Oxygen Therapy Decreases Blood Pressure in Patients with Chronic Wounds. Undersea Hyperb. Med. 2012, 39, 881. [Google Scholar]
- Capellino, S.; Claus, M.; Watzl, C. Regulation of Natural Killer Cell Activity by Glucocorticoids, Serotonin, Dopamine, and Epinephrine. Cell. Mol. Immunol. 2020, 17, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Poli, A.; Michel, T.; Thérésine, M.; Andrès, E.; Hentges, F.; Zimmer, J. CD56brightnatural Killer (NK) Cells: An Important NK Cell Subset. Immunology 2009, 126, 458–465. [Google Scholar] [CrossRef] [PubMed]
- de Wolde, S.D.; Hulskes, R.H.; de Jonge, S.W.; Hollmann, M.W.; van Hulst, R.A.; Weenink, R.P.; Kox, M. The Effect of Hyperbaric Oxygen Therapy on Markers of Oxidative Stress and the Immune Response in Healthy Volunteers. Front. Physiol. 2022, 13, 826163. [Google Scholar] [CrossRef]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M.; Telser, J. Free Radicals and Antioxidants in Normal Physiological Functions and Human Disease. Int. J. Biochem. Cell Biol. 2007, 39, 44–84. [Google Scholar] [CrossRef]
- Hedetoft, M.; Garred, P.; Madsen, M.B.; Hyldegaard, O. Hyperbaric Oxygen Treatment Is Associated with a Decrease in Cytokine Levels in Patients with Necrotizing Soft-Tissue Infection. Physiol. Rep. 2021, 9, e14757. [Google Scholar] [CrossRef]
- Bosco, G.; Vezzani, G.; Mrakic Sposta, S.; Rizzato, A.; Enten, G.; Abou-samra, A.; Malacrida, S.; Quartesan, S.; Vezzoli, A.; Camporesi, E. Hyperbaric Oxygen Therapy Ameliorates Osteonecrosis in Patients by Modulating Inflammation and Oxidative Stress. J. Enzym. Inhib. Med. Chem. 2018, 33, 1501–1505. [Google Scholar] [CrossRef]
- Watford, W.T.; Moriguchi, M.; Morinobu, A.; O’Shea, J.J. The Biology of IL-12: Coordinating Innate and Adaptive Immune Responses. Cytokine Growth Factor Rev. 2003, 14, 361–368. [Google Scholar] [CrossRef]
- Hartmann, G.; Tschöp, M.; Fischer, R.; Bidlingmaier, C.; Riepl, R.; Tschöp, K.; Hautmann, H.; Endres, S.; Toepfer, M. High Altitude Increases Circulating Interleukin-6, Interleukin-1 Receptor Antagonist and c-Reactive Protein. Cytokine 2000, 12, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Del Valle-Mendoza, J.; Tarazona-Castro, Y.; Merino-Luna, A.; Carrillo-Ng, H.; Kym, S.; Aguilar-Luis, M.A.; del Valle, L.J.; Aquino-Ortega, R.; Martins-Luna, J.; Peña-Tuesta, I.; et al. Comparison of Cytokines Levels among COVID-19 Patients Living at Sea Level and High Altitude. BMC Infect. Dis. 2022, 22, 96. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | SD |
|---|---|---|
| Height (cm) | 160.63 | 5.83 |
| Body weight (kg) | 54.24 | 8.99 |
| Body Fat (%) | 28.32 | 6.11 |
| Fat Mass (kg) | 15.81 | 6.20 |
| Lean mass (kg) | 38.45 | 3.68 |
| Muscle mass (kg) | 36.26 | 3.36 |
| Total body water (kg) | 26.68 | 3.05 |
| Estimated bone mass (kg) | 2.19 | 0.33 |
| Basal metabolic rate (kcal) | 1184.25 | 125.32 |
| Body age (years) | 26 | 9.38 |
| Visceral fat level | 3.06 | 1.88 |
| Leg muscle mass score | 95.75 | 10.81 |
| Variables | Pre NBO | Post NBO | Pre Mild HBO | Post Mild HBO | F-Ratio | p Value |
|---|---|---|---|---|---|---|
| IL-6 (pg/mL) | 1.1 ± 0.4 | 1.1 ± 0.3 | 1.3 ± 0.3 | 1.3 ± 0.4 | 0.065 | 0.38 |
| IL-12p70 (pg/mL) | 0.6 ± 0.3 | 0.5 ± 0.2 | 0.6 ± 0.3 | 0.5 ± 0.3 | 1.816 | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nisa, B.U.; Nakanishi, R.; Tanaka, M.; Lin, H.; Hirabayashi, T.; Maeshige, N.; Kondo, H.; Fujino, H. Mild Hyperbaric Oxygen Exposure Enhances Peripheral Circulatory Natural Killer Cells in Healthy Young Women. Life 2023, 13, 408. https://doi.org/10.3390/life13020408
Nisa BU, Nakanishi R, Tanaka M, Lin H, Hirabayashi T, Maeshige N, Kondo H, Fujino H. Mild Hyperbaric Oxygen Exposure Enhances Peripheral Circulatory Natural Killer Cells in Healthy Young Women. Life. 2023; 13(2):408. https://doi.org/10.3390/life13020408
Chicago/Turabian StyleNisa, Badur Un, Ryosuke Nakanishi, Minoru Tanaka, Hao Lin, Takumi Hirabayashi, Noriaki Maeshige, Hiroyo Kondo, and Hidemi Fujino. 2023. "Mild Hyperbaric Oxygen Exposure Enhances Peripheral Circulatory Natural Killer Cells in Healthy Young Women" Life 13, no. 2: 408. https://doi.org/10.3390/life13020408
APA StyleNisa, B. U., Nakanishi, R., Tanaka, M., Lin, H., Hirabayashi, T., Maeshige, N., Kondo, H., & Fujino, H. (2023). Mild Hyperbaric Oxygen Exposure Enhances Peripheral Circulatory Natural Killer Cells in Healthy Young Women. Life, 13(2), 408. https://doi.org/10.3390/life13020408