
Can Lung Imaging Scores and Clinical Variables Predict Severe Course and Fatal Outcome in COVID-19 Pneumonia Patients? A Single-Center Observational Study

 , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
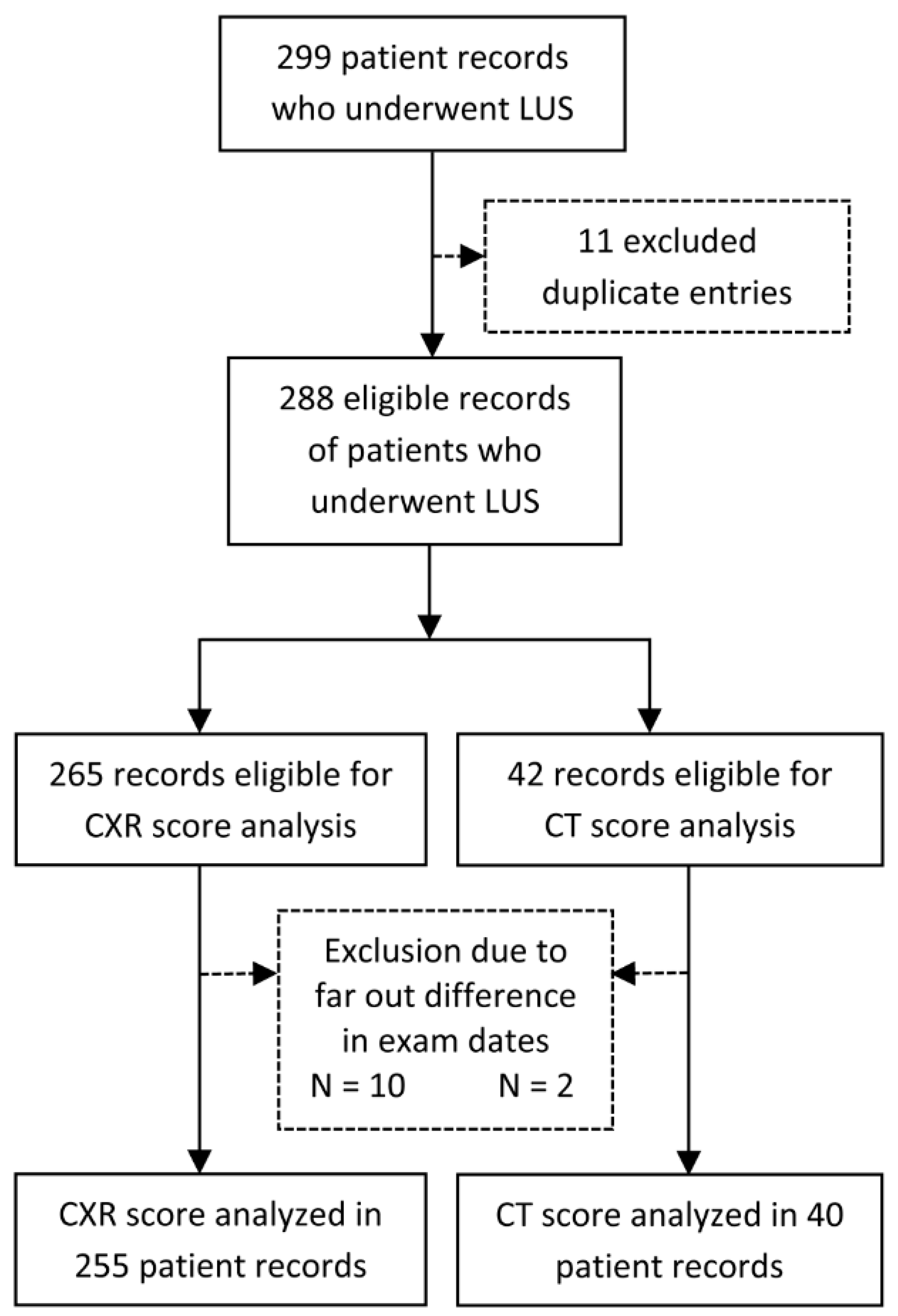
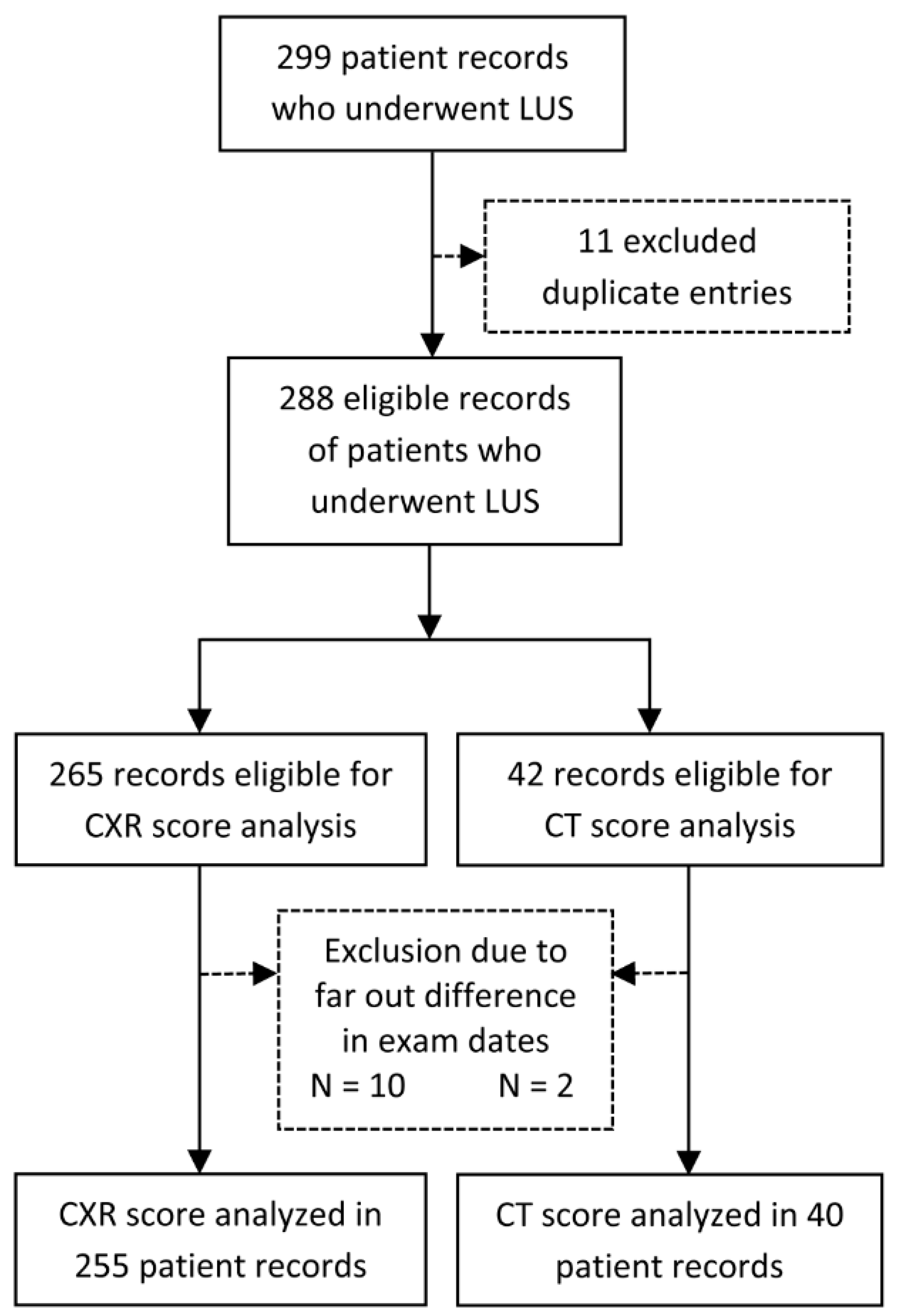
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Outcomes
2.4. Data Extraction
2.5. Acquisition Protocol
2.6. Bias
2.7. Study Size
2.8. Statistical Analysis
2.9. Reporting
3. Results
3.1. Patients and Characteristics
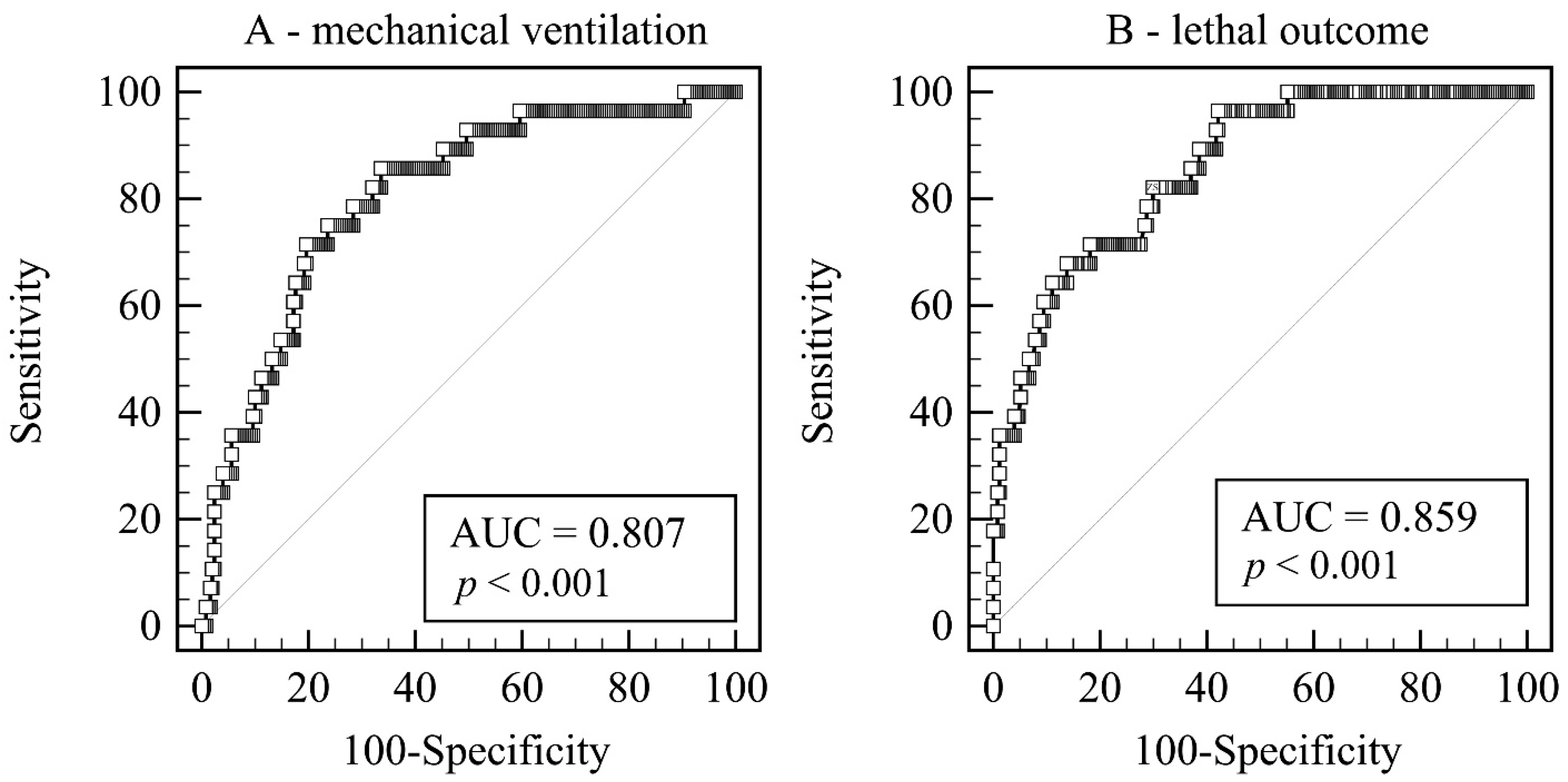
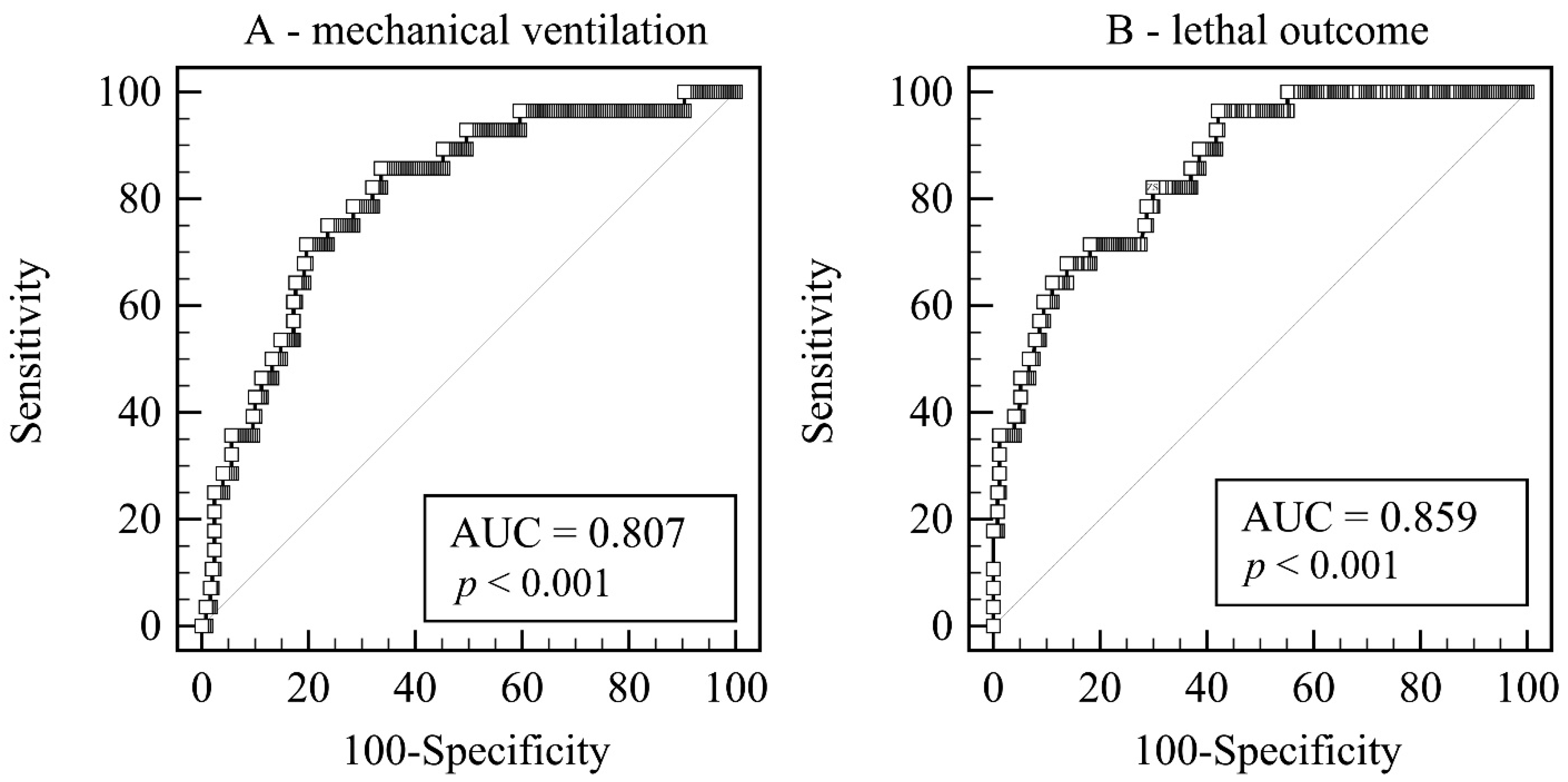
3.2. Predictors of Necessity for MV or a Lethal Outcome
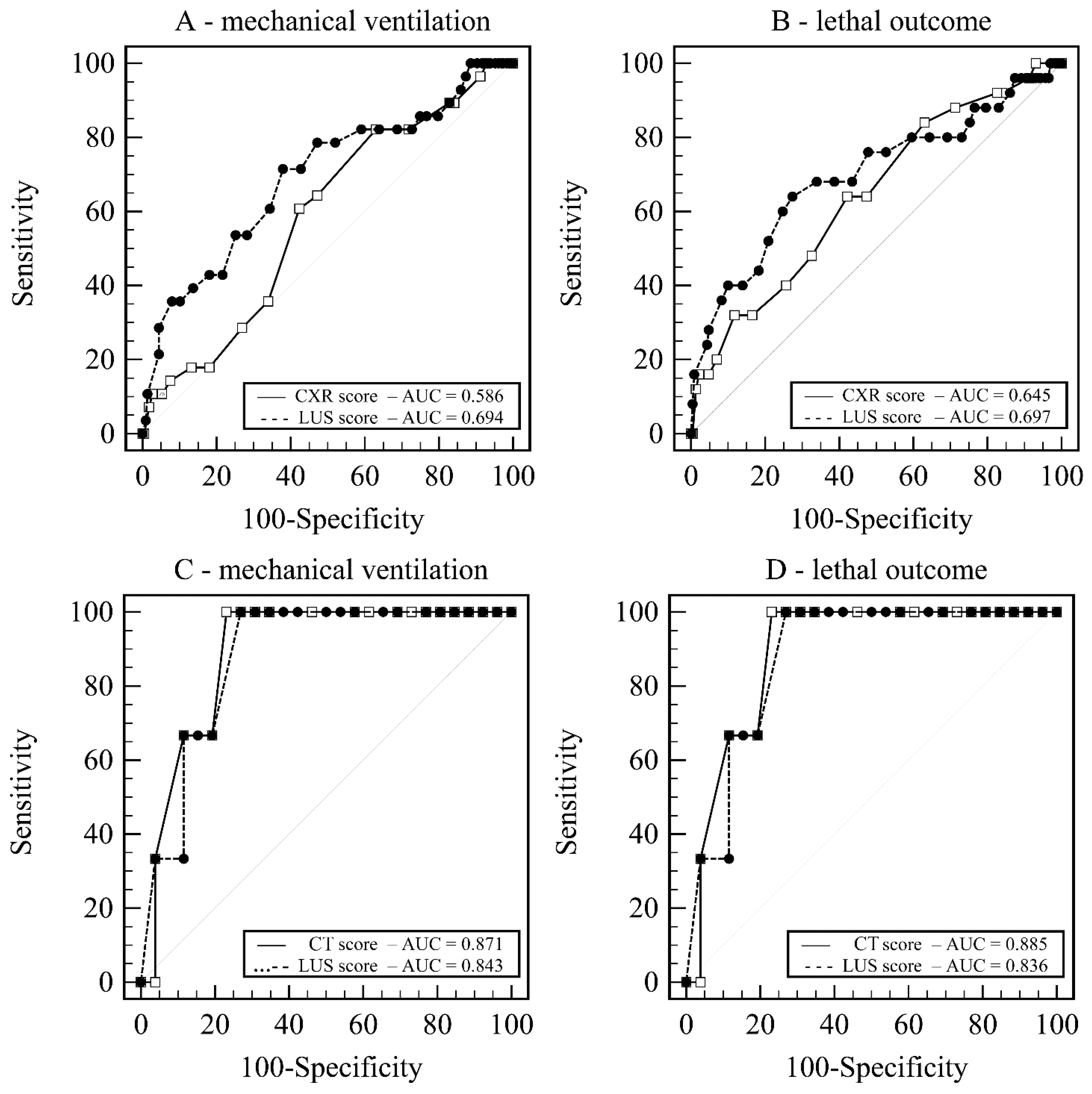
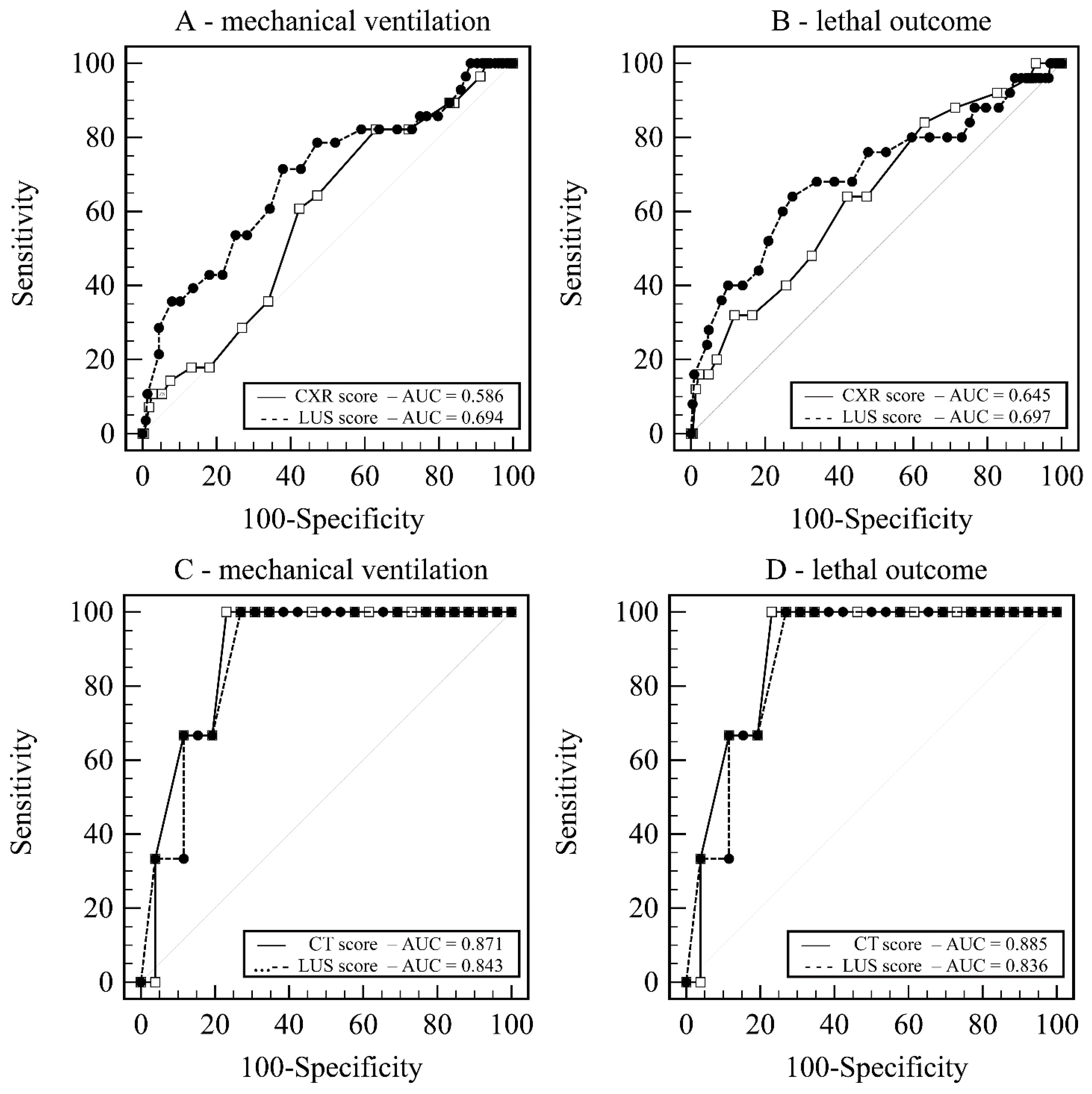
3.3. Relationship between LUS and CXR Scores
3.4. Relationship between LUS and CT Scores
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Diagnostic Testing for SARS-CoV-2. Available online: https://www.who.int/publications/i/item/diagnostic-testing-for-sars-cov-2 (accessed on 18 April 2021).
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.C.; Di Napoli, R.S. Features, Evaluation, and Treatment of Coronavirus; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Borakati, A.; Perera, A.; Johnson, J.; Sood, T. Diagnostic accuracy of X-ray versus CT in COVID-19: A propensity-matched database study. BMJ Open 2020, 10, e042946. [Google Scholar] [CrossRef] [PubMed]
- Kovács, A.; Palásti, P.; Veréb, D.; Bozsik, B.; Palkó, A.; Kincses, Z.T. The sensitivity and specificity of chest CT in the diagnosis of COVID-19. Eur. Radiol. 2021, 31, 2819–2824. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, A.E.; Naidu, S.; Ramachandran, S.; Kaufman, D.S.; Fayad, Z.A.; Mani, V. Review of radiographic findings in COVID-19. World J. Radiol. 2020, 12, 142–155. [Google Scholar] [CrossRef]
- Jackson, K.; Butler, R.; Aujayeb, A. Lung ultrasound in the COVID-19 pandemic. Postgrad. Med. J. 2021, 97, 34–39. [Google Scholar] [CrossRef]
- Lieveld, A.W.; Kok, B.; Schuit, F.H.; Azijli, K.; Heijmans, J.; van Laarhoven, A.; Assman, N.L.; Kootte, R.S.; Olgers, T.J.; Nanayakkara, P.W.; et al. Diagnosing COVID-19 pneumonia in a pandemic setting: Lung Ultrasound versus CT (LUVCT)—A multicentre, prospective, observational study. ERJ Open Res. 2020, 6, 00539-2020. [Google Scholar] [CrossRef]
- Ottaviani, S.; Franc, M.; Ebstein, E.; Demaria, L.; Lheure, C.; Debray, M.; Khalil, A.; Crestani, B.; Borie, R.; Dieudé, P. Lung ultrasonography in patients with COVID-19: Comparison with CT. Clin. Radiol. 2020, 75, 877.e1–877.e6. [Google Scholar] [CrossRef]
- Nouvenne, A.; Zani, M.D.; Milanese, G.; Parise, A.; Baciarello, M.; Bignami, E.G.; Odone, A.; Sverzellati, N.; Meschi, T.; Ticinesi, A. Lung Ultrasound in COVID-19 Pneumonia: Correlations with Chest CT on Hospital admission. Respir. Int. Rev. Thorac. Dis. 2020, 99, 617–624. [Google Scholar] [CrossRef]
- Skopljanac, I.; Ivelja, M.; Barcot, O.; Brdar, I.; Dolic, K.; Polasek, O.; Radic, M. Role of Lung Ultrasound in Predicting Clinical Severity and Fatality in COVID-19 Pneumonia. J. Pers. Med. 2021, 11, 757. [Google Scholar] [CrossRef]
- Gutsche, H.; Lesser, T.G.; Wolfram, F.; Doenst, T. Significance of Lung Ultrasound in Patients with Suspected COVID-19 Infection at Hospital Admission. Diagnostics 2021, 11, 921. [Google Scholar] [CrossRef]
- Mohammad, S.; Aziz, R.; Al Mahri, S.; Malik, S.S.; Haji, E.; Khan, A.H.; Khatlani, T.S.; Bouchama, A. Obesity and COVID-19: What makes obese host so vulnerable? Immun. Ageing 2021, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients With COVID-19 Pneumonia: The CALL Score. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 1393–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, G.; Kovalic, A.J.; Graber, C.J. Prognostic Value of Leukocytosis and Lymphopenia for Coronavirus Disease Severity. Emerg. Infect. Dis. 2020, 26, 1839–1841. [Google Scholar] [CrossRef]
- Luo, X.; Zhou, W.; Yan, X.; Guo, T.; Wang, B.; Xia, H.; Ye, L.; Xiong, J.; Jiang, Z.; Liu, Y.; et al. Prognostic Value of C-Reactive Protein in Patients with Coronavirus 2019. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 2174–2179. [Google Scholar] [CrossRef]
- Fink, D.L.; Khan, P.Y.; Goldman, N.; Cai, J.; Hone, L.; Mooney, C.; El-Shakankery, K.H.; Sismey, G.; Whitford, V.; Marks, M.; et al. Development and internal validation of a diagnostic prediction model for COVID-19 at time of admission to hospital. QJM Mon. J. Assoc. Physicians 2021, 114, 699–705. [Google Scholar] [CrossRef]
- Guan, X.; Zhang, B.; Fu, M.; Li, M.; Yuan, X.; Zhu, Y.; Peng, J.; Guo, H.; Lu, Y. Clinical and inflammatory features based machine learning model for fatal risk prediction of hospitalized COVID-19 patients: Results from a retrospective cohort study. Ann. Med. 2021, 53, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Qi, J.; He, D.; Yang, D.; Wang, M.; Ma, W.; Cui, H.; Ye, F.; Wang, F.; Xu, J.; Li, Z.; et al. Severity-associated markers and assessment model for predicting the severity of COVID-19: A retrospective study in Hangzhou, China. BMC Infect. Dis. 2021, 21, 774. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Deng, G.; Cui, Y.; Zhang, Y.; Dai, M.; Chen, L.; Han, D.; Li, W.; Guo, K.; Chen, X.; et al. A predictive model for the severity of COVID-19 in elderly patients. Aging 2020, 12, 20982–20996. [Google Scholar] [CrossRef]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Proposal for International Standardization of the Use of Lung Ultrasound for Patients With COVID-19: A Simple, Quantitative, Reproducible Method. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2020, 39, 1413–1419. [Google Scholar] [CrossRef] [Green Version]
- Smargiassi, A.; Soldati, G.; Torri, E.; Mento, F.; Milardi, D.; del Giacomo, P.; de Matteis, G.; Burzo, M.L.; Larici, A.R.; Pompili, M.; et al. Lung Ultrasound for COVID-19 Patchy Pneumonia: Extended or Limited Evaluations. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2021, 40, 521–528. [Google Scholar] [CrossRef]
- Borghesi, A.; Maroldi, R. COVID-19 outbreak in Italy: Experimental chest X-ray scoring system for quantifying and monitoring disease progression. La Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Tukey, J.W. Exploratory Data Analysis; THETA: Reading, MA, USA, 1977; Volume 2. [Google Scholar]
- Gibbons, R.C.; Magee, M.; Goett, H.; Murrett, J.; Genninger, J.; Mendez, K.; Tripod, M.; Tyner, N.; Costantino, T.G. Lung Ultrasound vs. Chest X-Ray Study for the Radiographic Diagnosis of COVID-19 Pneumonia in a High-Prevalence Population. J. Emerg. Med. 2021, 60, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Rizzetto, F.; Perillo, N.; Artioli, D.; Travaglini, F.; Cuccia, A.; Zannoni, S.; Tombini, V.; di Domenico, S.L.; Albertini, V.; Bergamaschi, M.; et al. Correlation between lung ultrasound and chest CT patterns with estimation of pulmonary burden in COVID-19 patients. Eur. J. Radiol. 2021, 138, 109650. [Google Scholar] [CrossRef] [PubMed]
- Schalekamp, S.; Huisman, M.; van Dijk, R.A.; Boomsma, M.F.; Jorge, P.J.F.; de Boer, W.S.; Herder, G.J.M.; Bonarius, M.; Groot, O.A.; Jong, E.; et al. Model-based Prediction of Critical Illness in Hospitalized Patients with COVID-19. Radiology 2021, 298, E46–E54. [Google Scholar] [CrossRef] [PubMed]
- Mi, J.; Zhong, W.; Huang, C.; Zhang, W.; Tan, L.; Ding, L. Gender, age and comorbidities as the main prognostic factors in patients with COVID-19 pneumonia. Am. J. Transl. Res. 2020, 12, 6537–6548. [Google Scholar] [PubMed]
- Tong, X.; Cheng, A.; Yuan, X.; Zhong, X.; Wang, H.; Zhou, W.; Xu, X.; Li, Y. Characteristics of peripheral white blood cells in COVID-19 patients revealed by a retrospective cohort study. BMC Infect. Dis. 2021, 21, 1236. [Google Scholar] [CrossRef]
- Chen, R.; Liang, W.; Jiang, M.; Guan, W.; Zhan, C.; Wang, T.; Tang, C.; Sang, L.; Liu, J.; Ni, Z.; et al. Risk Factors of Fatal Outcome in Hospitalized Subjects with Coronavirus Disease 2019 From a Nationwide Analysis in China. Chest 2020, 158, 97–105. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Martha, J.W.; Wibowo, A.; Pranata, R. Prognostic value of elevated lactate dehydrogenase in patients with COVID-19: A systematic review and meta-analysis. Postgrad. Med. J. 2021. [Google Scholar] [CrossRef]
- Ismail, N.; Hassan, N.; Abd Hamid, M.H.N.; Yusoff, U.N.; Khamal, N.R.; Omar, M.A.; Wong, X.C.; Pathmanathan, M.D.; Mohd Zin, S.; Muhammad Zin, F.; et al. Association of smoking and severity of COVID-19 infection among 5889 patients in malaysia: A multi-center observational study. Int. J. Infect. Dis. 2022, 116, 189–196. [Google Scholar] [CrossRef]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Lian, N.; Deng, Y.; Lin, S. The impact of COPD and smoking history on the severity of COVID-19: A systemic review and meta-analysis. J. Med. Virol. 2020, 92, 1915–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission; Directorate-General for Communication; Directorate-General for Health and Food Safety. Attitudes of Europeans towards tobacco and electronic cigarettes: Report, European Commission. 2021. Available online: https://op.europa.eu/en/publication-detail/-/publication/c070c04c-6788-11eb-aeb5-01aa75ed71a1 (accessed on 19 April 2022). [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Score/ Grade | LUS Score | CT Score | CXR Score |
|---|---|---|---|
| 0 | regular finding: the existence of a regular and not thickened pleural line, with the sliding sign, and the presence of A-lines | no abnormalities | no abnormalities |
| 1 | some loss of aeration: irregular pleural line with some B lines | prevalent ground-glass opacities (GGOs) | interstitial infiltrates |
| 2 | severe loss of aeration: broken pleural line; small-to-large, consolidated areas with associated areas of white below the consolidated area | GGOs mixed with consolidations | interstitial and alveolar infiltrates (interstitial predominance) |
| 3 | complete loss of aeration: scanned area shows large dense consolidations; “white lung” | prevalent consolidations | interstitial and alveolar infiltrates (alveolar predominance) |
| No MV n/N (%), Median (IQR) | MV Required n/N (%), Median (IQR) | p * | No Death n/N (%), Median (IQR) | Death n/N (%), Median (IQR) | p * | |
|---|---|---|---|---|---|---|
| Comorbidity/habit | ||||||
| Arterial hypertension | 132/253 (52.2%) | 14/28 (50.0%) | 0.827 | 126/253 (49.8%) | 20/28 (71.4%) | 0.030 |
| Cardiovascular disease | 34/253 (13.4%) | 8/28 (28.6%) | 0.033 | 31/253 (12.3%) | 11/28 (39.3%) | 0.000 |
| COPD | 14/253 (5.5%) | 1/28 (3.6%) | 0.662 | 14/253 (5.5%) | 1/28 (3.6%) | 0.662 |
| CVI or TIA | 3/253 (1.2%) | 0/28 (0.0%) | 0.563 | 3/253 (1.2%) | 0/28 (0.0%) | 0.563 |
| Dementia | 3/253 (1.2%) | 0/28 (0.0%) | 0.563 | 1/253 (0.4%) | 2/28 (7.1%) | 0.001 |
| Diabetes | 50/253 (19.8%) | 6/28 (21.4%) | 0.835 | 50/253 (19.8%) | 6/28 (21.4%) | 0.835 |
| Hemiplegia | 0/253 (0.0%) | 1/28 (3.6%) | 0.003 | 0/253 (0.0%) | 1/28 (3.6%) | 0.003 |
| Kidney failure | 12/253 (4.7%) | 1/28 (3.6%) | 0.780 | 10/253 (4.0%) | 3/28 (10.7%) | 0.107 |
| Leukemia | 3/253 (1.2%) | 2/28 (7.1%) | 0.024 | 4/253 (1.6%) | 1/28 (3.6%) | 0.451 |
| Liver failure | 7/253 (2.8%) | 0/28 (0.0%) | 0.374 | 6/253 (2.4%) | 1/28 (3.6%) | 0.700 |
| Lymphoma | 7/253 (2.8%) | 0/28 (0.0%) | 0.374 | 6/253 (2.4%) | 1/28 (3.6%) | 0.700 |
| Malignancy | 25/253 (9.9%) | 4/27 (14.8%) | 0.425 | 22/253 (8.7%) | 7/28 (25.0%) | 0.008 |
| Myocardial infarct | 10/253 (4.0%) | 3/28 (10.7%) | 0.107 | 10/253 (4.0%) | 3/28 (10.7%) | 0.107 |
| Peptic ulcer | 2/253 (0.8%) | 1/28 (3.6%) | 0.175 | 2/253 (0.8%) | 1/28 (3.6%) | 0.175 |
| Peripheral vascular disease | 10/253 (4.0%) | 1/28 (3.6%) | 0.922 | 9/253 (3.6%) | 2/28 (7.1%) | 0.354 |
| Rheumatological disease | 8/253 (3.2%) | 0/28 (0.0%) | 0.341 | 8/253 (3.2%) | 0/28 (0.0%) | 0.341 |
| Smoker | 33/243 (13.6%) | 4/27 (14.8%) | 0.860 | 34/246 (13.8%) | 3/24 (12.5%) | 0.858 |
| Biometrics | ||||||
| Female gender | 68/252 (27.0%) | 10/28 (35.7%) | 0.952 | 66/252 (26.2%) | 12/28 (42.9%) | 0.063 |
| Age (years) | 62 (55–70) | 69 (62–75) | 0.004 | 62 (54–68) | 75 (69–82) | 0.000 |
| Weight (kg) | 91 (84–103) | 94 (82–103) | 0.627 | 91 (84–103) | 92 (80–97) | 0.388 |
| Height (cm) | 180 (173–186) | 175 (170–186) | 0.356 | 179 (173–187) | 176 (168–180) | 0.181 |
| BMI (kg/m2) | 28.3 (26.1–30.9) | 29.4 (27.8–33.1) | 0.088 | 28.4 (26.1–31.1) | 28.7 (26.9–32.9) | 0.803 |
| Day of the illness | 9 (6–12) | 6 (5–8) | 0.002 | 9 (6–12) | 7 (4–10) | 0.035 |
| Biochemical parameters | ||||||
| CRP (mg/L) | 76.3 (47.8–136.8) | 98 (67.8–146.6) | 0.101 | 79.9 (49.3–136.8) | 95.8 (61.4–146.6) | 0.416 |
| D–dimer (µg/L) | 0.92 (0.61–1.49) | 1.05 (0.61–2.20) | 0.529 | 0.88 (0.60–1.48) | 1.48 (0.72–2.66) | 0.051 |
| LDH (U/L) | 351 (282–424) | 434 (306–456) | 0.043 | 355 (285–429) | 366 (285–448) | 0.545 |
| Leukocyte count (109/L) | 7.9 (5.7–10.8) | 5.7 (4.5–8.7) | 0.010 | 7.9 (5.7–10.6) | 5.7 (4.4–10.5) | 0.042 |
| Lymphocytes (%) | 13.0 (8.4–18.4) | 16.3 (10.8–23.9) | 0.103 | 13.0 (8.5–18.4) | 16.3 (9.2–23.8) | 0.272 |
| Neutrophils (%) | 81.2 (74.6–86.9) | 75.8 (70.9–83.1) | 0.117 | 81.2 (74.8–86.7) | 75.8 (69.4–83.0) | 0.123 |
| pO2 (kPa) | 7.30 (6.51–7.97) | 7.27 (6.18–7.78) | 0.599 | 7.30 (6.50–7.95) | 7.20 (6.06–7.97) | 0.506 |
| spO2 (%) | 91 (88–93) | 89 (83–94) | 0.151 | 91 (88–93) | 88 (82–93) | 0.022 |
| hs-Troponin (ng/L) | 9.45 (6.50–15.30) | 10.9 (8.0–20.9) | 0.216 | 9.25 (6.55–14.65) | 14.6 (8.60–44.10) | 0.012 |
| Radiological scores | ||||||
| LUS score | 25 (19–31) | 31 (26–37) | 0.001 | 25 (18–31) | 32 (26–36) | 0.000 |
| CXR score | 6 (4–10) | 8 (6–10) | 0.125 | 6 (4–10) | 8 (6–12) | 0.016 |
| CT score | 22.0 ± 8.0 | 29.0 ± 2.0 | 0.146 | 21.6 ± 7.9 | 29.0 ± 3.8 | 0.050 |
| Variable | Coefficient | p | Odds Ratio | 95% CI | Cutoff | Sensitivity | Specificity |
| Mechanical ventilation | |||||||
| LUS score | 0.101 | <0.001 | 1.11 | 1.04–1.17 | >27 | 72.4% | 60.8% |
| Day of illness | −0.131 | 0.022 | 0.88 | 0.78–0.98 | ≤7 | 72.4% | 64.1% |
| Leukocyte count | −0.160 | 0.021 | 0.85 | 0.74–0.98 | ≤6.3 | 64.3% | 66.7% |
| Cardiovascular disease present | 1.019 | 0.041 | 2.77 | 1.04–7.35 | positive | 28.6% | 86.6% |
| Correctly Classified | AUC | 95% CI | Cutoff | Sensitivity | Specificity | ||
| Combined score | 88.9% | 0.807 | 0.755–0.851 | >0.51 | 85.7% | 66.4% | |
| Death | Coefficient | p | Odds Ratio | 95% CI | Cutoff | Sensitivity | Specificity |
| Age | 0.153 | <0.0001 | 1.17 | 1.10–1.24 | >65 | 89.3% | 65.4% |
| LUS score | 0.088 | 0.005 | 1.09 | 1.03–1.16 | >29 | 69.0% | 72.2% |
| Correctly Classified | AUC | 95% CI | Cutoff | Sensitivity | Specificity | ||
| Combined score | 93.2% | 0.859 | 0.814–0.901 | >9.6 | 96.5% | 57.9% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skopljanac, I.; Pavicic Ivelja, M.; Budimir Mrsic, D.; Barcot, O.; Jelicic, I.; Domjanovic, J.; Dolic, K. Can Lung Imaging Scores and Clinical Variables Predict Severe Course and Fatal Outcome in COVID-19 Pneumonia Patients? A Single-Center Observational Study. Life 2022, 12, 735. https://doi.org/10.3390/life12050735
Skopljanac I, Pavicic Ivelja M, Budimir Mrsic D, Barcot O, Jelicic I, Domjanovic J, Dolic K. Can Lung Imaging Scores and Clinical Variables Predict Severe Course and Fatal Outcome in COVID-19 Pneumonia Patients? A Single-Center Observational Study. Life. 2022; 12(5):735. https://doi.org/10.3390/life12050735
Chicago/Turabian StyleSkopljanac, Ivan, Mirela Pavicic Ivelja, Danijela Budimir Mrsic, Ognjen Barcot, Irena Jelicic, Josipa Domjanovic, and Kresimir Dolic. 2022. "Can Lung Imaging Scores and Clinical Variables Predict Severe Course and Fatal Outcome in COVID-19 Pneumonia Patients? A Single-Center Observational Study" Life 12, no. 5: 735. https://doi.org/10.3390/life12050735
APA StyleSkopljanac, I., Pavicic Ivelja, M., Budimir Mrsic, D., Barcot, O., Jelicic, I., Domjanovic, J., & Dolic, K. (2022). Can Lung Imaging Scores and Clinical Variables Predict Severe Course and Fatal Outcome in COVID-19 Pneumonia Patients? A Single-Center Observational Study. Life, 12(5), 735. https://doi.org/10.3390/life12050735